

Abstract
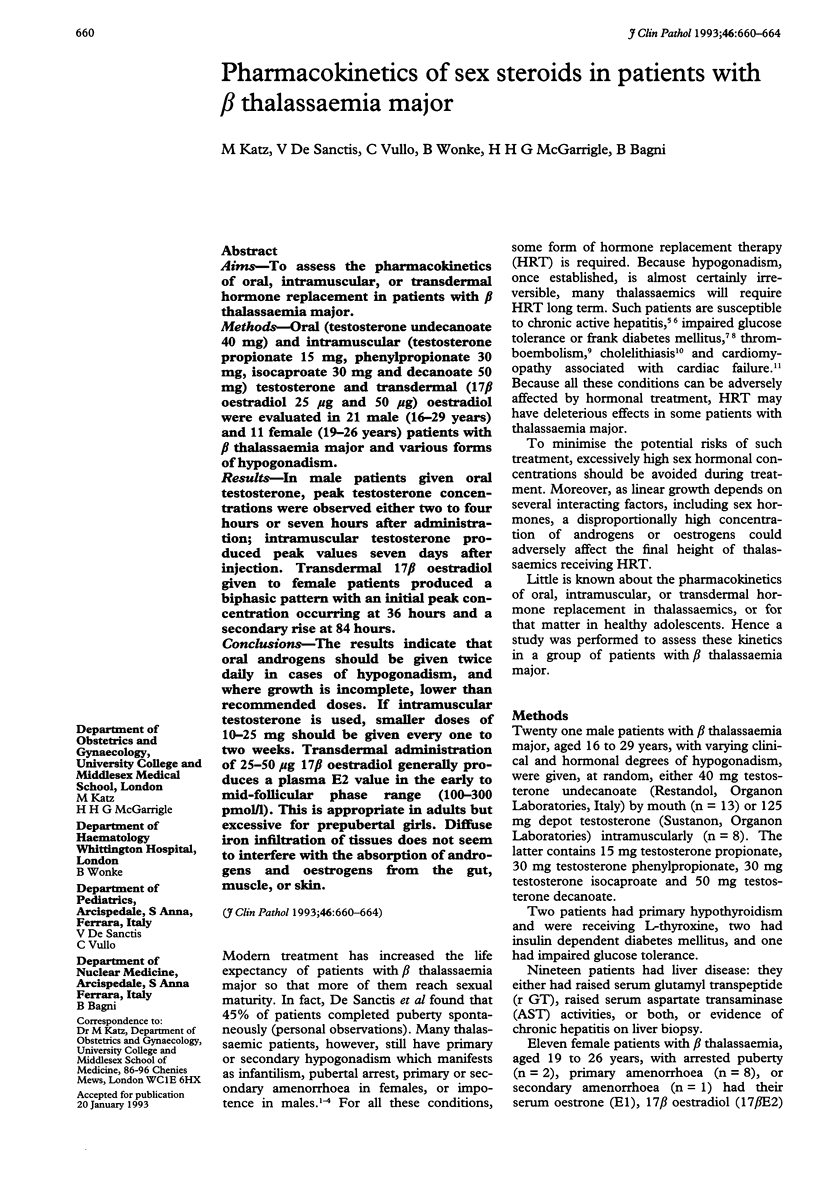
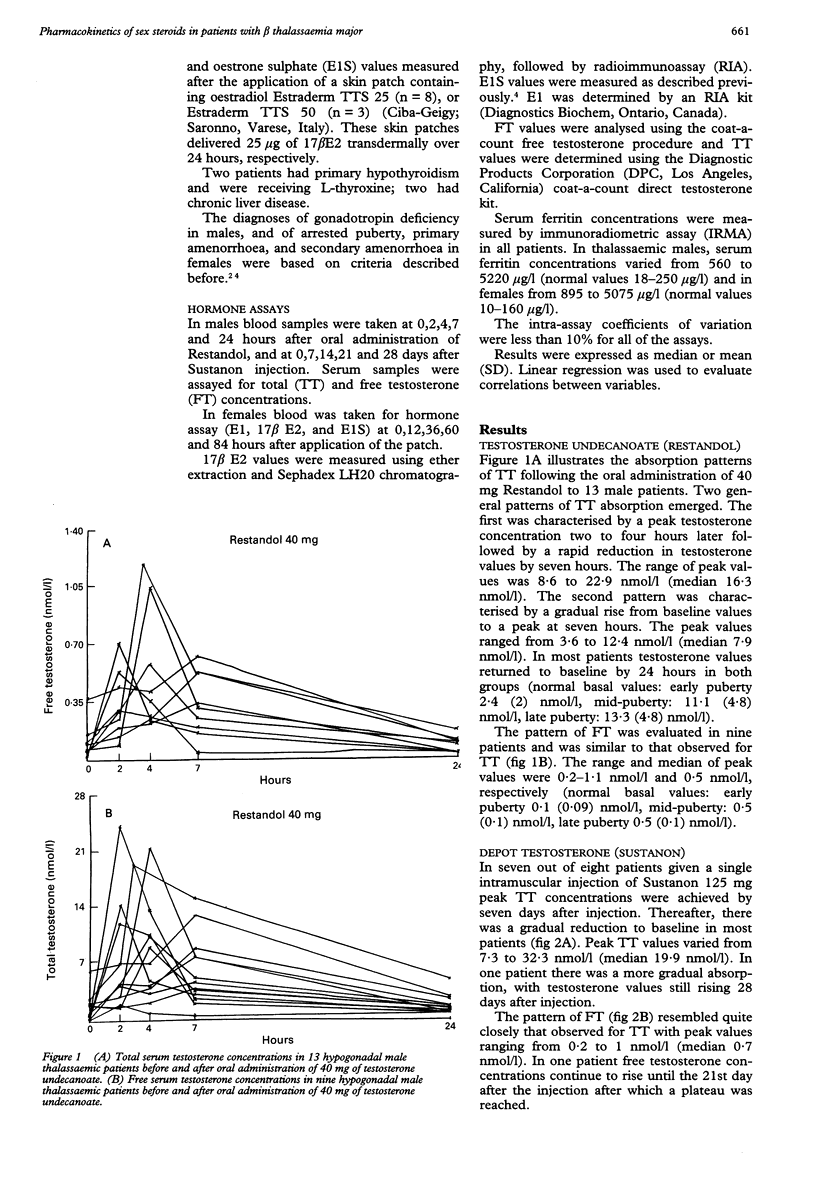
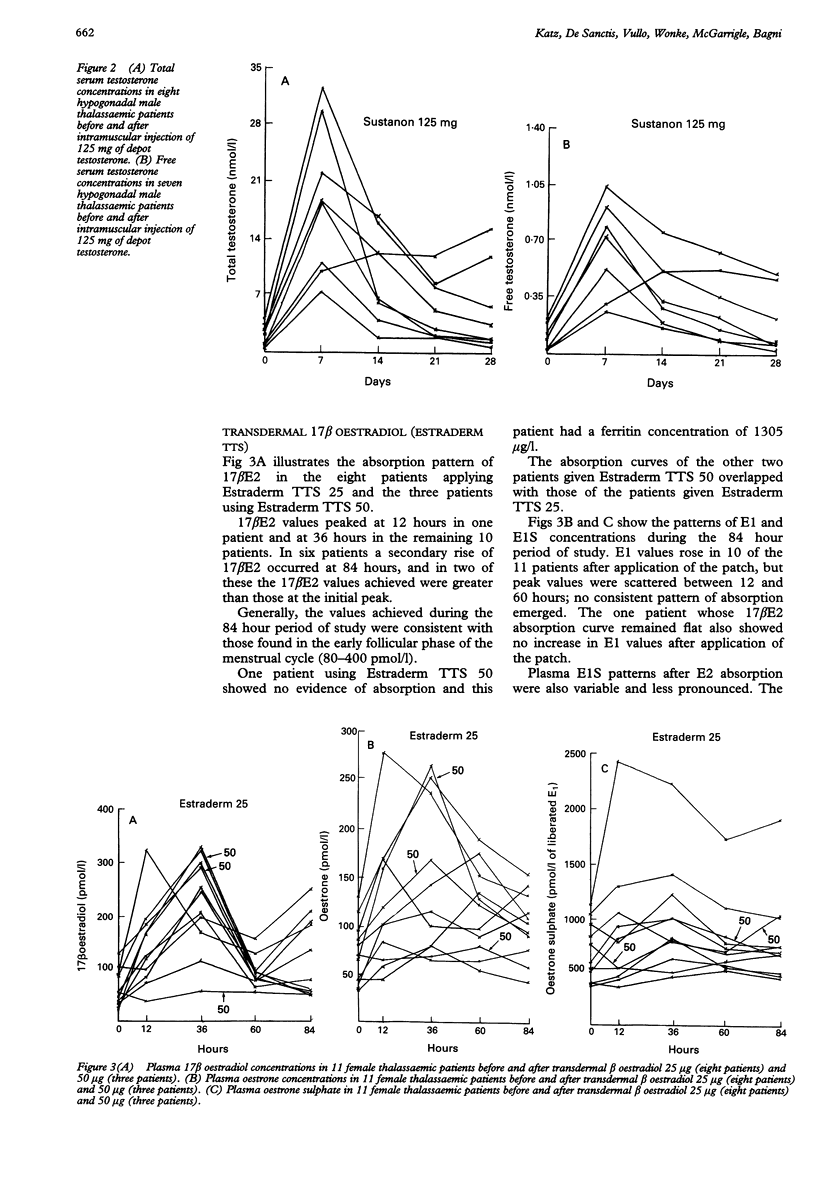
AIMS--To assess the pharmacokinetics of oral, intramuscular, or transdermal hormone replacement in patients with beta thalassaemia major. METHODS--Oral (testosterone undecanoate 40 mg) and intramuscular (testosterone propionate 15 mg, phenylpropionate 30 mg, isocaproate 30 mg and decanoate 50 mg) testosterone and transdermal (17 beta oestradiol 25 micrograms and 50 micrograms) oestradiol were evaluated in 21 male (16-29 years) and 11 female (19-26 years) patients with beta thalassaemia major and various forms of hypogonadism. RESULTS--In male patients given oral testosterone, peak testosterone concentrations were observed either two to four hours or seven hours after administration; intramuscular testosterone produced peak values seven days after injection. Transdermal 17 beta oestradiol given to female patients produced a biphasic pattern with an initial peak concentration occurring at 36 hours and a secondary rise at 84 hours. CONCLUSIONS--The results indicate that oral androgens should be given twice daily in cases of hypogonadism, and where growth is incomplete, lower than recommended doses. If intramuscular testosterone is used, smaller doses of 10-25 mg should be given every one to two weeks. Transdermal administration of 25-50 micrograms 17 beta oestradiol generally produces a plasma E2 value in the early to mid-follicular phase range (100-300 pmol/l). This is appropriate in adults but excessive for prepubertal girls. Diffuse iron infiltration of tissues does not seem to interfere with the absorption of androgens and oestrogens from the gut, muscle, or skin.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aldouri M. A., Wonke B., Hoffbrand A. V., Flynn D. M., Laulicht M., Fenton L. A., Scheuer P. J., Kibbler C. C., Allwood C. A., Brown D. Iron state and hepatic disease in patients with thalassaemia major, treated with long term subcutaneous desferrioxamine. J Clin Pathol. 1987 Nov;40(11):1353–1359. doi: 10.1136/jcp.40.11.1353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barry M., Flynn D. M., Letsky E. A., Risdon R. A. Long-term chelation therapy in thalassaemia major: effect on liver iron concentration, liver histology, and clinical progress. Br Med J. 1974 Apr 6;2(5909):16–20. doi: 10.1136/bmj.2.5909.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borgna-Pignatti C., De Stefano P., Zonta L., Vullo C., De Sanctis V., Melevendi C., Naselli A., Masera G., Terzoli S., Gabutti V. Growth and sexual maturation in thalassemia major. J Pediatr. 1985 Jan;106(1):150–155. doi: 10.1016/s0022-3476(85)80488-1. [DOI] [PubMed] [Google Scholar]
- Costin G., Kogut M. D., Hyman C. B., Ortega J. A. Endocrine abnormalities in thalassemia major. Am J Dis Child. 1979 May;133(5):497–502. doi: 10.1001/archpedi.1979.02130050041009. [DOI] [PubMed] [Google Scholar]
- Dandona P., Hussain M. A., Varghese Z., Politis D., Flynn D. M., Hoffbrand A. V. Insulin resistance and iron overload. Ann Clin Biochem. 1983 Mar;20(Pt 2):77–79. doi: 10.1177/000456328302000203. [DOI] [PubMed] [Google Scholar]
- De Sanctis V., Vullo C., Katz M., Wonke B., Hoffbrand A. V., Bagni B. Hypothalamic-pituitary-gonadal axis in thalassemic patients with secondary amenorrhea. Obstet Gynecol. 1988 Oct;72(4):643–647. [PubMed] [Google Scholar]
- De Sanctis V., Vullo C., Katz M., Wonke B., Nannetti C., Bagni B. Induction of spermatogenesis in thalassaemia. Fertil Steril. 1988 Dec;50(6):969–975. doi: 10.1016/s0015-0282(16)60382-5. [DOI] [PubMed] [Google Scholar]
- De Sanctis V., Zurlo M. G., Senesi E., Boffa C., Cavallo L., Di Gregorio F. Insulin dependent diabetes in thalassaemia. Arch Dis Child. 1988 Jan;63(1):58–62. doi: 10.1136/adc.63.1.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geere G., Jones J., Atherden S. M., Grant D. B. Plasma androgens after a single oral dose of testosterone undecanoate. Arch Dis Child. 1980 Mar;55(3):218–220. doi: 10.1136/adc.55.3.218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldfarb A., Grisaru D., Gimmon Z., Okon E., Lebensart P., Rachmilewitz E. A. High incidence of cholelithiasis in older patients with homozygous beta-thalassemia. Acta Haematol. 1990;83(3):120–122. doi: 10.1159/000205186. [DOI] [PubMed] [Google Scholar]
- Grisaru D., Goldfarb A. W., Gotsman M. S., Rachmilewitz E. A., Hasin Y. Deferoxamine improves left ventricular function in beta-thalassemia. Arch Intern Med. 1986 Dec;146(12):2344–2349. [PubMed] [Google Scholar]
- Illig R., DeCampo C., Lang-Muritano M. R., Prader A., Torresani T., Werder E. A., Willi U., Schenkel L. A physiological mode of puberty induction in hypogonadal girls by low dose transdermal 17 beta-oestradiol. Eur J Pediatr. 1990 Dec;150(2):86–91. doi: 10.1007/BF02072044. [DOI] [PubMed] [Google Scholar]
- Johnson P. J. Sex hormones and the liver. Clin Sci (Lond) 1984 Apr;66(4):369–376. doi: 10.1042/cs0660369. [DOI] [PubMed] [Google Scholar]
- Long R. G. Endocrine aspects of liver disease. Br Med J. 1980 Jan 26;280(6209):225–228. doi: 10.1136/bmj.280.6209.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonakul D., Pacharee P., Laohapand T., Fucharoen S., Wasi P. Pulmonary artery obstruction in thalassaemia. Southeast Asian J Trop Med Public Health. 1980 Dec;11(4):516–523. [PubMed] [Google Scholar]