

Abstract
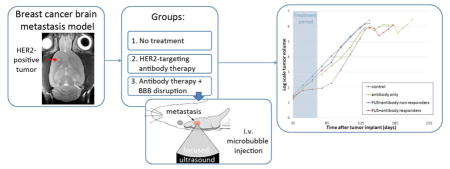
HER2-targeting antibodies (i.e. trastuzumab and pertuzumab) prolong survival in HER2-positive breast cancer patients with extracranial metastases. However, the response of brain metastases to these drugs is poor, and it is hypothesized that the blood-brain barrier (BBB) limits drug delivery to the brain. We investigated whether we could improve the response by temporary disruption of the BBB using focused ultrasound in combination with microbubbles. To study this, we inoculated 30 nude rats with HER2-positive cells derived from a brain metastasis of a breast cancer patient (MDA-MB-361). The animals were divided into three groups: a control-group that received no treatment; an antibody-only group that received six weekly treatments of trastuzumab and pertuzumab; and an ultrasound+antibody group that received trastuzumab and pertuzumab in combination with six weekly sessions of BBB disruption using focused ultrasound. In two animals, the leakiness of the tumors before disruption was evaluated using contrast-enhanced T1-weighted magnetic resonance imaging and found that the tumors were not leaky. The same technique was used to evaluate the effectiveness of BBB disruption, which was successful in all sessions.
The tumor in the control animals grew exponentially with a growth constant of 0.042±0.011 mm3/day. None of the antibody-only animals responded to the treatment and the growth constant was 0.033±0.009 mm3/day during the treatment period. Four of the ten animals in the ultrasound+antibody-group showed a response to the treatment with an average growth constant of 0.010±0.007 mm3/day, compared to a growth constant 0.043±0.013 mm3/day for the six non-responders. After the treatment period, the tumors in all groups grew at similar rates. As the tumors were not leaky before BBB disruption and there were no responders in the antibody-only group, these results show that at least in some cases disruption of the BBB is necessary for a response to the antibodies in these brain metastases. Interestingly, only some of the rats responded to the treatment. We did not observe a difference in tumor volume at the start of the treatment, nor in HER2 expression or in contrast-enhancement on MRI between the responders and non-responders to explain this. Better understanding of why certain animals respond is needed and will help in translating this technique to the clinic. In conclusion, we demonstrate that BBB disruption using focused ultrasound in combination with antibody therapy can inhibit growth of breast cancer brain metastasis.
Keywords: Blood-brain barrier, Focused Ultrasound, Brain metastasis, HER2-Targeting antibodies, Targeted drug delivery
Graphical abstract
Introduction
Of the patients with breast cancer, 5–15% develop metastases in the central nervous system (Leyland-Jones 2009). The prognosis for patients with metastases in the brain is poor: for patients with multiple metastases the one-year survival rate is around 25% (Harputluoglu et al. 2008), and neurologic disease is the cause of death, or a major factor, in 68% of these patients (Boogerd et al. 1993). The incidence of brain metastases seems to be higher in patients that overexpress human epidermal growth factor receptor 2 (HER2) and who have been treated with trastuzumab (Yau et al. 2006). This HER2-targeting antibody is effective in extracranial metastases and prolongs survival, which might be the reason for the higher incidence of brain metastases (Pieokowski and Zielinski 2009). It is hypothesized that the blood-brain barrier (BBB), or the blood-tumor barrier (BTB), is the reason for the poor response of brain metastases to drugs that are effective extra-cranially, such as trastuzumab. Most small molecule and essentially all large molecule drugs are prevented from reaching the brain parenchyma due to this barrier (Pardridge 2007). Although blood vessels in brain metastases are somewhat leaky, this permeability is heterogeneous and mice studies have shown that the delivery of chemotherapeutics in breast cancer brain metastases stays below therapeutic levels in the vast majority of the brain metastases (Lockman et al. 2010).
Focused ultrasound (FUS) in combination with microbubbles, small gas bubbles used as ultrasound contrast agents, has been shown to enable temporarily and focal disruption of the BBB (Hynynen et al. 2001). Preclinical studies have shown that the interaction between acoustic pressure waves and microbubbles leads to temporary disassembly of the tight junction proteins, making drug delivery past the BBB possible (Sheikov et al. 2008; Sheikov et al. 2006; Shang et al. 2011). The advantage of this technique is that it is non-invasive, repeatable, and targets only specific regions of the brain and is compatible with approved drugs. Two approved therapeutic agents that are effective for HER2-positive breast cancer and extracranial metastases are trastuzumab and pertuzumab, which are monoclonal HER2-recepter targeting antibody therapies. For these drugs to be effective in brain metastases, they will need to pass the BBB/BTB. Previously, it has been demonstrated that the delivery of trastuzumab to the mouse brain can be enhanced by BBB disruption using FUS in combination with microbubbles (Kinoshita et al. 2006). Furthermore, in an animal study using nude rats that were injected with human breast cancer cells (BT-474), it was demonstrated that median survival time increased by at least 32% in animals that received trastuzumab in combination with ultrasound-mediated disruption of the BBB compared to animals that were not treated (Park et al. 2012). In four of ten animals treated with FUS and trastuzumab, the tumor appeared to be completely resolved in the follow-up MRI. However, in that study a cell line was used that was derived from a primary breast tumor that is highly sensitive to trastuzumab (Park et al. 2012). Therefore, it might not be the most appropriate model for translational studies. Here we evaluate the treatment effect of FUS-induced BBB disruption using a HER2-overexpressing human cancer cell line that has been derived from a brain metastasis of a breast cancer patient. Similar to the clinic, we use trastuzumab in combination with pertuzumab and we kept all animals alive until they met the criteria for euthanasia in order to perform a complete survival analysis.
Materials and methods
Study design
In this prospective study the treatment benefit of trastuzumab and pertuzumab in combination with FUS-mediated BBB disruption was determined in a breast cancer brain metastasis model. The experiments were approved by the Harvard Medical Area Standing Committee on Animals. The brain metastasis model was obtained by implanting MDA-MB-361 HER2-positive human cancer cells in the right brain hemisphere of nude rats. The animals were divided in three treatment groups of 10 animals each: group 1 received no treatment; group 2 received trastuzumab and pertuzumab treatment; and group 3 received trastuzumab and pertuzumab in combination with FUS-mediated BBB disruption. Previous studies have demonstrated that FUS-mediated disruption of the blood-brain barrier without administration of the drugs has no therapeutic effect on different brain tumor models (Chen et al. 2010; Park et al. 2012; Aryal et al. 2013; Treat et al. 2012). For that reason, we did not include an arm with FUS mediated BBB-disruption-only. The weekly treatments started five weeks after tumor implantation, when the maximum tumor diameter was around 2 mm, and lasted six weeks. Comparable to the clinical protocol, trastuzumab and pertuzumab (provided by Genentech, South San Francisco, CA) were administered intravenously at a dose of 4 mg/kg (loading dose) in the first treatment week and 2 mg/kg during the following weeks (maintenance dose). Every other week, the tumor size was monitored with high-resolution MR-imaging. The animals were euthanized if the tumor diameter exceeded 13 mm, the animal showed excessive weight loss, or if there were signs of suffering or poor condition. Figure 1 shows the time-line of the experiments. Cell growth assays were performed to compare the response of the MDA-MB-361 and BT-474 cell lines to trastuzumab and pertuzumab therapy.
Figure 1.

Study design.
Cell growth assays
The HER2-positive human cancer cells BT-474 and MDA-MB-361 were obtained from ATCC (Manassas, VA). Variants of these cell lines transfected with the GFP-labeled histone H2B (MDA-MB-361-H2B-GFP and BT-474-H2B-GFP) were used to evaluate drug-induced growth inhibition over time using a laser scanning cytometer (TTP Labtech, Cambridge, MA). Cells were cultured in RPMI 1640 medium containing 10% fetal bovine serum at 37 °C in 5% CO2. Forty-eight hours before adding the HER2 targeting antibodies, 5·103 tumor cells/well were seeded in 96-well plates. Trastuzumab, pertuzumab or both antibodies were added to the wells at concentrations of 0, 7.47, 22.22, 66.67 or 200 μg/ml, that were selected to match the maximum concentration measured in patients (Leyland-Jones 2009). To measure cell growth in the presence of each drug and their combination we measured cell numbers at day 0, day 3 and day 6 for the MDA-MB-361-H2B-GFP and BT-474-H2B-GFP cells. Specifically, we quantified the total area of nuclei (Anuclei) at each time point, and next calculated normalized cell growth by dividing Anuclei(day x) by Anuclei(day 0). These experiments were executed in duplicates and used to determine which duration of antibody therapy was necessary to observe treatment effects. Based on these studies, we decided to treat MDA-MB-361 and BT-474 cells for six days. At day 6, the cells were fixed with 4% paraformaldehyde (Sigma-Aldrich, St. Louis, MO, USA) and Hoechst and Propidium Iodide (PI, Sigma Adrich) were added to stain cell nuclei and dead cell, respectively. To estimate the number of viable cells (total cells – dead cells) we computed the differences between the area of all cells (Anuclei) from the Hoechst stain and the area of dead cells (Adead) from the PI stain. Using this method we determined growth inhibition due to HER2-targeting antibodies for each well as follows:
where Acontrol is the average area of viable cells in the wells that did not receive treatment. These experiments were performed in six replicates and for each concentration and drug combination the average growth inhibition was determined. The Spearman’s rank correlation coefficient between the concentration and inhibition was determined. The differences between the growth inhibition at each concentration of the different treatments were evaluated using one-way ANOVA with a Tukey’s post-test.
Cell culture and tumor implantation
MDA-MB-361 cells were cultured in Leibovitz’s L-15 Medium (ATCC) with 20% fetal bovine serum and 5% penicillin streptomycin at 37 °C without additional CO2. For tumor implantations, cells were suspended in cell culture medium at 1·106 cells per 2 μl medium. Thirty male nude rats (Charles River Laboratories, Boston, MA) were included in the study. One week before tumor implantation, a 17β-estradiol pellet (1.7 mg estrogen/pellet, Innovative Research of America, Sarasota, FL) was implanted subcutaneously using 2% isoflurane as anesthetic. As the pellet releases estrogen for 90 days, this procedure was repeated every 90 days. For tumor implantation, the animals were anesthetized with a mix of 80 mg/kg ketamine (Aveco Co., Inc., Fort Dodge, IA) and 10 mg/kg of xylazine (Lloyd Laboratories, Shenandoah, IA) via intraperitoneal injection. A 1-mm-diameter hole was drilled 2 mm anterior to the bregma and 2 mm to the right of sagittal suture. A 10 μl Hamilton syringe with a 27 G needle was used to inject 4 μl of the cell suspension into the right frontal lobe at a depth of 3.5 mm relative to the skull surface. During 5 minutes, the cells were injected with an infusion pump (Harvard Apparatus, Holliston, MA) positioned in a stereotactic positioner. After a 5-minute wait, the needle was slowly withdrawn from the brain. The burr hole was closed with sterile bone wax and the skin sutured. Lastly, 2.5 mg/kg antibiotic (Baytril®, Bayer Healthcare, Shawnee Mission, KS) and 0.05 mg/kg analgesic (Buprenex®, Reckitt Benckiser Pharmaceuticals, Richmond, VA) were administered.
MR-guided ultrasound procedures
Setup
An MR-compatible single-element, spherically-focused transducer (diameter 4.0 cm, radius of curvature 3.5 cm, frequency 690 kHz) was mounted to a three-axis positioning system. The focal region of the transducer had a half-maximum pressure amplitude width of 3 mm and length of 18 mm. The transducer was placed in a tank with degassed water and connected to a matching circuit. The matching circuit was connected to an RF amplifier (Model 240L, ENI Inc., Rochester, NY) and arbitrary waveform generator (33220A, Agilent, Santa Clara, CA). The electrical power was monitored with a power meter (Model E4419B, Agilent, Santa Clara, CA) and a dual-directional coupler (Model C594810-C, Werlatone, Patterson, NY). The sonications were performed in a 7T Bruker Biospec animal MR-system (Biospec, Bruker, Billerica, MA). A home-built MR-coil was connected to the scanner interface and tuned and matched after placement of the first rat in the system for that experimental session. The location of the focal point in the MRI coordinate space was found before the rat experiments by observing heating in a silicone ultrasound imaging standoff pad.
Animal preparation
For the sonications, the animals were anesthetized with a mix of 80 mg/kg ketamine and 10 mg/kg of xylazine via intraperitoneal injection. The hair on the head of the sedated animal was removed. After insertion of the catheter into the tail vein, the animal was placed in supine position in the sonication system.
MRI-guidance
The exam started with fast gradient echo images to localize the brain. Next, axial T1-weighted (T1w), T2-weighted (T2w) and T2*-weighted (T2*w) images were obtained before the sonications (parameters in table 1). T1w imaging in combination with a gadolinium-based MRI contrast agent is commonly used to access tumor permeability and to confirm BBB disruption. The intact BBB does not allow the agent to extravasate from the capillaries. Gadolinium shortens the T1 relaxation time of the tissue, thus extravasation leads to a hyper-intense region on post-contrast T1w images, indicating permeability of the brain vasculature. In two animals, every week before the sonications, a bolus of 0.25 ml/kg gadopentetate dimeglumine (Gd-DTPA, molecular weight 938 Da) (Magnevist, Bayer HealthCare Pharmaceuticals Inc., Wayne, NJ, USA) was injected and T1w imaging was repeated to evaluate leakiness of the brain metastasis. After the sonications, T2*w imaging was repeated in all animals. Furthermore, all 10 animals received a bolus of 0.25 ml/kg Gd-DTPA after the sonications and T1w imaging was repeated in the axial and sagittal plane to confirm successful BBB disruption.
Table 1.
MR imaging parameters
| Echo time (ms) | Repetition time (ms) | Slice thickness (mm) | Field of view (mm) | Matrix | Number averages | Sequence | |
|---|---|---|---|---|---|---|---|
| Parameters during MR-guided sonications: | |||||||
| T1w imaging | 18 | 651 | 1 | 35 × 35 | 128 × 128 | 4 | RARE – ETL: 4 |
| T2w imaging | 65 | 3260 | 1 | 35 × 35 | 128 × 128 | 2 | RARE – ETL: 8 |
| T2* w imaging | 15 | 495 | 1 | 35 × 35 | 128 × 128 | 2 | Gradient echo – α= 30 |
| Parameters for high-resolution tumor monitoring: | |||||||
| T2w imaging | 52 | 3500 | 1 | 30 × 25.6 | 300 × 252 | 6 | RARE – ETL: 14 |
RARE = Rapid imaging with refocused echoes, ETL = echo train length.
Sonications
Before the first sonication, trastuzumab and pertuzumab were injected at the desired dose. The ultrasound focal point was related to the MR coordinates, and pre-sonication MR-images were used to obtain tumor coordinates. The complete tumor was treated in 4 to 14 sonications that were separated by 1 to 1.5 mm. Before each sonication 100 μl/kg of the ultrasound contrast agent Optison (GE Healthcare, Milwaukee, WI, USA) was injected, which was diluted 10 times with saline. Immediately after injection of the microbubbles, 10-ms burst sonications were applied (1 Hz repetition frequency, 60s duration). The ultrasound contrast agent was flushed with saline. A delay of two minutes between sonications was used to clear most microbubbles from the vasculature. Acoustic powers between 0.40 and 0.70 W were used, which corresponds to peak negative pressure amplitudes in water between 0.46 and 0.62 MPa.
MRI tumor monitoring
High-resolution T2w images to access tumor volume were obtained every other week on the 7T Bruker MR-scanner using a phased array coil (Bruker) for signal reception (parameters in table 1). The animals were anesthetized with 2% isoflurane for the imaging procedure. When the tumor diameter approached 13 mm, the frequency of imaging was increased to once a week.
Histology
When the study endpoint was reached (tumor size exceeded 13 mm in diameter or the animal showed excessive weight loss, signs of suffering or poor condition), the rat was deeply anesthetized with ketamine and xylazine and euthanized by transcardial perfusion of 100 ml 0.9% NaCl, followed by 250 ml 10% buffered formalin phosphate to fix the brain. From three animals in each group, the brains were embedded in paraffin and serially cut in 5 μm axial sections. Per animal, six sections, 250 μm apart, were stained with hematoxylin and eosin (H&E). Furthermore, with five animals, one section was stained with the antibody for the HER2-receptor.
Data analysis
On the high-resolution T2w images the tumor was manually segmented in 3D Slicer (Fedorov et al. 2012) and the tumor volume was calculated. The growth constant (r) was determined by fitting the tumor volumes to the following formula:
where t is the time in days. The growth rate of each tumor was determined for the treatment period (week 5 to 11), and for the follow-up period (week 11 till sacrifice). An animal was classified as ‘responder’ if r during the treatment period was lower than the mean r of the control animals minus two standard deviations. The tumor volumes of the three groups at week 5, when the treatment started, and the growth rates were compared using ANOVA with a Tukey posthoc test.
Survival curves were made for the three groups and the median survival times were determined. The curves were compared using a log-rank (Mantel-Cox) test and Bonferroni correction was applied to correct for multiple comparisons.
To study the permeability of the tumor before the sonication, a square region of interest (ROI) was drawn on the slice with the largest tumor diameter. The size of the ROI was chosen to fit the tumor and a ROI of the same size was drawn on the contralateral side of the brain. The percentage change in signal intensity on pre- and post-contrast T1w imaging was determined and the difference in change between the tumor and contralateral ROI was determined (ΔSI%). The same analysis to calculate ΔSI% was performed in all 10 rats before and after sonication for to quantify BBB disruption.
Next, a qualitative analysis was performed of the T2*w images. The T2*w images were inspected for the presence of hypo-intensities in the sonicated region. Hypo-intense regions on T2*w images can indicate extravasated erythrocytes, but also hemosiderin, the remains of dead erythrocytes. Therefore, the T2*w images obtained before and after the sonications were compared and classified as exhibiting: 1) no difference between pre- and post sonication T2*w images; 2) minimal differences in hypo-intensity; 3) clearly more hypo-intense region(s) on the post-sonication T2*w image.
Results
Cell growth assays
Analysis of the cell growth response for the fluorescence-expressing MDA-MB-361-H2B-GFP and BT-474-H2B-GFP cells in the presence of drugs as a function of time indicated that significant differences between control and treatment arms were observed at day 6 in vitro (Figure 2A–B). Therefore, we decided to set the experiment duration at 6 days for MDA-MB-361 and BT-474 cell lines whose growth could not be monitored in real time and were used for the in vivo experiments. As none of the treatments (trastuzumab, pertuzumab or the combination) showed a significant correlation between growth inhibition and drug concentration, suggesting that even low drug concentrations can have growth-inhibitory effects, we present the growth-inhibition results for the median antibody concentration of 22.2 ug/ml (similar results were observed for higher concentrations). For the endpoint measurements (six days of drug treatment), pertuzumab treatment resulted in minimal growth inhibition for the BT-474 cells. However, trastuzumab and the combination of both antibodies significantly inhibited growth at similar levels (Figure 2C), suggesting that the addition of pertuzumab to the antibody drug combination is not providing any growth-inhibitory benefit for the BT-474 cells. For the MDA-MB-361 cells, all antibody treatments inhibited growth, compared to the controls, but no differences among the antibody groups were observed (Figure 2D). Furthermore, the inhibition in MDA-MB-361 was less strong than for BT-474 cells. When the BT-474-H2B-GFP cells were treated with trastuzumab, the cell number at day 6 was lower than the number of cells at day 0 (Figure 2A), indicating this therapy can induce cell death that could potentially result in decreased tumor volume in vivo for these cells. This was not the case for MDA-MB-361-H2B-GFP cells, where cell growth stabilized after day 3 for trastuzumab and pertuzumab treatment (Figure 2B).
Figure 2.

(A–B) Growth curves (relative cell number to Day0 at days 3 and 6) for fluorescence expressing BT-474-HB2-GFP (A) and MDA-MB-361-H2B-GFP (B) cells treated with trastuzumab (red), pertuzumab (green) or both antibodies (magenta) at a concentration of 22 μg/ml. Controls received no treatment (blue).
(C–D) Endpoint measurement of growth inhibition relative to cells without treatment for BT-474 cells (C) and MDA-MB-361 (D) after six days of exposure to trastuzumab, pertuzumab or the combination at 22 μg/ml.
Animal studies
Blood-brain barrier disruption
BBB disruption was successful in all sessions with an average ΔSI% of 21.2% (range 4.5 – 77.6%) over all rats and all sessions. There was no difference in average ΔSI% between the rats. The mean ΔSI% and standard deviation of the two tumors before BBB disruption during the six treatment weeks were 0.4±2.3% and 0.6±1.4%, indicating that the tumors were not leaky before disruption (Figure 3). There was no relation of ΔSI% with time in these two animals. In 37% (22/60) of the sessions, a region was present on the post-sonication T2*w images that was clearly more hypo-intense than on the pre-sonication image. In the remaining 63% (38/60) of the sessions, no or only a minimal difference in hypo-intensity was observed. In one animal, a cyst developed after the first treatment (ΔSI=25.7%).
Figure 3.

A) T1w image before contrast administration. The tumor is indicated with the red arrow. B) Before the sonications, no difference in tumor enhancement is observed after contrast administration (ΔSI=0.4%). C) After focused ultrasound-mediated blood-brain barrier disruption, the tumor enhances after contrast administration (ΔSI=30.1%)
Tumor growth and survival
At the start of the treatment (week 5) the mean tumor volume and standard deviation of all animals was 3.7±1.9 mm3 and no significant differences in volume were observed at this time point between the treatment groups. The mean growth constants during the treatment period (week 5 to week 11) were not significantly different with 0.042±0.011, 0.033±0.009 and 0.030±0.020 mm3/day for the control, antibody-only and FUS+antibody animals, respectively. In the FUS+antibody group, four animals were classified as responders and their average growth constant was 0.010±0.007 mm3/day, while the growth constant of the six non-responders was 0.043±0.013 mm3/day (Figure 4). ΔSI% of the responding rats (20.9%±16.1) and the non-responding rats (21.3%±10.4) were not significantly different. Also the mean tumor volume in week 5 was not significantly different between responders (4.1±2.5 mm3) and non responders (4.4±2.2 mm3). No animals were classified as responders in the antibody-only group.
Figure 4.

Tumor volume measurements for each group from the start of the treatment period (day 35) till sacrifice. The measurements were obtained every other week. Four rats in the FUS+antibody group were classified as responder during the treatment period. After treatment, their growth curves follow the same pattern as the other groups.
In the follow-up period (week 11 till sacrifice), growth constants were higher, but not significantly different among the treatment groups: 0.065±0.009, 0.055±0.017, and 0.056±0.012 for controls, antibody-only, and FUS+antibody animals respectively. The four animals that were classified as responder in the treatment period had an average growth constant of 0.060±0.016 during the follow-up period, indicating that the treatment benefit was temporary.
The median survival was 137 days for the control animals, 148 days for the antibody-only and 144 day for the FUS+antibody group. The survival curves of the antibody-only and FUS+antibody animals were significantly different from the control animals, but did not differ among themselves (Figure 5).
Figure 5.

Kaplan-Meier survival curves for the three treatment groups.
High-resolution T2w imaging showed that the tumor was homogenous till week 13–15, when in most animals cystic and necrotic areas started to develop. The tumors showed also a heterogeneous appearance on H&E-stained sections and the entire tumor was HER2-expressing in the examined brains (Figure 6 and 7).
Figure 6.

MRI images and histology of a control animal who did not receive treatment. A) Tumor on T2w imaging 5 weeks after implantation. B) Tumor on MR imaging when the animal reached the study endpoint. The tumor shows a heterogeneous appearance with cystic cavities. C) The hematoxylin & eosin-stained section corresponds well with MR-imaging and cysts are present. D) The HER2-stained section demonstrates that the complete tumor is HER2-expressing.
Figure 7.

MRI images and histology of a FUS+antibody animal who was classified as a responder. A) Tumor on MR imaging 5 weeks after implantation. B) Tumor on MR imaging when the animal reached the study endpoint. C) The hematoxylin & eosin-stained section has, like the MR image, a heterogeneous appearance with cystic areas, which was observed also in the other animals at the study endpoint. D) HER2-stained section confirms that the tumor is HER2-expressing. The box indicates the location of the enlargements in E (H&E) and F (HER2).
Discussion
In this study we have demonstrated that we can slow down growth of brain metastases from breast cancer using the HER2-targeting antibodies trastuzumab and pertuzumab in combination with FUS-mediated BBB disruption in some cases. Since the tumors were not leaky before BBB disruption and there were no responders in the antibody-only group, the disruption of the BBB appears to be necessary for drug delivery to these brain metastasis. Interestingly, only a portion of the rats responded to the treatment; the other animals had the same growth constant as the control-group. After the treatment, the growth constant of these animals was similar to the other animals, indicating that the effect is only present for the duration of the treatment. Although the treatment lasted only 6 weeks, this was enough to observe an improvement in survival compared to animals that were not treated.
Previously, it was demonstrated that median survival time increased by 32% in animals that received trastuzumab in combination with ultrasound-mediated disruption of the BBB compared to control animals (Park et al. 2012). In four of ten animals that were treated with FUS and trastuzumab, the tumor appeared to be resolved in follow-up MRI. In our study, we do not observe a decrease in tumor volume, but we did find an inhibition of tumor growth. The tumor cells used in the previous study were HER2-expressing BT-474 cells derived from a primary breast tumor. It is know that these cells are highly sensitive to trastuzumab (e.g. Narayan et al. 2009). Here, MDA-MB-361 cells were used, which were derived from a brain metastasis of a breast cancer patient, which might be a more appropriate model for translational purposes.
We performed cell growth assays with both cell lines to determine if the differences in results could be explained by the different cell lines. In vitro it was demonstrated that the response of the BT-474 cells was much stronger to trastuzumab than the response of the MDA-MB-361 cells, which is in line with our in vivo results where the response was not as impressive as in the study of Park et al. Furthermore, for the BT-474 cells a decrease in tumor cells was observed compared to day 0, which is in line with the in vivo observation of Park et al. where in the four responders the tumor appeared to be resolved on MR imaging after treatment. In clinical practice, the response to these antibodies for extracranial metastasis of breast cancer is heterogeneous with the largest number of patients showing a partial response, although also complete responses have been observed. (Baselga et al. 2012). Our study demonstrates that patients with tumors that are less sensitive to trastuzumab and/or pertuzumab can also potentially benefit from FUS-mediated BBB disruption.
We chose to combine trastuzumab with pertuzumab treatment, as combination of these antibodies has shown to improve the response in patients compared to using only trastuzumab as antibody (Baselga et al. 2012). Although in our in vitro study no significant improvement of the combination was observed compared to trastuzumab alone, MDA-MB-361 cells responded to both antibodies and the combination seemed to have the best effect. In clinical practice, trastuzumab and pertuzumab are combined with docetaxel, an anti-mitotic chemotherapeutic (Baselga et al. 2012). We did not include docetaxel in our study as our main interest was to demonstrate the effectiveness of FUS-mediated BBB disruption in this tumor model. Adding docetaxel might further improve the response; however, the toxic effect of delivery of docetaxel to the brain remains to be studied.
In our study, the median survival of the FUS+antibody animals was longer compared to the control group. As the treatment period was only 6 weeks, a longer treatment period might further elongate survival. The antibody-only arm also showed improved survival and we did not observe a difference in survival between the antibody-only and FUS+antibody arms. It is unclear why the animals in the antibody-only group lived longer, as our data suggests that tumor vessels were not leaky during the treatment period, and we did not see any cases with significant tumor growth inhibition.
Interestingly, in our study as well as studies by Park (Park et al. 2012) an Alkins (Alkins et al. 2016) a response was observed only in some of the animals. Both studies used tumor model based on HER2-positive cells from a breast cancer patient. There was no obvious reason for the difference in response. No difference in tumor volume at the start of the treatment was observed, nor were there differences in contrast-enhancement on T1w images between the responders and non-responders. Five brains were examined for HER2-expression, of which one belonged to a responder, and in all cases the whole tumor was HER2-expressing. In two rats, we performed additional T1w imaging to study tumor leakiness. In both animals, no enhancement of the tumor was observed, suggesting that these tumors were not leaky during the treatment period. One rat was classified as responder, while the other was not. Although we only studied tumor vascular permeability in two animals, these results suggest that leakiness is not the underlying difference between the groups. However, a difference in vasculature between the two groups at the time of the treatment cannot be eliminated using our MR imaging methods. The effects of FUS in combination with microbubbles vary for different vessel sizes. In vessels with a diameter around 20–30 um, more vasospasm (Raymond et al. 2007) and faster leakage and higher permeability (Nhan et al. 2013) are observed after sonications compared to larger vessels of ~40–60 um. This means that a potential difference in vessel size between the groups can lead to different responses to the FUS-treatment. As the time between treatment and sacrifice was long and tumors grew substantially in the meantime, no information on the vessel-size distribution at the time of treatment could be obtained with a blood-vessel staining in this study. In mice growing subcutaneous MDA-MB-361 tumors, 50% of the animals became unresponsive to trastuzumab after three weeks of treatment (Fujimoto-Ouchi et al. 2010). Similar to our study, no difference in tumor size at the start of the treatment was observed and the tumors remained HER2-expressing. However, in their study, all animal were responsive at the start of the treatment, which we did not observe. Whether the absence of a response in part of the animals is due to a lack of a response to the antibodies, is related to the quality of BBB disruption, comes from a difference in micro-vasculature, or is influenced by a response of the remaining remnant of the immune system or has another cause, remains unclear. In a future study, sacrifice directly after the treatment period might be preferable in order to investigate underlying differences between tumors that respond and do not respond to treatment. In the present study the time between treatment and sacrifice was large. As there were changes observed in the appearance of the tumors on MR images, we know that the tumors have changed and staining at the moment of sacrifice might not be representative for the tumor at the time of treatment. Therefore, it would be interesting to sacrifice and perform additional stainings like a blood-vessel staining (e.g. CD31) or HER2-receptor staining immediately after treatment. This hopefully would elucidate the difference in response. Better understanding of why certain animals respond is needed and will help in translating this technique to the clinic.
Here, we have demonstrated in a clinically relevant model that FUS-mediated BBB disruption can inhibit the growth of brain metastases from breast cancer. The duration of this growth inhibition was only during the treatment period and the growth constant after treatment was similar to the other animals. We could not explain why only a part of the animals responded and this remains topic for further research.
Acknowledgments
This study was financially supported by NIH grant P01CA174645, ERC grant PIOF-GA-2012-331813, and Dutch Cancer Society (KWF 2013-5861). We thank Chanikarn (Yui) Power for assisting during the animal procedures and Genentech for kindly providing the antibodies.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Thiele Kobus, Email: thiele.kobus@radboudumc.nl.
Ioannis K. Zervantonakis, Email: Ioannis_Zervantonakis@hms.harvard.edu.
Yongzhi Zhang, Email: yongzhiz@bwh.harvard.edu.
Nathan J. McDannold, Email: njm@bwh.harvard.edu.
References
- Alkins Ryan, Burgess Alison, Kerbel Robert, Wels Winfried S, Hynynen Kullervo. Early Treatment of HER2-Amplified Brain Tumors with Targeted NK-92 Cells and Focused Ultrasound Improves Survival. Neuro-Oncology. 2016 Jan; doi: 10.1093/neuonc/nov318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aryal Muna, Vykhodtseva Natalia, Zhang Yong-Zhi, Park Juyoung, McDannold Nathan. Multiple Treatments with Liposomal Doxorubicin and Ultrasound-Induced Disruption of Blood–tumor and Blood–brain Barriers Improve Outcomes in a Rat Glioma Model. Journal of Controlled Release. 2013;169(1–2):103–11. doi: 10.1016/j.jconrel.2013.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baselga José, Cortés Javier, Kim Sung-Bae, Im Seock-Ah, Hegg Roberto, Im Young-Hyuck, Roman Laslo, et al. Pertuzumab plus Trastuzumab plus Docetaxel for Metastatic Breast Cancer. New England Journal of Medicine. 2012;366(2):109–19. doi: 10.1056/NEJMoa1113216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boogerd W, Vos VW, Hart AaM, Baris G. Brain Metastases in Breast Cancer; Natural History, Prognostic Factors and Outcome. Journal of Neuro-Oncology. 1993;15(2):165–74. doi: 10.1007/BF01053937. [DOI] [PubMed] [Google Scholar]
- Chen Pin-Yuan, Liu Hao-Li, Hua Mu-Yi, Yang Hung-Wei, Huang Chiung-Yin, Chu Po-Chun, Lyu Lee-Ang, et al. Novel Magnetic/ultrasound Focusing System Enhances Nanoparticle Drug Delivery for Glioma Treatment. Neuro-Oncology. 2010;12(10):1050–60. doi: 10.1093/neuonc/noq054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fedorov Andriy, Beichel Reinhard, Kalpathy-Cramer Jayashree, Finet Julien, Fillion-Robin Jean-Christophe, Pujol Sonia, Bauer Christian, et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magnetic Resonance Imaging. 2012;30(9):1323–41. doi: 10.1016/j.mri.2012.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fujimoto-Ouchi Kaori, Sekiguchi Fumiko, Yamamoto Kaname, Shirane Masatoshi, Yamashita Yoriko, Mori Kazushige. Preclinical Study of Prolonged Administration of Trastuzumab as Combination Therapy after Disease Progression during Trastuzumab Monotherapy. Cancer Chemotherapy and Pharmacology. 2010;66(2):269–76. doi: 10.1007/s00280-009-1160-0. [DOI] [PubMed] [Google Scholar]
- Harputluoglu Hakan, Dizdar Omer, Aksoy Sercan, Kilickap Saadettin, Dede Didem S, Ozisik Yavuz, Guler Nilufer, et al. Characteristics of Breast Cancer Patients with Central Nervous System Metastases: A Single-Center Experience. Journal of the National Medical Association. 2008;100(5):521–26. doi: 10.1016/s0027-9684(15)31298-0. [DOI] [PubMed] [Google Scholar]
- Hynynen Kullervo, McDannold Nathan, Vykhodtseva Natalia, Jolesz Ferenc A. Noninvasive MR Imaging–guided Focal Opening of the Blood-Brain Barrier in Rabbits. Radiology. 2001;220(3):640–46. doi: 10.1148/radiol.2202001804. [DOI] [PubMed] [Google Scholar]
- Kinoshita M, McDannold N, Jolesz FA, Hynynen K. Noninvasive Localized Delivery of Herceptin to the Mouse Brain by MRI-Guided Focused Ultrasound-Induced Blood-Brain Barrier Disruption. Proceedings of the National Academy of Sciences of the United States of America. 2006;103(31):11719–23. doi: 10.1073/pnas.0604318103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leyland-Jones B. Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer and Central Nervous System Metastases. J Clin Oncol. 2009;27(31):5278–86. doi: 10.1200/JCO.2008.19.8481. [DOI] [PubMed] [Google Scholar]
- Lockman Paul R, Mittapalli Rajendar K, Taskar Kunal S, Rudraraju Vinay, Gril Brunilde, Bohn Kaci A, Adkins Chris E, et al. Heterogeneous Blood–Tumor Barrier Permeability Determines Drug Efficacy in Experimental Brain Metastases of Breast Cancer. Clinical Cancer Research. 2010;16(23):5664–78. doi: 10.1158/1078-0432.CCR-10-1564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Narayan Murli, Wilken Jason A, Harris Lyndsay N, Baron Andre T, Kimbler Kimberly D, Maihle Nita J. Trastuzumab-Induced HER Reprogramming In ‘resistant’ breast Carcinoma Cells. Cancer Research. 2009;69(6):2191–94. doi: 10.1158/0008-5472.CAN-08-1056. [DOI] [PubMed] [Google Scholar]
- Nhan Tam, Burgess Alison, Cho Eunice E, Stefanovic Bojana, Lilge Lothar, Hynynen Kullervo. Drug Delivery to the Brain by Focused Ultrasound Induced Blood–brain Barrier Disruption: Quantitative Evaluation of Enhanced Permeability of Cerebral Vasculature Using Two-Photon Microscopy. Journal of Controlled Release. 2013;172(1):274–80. doi: 10.1016/j.jconrel.2013.08.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pardridge WM. Blood-Brain Barrier Delivery. Drug Discov Today. 2007;12(1–2):54–61. doi: 10.1016/j.drudis.2006.10.013. [DOI] [PubMed] [Google Scholar]
- Park Eun-Joo, Zhang Yong-Zhi, Vykhodtseva Natalia, McDannold Nathan. Ultrasound-Mediated Blood–brain/blood-Tumor Barrier Disruption Improves Outcomes with Trastuzumab in a Breast Cancer Brain Metastasis Model. Journal of Controlled Release. 2012 doi: 10.1016/j.jconrel.2012.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pieokowski T, Zielinski CC. Trastuzumab Treatment in Patients with Breast Cancer and Metastatic CNS Disease. Ann Oncol. 2009;21(5):917–24. doi: 10.1093/annonc/mdp353. [DOI] [PubMed] [Google Scholar]
- Raymond Scott, Skoch Jesse, Hynynen Kullervo, Bacskai Brian J. Multiphoton Imaging of ultrasound/Optison Mediated Cerebrovascular Effects in Vivo. Journal of Cerebral Blood Flow & Metabolism. 2007;27(2):393–403. doi: 10.1038/sj.jcbfm.9600336. [DOI] [PubMed] [Google Scholar]
- Shang Xiuli, Wang Ping, Liu Yunhui, Zhang Zhen, Xue Yixue. Mechanism of Low-Frequency Ultrasound in Opening Blood–tumor Barrier by Tight Junction. Journal of Molecular Neuroscience. 2011;43(3):364–369. doi: 10.1007/s12031-010-9451-9. [DOI] [PubMed] [Google Scholar]
- Sheikov Nickolai, McDannold Nathan, Jolesz Ferenc, Zhang Yong-Zhi, Tam Karen, Hynynen Kullervo. Brain Arterioles Show More Active Vesicular Transport of Blood-Borne Tracer Molecules than Capillaries and Venules after Focused Ultrasound-Evoked Opening of the Blood-Brain Barrier. Ultrasound in Medicine & Biology. 2006;32(9):1399–1409. doi: 10.1016/j.ultrasmedbio.2006.05.015. [DOI] [PubMed] [Google Scholar]
- Sheikov Nickolai, McDannold Nathan, Sharma Shipra, Hynynen Kullervo. Effect of Focused Ultrasound Applied With an Ultrasound Contrast Agent on the Tight Junctional Integrity of the Brain Microvascular Endothelium. Ultrasound in Medicine & Biology. 2008;34(7):1093–1104. doi: 10.1016/j.ultrasmedbio.2007.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treat LH, McDannold N, Zhang Y, Vykhodtseva N, Hynynen K. Improved Anti-Tumor Effect of Liposomal Doxorubicin after Targeted Blood-Brain Barrier Disruption by Mri-Guided Focused Ultrasound in Rat Glioma. Ultrasound in Medicine and Biology. 2012 doi: 10.1016/j.ultrasmedbio.2012.04.015. http://www.scopus.com/inward/record.url?eid=2-s2.0-84863861914&partnerID=40&md5=f7994eee11cb0d7ce7af472c5e39c775. [DOI] [PMC free article] [PubMed]
- Yau Thomas, Swanton Charles, Chua Sue, Sue Ashley, Walsh Geraldine, Rostom A, Johnston Stephen R, O’Brien Mary ER, Smith Ian E. Incidence, Pattern and Timing of Brain Metastases among Patients with Advanced Breast Cancer Treated with Trastuzumab. Acta Oncologica (Stockholm, Sweden) 2006;45(2):196–201. doi: 10.1080/02841860500486630. [DOI] [PubMed] [Google Scholar]