

Abstract
Objectives.
Subjective life expectancy (SLE) has been suggested as a predictor of mortality and mortality-related behaviors. Although critical for culturally diverse societies, these findings do not consider cross-cultural methodological comparability. Culture-specific reporting heterogeneity is a well-known phenomenon introducing biases, and research on this issue with SLE is not established.
Method.
Using data from the Health and Retirement Study, we examined reporting heterogeneity in SLE focusing on item nonresponse, focal points, and reports over time for five ethnic-cultural groups: non-Hispanic Whites, non-Hispanic Blacks, non-Hispanic other races, English-interviewed Hispanics, and Spanish-interviewed Hispanics.
Results.
On item nonresponse, Spanish-interviewed Hispanics said, “I don’t know,” to SLE significantly more than any other groups. Nearly half of the respondents chose 0, 50, or 100, making them focal points. However, the focal points differed: 50 for Whites, 100 for Blacks, and 0 for Spanish-interviewed Hispanics. The relationship of SLE measured at two time points was higher for Whites than minorities. Moreover, those who said “I don’t know” to SLE showed higher subsequent mortality than those who gave an answer. SLE was not a significant mortality predictor for Hispanics.
Discussion.
Overall, SLE is not free from culture-specific reporting heterogeneity. This warrants further research about its culture-relevant measurement mechanisms.
Key Words: Mortality predictions, Nonresponse, Racial and ethnic minorities, Reporting heterogeneity, Subjective life expectancy
Within the last two decades, the subjective life expectancy (SLE) question has emerged as a predictor of mortality in the literature (Elder, 2013; Ferraro, 2014; Hurd & McGarry, 1995, 2002; Perozek, 2008; van Doorn & Kasl 1998). The Health and Retirement Study (HRS) is credited as a main impetus for the emergence of SLE (Elder, 2013; Jylhä, 2011; Perozek, 2008), for which the origin and history are well documented (e.g., Dominitz & Manski, 1999; Manski, 1990). SLE asks respondents to estimate the probability that they will live up to a certain age. A current version of SLE in the HRS reads as follows: “I would like for you to give me a number from 0 to 100, where 0 means that you think there is absolutely no chance, and 100 means that you think the event is absolutely sure to happen. . . . What is the percent chance that you will live to be [75 (if age is less 65 or less)/80 (if age is 66–69)/85 (if age is 70–74)/90 (if age is 75–79)/95 (if age is 80–84)/100 (if age is 85–89)] or more?” The target age in expectation is a function of respondents’ current age. Note that a number of SLE-related studies (e.g., Brouwer & van Exel, 2005; Mirowsky, 1997; 1999; Mirowsky & Ross, 2000) used data asking SLE with a different wording: “to what age do you expect to live?” Currently, SLE is asked in a number of longitudinal surveys of older persons, such as the HRS, the English Longitudinal Study of Ageing, the Study of Health and Ageing in Europe, and the China Health and Retirement Longitudinal Study. Responses to this question are shown to be predictive of subsequent mortality even after controlling for mortality-related characteristics, such as demographic and socioeconomic characteristics and objective health measures (Perozek 2008; Siegel, Bradley, & Kasl, 2003; Smith, Taylor, & Sloan, 2001; van Doorn & Kasl 1998). A study by Perozek (2008) showed that SLE was in the same direction of revision to the life tables produced by the Social Security Administration. The predictive power of SLE has been linked to the possibilities that this measure incorporates private and subtle information germane to mortality yet unmeasurable through objective questions (Perozek, 2008). Hence, SLE is used to predict and understand individuals’ economic behaviors related to later stages of life (e.g., Hamermesh, 1985; Salm, 2010) and health behaviors (e.g., Carbone, Kverndokk, & Rogeberg, 2005; Scott-Sheldon, Carey, Vanable, & Senn, 2010).
Although the empirical evidence for SLE is impressive, there has been a debate over whether people are able to carry out probabilistic tasks cognitively (e.g., Gigerenzer, 1996; Manski, 2004; Tversky & Kahneman, 1974). Even if it were realistic to expect people to process probabilities, it should be noted that that SLE is a highly subjective measure, prone to measurement error (Elder, 2013; Griffin, Loh, & Hesketh, 2013; Hurd, 2009). The underlying mechanism of the measurement error in SLE can be illustrated with the survey question-answering process. In any given survey task, respondents first need to comprehend what the question is asking for. Based on this comprehension, they search for relevant information in the memories, judge the retrieved information in relation to the question, and formulate an answer in the solicited format. This is, in fact, a main framework used in the survey measurement literature (Schwarz, 2007) and suggests that response difficulties may arise in any of these steps.
The straightforward concept of life expectancy (life vs death) is unlikely to cause difficulties with the SLE question comprehension. Rather, it is the steps of searching for and retrieving relevant information and formulating an answer that respondents experience difficulties with. At the time of the interview, respondents may feel that the personal information they need in order to respond is uncertain in quality and insufficient in quantity (Jylhä, 2011). Consider a hypothetical respondent in his 50s and compare the SLE question to a question asking probabilities to retire by the age of 65 years. It is reasonable that the quantity and quality of relevant information may well differ between these two questions. This may explain the findings by Griffin and colleagues (2013): When answering SLE, respondents incorporated factors related to actual mortality, but the relative importance assigned to these factors was not realistic. Like all types of subjective probabilistic questions (e.g., de Bruin, Fischhoff, Millstein, & Halpern-Felsher, 2000), the tendency of SLE response heaping at certain focal values, such as 50 (Hurd &McGarry, 1995), is another indication of difficulty.
There is a scarce yet growing body of literature addressing noncomparability of SLE across racial and ethnic groups in the United States (e.g., Bulanda & Zhang, 2009; Mirowsky 1999; Mirowsky & Ross 2000). While Blacks, whose actual life expectancy is lower, report higher SLE than Whites (Hurd & McGarry, 1995), Mexican Americans report lower SLE than Whites, despite higher actual expectancy (Bulanda & Zhang, 2009). This noncomparability in SLE may be explained by differences in the type, availability, and integration of personal data necessary for responding to SLE across racial and ethnic groups. This, in turn, leads to differential cognitive difficulties associated with the question-answering process described above.
Furthermore, the implicit yet important premise of SLE is that respondents cognitively organize their personal experiences relevant for future events, known as the future-oriented time perspective (Gonzalez & Zimbardo, 1985). Time perspective is an unconscious yet fundamental cognitive process that people use to arrange personal experiences in the categories of past, present, or future (Block, 1990; Zimbardo & Boyd, 1999). The effects of time perspectives are examined through their relationships to various behaviors and attitudes, including health risk behaviors (Harwood, 1981; Henson, Carey, Carey, & Mais, 2006; Zimbardo, Keough, & Boyd, 1997), willingness to delay gratification (Romer, Duckworth, Sznitman, & Park, 2010), as well as subjective well-being (Drake, Duncan, Sutherland, Abernethy, & Henry, 2008; Guthrie, Butler, & Ward, 2009). As time perspective is mainly a product of culture (Graham, 1981), there may be a conflict in time perspective held by respondents and assumed in SLE. In other words, the level of difficulty may differ depending on respondents’ cultural background, and the cultural differences may invite distinctive response patterns, consequently resulting in reporting heterogeneity. The literature mainly discusses reporting heterogeneity with respect to verbally labeled ordinal response scales (e.g., Dowd & Todd 2011; Grol-Prokopczyk, Freese, & Hauser, 2011). However, it applies to all types of response scales, as reporting heterogeneity is essentially a variation in responses caused by a systematic variation related to respondent characteristics (e.g., Hispanics vs Whites) rather than a variation in the true yet unobservable state (Shmueli, 2003).
With this literature in mind, we postulated that there would be reporting heterogeneity in SLE, in particular, between Hispanics and non-Hispanic Whites associated with cultural differences. Although race and ethnicity are not cultures themselves, they are carriers of culture (Hong, 2009), playing a central role in establishing structures for organizing cognition (Nisbett, Peng, Choi, & Norenzayan, 2001).
Specifically, there are three cultural differences relevant to reporting heterogeneity of SLE. The first difference is related to time perspectives. Whites are described as future oriented (Graham, 1981; Kluckhohn & Strodtbeck, 1961), whereas Hispanics are described present oriented (Hall, 1959; Marín & Marín, 1991; Zea, Quezada, & Belgrave, 1994). The time perspective assumed in SLE may conflict with Hispanics’ time perspective but not with Whites.’ Second, Hispanics are reported to hold a fatalistic view, a belief that the course of life is beyond one’s control and there is little that one can do change the fate (Abraído-Lanza et al., 2007; Chavez, Hubbell, Mishra, & Valdez, 1997; Pérez-Stable, Sabogal, Otero-Sabogal, Hiatt, & McPhee, 1992). Fatalism is often translated to pessimistic beliefs about health and health outcomes. Coincidentally, fatalism is also characterized with the present time orientation (Zimbardo & Boyd, 1999). Third, the literature suggests that Hispanics tend to select end points of response scales more frequently than Whites (Hui & Triandis, 1989; Marín, Gamba, & Marín, 1992). Known as extreme response style, this tendency introduces biases in the measurement (Yang, Harkness, Chin, & Villar, 2010).
These cultural differences render two hypotheses relevant to SLE reporting heterogeneity. First, Hispanics, being focused on the present time, may not think about the future as much as Whites do and may not organize their personal data to be relevant for future events, such as mortality. This may lead Hispanics, compared with Whites, to experience a higher level of difficulty with SLE. This may further lead them to say, “I don’t know,” to SLE, resulting in a higher level of item nonresponse. Although the extant literature does not address SLE item nonresponse specifically, there is indirect evidence that the nonresponse for this item may be a nontrivial concern. SLE in the 1995 survey of Aging, Status and the Sense of Control Survey, for example, was subject to a high item nonresponse rate of 21.4% with 555 of out of 2,592 eligible cases not responding, and the higher hazards of SLE item nonresponse for Blacks than Whites adds more to this concern (Mirowsky & Ross, 2000).
Second, Hispanics’ fatalistic beliefs combined with their extreme response style may lead them to report a zero chance of living to be the target age at a higher level than Whites. Among Hispanics, the patterns of item nonresponse and a zero probability report may be more pronounced for those interviewed in Spanish rather than in English, regardless of whether the respondent is a monolingual Spanish speaker or a bilingual English–Spanish speaker. Monolingual Spanish-speaking Hispanics are more likely than bilingual Hispanics to be associated with Hispanic cultural values as Hispanics’ language use is a critical acculturation factor (Angel, Buckley, & Finch, 2001; Vega, Zimmerman, Warheit, Apospori, & Gil, 1993), sometimes found to be more influential than the country of origin or ancestry (Tompson & Lavrakas 2013). For bilingual speakers, interview language is known to introduce cultural norms associated with that language to the interview (Ross, Xun, & Wilson, 2002). Hence, Hispanics interviewed in Spanish are expected to show Hispanic-specific reporting heterogeneity more than those interviewed in English. This study examines these hypotheses using data from a major longitudinal survey of the aging population.
Data and methods
Source and Description
The data come from the 2004, 2006, 2008, and 2010 waves of the HRS. HRS is an age-cohort–based longitudinal panel survey of persons aged 50 years and older in the United States. Since its inception, HRS has conducted interviews in both English and Spanish. Spanish interviews account for about a half of the Hispanic sample, a figure comparable with the Hispanic sample in the National Health Interview Survey (NHIS) for the same age group (e.g., 46.5% in the HRS 2004 and 45.6% in the NHIS 2004). At the SLE question level, there had been changes to the wording and skip patterns prior to 2000. Since then, SLE has been asked among self-respondents aged 50–89 years in a consistent manner (see the Expectations section content area on http://hrsonline.isr.umich.edu/index.php?p=qnaires for detail).
SLE is asked differently based on respondents’ current age. Those aged 66–89 years are asked about SLE only once using the target age in the question wording presented earlier. For those aged 50–65 years, SLE was first asked with the target age of 75 years; unless they reported 0, SLE was then asked with 80 years as the target age. We combined these two questions in the analysis.
SLE is included in the middle of a series of questions that ask respondents to estimate the probabilities of future events on a scale of 0–100. One distinctive feature of this section is that those who do not give a response to the first three items are skipped to the next section, and hence, not asked the SLE item. The first three questions were expectations about income keeping up with inflation, leaving an inheritance, and receiving an inheritance. The skip rate is modest at, for example, 1.3% in the HRS 2004, with a slight variation by race/ethnicity with non-Hispanic Whites lowest at 1.0%, followed by Hispanics at 1.6%, and the remainder at 3.2%. The skipped cases are excluded from the analysis.
We examine SLE response patterns across five ethnic-cultural groups: non-Hispanic Whites, non-Hispanic Blacks, non-Hispanic other races, English-interviewed Hispanics, and Spanish-interviewed Hispanics. Our analysis applies to older adults aged 50–89 years and excludes proxy responses due to the nature of the SLE question. For the HRS 2004, this equates to a sample size of 17,158, among whom 12,875 were Whites, 2,404 were Blacks, 259 were other races, 827 were English-interviewed Hispanics, and 793 were Spanish-interviewed Hispanics. The skip rates described above were modest across these comparison groups, for example, ranging from 0.8% (for Whites) to 4.3% (for other races). Note that interview language (English or Spanish) in the HRS is chosen by respondents. Although respondents have an option of switching the language between waves, this occurs far less than 1% of the time. Hence, interview language is a rather static characteristic within person.
Analysis Plan
The analysis is conducted in three stages using Whites as a reference group in comparisons. The first stage focuses on a cross-sectional analysis of SLE. Item nonresponse that includes both “I don’t know” answers and refusals is examined. As refusals account for only about 7% of the SLE item nonresponse, item nonresponse can be regarded as a result of “don’t know” responses. Figure 1 illustrates the cumulative percent of each number response from 0 to 100 and item nonresponse to SLE from the HRS 2004. Numbers other than the focal points of 0, 50, and 100 are chosen rather infrequently. To understand these focal points while maintaining the granularity of information, we recode reported probabilities (P) into 13 ordinal categories: (1) P = 0, (2) 0 < P < 10, (3) 10 ≤ P < 20, (4) 20 ≤ P < 30, (5) 30 ≤ P < 40, (6) 40 ≤ P < 50, (7) P = 50, (8) 50 < P < 60, (9) 60 ≤ P < 70, (10) 70 ≤ P < 80, (11) 80 ≤ P < 90, (12) 80 ≤ P < 100, and (13) P = 100. We examine these response patterns as a function of race, ethnicity, and interview language, controlling for potential covariates: age, gender, marital status, educational attainment, number of chronic conditions, cognitive ability measured by word recall tasks, religious preference (Catholic, Protestant, Jewish, other, and none), importance of religion and frequency of religious service attendance, and interview mode.
Figure 1.

Cumulative distribution of detailed number responses and item nonresponse to subjective life expectancy, unweighted, adults aged 50–89 years, Health and Retirement Study 2004.
The second stage of analysis examines the longitudinal aspect of SLE measurement, specifically within-person changes in SLE reported across survey years. Understanding changes in SLE over time is an important topic as they may influence the changes in economic and health behaviors. This analysis is restricted to those who completed surveys in all relevant years and were asked of SLE using the same target age, resulting in a smaller sample size (n = 9,374 for the HRS 2004 and 2006).
In the third stage, we link SLE report from 2004 to the actual mortality status in 2006, 2008, 2010, and 2012 and examine how SLE from 2004, including its item nonresponse, differentiates subsequent mortality as well as how comparable its level of mortality prediction is across ethnic-cultural groups. In order to examine subsequent mortality based on SLE responses and nonresponse, we recode SLE as follows: (1) nonresponse, (2) P = 0, (3) 0 < P < 50, (4) P = 50, (5) 50 < P < 100, and (6) P = 100. This category coding is the same to that applied by Hurd, Smith, & Zissimopoulos (2004). It allows us to examine whether SLE item nonresponse includes subsequent mortality-related information and also collapses data on the 0–100 scale into categories with sufficiently large samples.
Results
We analyzed the HRS 2004, 2006, 2008, 2010, and 2012 data for cross-sectional analyses and found consistent results. Hence, we present our results using the HRS 2004 data for brevity in this section. Because weighted and unweighted analyses show similar results, we present unweighted findings for convenience of describing the sample rather than the population in the first and second analyses. In the third analysis, weighted results are presented to enable a discussion of the usage of SLE for predicting mortality in population-based research.
Subjective Life Expectancy Response Patterns
Item nonresponse
Overall, the item nonresponse rate is moderate at 4.9%. However, when this is examined by race and ethnicity, significant variations emerge as shown in Figure 2A. The item nonresponse rate is as low as 2.9% for Whites and as high as 14.8% for Hispanics, a significant difference with p < .001. Item nonresponse rates of Blacks and other races are 8.7% and 7.7%, both significantly higher than that of Whites. Once Hispanics are divided by interview language, the rates diverge. Spanish-interviewed Hispanics in the sample said, “I don’t know,” on SLE 25.0% of the time, a rate 22.1 percentage points higher than Whites.’ On the other hand, English-interviewed Hispanics did so 5.0% of the time, a rate rather comparable with Whites’, although statistically significantly higher.
Figure 2.
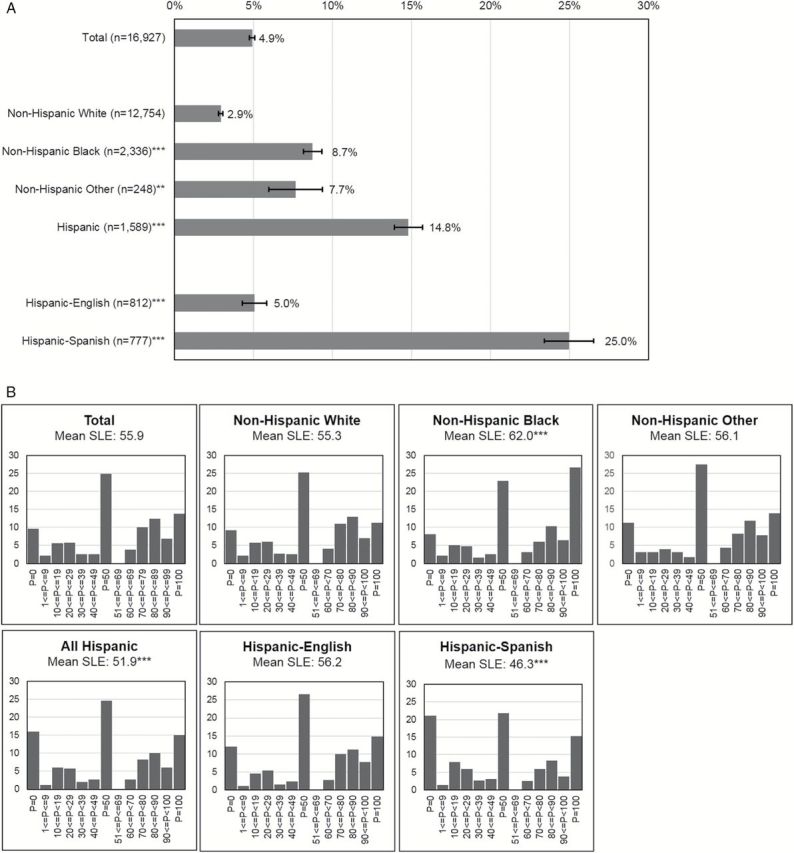
Response patterns to subjective life expectancy by race, ethnicity, and interview language, unweighted, adults aged 50–89 years, Health and Retirement Study 2004. (A) Item nonresponse to subjective life expectancy and the 95% confidence interval. Item nonresponse rate is significantly different from non-Hispanic Whites’ at **p < .01 and ***p < .001. (B) Distribution of subjective life expectancy responses. The mean of SLE is significantly different from non-Hispanic Whites’ at ***p < .001
Focal response points
Respondents on SLE can choose any number between 0 and 100. However, nearly half of them (48.3%) chose numbers 0, 50, or 100, making these numbers focal points. When examining by race, ethnicity, and interview language, the rate of choosing these focal points is highest for Spanish-interviewed Hispanics at 58.2%, followed by Blacks at 57.7%, English-interviewed Hispanics at 53.4%, other races at 52.8%, and Whites at 45.8%. All minority groups’ rates are significantly higher than Whites’.
Among these three focal points, 50 is chosen most frequently at 24.9% of the time, followed by 100 at 13.7% and 0 at 9.6%. Figure 2B shows the actual response distribution as well as the estimate of mean SLE for each group. For Whites, other races, and English-interviewed Hispanics, the focal point is 50 chosen by 25.2%, 27.5%, and 26.6% of the respondents, respectively, and the responses are distributed rather symmetrically around this focal point. However, that is not the case for Blacks and Spanish-interviewed Hispanics. For these groups, responses show an asymmetric distribution in opposite directions. For Blacks, 100 is the focal point selected 26.7% of the time, whereas it is 0 for Spanish-interviewed Hispanics selected 21.1% of the time, in addition to 50 chosen 21.8% of the time.
Item nonresponse and focal responses controlling for covariates
In a multinomial logistic regression, SLE response pattern (with five categories: (a) item nonresponse, (b) a focal response of 0, (c) a focal response of 50, (d) a focal response of 100, and (e) responses using other numbers (i.e., 1–49 and 51–99) where the last is used as the reference category) is modeled with race and ethnicity while controlling for potential covariates introduced earlier. Each column in Table 1 reports the odds of a specific response category compared with the reference category. For item nonresponse on SLE, all minority groups are associated with significantly higher odds, compared with Whites, with Spanish-interviewed Hispanics showing the highest odds of 12.623 (p < .001). On the focal response of 0, again minority groups, except for Blacks, show higher odds. When comparing the focal response of 50 to other number responses, the patterns are not significantly different across race and ethnicity. However, Blacks and Spanish-interviewed Hispanics, compared with Whites, are significantly more likely to report the focal response of 100 over responses of 1–49 and 51–99. As the response pattern of Hispanics differ by interview language, we examine Hispanics separated by interview language for the rest of the study. In an analysis not presented in this paper, we also examined the effect of nativity (U.S. born vs foreign born) specifically for Hispanics on these response patterns and found no significant relationship.
Table 1.
Multinomial Logistic Regression Model of Response Patterns (Item Nonresponse, Focal Response at 0, Focal Response at 50, Focal Response at 100, and Other Number Responses) on Subjective Life Expectancy, Unweighted, Adults Aged 50–89 Years, Health and Retirement Study 2004
| Dependent variable: Response patterna | ||||
|---|---|---|---|---|
| Item nonresponse | Focal at 0 | Focal at 50 | Focal at 100 | |
| odds ratio | Odds ratio | Odds ratio | Odds ratio | |
| Independent variable | ||||
| Race/ethnicity/language | ||||
| Non-Hispanic Whites | Ref. | Ref. | Ref. | Ref. |
| Non-Hispanic Blacks | 3.160*** | 1.141 | 1.087 | 2.775*** |
| Non-Hispanic others | 3.997*** | 1.928*** | 1.177 | 1.322 |
| English-interviewed Hispanic | 1.755** | 1.641** | 1.158 | 1.206 |
| Spanish-interviewed Hispanic | 12.623*** | 3.043*** | 0.924 | 1.312* |
| Control variables | ||||
| Age (year) | 1.037*** | 1.057*** | 1.002 | 0.983*** |
| Sex: female vs male | 1.372*** | 0.932 | 0.916* | 0.993 |
| Marital status: not married vs married | 1.502*** | 1.317*** | 1.120** | 1.109 |
| Education: ≤high school vs some college+ | 2.025*** | 2.118*** | 1.461*** | 1.564*** |
| Number of chronic conditions (0–8) | 1.059 | 1.281*** | 1.036* | 0.867*** |
| Cognition: word recall score (0–20) | 0.877*** | 0.914*** | 0.990 | 1.001 |
| Religion | 0.684 | 0.980 | 1.104 | 1.029 |
| Catholic vs none | ||||
| Protestant vs none | 0.624* | 0.851 | 1.026 | 0.890 |
| Jewish vs none | 2.590*** | 1.196 | 1.097 | 1.324 |
| Other vs none | 0.968 | 0.618 | 0.847 | 1.049 |
| Importance of religion | 1.369*** | 1.000 | 1.028 | 1.235*** |
| Religious service attendance frequency | 1.028 | 0.859*** | 0.989 | 0.974 |
| Interview mode: face-to-face vs telephone | 0.635*** | 0.901 | 0.894* | 0.789*** |
Notes. aThe reference category is other number response with values 1–49, 51–99.
Significant at *p < .05. **p < .01. ***p < .001.
Table 1 shows that, all minority groups are more likely to choose these focal points on SLE than Whites, a significant result even after controlling for likely correlates of response styles.
Among the control variables, it is notable that education shows consistently significant relationships with all response patterns. Those with high school or less education are associated with a higher odds of item nonresponse and using all three focal points than those with some college or higher education. Even after education is accounted for, those scoring higher on cognitive ability (memory) are less likely to report, “I don’t know,” or the focal point of 0 to SLE. Religion also plays a role in response patterns of SLE. Notably, Jewish respondents are significantly more likely to say, “I don’t know,” to SLE, compared with those with no religion, whereas Protestants are significantly less likely to do so. Those who view religion as important are more likely to say, “I don’t know,” or 100 to SLE, whereas those who attend religious service frequently are less likely to choose 0 on SLE.
Changes in Subjective Life Expectancy Across Years
If respondents are asked about life expectancy toward the same target age at two time points, the changes can be examined only when they respond both times. Between 2004 and 2006, a total of 10,081 respondents were asked about SLE for the same target age. Among them, 93.0% provided answers both times. This rate differs substantially (Rao-Scott =χ2 = 836.7; p < .001), as Whites show the highest rate at 95.8%, followed by English-interviewed Hispanics (91.5%), Blacks (87.7%), other races (87.6%), and Spanish-interviewed Hispanics (61.4%).
Among those who responded both times, we examine the changes in SLE reports: whether the reported expectancy decreased, remained the same, or increased. Overall, the corresponding rates are 37.6%, 28.9%, and 33.6%. There is no difference across ethnic-cultural groups in these rates (Rao-Scott χ2 = 9.3; p = .317).
SLEs measured at two time points are conceptually related. On one hand, it is imaginable that the reported expectancy toward the same target age should not increase over time as respondents become older. On the other hand, because respondents’ age becomes closer to the target age in SLE question over time, higher expectancy may be expected. We examine SLE measured in 2006 as a function of SLE in 2004 through simple linear regression separately by race, ethnicity, and interview language (Supplementary Table 1). The focus is the magnitudes of the regression coefficients as well as how much variance in SLE in 2006 is explained by SLE in 2004 through R 2. Overall, the two SLE measures show a positive relationship with = 0.621 (p < .001), and 38.1% of the variance in SLE 2006 is explained by SLE 2004. The relationship between the two SLE measures is significantly higher for Whites ( = 0.658) than for Blacks ( = 0.481), other races ( = 0.416), and both Hispanic groups ( = 0.502 for English interviewees and = 0.580 for Spanish interviewees). Moreover, the model fit is highest for Whites with an R 2 of 0.430 and lowest for other races as SLE measured in 2004 accounts for 20.0% of the variance of SLE in 2006.
Relationship Between Subjective Life Expectancy and Subsequent Survival
The measurement utility of SLE is examined by linking SLE in 2004 with actual mortality status in 2006, 2008, 2010, and 2012, which provides 2-, 4-, 6-, and 8-year survival rates. Supplementary Table 2 includes proportions of surviving respondents across ethnic-cultural groups. (Due to small sample sizes, we exclude other race respondents in this analysis.) Naturally, survival rates of those who were asked of SLE in 2004 decrease from 96.3% in 2006 to 92.1% in 2008, to 86.3% in 2010, and to 81.7% in 2012. The 2-year rate is not significantly different across comparison groups based on the Rao-Scott χ2 test, but the rates from later years are, mainly due to higher survival rates of Hispanic groups and lower rates of non-Hispanic Blacks.
In order to assess whether SLE differentiates mortality in subsequent years, the subsequent survival rates are examined by SLE response categories of nonresponse, P = 0, 0 < P < 50, P = 50, 50 < P < 100, and P = 100. If SLE is a good predictor, there should be noticeable gaps in the survival rates across these categories, and the survival rates should increase as probabilities given to SLE increase. For instance, the survival rates of those who report 0 on SLE should decline more than the rates of those who report 100, whereas the rates of those who report 50 should be placed somewhere in the middle. Figure 3 shows that overall, those who report 0 experience lower survival than those reporting 100 with a 8-year survival rates of 57.7% and 86.8%. Differences in survival rates across the SLE categories are not monotonic. In fact, the highest survival rate is observed for those who report values 51–99 at 90.8%. One notable pattern is the survival rate of SLE item nonrespondents who appear to experience mortality far more than the respondents except for those reporting 0. Their 8-year survival rate is 70.1%. This is further examined in Supplementary Table 3, controlling for correlates of mortality measured in 2004, similar to those in Table 1. Those who say, “I don’t know,” to SLE show a comparable survival rate with those who report 0 on SLE and significantly lower mortality than those reporting numbers 50–99 but not those reporting 1–49 or 100.
Figure 3.

Two-, four-, six-, and eight-year survival rates (%) by response to subjective life expectancy at baseline by race, ethnicity, and interview language, weighted, adults aged 50–89 years at baseline, Health and Retirement Study 2004 (baseline), 2006, 2008, 2010, and 2012.
If the mortality prediction of SLE is comparable across ethnic-cultural groups, the decreasing pattern of survival rates based on SLE responses should be comparable. Figure 3 does not support this. For Whites, the 8-year survival rates are 55.0% and 87.7% for those reporting 0 and 100, respectively, resulting in a 32.7 percentage points difference. For Blacks, the difference was 24.2 percentage points (58.4% vs 82.6%). However, for English-interviewed Hispanics, the difference between these two SLE response categories was 5.6 percentage points (82.2% vs 87.9% survival rates) and for Spanish-interviewed Hispanics, it was 11.4 percentage points (74.0% vs 85.4% survival rates). This is confirmed by multivariate analyses that control for mortality-related correlates as those in Supplementary Table 3 (results not shown). The effect of SLE for predicting 8-year mortality is significant for Whites and Blacks but not for either Hispanic groups. This holds regardless of how SLE is used–whether using SLE as a continuous variable on the scale of 0–100 or an ordinal variable with categories in Figure 3 and whether including or excluding nonresponse. The low survival rates of SLE item nonrespondents discussed earlier hold across all comparison groups. Respondents who show the highest survival rates across all comparison groups are not those who report 100 to SLE but those who report 51–99.
Discussion
This study shows that SLE, although not perfect, predicts subsequent mortality reasonably for Whites and Blacks, who comprise the majority of the elderly U.S. population. For Hispanics, however, SLE does not differentiate subsequent mortality well. The likely reason is not only the potential measurement error in SLE but also the noncomparability in the measurement error across ethnic-cultural groups examined in this study. The noncomparability is manifested through reporting patterns heterogeneous to each group. Most notably, more than 20% of Hispanic respondents interviewed in Spanish responded to SLE with “I don’t know,” resulting in no data for more than one out of five cases. This item nonresponse pattern affected not only cross-sectional but also longitudinal examinations of SLE. The changes in SLE between 2004 and 2006 for Spanish-interviewed Hispanics were subject to nearly 40% missing, as they did not provide an answer to SLE at either time points. Reporting heterogeneity was also evident among respondents. Among Whites who responded to SLE, more than one out of four reported a 50% chance of life expectancy, making it a focal point. The focal point, however, was heterogeneous across comparison groups as it was 100 for Blacks and 0 for Spanish-interviewed Hispanics. This culture-specific reporting heterogeneity appears to influence examination of SLE measured at two time points, which should be related conceptually. The extent to which SLE measured in 2004 explained that SLE 2006 was much larger for White respondents than for the minority groups. In particular, SLE in 2004 accounts for the variance of SLE in 2006 less for minority groups than Whites.
Given the use of SLE in analyses informing policies, the hypotheses examined in this study have implications far beyond methodological aspects of SLE. In particular, mortality prediction is an important utility of SLE for both research and policy purposes. This study offers two methodological observations relevant for these purposes. First, item nonresponse on SLE appeared to contain important information related to mortality. Those who said, “I don’t know,” were equally likely to experience mortality in subsequent time points as those reporting 0 and significantly more likely than those who provided an answer with other numbers. Using only the cases that responded to SLE for predictions as done in the current literature ignores this mortality-relevant information contained in the missingness. This somewhat echoes analyses by Hurd and colleagues (2004). With a recoded categorical SLE similar to the one in the present study, their models for predicting retirement and Social Security benefits of claiming behaviors showed a significant effect of SLE nonresponse as the nonresponse was associated with decreased probabilities of retirement and claiming Social Security benefits by the age of 62 years. Unfortunately, as item nonresponse was not the focus of their study, Hurd and colleagues made no further comment on the finding. However, if Social Security policies are informed by a SLE-based analysis that ignores the item nonresponse, such policies may be ineffective and potentially erroneous.
Second, the racial, ethnic, and linguistic composition of the elderly population in the United States is shifting quickly. Hispanics are emerging as the major minority group in the population (U.S. Census Bureau, 2011). This trend is contributing to a projected growth of Spanish usage (Shin & Ortman, 2011). Hence, mortality prediction for Hispanics is important not only as such but also for understanding changes in the composition of the older population in general. The noncomparability of SLE across race and ethnicity is not overly surprising, as little has been examined about SLE beyond the White population (Irby-Shasanmi, 2013). However, the inconclusive predictive power of SLE for Hispanics combined with reporting heterogeneity manifested through high item nonresponse and frequent use of the focal point of 0 especially with Spanish-interviewed Hispanics raises concerns about the effectiveness of the current practice of SLE data collection and policy-relevant analyses. For example, high item nonresponse rates by Spanish-interviewed Hispanics in this study mean that a disproportionately larger amount of mortality-related information is ignored for that group, which, in turn, may dampen prediction of mortality and mortality-related characteristics in unknown directions.
These findings do not deny the utility of SLE. As shown in the present study as well as other studies, SLE is a reasonable predictor of subsequent mortality and mortality-related behaviors. Rather, the findings in this study warrant future research that could improve the utility of SLE in a number of ways. First, one may consider imputing SLE for nonrespondents and examine the effect of ignoring versus incorporating missing cases in the analysis. Identifying key covariates for imputation will be an important step for this.
Second, research could investigate the connotations underlying certain number responses. For example, does 100% really indicate a higher chance than 99%? Is 50% an indirect way of saying, “I don’t know”? For the second question, our analysis using a different data source suggests this may be the case (results not shown). In that study, when respondents reported 50% on subjective expectancy questions, they were asked a follow-up question about the level of certainty in their response. A large proportion of the respondents indicated uncertainty. More importantly, when “I don’t know” and uncertain 50% are combined into a category to code uncertain response, the racial-ethnic differences observed with “I don’t know” were attenuated largely. This suggests that 50% may be a way of expressing uncertainty for Whites, whereas “I don’t know” is an expression of uncertainty for the racial and ethnic minorities.
Third, if not SLE, what are the alternatives for mortality prediction? Self-rated health (SRH) is an obvious choice supported by a volume of research repeatedly confirming its power for mortality prediction (e.g., Idler & Benyamini, 1997; Mossey & Shapiro, 1982). However, this is subject to a debate. SLE and SRH are shown to have independent effects on mortality (Siegel, Bradley, & Kasl, 2003), meaning that SLE explains aspects of mortality that SRH does not capture. Additionally, recent studies on SRH show that this measure is sensitive to its order in a questionnaire for Hispanics, in particular Spanish-speaking Hispanics, but not for Whites (Lee, Schwarz, & Goldstein, 2014) and that this sensitivity affects mortality prediction for Hispanics (Lee & Schwarz, 2014).
These questions call for scrutinizing the underlying measurement mechanism of SLE, as recommended by Jylhä (2011) and Griffin and colleagues (2013). One of the best ways to understand the measurement mechanism of any survey item is to directly examine the question-answering process discussed earlier. For example, cognitive interviews and/or focus groups could be used to determine what respondents understand about the intent of the SLE and the reason they give different responses. Studies could also compare findings based on cruder measures, such as a 5-point scale (e.g., very likely, somewhat likely, neutral, somewhat unlikely, and very unlikely), with those given on the 0%–100% probability scale of the current SLE. In all these examinations, it will be important to consider various ethnic-cultural groups systematically to improve comparability.
Measurement mechanisms, when examined systematically across ethnic-cultural groups, have the potential to reveal group-specific correlates of not only SLE responses but also distinctive response patterns, including “I don’t know” and focal responses, that are germane to mortality prediction. Without such systematic examinations, we may continue to use SLE without understanding what it really measures and without being able to explain noncomparability of SLE across ethnic-cultural groups. This limits the utility of SLE in predicting mortality and mortality-related behaviors especially when accounting for minority populations.
Supplementary Material
Supplementary material can be found at: http://psychsocgerontology.oxfordjournals.org/
Funding
This work was supported partially by a grant (U01 AG009740) from the National Institute of Aging.
Supplementary Material
Acknowledgments
S. Lee originated the study idea, performed the analyses, and led the paper writing. J. Smith helped in planning the study and analyses and contributed to writing and revising the paper.
References
- Abraído-Lanza A. F. Viladrich A. Flórez K. R. Céspedes A. Aguirre A. N., & De La Cruz A. A (2007). Commentary: Fatalismo reconsidered: A cautionary note for health-related research and practice with Latino populations. Ethnicity & Disease, 17, 153–158. [PMC free article] [PubMed] [Google Scholar]
- Angel J. L. Buckley C. J., & Finch B. K (2001). Nativity and self-assessed health among pre-retirement age Hispanics and Non-Hispanic Whites. International Migration Review, 35, 784–803. doi:10.1111/j.1747-7379.2001.tb00041.x [Google Scholar]
- Block R. A. (1990). Introduction. In Block R. A. (Ed.), Cognitive models of psychological time (pp. xiii–xviii). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Brouwer W. B. F., & van Exel N. J. A (2005). Expectations regarding length and health related quality of life: some empirical findings. Social Science & Medicine, 61, 1083–1094. doi:10.1016/j.socscimed.2005.01.008 [DOI] [PubMed] [Google Scholar]
- Bulanda J. R., & Zhang Z (2009). Racial-ethnic differences in subjective survival expectations for the retirement years. Research on Aging, 31, 688–709. doi:10.1177/0164027509343533 [Google Scholar]
- Carbone J. C. Kverndokk S., & Rogeberg O. J (2005). Smoking, health, risk, and perception. Journal of Health Economics, 24, 631–653. doi: 10.1016/j.jhealeco.2004.11.001 [DOI] [PubMed] [Google Scholar]
- Chavez L. R. Hubbell F. A. Mishra S. I., & Valdez R. B (1997). The influence of fatalism on self-reported use of Papanicolaou smears. American Journal of Preventive Medicine, 13, 418–424. [PubMed] [Google Scholar]
- de Bruin W. B. Fischhoff B. Millstein S. G., & Halpern-Felsher B. L (2000). Verbal and numerical expressions of probability: ‘It’s a fifty-fifty chance.’ Organizational Behavior and Human Decision Processes, 81, 115–131. doi:10.1006/obhd.1999.2868 [DOI] [PubMed] [Google Scholar]
- Dominitz J., & Manski C. F (1999). The several cultures of research on subjective expectations. In Smith J. P., Willis R. J. (Eds.), Wealth, work, and health: Innovations in measurement in the social sciences (pp. 15–33). Ann Arbor, MI: The University of Michigan Press. [Google Scholar]
- Dowd J., & Todd M (2011). Does self-reported health bias the measurement of health inequalities in U.S. adults? Evidence using anchoring vignettes from the Health and Retirement Study. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 66, 478–489. doi:10.1093/geronb/gbr050 [DOI] [PubMed] [Google Scholar]
- Drake L. Duncan E. Sutherland F. Abernethy C., & Henry C. (2008). Time perspective and correlates of wellbeing. Time & Society, 17, 46–61. doi:10.1177/0961463X07086304 [Google Scholar]
- Elder T. E. (2013). The predictive validity of subjective mortality expectations: evidence from the Health and Retirement Study. Demography, 50, 569–589. doi:10.1007/s13524-012-0164-2 [DOI] [PubMed] [Google Scholar]
- Ferraro K. F. (2014). The time of our lives: recognizing the contributions of Mannheim, Neugarten, and Riley to the study of aging. The Gerontologist, 54, 127–133. doi:10.1093/geront/gnt048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gigerenzer G. (1996). On narrow norms and vague heuristics: A reply to Kahneman and Tversky. Psychological Review, 103, 592–596. [Google Scholar]
- Gonzalez A., & Zimbardo P. G (1985). Time in perspective. Psychology Today, 19, 21–26. [Google Scholar]
- Graham R. J. (1981). The role of perception of time in consumer research. Journal of Consumer Research, 7, 335–342. doi:10.1086/208823 [Google Scholar]
- Griffin B. Loh V., & Hesketh B (2013). A mental model of factors associated with subjective life expectancy. Social Science & Medicine, 82, 79–86. doi:10.1016/j.socscimed.2013.01.026 [DOI] [PubMed] [Google Scholar]
- Grol-Prokopczyk H. Freese J., & Hauser R. M (2011). Using anchoring vignettes to assess group differences in general self-rated health. Journal of Health and Social Behavior, 52, 246–261. doi:10.1177/0022146510396713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guthrie L. C. Butler S. C., & Ward M. M (2009). Time perspective and socioeconomic status: A link to socioeconomic disparities in health? Social Science & Medicine, 68, 2145–2151. doi:10.1016/j.socscimed.2009.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall E. T. (1959). The silent language. Garden City, NY: Doubleday. [Google Scholar]
- Hamermesh D. S. (1985). Expectations, life expectancy, and economic behavior. The Quarterly Journal of Economics, 100, 389–408. doi:10.2307/1885388 [Google Scholar]
- Harwood A. (1981). Ethnicity and medical care. Cambridge, MA: Harvard University Press. [Google Scholar]
- Henson J. M. Carey M. P. Carey K. B., & Maisto S. A. (2006). Associations among health behaviors and time perspective in young adults: Model testing with boot-strapping replication. Journal of Behavioral Medicine, 29, 127–137. doi:10.1007/s10865-005-9027-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hong Y. (2009). A dynamic constructivist approach to culture: Moving from describing culture to explaining culture. In Wyer R. S. Chiu C., & Hong Y. (Eds.), Understanding culture. Theory, research, and application (pp. 3–24). New York, NY: Psychology Press. [Google Scholar]
- Hui C. H., & Triandis H. C (1989). Effects of culture and response format on extreme response style. Journal of Cross-Cultural Psychology, 20, 296–309. doi:10.1177/0022022189203004 [Google Scholar]
- Hurd M. D. (2009). Subjective probabilities in household surveys. Annual Review of Economics, 1, 543–562. doi:10.1146/annurev.economics.050708.142955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurd M. D., & McGarry K (1995). Evaluation of the subjective probabilities of survival in the Health and Retirement Study. Journal of Human Resources, 30, 268–292. doi:10.2307/146285 [Google Scholar]
- Hurd M. D., & McGarry K (2002). The predictive validity of subjective probabilities of survival. The Economic Journal, 112, 966–985. doi:10.1111/1468-0297.00065 [Google Scholar]
- Hurd M. D. Smith J. P., & Zissimopoulos J. M (2004). The effects of subjective survival on retirement and Social Security claiming. Journal of Applied Econometrics, 19, 761–775. doi:10.1002/jae.752 [Google Scholar]
- Idler E., & Benyamini Y (1997). Self-rated health and mortality: a review of twenty-seven community studies. Journal of Health Social Behavior, 38, 21–37. doi:10.2307/2955359 [PubMed] [Google Scholar]
- Irby-Shasanmi A. (2013). Predictors of subjective life expectancy among African Americans. Research on Aging, 35, 322–347. doi:10.1177/0164027512442945 [Google Scholar]
- Jylhä M. (2011). Self-rated health and subjective survival probabilities as predictors of mortality. In Rogers R. G., Crimmins E. M. (Eds.), International handbooks of population 2: International handbook of adult mortality (pp. 329–344). New York, NY: Springer. [Google Scholar]
- Kluckhohn F. R., & Strodtbeck F. L (1961). Variations in value orientations. Evanston, IL: Row-Paterson. [Google Scholar]
- Lee S., & Schwarz N (2014). Question context and priming meaning of health: Effect on differences in self-rated health between Hispanics and non-Hispanic Whites. American Journal of Public Health, 104, 179–185. doi:10.2105/AJPH.2012.301055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee S. Schwarz N., & Goldstein L. S (2014). Culture-sensitive question order effects of self-rated health between older Hispanic and non-Hispanic adults in the United States. Journal of Aging and Health, 26, 860–883. doi:10.1177/0898264314532688 [DOI] [PubMed] [Google Scholar]
- Manski C. F. (1990). The use of intentions data to predict behavior: A best case analysis. Journal of the American Statistical Association, 85, 934–940. doi:10.1080/01621459.1990.10474964 [Google Scholar]
- Manski C. F. (2004). Measuring expectations. Econometrica, 72, 1329–1376. doi:10.1111/j.1468-0262.2004.00537.x [Google Scholar]
- Marín G., & Marín B. V (1991). Research with Hispanic populations. Newbury Park, CA: Sage. [Google Scholar]
- Marín G. Gamba R. J., & Marín B. V (1992). Extreme response style and acquiescence among Hispanics: The role of acculturation and education. Journal of Cross-Cultural Psychology, 23, 498–509. doi:10.1177/0022022192234006 [Google Scholar]
- Mirowsky J. (1997). Age, subjective life expectancy, and the sense of control: the horizon hypothesis. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 52, 125–134. doi:10.1093/geronb/52B.3.S125 [DOI] [PubMed] [Google Scholar]
- Mirowsky J. (1999). Subjective life expectancy in the US: Correspondence to actuarial estimates by age, sex and race. Social Science & Medicine, 49, 967–979. doi:10.1016/S0277-9536(99)00193-8 [DOI] [PubMed] [Google Scholar]
- Mirowsky J., & Ross C. E (2000). Socioeconomic status and subjective life expectancy. Social Psychology Quarterly, 63, 133–151. doi:10.2307/2695888 [Google Scholar]
- Mossey J., & Shapiro E (1982). Self-rated health: a predictor of mortality among the elderly. American Journal of Public Health, 72, 800–808. doi:10.2105/AJPH.72.8.800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nisbett R. E. Peng K. Choi I., & Norenzayan A (2001). Culture and systems of thought: holistic versus analytic cognition. Psychological Review, 108, 291–310. doi:10.1037/0033-295X.108.2.291 [DOI] [PubMed] [Google Scholar]
- Pérez-Stable E. J. Sabogal F. Otero-Sabogal R. Hiatt R. A., & McPhee S. J (1992). Misconceptions about cancer among Latinos and Anglos. JAMA: the journal of the American Medical Association, 268, 3219–3223. [DOI] [PubMed] [Google Scholar]
- Perozek M. (2008). Using subjective expectations to forecast longevity: Do survey respondents know something we don’t know? Demography, 45, 95–113. doi:10.1353/dem.2008.0010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romer D. Duckworth A. L. Sznitman S., & Park S (2010). Can adolescents learn self-control? Delay of gratification in the development of control over risk taking. Prevention Science, 11, 319–330. doi:10.1007/s11121-010-0171-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross M. Xun W. Q. E., & Wilson A. E (2002). Language and the bicultural self. Personality and Social Psychology Bulletin, 28, 1040–1050. doi:10.1177/01461672022811003 [Google Scholar]
- Salm M. (2010). Subjective mortality expectations and consumption and saving behaviours among the elderly. Canadian Journal of Economics/Revue canadienne d’économique, 43, 1040–1057. doi:10.1111/j.1540-5982.2010.01605.x [Google Scholar]
- Schwarz N. (2007). Cognitive aspects of survey methodology. Applied Cognitive Psychology, 21, 277–287. doi:10.1002/acp.1340 [Google Scholar]
- Scott-Sheldon L. A. Carey M. P. Vanable P. A., & Senn T. E (2010). Subjective life expectancy and health behaviors among STD clinic patients. American Journal of Health Behavior, 34, 349–361. doi:10.5993/AJHB.34.3.10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shin H. B., & Ortman J. M (2011). Language projections: 2010 to 2020. Paper presented at the 2011 Federal Forecasters Conference, Washington, DC: Retrieved from http://www.census.gov/hhes/socdemo/language/data/acs/Shin_Ortman_FFC2011_paper.pdf [Google Scholar]
- Shmueli A. (2003). Socio-economic and demographic variation health and in its measure: the issue of reporting heterogeneity. Social Science & Medicine, 57, 125–134. doi:10.1016/S0277-9536(02)00333-7 [DOI] [PubMed] [Google Scholar]
- Siegel M. Bradley E. H., & Kasl S. K (2003). Self-rated life expectancy as a predictor of mortality: Evidence from the HRS and AHEAD surveys. Gerontology, 49, 265–71. doi:10.1159/000070409 [DOI] [PubMed] [Google Scholar]
- Smith V. K. Taylor D. H., & Sloan F. A (2001). Longevity expectations and death: Can people predict their own demise? The American Economic Review. 91, 1126–1134. doi:10.2139/ssrn.236813 [Google Scholar]
- Tompson T., Lavrakas P. J. (2013). Cross-cultural perspectives on surveys of the U.S. Hispanic population. Paper presented at the annual meeting of the American Association for Public Opinion Research, Boston, MA. [Google Scholar]
- Tversky A., & Kahneman D (1974) Judgment under uncertainty: Heuristics and biases. Science, 185, 1124–1131. doi:10.1126/science.185.4157.1124 [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau (May 2011). The Hispanic Population: 2010: 2010 Census Briefs. Washington, D.C: U.S. Department of Commerce; Retrieved from http://www.census.gov/prod/cen2010/briefs/c2010br-04.pdf [Google Scholar]
- van Doorn C., & Kasl S. V (1998). Can parental longevity and self-rated life expectancy predict mortality among older persons? Results from an Australian cohort. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 53, 28–34. doi:10.1093/geronb/53B.1.S28 [DOI] [PubMed] [Google Scholar]
- Vega W. A. Zimmerman R. S. Warheit G. J. Apospori E., & Gil A. G (1993). Risk factors for early adolescent drug use in four ethnic and racial groups. American Journal of Public Health, 83, 185–189. doi:10.2105/AJPH.83.2.185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang Y. Harkness J. A. Chin T. Y., & Villar A (2010). Response styles and culture. In Harkness J.A. Braun M. Edwards B. Johnson T. P. Lyberg L. Mohler P. Pennell B. E. & Smith T. W. (Eds.), Survey methods in multinational, multiregional and multicultural contexts (pp. 203–223). Hoboken, NJ: Wiley. [Google Scholar]
- Zea M. C. Quezada T., & Belgrave F. Z (1994). Latino cultural values: Their role in adjustment to disability. Journal of Social Behavior & Personality, 9, 185–200. [Google Scholar]
- Zimbardo P. G., & Boyd J. N (1999). Putting time in perspective: A valid, reliable, individual-differences metric. Journal of Personality and Social Psychology. 77, 1271–1288. doi:10.1037/0022-3514.77.6.1271 [Google Scholar]
- Zimbardo P. G. Keough K. A. & Boyd J. N. (1997). Present time perspective as predictor of risky driving. Personality and Individual Differences, 23, 1007–1023. doi:10.1016/S0191-8869(97)00113-X [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.