

Abstract
Allogeneic hematopoietic stem cell transplantation is required as rescue therapy in about 20% of pediatric patients with acute lymphoblastic leukemia. However, the relapse rates are considerable, and relapse confers a poor outcome. Early assessment of the risk of relapse is therefore of paramount importance for the development of appropriate measures. We used the EuroChimerism approach to investigate the potential impact of lineage-specific chimerism testing for relapse-risk analysis in 162 pediatric patients with acute lymphoblastic leukemia after allogeneic stem cell transplantation in a multicenter study based on standardized transplantation protocols. Within a median observation time of 4.5 years, relapses have occurred in 41/162 patients at a median of 0.6 years after transplantation (range, 0.13–5.7 years). Prospective screening at defined consecutive time points revealed that reappearance of recipient-derived cells within the CD34+ and CD8+ cell subsets display the most significant association with the occurrence of relapses with hazard ratios of 5.2 (P=0.003) and 2.8 (P=0.008), respectively. The appearance of recipient cells after a period of pure donor chimerism in the CD34+ and CD8+ leukocyte subsets revealed dynamics indicative of a significantly elevated risk of relapse or imminent disease recurrence. Assessment of chimerism within these lineages can therefore provide complementary information for further diagnostic and, potentially, therapeutic purposes aiming at the prevention of overt relapse. This study was registered at clinical.trials.gov with the number NC01423747.
Introduction
Treatment of acute lymphoblastic leukemia (ALL) according to current Berlin-Frankfurt-Münster (BFM)-ALL or similar intensive protocols results in cure rates of approximately 80% with chemotherapy alone.1,2 Nevertheless, a significant proportion of patients with resistant or relapsed disease require allogeneic hematopoietic stem cell transplantation (HSCT) as rescue therapy. Across all subtypes of pediatric ALL, about 20% of patients in industrialized countries currently undergo allogeneic HSCT from related or unrelated donors.3 Disease relapse, with an overall incidence of approximately 25%, is the dominant cause of mortality in this setting.4 Clone-specific markers for the detection of minimal residual disease (MRD) are available in most instances, and the current detection limit of these approaches is in the range of one in ten thousand cells (10−4).5,6 Potentially more sensitive detection of MRD can be achieved by real-time polymerase chain reaction (PCR) analysis of leukemia-specific fusion gene transcripts, but such markers are available only in a limited proportion of ALL patients.7
In patients undergoing allogeneic HSCT for treatment of various types of leukemia, persistence or recurrence of autologous cells detectable in either whole peripheral blood (PB) samples or within specific leukocyte subsets expected to harbor the malignant cells, if present, was shown to be indicative of imminent disease relapse.8,9 The identification of recipient-derived cells in whole PB specimens is hampered by the limited sensitivity offered by the most common approaches to chimerism analysis based on PCR amplification of microsatellite/short tandem repeat markers.10 These techniques are highly variable among different centers, and usually do not permit detection of recipient cells below the level of 10−2, thus lacking the sensitivity required for the assessment of residual leukemia.11 We and others have shown that it is readily possible to isolate individual leukocyte subsets by immunophenotype-based flow sorting, even if they account for as little as 1% of the total white blood cell count.12 The performance of chimerism analysis within specifically enriched leukocyte populations also has a detection limit in the range of 10−2, thereby permitting the identification of autologous cells in PB with an overall sensitivity of up to 10−4.10 Lineage-specific analysis of chimerism therefore offers a limit of detection for autologous and potentially leukemic cells in the range of sensitivity achievable by the commonly used methods for monitoring MRD. We have recently demonstrated that the assessment of lineage-specific chimerism within the first weeks after allogeneic HSCT facilitates prediction of the risk of graft rejection in transplant recipients, including children with ALL.13 In the present prospective multicenter study performed in a large cohort of pediatric patients with high-risk ALL over a period of 10 years, we have addressed the possibility of exploiting lineage-specific monitoring of chimerism for timely assessment of the risk of relapse after allogeneic HSCT. The study was performed in a blinded fashion to prevent the lineage-specific chimerism test results from having any influence on clinical decisions.
Methods
Patients
The present study was an ancillary research project of the international multicenter ALL-SCT-BFM 2003 trial,14 and was performed with the approval of the local institutional review board at each participating site in accordance with the Declaration of Helsinki. Patients and/or their legal guardians provided written informed consent before enrollment. During the recruitment period between September 2003 and December 2008, a total of 162 high-risk ALL patients with a median age of 10.5 years (range, 0.6–23.1) who underwent allogeneic HSCT at 16 pre-selected centers were included in our study. The indication for allogeneic HSCT was established according to the risk-adapted stratification criteria of the BFM Study Group,15–17 and included children in first, second or subsequent complete morphological remission of ALL. Of 41 documented relapses in the entire cohort of patients studied, 28 occurred only in the bone marrow, eight were extramedullary, and five combined. Among these, six relapses were observed in patients with T-ALL, including three extramedullary and three bone marrow relapses, while the majority of bone marrow, extramedullary and combined relapses occurred in patients with B-cell precursor ALL. The blast cells in all relapses occurring in patients with B-cell precursor ALL displayed the CD19+/CD34+ marker profile.
Sample collection and handling
PB specimens (≥3 mL EDTA-PB) were investigated at predefined time points including weekly intervals between days +7 and +49, followed by 2-week intervals until day +100, and four additional time points on days +120, +150, +180 and +360, whenever possible. Eight or more consecutive PB specimens were available for chimerism analysis in the majority of transplant recipients studied, with a mean of 8.6 samples per patient (median 8; range, 2–20).
Isolation of specific leukocyte subsets by flow-sorting
The post-transplant PB samples were analyzed by four-color quantitative fluorescence activated cell sorting (FACS) on a FACSCalibur (BD Biosciences) as described elsewhere.18 All cell types forming ≥1% of nucleated cells were targets for cell sorting. Routinely sorted cells comprised CD33+ monocytes, CD15+ granulocytes, CD3+/CD4+ helper T cells, CD3+/CD8+ cytotoxic T cells, CD19+/CD34− mature B cells, CD3−/CD56+ natural killer cells and CD34+ early hematopoietic progenitor cells (also including CD34+/CD19+ cells). The targeted number of cells sorted for subsequent analysis of chimerism19,20 was 4 000 per cell population, and ranged between 1 000 and 15 000. The purity of the sorted leukocyte fractions was >98%.
Analysis of donor/recipient chimerism and minimal residual disease
DNA was extracted from nucleated cells using the QIAamp Blood kit (Qiagen, Hilden, Germany). Chimerism was evaluated using the EuroChimerism approach, an internationally validated assay for quantitative analysis of donor and recipient cells after transplantation.11 Data from PCR-based MRD analysis21 were available at similar time points to chimerism testing in ten patients, thereby permitting a limited direct comparison between the methodological approaches.
Definitions
Complete donor chimerism (DC) was defined as the exclusive presence of donor-derived cells, as determined by PCR analysis of an informative microsatellite (short tandem repeat) marker in the specimen investigated. Mixed chimerism (MC) was defined as the presence of both donor and recipient cells at any ratio in the sample tested. ALL relapse following allogeneic HSCT was defined as the presence of ≥5% blasts in representative bone marrow smears.
Statistics
The analysis was performed using the Statistical Analysis System (SAS Institute, Cary, NC, USA). Since mortality not attributable to relapse was low (9%) in the cohort of patients investigated, the statistical analysis was restricted to the assessment of chimerism data with regard to relapse occurrence. Cumulative incidences of relapse were estimated considering the competing risk of death. Starting from the time of transplantation, the proportional cause-specific hazard model with time-dependent co-variates considering the time points of first achievement of DC, and first recurrence of MC after a period of DC, was used to determine the correlation of lineage-specific chimerism with relapse. The hazard ratios (HR) for patients with recurrent MC in comparison to patients who achieved persistent DC are indicated with 95% confidence intervals (CI). The comparison of patients who had recurrent MC with those who had persistent DC was restricted to individuals who had achieved DC during the post-transplant course, and the first observation of DC was the time of entry into the risk evaluation set. In patients with reappearance of MC after previous documentation of DC, the cumulative incidence of relapse was estimated from the time of MC recurrence as the starting point. Cumulative incidences of the residual relapse risk in patients who achieved DC were estimated for illustrative and exploratory purposes by censoring patients who subsequently switched to MC. The interval for this evaluation started at the median time to MC recurrence, and only patients who had reached DC at this time point were included. The correlation of recurring MC in the CD34+ and CD8+ cell fractions with ensuing relapse was assessed by multivariate analysis including other known risk factors such as the remission status before transplantation and the type of donor (Table 3). All indicated P-values are two-sided, and P-values ≤0.05 are considered statistically significant.
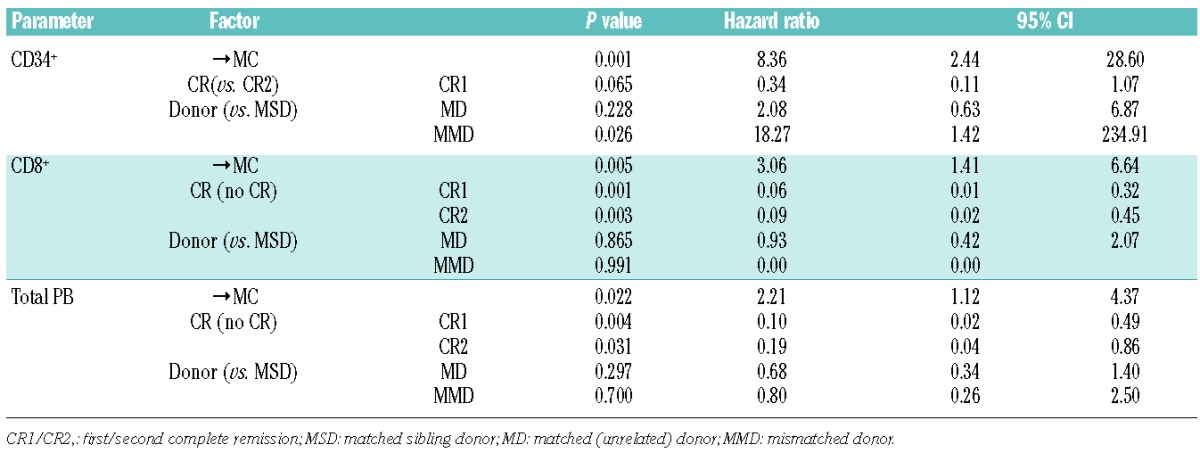
Table 3.
Multivariate analysis of risk factors for relapse after allogeneic HCST. In addition to the reappearance of mixed chimerism (MC) in the leukocyte subsets CD34+, CD8+ and total peripheral blood (indicated as →MC in the Table), the influence of additional factors including the remission status before HSCT and the type of donor, which indicated a correlation with relapse risk in univariate analysis, were subjected to multivariate analysis. While the donor type had no influence on the relapse risk in this setting, the achievement of first or second complete remission prior to HSCT was significantly correlated with a decreased risk of relapse. Immunophenotype was not associated with higher relapse hazards and the results remained essentially unchanged when immunophenotype was added to the model. Reappearing MC in the indicated cell populations remained an independent risk factor for ensuing leukemia relapse even after adjustment for all other variables tested. The 95% confidence intervals (95%CI) of the calculated hazard ratios are indicated.
Results
In the present study, lineage-specific and overall chimerism were monitored at defined time points at a single reference center during the first year after allogeneic HSCT in 162 children with high-risk ALL. The patients’ characteristics are shown in Table 1. The risk of relapse was assessed in relation to the presence and dynamics of chimerism in whole blood and within individual leukocyte subsets. The 5-year cumulative incidence of relapse in the cohort of patients presented was 26%, and the correlation of relapse occurrence with overall and lineage-specific chimerism was evaluated in patients who achieved persistent DC, in comparison with those who had continuous MC or reappearance of autologous cells after a phase of DC (Table 2). Significant associations with relapse were observed for recurrence of MC at any level in the CD34+ and CD8+ compartments, and to a lesser extent in whole PB, in patients with a preceding period of DC in the indicated cell compartments (Figure 1). The detection of reappearing autologous cells in one or more consecutive specimens within the CD34+ and CD8+ cell compartments enriched from PB revealed markedly elevated hazard ratios for ensuing disease relapse of 5.2 (P=0.003) and 2.8 (P=0.008), respectively (Table 2). Recurrence of MC detectable in whole PB specimens was also associated with an elevated risk of relapse (HR 2.1), albeit with lower statistical significance (P=0.024) (Table 2). No significant correlations were found for the remaining leukocyte lineages investigated. The cumulative incidence of relapse for patients with documented reappearance of MC in the CD34+ cell fraction was 67% (±16). The switch from DC to MC in this compartment occurred a mean time of 6 months after transplantation when the intervals of investigation were rather large, and the time span between detection of MC and hematologic relapse was less than 1 month in most instances (Figure 1). Since a proportion of relapses occurred already during the first weeks and months after transplantation, the time-dependent residual relapse risk in the subset of patients with detectable CD34+ cells in PB and the presence of DC within this cell fraction at 6 months after transplantation was 31% (±10). By contrast, in patients in whom CD34+ cells in PB were undetectable by FACS analysis or insufficiently abundant for isolation by flow sorting (usually <1% of total leukocytes), the cumulative incidence of relapse was 8% (±3). Hence, the presence of circulating CD34+ cells in PB at levels readily amenable to isolation by flow sorting (≥1% of total leukocytes) also correlated with an elevated risk of relapse (HR 4.3, P<0.001, 95% CI 2.116–8.735), irrespectively of the chimerism status within this cell fraction. The median time span between first detection of circulating CD34+ cells in PB after transplantation and onset of relapse was 183 days (lower quartile: 75 days, upper quartile: 315 days).
Table 1.
Patients’ baseline characteristics.
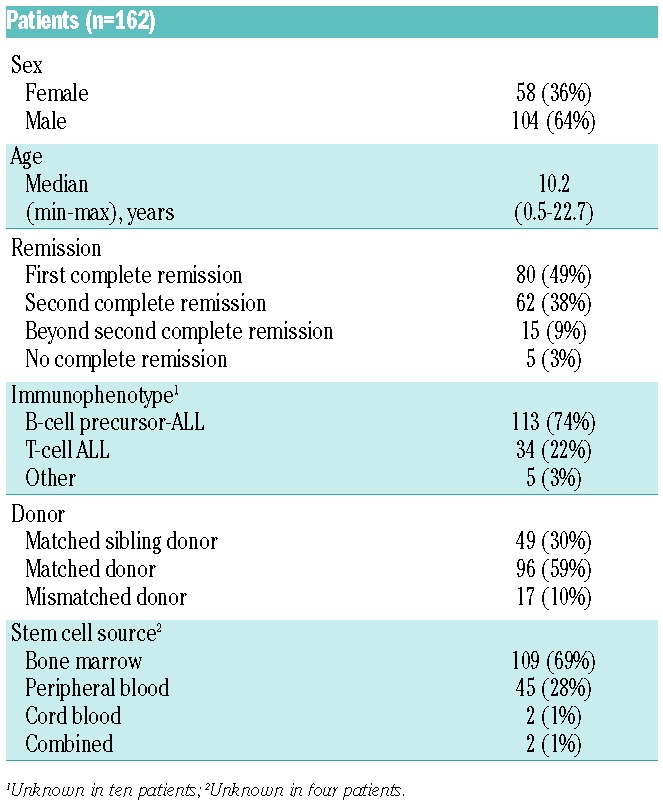
Table 2.
Post-transplant evolution of chimerism in whole blood and selected cell lineages. Within the entire cohort of 162 pediatric patients with ALL undergoing rescue therapy by allogeneic HSCT, chimerism was successfully analyzed within total leukocytes from peripheral blood (total PB), and specific cell fractions isolated by flow sorting from PB in the indicated number of instances. Enrichment of CD34+ cells from PB by flow sorting was achievable in 91/162 patients, but the cell numbers were sufficient for subsequent analysis of chimerism in 62 cases only. The leukocyte lineages statistically correlating in univariate analysis with the risk of relapse, including the CD8+ and the CD34+ cell subsets, are displayed, and the respective numbers of patients who reached complete donor chimerism (DC) or switched to MC after previous documentation of DC (DC→MC) are indicated. The 5-year cumulative risk of relapse (CIR) and the hazard ratios (HR) derived from a Cox-regression analysis with time-dependent covariates are indicated with the corresponding 95% confidence intervals (CI). The CD19+/CD34− cell lineage in which the presence of MC correlated with decreased CIR (statistically not significant) is shown for comparison.
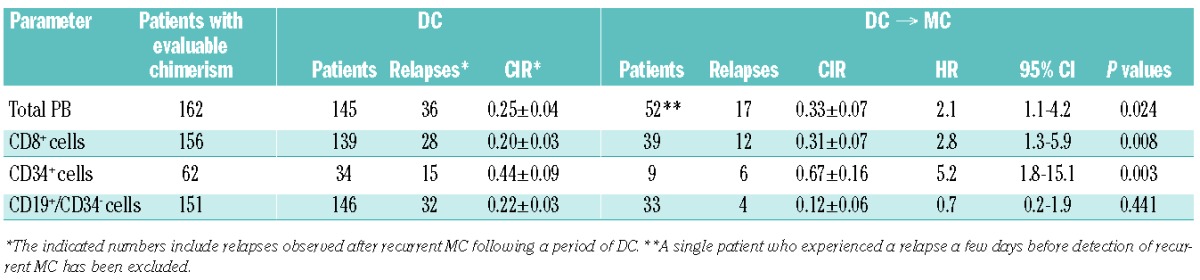
Figure 1.
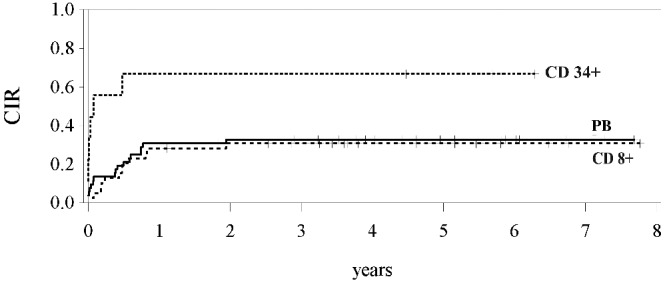
Cumulative risk of relapse (CIR) in relation to post-transplant chimerism. In patients showing recurrence of MC within specific cell fractions including CD34+ and CD8+ cells or within total leukocytes isolated from peripheral blood (PB), a significantly increased risk of relapse was observed, with hazard ratios (HR) and CIR values specified in Table 2. The median time between recurrence of MC and relapse was different for the cell subsets analyzed: 5 months for CD8+ and total PB, and less than 1 month for CD34+ cells.
Monitoring by flow cytometry revealed the presence of CD34+ cells in PB amenable to sorting and molecular testing in a limited proportion of patients (Table 2), while successful chimerism analysis within total leukocyte populations was possible in virtually all specimens tested. Given the commonly observed delayed reconstitution of T-lymphocytes, CD8+ cells could not be readily isolated for chimerism testing during the first weeks after transplantation. However, from 6 to 7 weeks after HSCT onward, chimerism analysis within the CD8+ cell subset was possible in ≥80% of all cases with available PB specimens. Among the children who had a recurrence of MC either in the CD8+ cell compartment or within whole PB, the cumulative incidence of relapse was 33% (±7). The switch from DC to MC in whole PB and within the CD8+ cell lineage was detected a median period of 3 months after allografting, at stages when the time-dependent residual relapse risk was 18% (±4) and 15%(±4), respectively. The median time to relapse after detection of recurrent MC in whole PB or CD8+ cells was 5 months (range, 0.5–24 months), as displayed in Figure 1. Rising levels of autologous cells were identified by quantitative monitoring of MC in a proportion of patients who subsequently progressed to overt relapse, but the observation of expanding recipient cells did not further increase the statistical significance of risk assessment for ensuing relapse when compared to the recurrence of MC at any level. In contrast to reappearance of MC after a period of DC, the constant presence and persistence of MC did not indicate a significantly increased risk of relapse, irrespectively of the cell populations affected (CD34+: HR 1.3, P=0.504; CD8+: HR 1.9, P=0.185; PB: HR 1.2, P=0.697).
The CD19+/CD34− cell compartment was the only leukocyte subset analyzed in which the observation of MC revealed hazard ratios for relapse below 1.0 in all statistical analyses performed (Table 2). Although the indication of decreased risk of relapse (HR 0.7) failed to reach statistical significance (P=0.441), the relapse rate in patients with reappearance or persistence of MC within CD19+/CD34-cells was 12.5% in cases of B-cell precursor ALL, and 0% in cases with T-ALL, as compared to 28% and 11% in patients with DC in this cell compartment.
Discussion
In this prospective, multicenter study, we have investigated the potential role of lineage-specific chimerism analysis for risk assessment of relapse in a large cohort of pediatric patients with high-risk ALL who underwent allogeneic HSCT according to uniform protocols. The significant correlation of recurring MC in the CD34+ and CD8+ cell fractions with ensuing relapse was confirmed by multivariate analysis including other known risk factors such as the remission status before transplantation and the type of donor. The observation that recurrent but not persistent MC was significantly associated with an increased risk of relapse may suggest that reappearing autologous cells mediate or indicate hitherto unknown immune processes facilitating disease recurrence. It is of note that flow cytometry-based detection of CD34+ cells circulating in the PB also indicated a significantly elevated risk of relapse, irrespectively of the chimerism status. One may speculate that increased mobilization of CD34+ cells from the bone marrow could be related to perturbation of the stem cell niche or cytokine-mediated release attributable to leukemic progenitor cells.
The detection of residual or reappearing recipient cells by chimerism analysis in whole PB or within specific cell lineages isolated according to the immunophenotype of the original leukemia may reflect the presence of malignant cells.10 The ability to identify cells belonging to the leukemic clone by chimerism analysis would be particularly useful in transplant settings in which neither disease-specific nor clone-specific markers are available for the detection of minimal residual or recurrent leukemia.12,22 However, in patients with ALL, specific markers permitting sensitive detection of leukemic cells are usually available, and can also be exploited for the monitoring of MRD after allogeneic HSCT.23 The identification of autologous cells in the CD34+ compartment may indicate incomplete myeloablation by the conditioning regimen. Alternatively, it may reflect persistence or recurrence of the malignant clone, but this finding is inherently less specific than surveillance of clone- or disease-specific molecular MRD markers. In the present study, identification of recurrent MC in the CD34+ cell fraction correlated in most instances with available results of MRD analysis based on PCR detection of clone-specific immunoglobulin or T-cell receptor gene rearrangements at levels of ≥10−4. The limited amount of MRD data obtained at time points similar to those of lineage-specific chimerism analyses did not permit systematic comparison of the diagnostic approaches. Nevertheless, in one patient who ultimately progressed to overt relapse, reversion from DC to MC in the CD34+ compartment was observed at a time at which MRD analysis did not provide any evidence of the presence of leukemic cells. This anecdotal observation highlights the potential complementarity of different diagnostic approaches usually yielding similar information.24,25
Although the analysis of chimerism within total leukocyte preparations from PB is not sensitive enough to reveal small numbers of leukemic cells, it was shown that persistence or recurrence of low-level MC may nevertheless correlate with an increased risk of relapse.9 These observations indicate that chimerism testing and MRD analysis assess different aspects contributing to relapse occurrence. The monitoring of chimerism provides insights beyond mere detection of potentially leukemic cells, including particularly immunological processes contributing to graft rejection and relapse which are not amenable to detection by MRD analysis. Findings indicative of impending allograft rejection also herald the loss of the graft-versus-leukemia effect which may be associated with a high risk of disease recurrence. It is also conceivable that additional hitherto incompletely understood immunological interactions occurring between donor and recipient play a role in the ensuing leukemia relapse. The observed correlation between the recurrence of MC at any level within the CD8+ lymphocyte fraction and the risk of relapse, both in patients with T-cell and B-cell precursor leukemia, may serve as evidence supporting this notion. Although most patients with recurrent MC in the CD8+ cell fraction reverted again to DC, the risk of relapse remained elevated, similar to that of patients who retained MC, possibly indicating that the effect mediated by the recurrence of autologous cells within this compartment may not be reversible. Lineage-specific analysis of chimerism provides a sensitive approach to the investigation of such interactions, and the findings presented highlight the potential of this methodology to contribute to early assessment of the risk of relapse. The surveillance of chimerism can yield important information complementary to direct molecular detection of residual leukemia, and could provide a rational basis for timely considerations aiming at the prevention of overt relapse. In addition to close diagnostic monitoring of patients identified as having an increased risk of relapse, the measures could include immunomodulatory treatment to stabilize the graft and to enhance the graft-versus-leukemia effect.
Recurrence of recipient CD34+ cells in PB after transplantation, which could be assessed in a limited proportion (38%) of the patients studied, revealed the highest hazard ratio for ensuing disease relapse in the setting investigated, albeit with a short time to detection of hematologic relapse in most cases. In order to better exploit the informativeness of CD34+ cells for relapse prediction, it would be of interest to investigate bone marrow specimens. The CD34+ cells are present in greater abundance in this compartment and isolation of cell numbers adequate for chimerism analysis is, therefore, easier. Bone marrow aspirations are routinely performed in most centers around days +28 and +100 after transplantation for assessment of hematologic remission and engraftment status. This material could serve as a readily available source for analysis of lineage-specific chimerism in the CD34+ or other cell fractions, and could contribute to improving the predictive value of chimerism testing for impending relapse. Based on the observations presented, prospective evaluation of this concept would be warranted.
The observed association of persistent or reappearing MC in the mature B-cell compartment with decreased risk of relapse is intriguing, despite the fact that this finding did not reach statistical significance. The majority of ALL patients studied had a B-cell precursor phenotype, and it is very unlikely that the autologous CD19+/CD34− cells observed belonged to the leukemic clone. Moreover, the same observation was also made in patients with T-ALL. This observation cannot be readily explained and may, therefore, provide the grounds for a future, appropriately designed study to address this phenomenon.
Lineage-specific monitoring of leukocytes isolated from the PB of patients transplanted for treatment of ALL provides a basis for close diagnostic surveillance in individuals with increased risk of relapse, and for timely therapeutic considerations aiming at the prevention of overt relapse. The observations presented suggest that more frequent analyses of chimerism within the CD34+ compartment could enable earlier identification of patients with a particularly high risk of disease recurrence. Furthermore, the data provide an impetus for future studies addressing the potential benefit of lineage-specific chimerism analyses of bone marrow specimens. These efforts could increase the sensitivity and timeliness of identifying patients at high risk of leukemia relapse and contribute to improved outcomes in ALL patients undergoing allogeneic HSCT.
Acknowledgments
The study was supported by an institutional grant from the Children’s Cancer Research Institute (CCRI).
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/101/6/741
References
- 1.Schrappe M, Hunger SP, Pui CH, et al. Outcomes after induction failure in childhood acute lymphoblastic leukemia. N Engl J Med. 2012;366(15):1371–1381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pui CH, Pei D, Campana D, et al. A revised definition for cure of childhood acute lymphoblastic leukemia. Leukemia. 2014;28(12): 2336–2343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Balduzzi A, Valsecchi MG, Uderzo C, et al. Chemotherapy versus allogeneic transplantation for very-high-risk childhood acute lymphoblastic leukaemia in first complete remission: comparison by genetic randomisation in an international prospective study. Lancet. 2005;366(9486):635–642. [DOI] [PubMed] [Google Scholar]
- 4.Fagioli F, Quarello P, Zecca M, et al. Hematopoietic stem cell transplantation for children with high-risk acute lymphoblastic leukemia in first complete remission: a report from the AIEOP registry. Haematologica. 2013;98(8):1273–1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gandemer V, Pochon C, Oger E, et al. Clinical value of pre-transplant minimal residual disease in childhood lymphoblastic leukaemia: the results of the French minimal residual disease-guided protocol. Br J Haematol. 2014;165(3):392–401. [DOI] [PubMed] [Google Scholar]
- 6.Balduzzi A, Di Maio L, Silvestri D, et al. Minimal residual disease before and after transplantation for childhood acute lymphoblastic leukaemia: is there any room for intervention? Br J Haematol. 2014;164(3): 396–408. [DOI] [PubMed] [Google Scholar]
- 7.Pui CH, Mullighan CG, Evans WE, Relling MV. Pediatric acute lymphoblastic leukemia: where are we going and how do we get there? Blood. 2012;120(6):1165–1174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lion T, Daxberger H, Dubovsky J, et al. Analysis of chimerism within specific leukocyte subsets for detection of residual or recurrent leukemia in pediatric patients after allogeneic stem cell transplantation. Leukemia. 2001;15(2):307–310. [DOI] [PubMed] [Google Scholar]
- 9.Bader P, Kreyenberg H, Hoelle W, et al. Increasing mixed chimerism is an important prognostic factor for unfavorable outcome in children with acute lymphoblastic leukemia after allogeneic stem-cell transplantation: possible role for pre-emptive immunotherapy? J Clin Oncol. 2004;22(9):1696–1705. [DOI] [PubMed] [Google Scholar]
- 10.Preuner S, Lion T. Post-transplant monitoring of chimerism by lineage-specific analysis. Methods Mol Biol. 2014;1109:271–291. [DOI] [PubMed] [Google Scholar]
- 11.Lion T, Watzinger F, Preuner S, et al. The EuroChimerism concept for a standardized approach to chimerism analysis after allogeneic stem cell transplantation. Leukemia. 2012;26(8):1821–1828. [DOI] [PubMed] [Google Scholar]
- 12.Lion T. Detection of impending graft rejection and relapse by lineage-specific chimerism analysis. Methods Mol Med. 2007;134:197–216. [DOI] [PubMed] [Google Scholar]
- 13.Breuer S, Preuner S, Fritsch G, et al. Early recipient chimerism testing in the T- and NK-cell lineages for risk assessment of graft rejection in pediatric patients undergoing allogeneic stem cell transplantation. Leukemia. 2012;26(3):509–519. [DOI] [PubMed] [Google Scholar]
- 14.Peters C, Schrappe M, von Stackelberg A, et al. Stem-Cell Transplantation in children with acute lymphoblastic leukemia: a prospective international multicenter trial comparing sibling donors with matched unrelated donors-the ALL-SCT-BFM-2003 trial. J Clin Oncol. 2015;33(11):1265–1274. [DOI] [PubMed] [Google Scholar]
- 15.Schrauder A, Reiter A, Gadner H, et al. Superiority of allogeneic hematopoietic stem-cell transplantation compared with chemotherapy alone in high-risk childhood T-cell acute lymphoblastic leukemia: results from ALL-BFM 90 and 95. J Clin Oncol. 2006;24(36):5742–5749. [DOI] [PubMed] [Google Scholar]
- 16.Schrauder A, von Stackelberg A, Schrappe M, et al. Allogeneic hematopoietic SCT in children with ALL: current concepts of ongoing prospective SCT trials. Bone Marrow Transplant. 2008;41(Suppl 2):S71–74. [DOI] [PubMed] [Google Scholar]
- 17.von Stackelberg A, Volzke E, Kuhl JS, et al. Outcome of children and adolescents with relapsed acute lymphoblastic leukaemia and non-response to salvage protocol therapy: a retrospective analysis of the ALL-REZ BFM Study Group. Eur J Cancer. 2011;47(1):90–97. [DOI] [PubMed] [Google Scholar]
- 18.Fritsch G, Witt V, Dubovsky J, et al. Flow cytometric monitoring of hematopoietic reconstitution in myeloablated patients following allogeneic transplantation. Cytotherapy. 1999;1(4):295–309. [DOI] [PubMed] [Google Scholar]
- 19.Schraml E, Daxberger H, Watzinger F, Lion T. Quantitative analysis of chimerism after allogeneic stem cell transplantation by PCR amplification of microsatellite markers and capillary electrophoresis with fluorescence detection: the Vienna experience. Leukemia. 2003;17(1):224–227. [DOI] [PubMed] [Google Scholar]
- 20.Schraml E, Lion T. Interference of dye-associated fluorescence signals with quantitative analysis of chimerism by capillary electrophoresis. Leukemia. 2003;17(1):221–223. [DOI] [PubMed] [Google Scholar]
- 21.van der Velden VH, Panzer-Grumayer ER, Cazzaniga G, et al. Optimization of PCR-based minimal residual disease diagnostics for childhood acute lymphoblastic leukemia in a multi-center setting. Leukemia. 2007;21(4):706–713. [DOI] [PubMed] [Google Scholar]
- 22.Lion T. Chimerism testing after allogeneic stem cell transplantation: importance of timing and optimal technique for testing in different clinical-biological situations. Leukemia. 2001;15(2):292. [DOI] [PubMed] [Google Scholar]
- 23.Bruggemann M, Schrauder A, Raff T, et al. Standardized MRD quantification in European ALL trials: proceedings of the Second International Symposium on MRD assessment in Kiel, Germany, 18–20 September 2008. Leukemia. 2010;24(3):521–535. [DOI] [PubMed] [Google Scholar]
- 24.Bader P, Willasch A, Klingebiel T. Monitoring of post-transplant remission of childhood malignancies: is there a standard? Bone Marrow Transplant. 2008;42(Suppl 2):S31–34. [DOI] [PubMed] [Google Scholar]
- 25.Bader P, Kreyenberg H, von Stackelberg A, et al. Monitoring of minimal residual disease after allogeneic stem-cell transplantation in relapsed childhood acute lymphoblastic leukemia allows for the identification of impending relapse: results of the ALL-BFM-SCT 2003 trial. J Clin Oncol. 2015;33(11): 1275–1284. [DOI] [PubMed] [Google Scholar]