

Abstract
Introduction
Afterschool programs (ASPs) across the US are working towards achieving the standard of all children accumulating 30minutes of moderate-to-vigorous physical activity (MVPA) during program time. This study describes the two-year impact of an intervention designed to assist ASPs meeting the 30min/d MVPA standard.
Methods
Using a two-year delayed treatment, group randomized controlled trial, 20 ASPs serving ~1,700 children/year (6–12yrs) were randomized to either an immediate (n=10, baseline-2013 and 2yrs intervention fall-2013-to-spring-2015) or delayed group (n=10, baseline 2013–2014 and 1yr intervention fall-2014-to-spring-2015). The intervention, Strategies-To-Enhance-Practice (STEPs), focused on programming MVPA in the daily schedule, training of staff and leaders, and ongoing technical support/assistance. Accelerometry-derived proportion of children meeting the 30min/d MVPA standard was measured in the spring of each year. Mixed model logistic regressions were used to examine the change in the odds of achieving the MVPA standard. Analyses were conducted in 2015. Data were collected in one southeastern US state.
Results
Immediate boys (n=677) and delayed girls (n=658) increased the percent achieving 30min MVPA/d from 35.9% to 47.0% (odds ratio [OR]=1.88, 95%CI 1.18–3.00) and 13.1% to 19.1% (OR=1.42, 95%CI 1.03–1.96). Immediate girls (n=613) and delayed boys (n=687) exhibited a nonsignificant increase from 19.1% to 21.6% (OR=1.20, 95%CI 0.84–1.72) and 29.0% to 31.3% (OR=1.13, 95%CI 0.80–1.58).
Conclusions
STEPs can have an impact on children’s MVPA and time spent sedentary, yet was unable to fully achieve the goal of all children accumulating 30min MVPA/d. Additional efforts are need to identify strategies ASPs can use to meet this important public health standard.
Keywords: Obesity, Standards, School, Intervention, Accelerometer
Introduction
Across the US, afterschool programs (ASPs) serve more than 10 million children annually for up to 3 hours every day of the school year.[1] Given this extensive reach and contact time, ASPs have become a natural extension of the childhood obesity prevention efforts targeting schools. As part of these efforts, both national and state level organizations have developed and widely disseminated physical activity (PA) policies/standards to establish the amount of PA children should accumulate during an ASP.[2–5] One of the most prominent and potentially impactful policies is the standard that calls for all children attending an ASP to accumulate a minimum of 30 minutes per day of moderate-to-vigorous physical activity (MVPA) during program time and reduce the amount of time children are sedentary.[6] With the implementation of high-quality strategies to increase MVPA, achieving this standard has the potential to substantially impact children’s PA by providing at least half of their daily recommended MVPA during the ASP.[7] Unfortunately, many ASP providers struggle to achieve this goal.[8, 9]
While, numerous PA interventions have been developed and tested in the ASP setting,[10–17] few have attempted to achieve the 30min MVPA standard and few have reported more than a single year of intervention delivery.[18–20] Since staff turnover at the site leader and frontline staffing positions are one of the major challenges faced within the ASP setting,[21, 22] investigating the delivery of an intervention over multiple years within this setting is critical. Many of the staff employed at ASPs are part-time or transitional (only employed for a single school year) employees. Site leaders and staff are also directly responsible for the implementation of PA programming. Because of this, strategies need to be easily communicated to new staff and also unaffected by changes to the site leader position, the person responsible for the day-to-day operations of the program. Attention to this should facilitate a greater level of implementation of an intervention and, subsequently, lead to greater improvements in children’s MVPA.[23]
This study details the two year PA outcomes from the Making Healthy Eating and Physical Activity Policy Practice group randomized controlled trial in 20 diverse ASPs.[24, 25] The study used immediate and delayed treatment groups that allowed for the investigation of the effect of the intervention on children’s PA over multiple years in the immediate group and the replication of the intervention within the delayed group. It was hypothesized that two years of receiving the intervention would result in greater gains than a single year of intervention and the intervention effect would be replicated in the delayed treatment group.
Methods
A detailed description of the study design, intervention, measures, and first year outcomes are presented elsewhere.[24, 25] The study design is a repeated cross sectional group randomized controlled trial with a delayed treatment group. This design is appropriate when outcomes are tracked at a group level (e.g., ASPs), instead of at the individual level (e.g., children)[26, 27] and is consistent with recent large scale trials of site-level interventions for children and adolescents.[18, 28–32] The results presented in this study are from the final outcome year of a three year delayed intervention group.
Participants and Setting
Afterschool programs, defined as child care programs operating immediately after the school day, every day of the school year for a minimum of 2 hours, serving a minimum of 30 children of elementary age (6–12yrs), operated in a school, community, or faith setting, and located within a 1.5hr drive from the university were eligible to participate. Programs, from a single southeastern state in the US, were identified from a registry of ASPs operating in the state and randomly selected for invitation to participate in the study. Informed consent and verbal assent were obtained from parents and children participating in this study. All study procedures were approved by the Institutional Review Board of the lead author at the University of South Carolina.
Randomization
The twenty ASPs were randomized into one of two conditions: 1) immediate or 2) delayed group. Randomization was performed after baseline data collection, during June 2013 (see Figure 1). Programs were paired based on enrollment size and the percentage of children meeting the 30min of MVPA/day standard and then randomly assigned to immediate or delayed group using a random number generator by study staff. Characteristics for immediate and delayed ASPs are presented in Table 1. The delayed group was asked to continue with current ASP practices and received no technical assistance or support from the intervention staff until the final year of the study where they would receive the intervention. The immediate treatment group received two years of the intervention.
Figure 1.
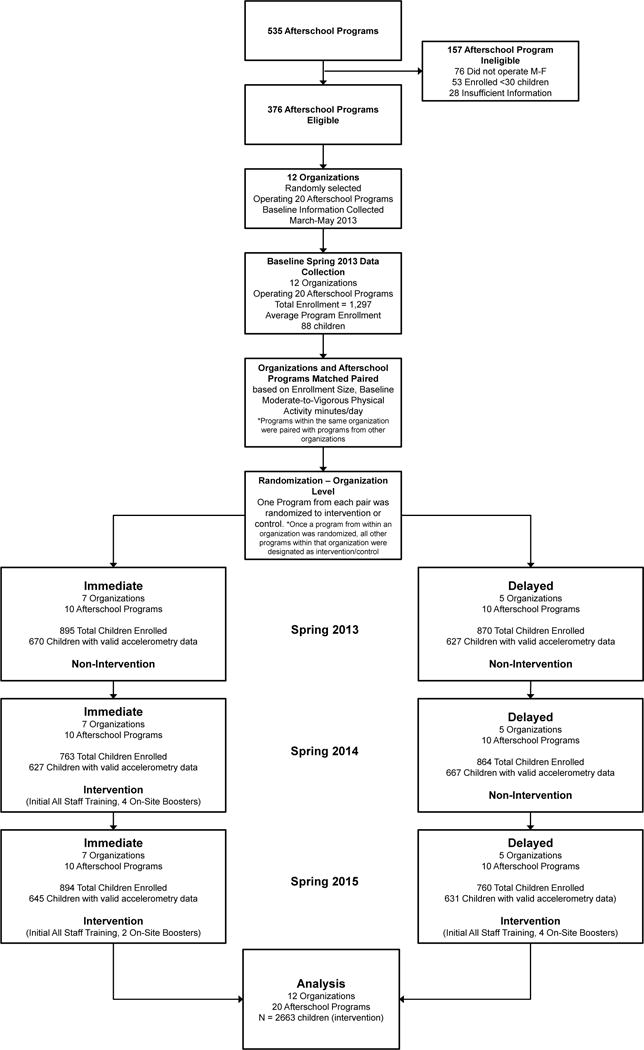
CONSORT diagram
Table 1.
Characteristics of Afterschool Programs and Children Enrolled by Treatment Condition
| Delayed Treatment | Immediate Treatment | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Spring 2013 (Baseline) | Spring 2014 (Baseline) | Spring 2015 (Intervention) | Spring 2013 (Baseline) | Spring 2014 (Intervention) | Spring 2015 (Intervention) | |||||||
| Afterschool program characteristics | ||||||||||||
| Total kids enrolled | 870 | 864 | 760 | 895 | 763 | 894 | ||||||
| Boys (%) | 52.4 | 51.3 | 50.4 | 53.3 | 52.4 | 54.2 | ||||||
| Average enrollment (no. of kids, M, SD) | 87.0 | ±47.8 | 86.4 | ±39.5 | 76.0 | ±44.2 | 89.5 | ±52.0 | 76.3 | ±45.9 | 89.4 | ±59.3 |
| Physical activity space (ft2) | ||||||||||||
| Indoor | 9,731 | ±7,617.9 | NC | NC | 13, 835 | ±17,003.5 | NC | NC | ||||
| Outdoor | 218,273 | ±320,146.3 | NC | ±320,146.3 | NC | ±320,146.3 | 199,243 | ±229,623.6 | NC | ±320,146.3 | NC | ±320,146.3 |
| Percentage of population in poverty, Census 2010 | 17.5 | ±10.2% | NC | NC | 13.3 | ±15.6% | NC | NC | ||||
| Daily program length (minutes per day, M, SD) | 205.5 | ±134.3 | NC | NC | 190.5 | ±128.7 | NC | NC | ||||
| Location (n) | ||||||||||||
| School | 6 | NC | NC | 3 | NC | NC | ||||||
| Faith/church | 1 | NC | NC | 3 | NC | NC | ||||||
| Community (e.g., recreation center) | 3 | NC | NC | 4 | NC | NC | ||||||
| Program schedule time for physical activity opportunities (minutes per day, M, SD) | 53.1 | ±15.6 | 75.5 | ±35.9 | 58.2 | ±14.2 | 94.8 | ±39.9 | 81.3 | ±29.2 | 88.7 | ±21.3 |
| Site Leader and Staff Turnover | ||||||||||||
| Number of ASPs with Site Leader Turnover | 3 | Sp14 vs. Sp13 | 5 | Sp15 vs. Sp14 | 1 | Sp14 vs. Sp13 | 2 | Sp15 vs. Sp14 | ||||
| Number of ASPs with Frontline Staff Turnover | 8 | 9 | 8 | 8 | ||||||||
| Median Percent Frontline Staff Turnover | 50 % | 33 % | 49 % | 48 % | ||||||||
| Child characteristics | ||||||||||||
| Race/Ethnicity (%) | ||||||||||||
| White non-Hispanic | 48.4 | 46.8 | 55.2 | 64.6 | 59.0 | 66.9 | ||||||
| African American | 44.7 | 45.5 | 38.7 | 29.7 | 34.3 | 26.1 | ||||||
| Other | 6.9 | 7.7 | 6.1 | 5.7 | 6.7 | 7.0 | ||||||
| Age (years, M, SD) | 8.1 | ±1.8 | 7.9 | ±1.9 | 7.8 | ±1.7 | 7.9 | ±1.8 | 7.9 | ±1.8 | 7.6 | ±1.7 |
| BMI (%) | ||||||||||||
| <85th percentile | 59.0 | 62.8 | 71.5 | 68.2 | DNC | |||||||
| ≥85th percentile, <95th percentile | 22.1 | 21.3 | 20.0 | 21.0 | DNC | |||||||
| ≥95th percentile | 19.0 | 15.9 | 8.5 | 10.8 | DNC | |||||||
| Accelerometer Estimates (minutes/day, unadjusted estimates) | ||||||||||||
| Boys | ||||||||||||
| Sedentary | 65.7 | ±24.7 | 61.6 | ±27.0 | 61.3 | ±23.7 | 60.1 | ±21.8 | 51.7 | ±19.0 | 47.4 | ±18.8 |
| Light PA | 42.2 | ±17.4 | 42.5 | ±16.8 | 45.4 | ±16.1 | 41.1 | ±15.9 | 43.2 | ±15.3 | 42.5 | ±15.3 |
| MVPA | 22.7 | ±14.6 | 22.9 | ±12.4 | 24.0 | ±11.7 | 24.6 | ±13.3 | 27.2 | ±14.0 | 26.5 | ±14.0 |
| Percentage meeting 30 minutes/d MVPA Standard | 31.8% | 29.8% | 31.7% | 35.6% | 41.0% | 39.6% | ||||||
| Total Wear Time | 130.5 | ±40.1 | 127.0 | ±40.7 | 130.7 | ±36.3 | 125.8 | ±34.2 | 122.1 | ±32.6 | 116.3 | ±30.9 |
| Girls | ||||||||||||
| Sedentary | 74.3 | ±28.1 | 71.5 | ±27.6 | 65.5 | ±23.0 | 62.4 | ±21.8 | 58.4 | ±20.1 | 57.4 | ±21.3 |
| Light PA | 42.7 | ±17.5 | 44.2 | ±16.8 | 43.7 | ±16.1 | 39.4 | ±16.9 | 40.8 | ±15.6 | 41.4 | ±15.1 |
| MVPA | 17.4 | ±11.0 | 17.9 | ±9.8 | 19.9 | ±10.1 | 18.0 | ±11.0 | 20.5 | ±11.8 | 19.4 | ±10.6 |
| Percentage meeting 30 minutes/d MVPA Standard | 15.0% | 12.8% | 19.5% | 16.2% | 21.3% | 18.2% | ||||||
| Total Wear Time | 134.4 | ±41.0 | 133.6 | ±39.2 | 129.1 | ±36.6 | 119.7 | ±33.7 | 119.7 | ±32.3 | 118.3 | ±31.3 |
| Boys and Girls | ||||||||||||
| Percentage meeting 30 minutes/d MVPA Standard (Baseline randomization factor) | 24.2% | 26.7% | ||||||||||
Abbreviations: NC, no change from baseline to post-assessment; DNC, did not collect; MVPA, Moderate-to-Vigorous Physical Activity; PA, Physical Activity
Intervention
A detailed description of the intervention is described elsewhere.[24] To achieve the 30-minute/day MVPA policy goal,[6] the following intervention approach was developed. Briefly, the Strategies To Enhance Practice for PA (STEPs) conceptual framework involved a multistep adaptive approach to incorporating MVPA into daily routine practice.[33–37] STEPs predominately focused on the ASP leader and worked with them to develop programmatic capacity in the form of high-quality schedules that included PA opportunities every day as well as clearly articulating the roles and responsibilities of staff during scheduled activity opportunities. Each ASP was also asked to schedule a minimum of 60 minutes/day for PA opportunities.[6] The staff component of STEPs LET US (Lines, Elimination, Team size, Uninvolved staff/kids, and Space, equipment and rules) Play[38] focused on developing the skills of staff to modify games staff are familiar with and children enjoy playing with the primary objective of maximizing children’s MVPA. This departed from prior interventions where staff were provided equipment and trained to play new games or relied on ASP leaders and staff to develop their own strategies.[10, 11, 13, 16, 18, 21, 22]
Trainings for ASPs in the immediate condition occurred during July/August of 2013 (first year of receiving the intervention) and 2014 (second year of receiving the intervention) and lasted approximately 3 hours. Trainings for the ASPs in the delayed condition occurred during July/August of 2014. For organizations operating two or more programs, a single training was provided for the ASP leaders at one location. During the first year of receiving the intervention for both the immediate and delayed ASPs, each ASP received four booster sessions. During the second year of receiving the intervention (for the immediate condition only) 2 booster sessions/ASP were provided. During non-intervention years for both groups, no intervention contacts occurred. Each booster session lasted for the entirety of a single ASP operating day (e.g., 3PM–6PM). The booster session included a walkthrough of the ASP with the site leader to identify PA opportunities and LET US Play principles.[33, 38] Both research personnel and site leaders and staff convened a 20–30-minute meeting immediately after the end of the ASP to discuss areas that were consistent and inconsistent with meeting the PA standards. Strategies to address any inconsistencies with meeting the PA standards were agreed upon and implemented. Follow-up booster phone calls with the site leader were conducted bi-weekly to address any implementation challenges. The total amount of intervention contact the immediate group received across the two years was 6 hours plus 30min for each of the 6 booster sessions. The delayed group received 3 hours plus 30min for each of the 4 booster sessions. Implementation of STEPs is published elsewhere.[39, 40]
Measures
All measurements occurred during the spring (March-April) of 2013, 2014, and 2015. Consistent with previously established protocols, each ASP was visited for PA data collection on four nonconsecutive, unannounced days Monday–Thursday.[8, 25, 41] Child demographics were self-reported, and standing height and weight were measured using standard protocols with children wearing light clothing at baseline 2013 and after the first intervention year 2014.[42] The primary PA and sedentary behavior outcome was derived via accelerometry. All children attending an ASP on unannounced measurement days had an opportunity to wear the ActiGraph GT3X+. The accelerometers were distilled using 5-second epochs to account for the intermittent and sporadic nature of children’s PA[43] and to improve the ability to capture the transitory PA patterns of children.[44–48] When children arrived to a program, they were fitted with an accelerometer and the arrival time was recorded (monitor time on). Before a child departed from a program, research staff removed the belt and recorded the time of departure (monitor time off). Children wore the monitors for their entire attendance at the ASPs.[8, 25, 41] Cutpoint thresholds associated with moderate and vigorous activity were used to distill the PA intensity levels[49] and sedentary behavior.[50] Children were considered to have a valid day of accelerometer data if their total wear time (time off minus time on) was ≥60 minutes.[8, 41, 51]
Statistical Analysis
Data were analyzed in 2015. Analyses were conducted only on children with at least one valid accelerometer wear day at any measurement occasion.[8, 41, 51] Descriptive means, SDs, and percentages (for dichotomous variables) for ASPs and child characteristics were computed. To evaluate the impact of STEPs on achieving the standard of 30 minutes/day of MVPA (study’s primary outcome), the minutes all children at each measurement occasion (i.e., spring 2013, 2014, and 2015) spent in MVPA were dichotomized to represent those children who achieved (i.e., ≥30 minutes MVPA/day) and those that failed to achieve (i.e., <30 minutes MVPA/day) the PA policy.[6] As a secondary outcome, time spent sedentary was dichotomized into children spending 60 minutes or more sedentary versus those children who spent less than 60 minutes sedentary while attending the ASP.[6] Repeated-measures random effects logit models, with days measured nested within children nested within ASPs, were estimated using the dichotomized variables as the dependent variable for boys and girls, separately, to compare changes in the primary outcomes between treatment groups over time. Included in the models were a main effect for treatment group, time, and the time-x-treatment interaction. Covariates in the model included the total time children attended each day, age (years), race (African American), allotted time for PA opportunities at each measurement year, total enrollment, staff turnover, and program location/setting (school, faith or community center). These models were also performed for those boys and girls that were present at each of the three measurement occasions. Changes in the amount of minutes spent in MVPA and sedentary were modeled using repeated- measures random effects quantile regression modeling[52] the 25th, 50th, and 75th quantiles of the distribution and design-matrix bootstrapped standard errors. This modeling approach was chosen due to the non-normal distribution of the outcome variables and to investigate the impact of the intervention on both high and low active children. The same covariates were used for the quantile regression. Where a significant time or time-treatment interaction occurred, post-hoc within and between group analyses were conducted. Matched pairs were not included in the analyses given the small number of pairs. All analyses were performed using Stata, version 13.1 (College Station, TX) using full information maximum likelihood estimators.
Results
The descriptive characteristics of the 20 ASPs and children are presented in Table 1. Unconditional intraclass correlation coefficients at the ASP and child level were 0.09 and 0.42, respectively. Across the three measurement waves the number of days children had with a valid day of data was 2.5±1.1, 2.3±1.0, and 2.4±1.1 days. The results of the logit models, examining the change in the proportion of boys accumulating 30 minutes of more of MVPA/d indicated a non-significant main effect for group and time, and a significant time-x-treatment interaction (see Figure 2). Compared to boys in the delayed group, boys in the immediate group increased the odds of meeting the standard by odds ratio (OR)=1.81 (95%CI 1.17–2.80) after the first year of receiving intervention, with this maintaining (OR=1.88, 95%CI 1.18–3.00) by the end of year two of the intervention. There were no significant changes for boys in the delayed group. Follow-up analyses indicated there were no significant differences in the gains observed between the first and second year of receiving the intervention in the immediate group. For girls, there was a significant time and time-x-treatment interaction. Girls in the immediate group increased the odds of meeting the standard by OR=1.91 (95%CI 1.21–3.01) in the first year of receiving the intervention, while girls in the delayed group increased the odds of meeting the standard by OR=1.42 (95%CI 1.03–1.96) after the first year of receiving the intervention. The increase observed with the girls’ in the immediate group was lost during the second year of receiving the intervention.
Figure 2.
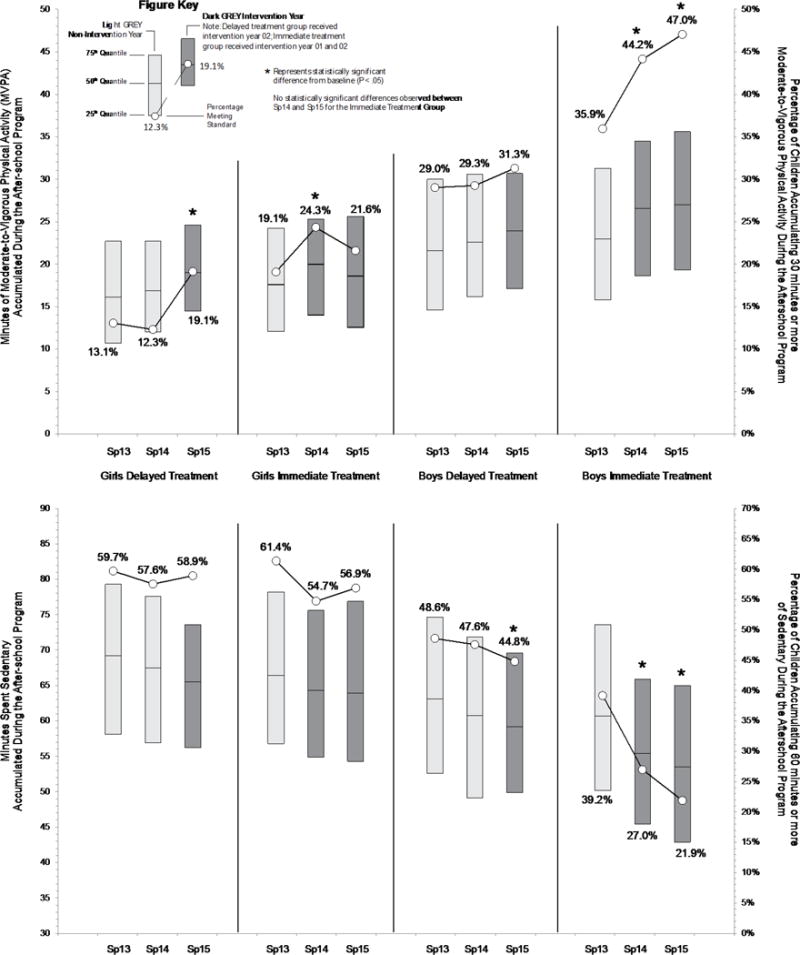
Minutes spent in moderate-to-vigorous physical activity (MVPA) and sedentary for boys and girls and treatment group, separately, across the study’s three measurement occasions (spring 2013, 2014, and 2015). Abbreviations: Sp = Spring
For boys and the amount of time spent sedentary, there was a non-significant main effect for group and a significant time and time-x-treatment effects. For boys in the immediate treatment group, there was decrease in the odds of accumulating 60 or more minutes of time spent sedentary after the first year of receiving the intervention by OR=0.49 (95%CI 0.32–0.76) and by OR=0.45 (95%CI 0.28–0.71) after the second year of intervention. Follow-up analyses indicated there were no significant differences in the decrease observed between year one and two in the immediate group. In the delayed group, there was a decrease in the odds of accumulating 60 or more minutes of time spent sedentary at year one of receiving the intervention by OR=0.67 (95%CI 0.48–0.93). For girls there was a non-significant main effect for group, time, and the time-x-treatment interaction.
A total of 187 boys and 142 girls were present at each measurement occasion and had at least one valid day of physical activity assessment. Overall, the effects were largely consistent to those from the total sample. For MVPA, there was an overall significant time-x-treatment interaction for boys. Boys in the immediate group increased their odds of meeting the MVPA standard by OR=2.37 (95%CI 1.27–4.42) and OR=1.95 (95%CI 1.02–3.70) at year one and year two of the intervention compared to boys attending the delayed programs. There were no significant effects for girls for MVPA for either group. For sedentary, there was a significant time-x-treatment interaction, with boys in the immediate group decreasing their odds of spending 60 or more minutes sedentary by OR=0.47 (95%CI 0.26–0.86) after the second year of intervention. For girls, there was a significant time effect, with girls attending the delayed group decreasing their odds of being sedentary by OR=0.52 (95%CI 0.31–0.89) after the first year of intervention. There were no significant effects for girls in the immediate group.
The results of the random effects quantile regressions on the 25th, 50th, and 75th quantiles of minutes of MVPA and sedentary are presented in Table 2. Changes in minutes spent sedentary or in MVPA are illustrated by gender and treatment group in Figure 2. Changes in minutes spent in MVPA and percentage meeting the 30min/d MVPA standard for boys and girls by ASP can be found in supplemental Figure 1S. As seen in Figure 2 and Table 2, for boys in the immediate group, statistically significant increases (3.5 to 4.3 minutes/day across quantiles) in MVPA were observed across the three quantiles from baseline (spring 2013) to spring 2015 (second year of intervention). For girls in the immediate group, no statistically significant increases were observed from baseline to the end of the second year of intervention. For boys in the delayed group, no significant changes were observed from the last year of baseline (spring 2014) to spring 2015 (first year of intervention). For girls in the delayed group, increases in MVPA were observed across the three quantiles (1.9 to 2.5 minutes/day) from baseline (spring 2014) to intervention. For time spent sedentary, boys in the immediate group had a significant reduction of 7.2 to 8.6 minutes of sedentary across quantiles by the end of the second intervention year (spring 2015, see Table 2 and Figure 2). For girls in the immediate group, a significant reduction of time spent sedentary was observed for only the 50th quantile (−2.5 minutes/day). For boys in the delayed group a significant reduction of time spent sedentary was observed for only the 75th quantile (2.3 minutes/day). Significant reductions were observed for girls in the delayed group across the 50th and 75th quantiles (2.0 to 4.0 minutes/day).
Table 2.
Model Estimated Changes in Moderate-to-Vigorous Physical Activity (MVPA) and Time Spent Sedentary from spring 2013, 2014, and 2015
| Moderate-to-Vigorous Physical Activity (minutes/day) | Time Spent Sedentary (minutes/day) | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Immediate | Delayed | Within-Between Group P-values |
Within Group P-values |
Immediate | Delayed | Within-Between Group P-values |
Within Group P-values |
||||||||||||||
| Quantile | Year | Est. | (SE) | Est. | (SE) | Differencea | Treatment | Time | Time- ×- Treatment |
Immediatec | Delayedb | Est. | (SE) | Est. | (SE) | Difference | Treatment | Time | Time- ×- Treatment |
Immediatec | Delayedb |
| Boys | |||||||||||||||||||||
| 25 th | Spring 13 | 15.8 | (0.6) | 14.6 | (0.7) | 1.2 | 0.173 | 0.001 | 0.175 | 50.2 | (0.9) | 52.6 | (1.4) | −2.4 | 0.0370 | 0.0020 | 0.0130 | ||||
| Spring 14 | 18.6 | (0.7) | 16.2 | (0.7) | 2.4 | 45.4 | (1.1) | 49.1 | (1.1) | −3.7 | |||||||||||
| Spring 15 | 19.3 | (0.7) | 17.1 | (0.9) | 2.2 | 42.9 | (1.3) | 49.9 | (1.3) | −7.0 | |||||||||||
| Baseline vs. Final Intervention Time Pointb | 3.5 | (0.7) | 0.9 | (0.8) | 2.6 | 0.093 | −7.3 | (1.1) | 0.8 | (1.3) | −8.1 | 0.970 | |||||||||
| Intervention Y01 vs. Y02c | 0.7 | (0.7) | — | 0.445 | −2.5 | (1.2) | — | 0.062 | |||||||||||||
| 50 th | Spring 13 | 23.0 | (0.7) | 21.6 | (0.9) | 1.4 | 0.131 | 0.010 | 0.011 | 60.7 | (1.0) | 63.1 | (1.3) | −2.4 | 0.015 | 0.001 | 0.047 | ||||
| Spring 14 | 26.6 | (0.7) | 22.6 | (0.9) | 4.0 | 55.4 | (0.9) | 60.8 | (1.1) | −5.4 | |||||||||||
| Spring 15 | 27.0 | (0.9) | 23.9 | (0.9) | 3.1 | 53.5 | (1.1) | 59.2 | (1.2) | −5.7 | |||||||||||
| Baseline vs. Final Intervention | 4.0 | (1.0) | 1.3 | (0.9) | 2.7 | 0.056 | −7.2 | (1.2) | −1.6 | (1.1) | −5.6 | 0.036 | |||||||||
| Time Pointb | |||||||||||||||||||||
| Intervention Y01 vs. Y02c | 0.4 | (0.8) | — | 0.494 | −1.9 | (0.9) | — | 0.007 | |||||||||||||
| 75 th | Spring 13 | 31.3 | (0.7) | 30.0 | (0.8) | 1.3 | 0.255 | 0.444 | 0.006 | 73.6 | (1.1) | 74.7 | (1.4) | −1.1 | 0.031 | 0.001 | 0.005 | ||||
| Spring 14 | 34.5 | (0.8) | 30.6 | (0.8) | 3.9 | 65.9 | (1.2) | 71.9 | (1.4) | −6.0 | |||||||||||
| Spring 15 | 35.6 | (0.8) | 30.7 | (0.7) | 4.9 | 65.0 | (1.5) | 69.6 | (1.6) | −4.6 | |||||||||||
| Baseline vs. Final Intervention Time Pointb | 4.3 | (0.9) | 0.1 | (0.9) | 4.2 | 0.204 | −8.6 | (1.5) | −2.3 | (1.2) | −6.3 | 0.078 | |||||||||
| Intervention Y01 vs. Y02c | 1.1 | (0.9) | — | 0.130 | −0.9 | (1.1) | — | 0.104 | |||||||||||||
| Girls | |||||||||||||||||||||
| 25 th | Spring 13 | 12.1 | (0.5) | 10.7 | (0.6) | 1.4 | 0.017 | 0.005 | 0.001 | 56.8 | (0.8) | 58.1 | (1.4) | −1.3 | 0.281 | 0.230 | 0.765 | ||||
| Spring 14 | 14.0 | (0.6) | 12.0 | (0.5) | 2.0 | 54.9 | (1.1) | 56.9 | (1.3) | −2.0 | |||||||||||
| Spring 15 | 12.6 | (0.7) | 14.5 | (0.6) | −1.9 | 54.3 | (1.2) | 56.2 | (1.5) | −1.9 | |||||||||||
| Baseline vs. Final Intervention Time Pointb | 0.5 | (0.7) | 2.5 | (0.5) | −2.0 | 0.001 | −2.5 | (1.3) | −0.7 | (1.1) | −1.8 | 0.448 | |||||||||
| Intervention Y01 vs. Y02c | −1.4 | (0.7) | — | 0.059 | −0.6 | (1.1) | — | 0.625 | |||||||||||||
| 50 th | Spring 13 | 17.6 | (0.6) | 16.1 | (0.5) | 1.5 | 0.023 | 0.001 | 0.147 | 66.4 | (0.8) | 69.2 | (1.2) | −2.8 | 0.007 | 0.001 | 0.436 | ||||
| Spring 14 | 20.0 | (0.7) | 16.9 | (0.5) | 3.1 | 64.3 | (1.2) | 67.5 | (1.2) | −3.2 | |||||||||||
| Spring 15 | 18.6 | (0.8) | 19 | (0.6) | −0.4 | 63.9 | (1.3) | 65.5 | (1.3) | −1.6 | |||||||||||
| Baseline vs. Final Intervention Time Pointb | 1.0 | (0.9) | 2.1 | (0.7) | −1.1 | 0.008 | −2.5 | (1.2) | −2.0 | (1.1) | −0.5 | 0.021 | |||||||||
| Intervention Y01 vs. Y02c | −1.4 | (0.7) | — | 0.057 | −0.4 | (1.2) | — | 0.800 | |||||||||||||
| 75 th | Spring 13 | 24.2 | (0.8) | 22.7 | (0.9) | 1.5 | 0.120 | 0.046 | 0.603 | 78.2 | (0.9) | 79.3 | (1.2) | −1.1 | 0.112 | 0.001 | 0.047 | ||||
| Spring 14 | 25.3 | (0.9) | 22.7 | (0.8) | 2.6 | 75.6 | (1.2) | 77.6 | (1.4) | −2.0 | |||||||||||
| Spring 15 | 25.6 | (0.9) | 24.6 | (1.0) | 1.0 | 76.9 | (1.5) | 73.6 | (1.5) | 3.3 | |||||||||||
| Baseline vs. Final Intervention Time Pointb | 1.4 | (0.8) | 1.9 | (0.8) | −0.5 | 0.012 | −1.3 | (1.5) | −4.0 | (1.2) | 2.7 | 0.013 | |||||||||
| Intervention Y01 vs. Y02c | 0.3 | (1.0) | — | 0.680 | 1.3 | (1.2) | — | 0.278 | |||||||||||||
Note: Immediate treatment group received the intervention spring 2014 and 2015. The delayed treatment group received the intervention spring 2015;
Between group difference for each measurement year;
Within group overall change: Immediate Spring 2015 (last year of intervention) vs. Spring 2013 (baseline), Delayed Spring 2015 (first year of intervention) vs. Spring 2014 (last year of baseline);
Difference between intervention Spring 2014 (intervention year 01) and Spring 2015 (intervention year 02) for the immediate group only
Sample size: Boys Immediate, n = 677; Boys Delayed, n = 687; Girls Immediate, n = 613; Girls Delayed, n = 658
Discussion
This study presents the second year outcomes of a three year delayed treatment, group randomized intervention designed to achieve the 30min MVPA standard for ASPs. Overall, the intervention was able to: increase the boys meeting the MVPA standard in the immediate group across the 2 years of receiving the intervention, improve mean percent of girls meeting the MVPA standard in the immediate group during the first year of intervention, and increase the mean percent of girls meeting the MVPA standard in the delayed group during their year of intervention, with limited changes in mean percent of the boys meeting the MVPA standard in the delayed group. Based on this, the hypothesis that receiving two years of intervention would be more effective than receiving one was not supported and the hypothesis that the intervention effect would be replicated in the delayed group partially supported. These findings highlight the heterogeneity within and between ASPs across three years of evaluation, as well as, the difficulties associated with achieving the 30min MVPA standard. Nevertheless, improvements were observed across groups for minutes spent in MVPA and reductions in minutes spent sedentary with some of the greatest increases (or reductions) occurring in the children who engaged in the least amount of MVPA (25th quantile) or were the most inactive (75th quantile of sedentary). Thus, while the STEPs intervention was unable to fully achieve the MVPA standard of all children accumulating 30 minutes of MVPA, meaningful improvements in the desired directions were attained.
As indicated in Figure 1S, there was substantial variability in MVPA within and between ASPs across all years of the study. Moreover, for those ASPs that were operated by the same organization, there was substantial variability in MVPA and responsiveness to STEPs. This illustrates several important challenges working in this setting. The variability in MVPA and responsiveness to the intervention within an organization suggests that children’s MVPA and programmatic structure changes are largely driven at the site-level, rather than at an organizational level. A clear example of this is represented in both the delayed and immediate treatment groups where some ASPs continued to improve as part of the intervention over the two years (e.g., ASPs 5 and 6 immediate group), some improved from receiving the intervention for one year (e.g., ASPs 1, 2, and 5 delayed group), some remained relatively unchanged (e.g., ASP 7 immediate group), and some decreased MVPA despite receiving the intervention (e.g., ASP 4 immediate and ASPs 3 and 4 delayed group). These findings suggest that efforts should primarily be directed to the site level and the individuals responsible for the day-to-day operations of the program and their staff. Thus, additional efforts in working with these individuals are necessary.
The lack of an improvement for the boys in the delayed group was unexpected, yet was likely due to a reduction of time allocated for physical activity only opportunities in the delayed ASPs. As detailed in the process evaluation,[39, 40] during spring 2015 (the only year of intervention for the delayed group) 9 of the 10 delayed ASPs reduced their schedule PA opportunities to no more than 60 minutes/day and 5 of them allowed children to select a sedentary activity, such as using the computer lab, during this time. Two recent study show that extending the time allocated for PA[53] and not allowing children to select an inactive activity[54] were associated with higher levels of MVPA and less time spent sedentary in ASPs. Thus, ensuring ample time is allocated and children can only be active during this time appear to be important strategies ASPs can use to get children more active. Improvements, however, were found in the LET US Play enhancements of STEPs (e.g., verbal encouragement, removing lines) which likely helped boys maintain and girls improve their level of MVPA despite the reduction in allocated time for PA. The limited improvement observed across both treatment groups for girls was disappointing and, unfortunately, consistent with other studies attempting to increase girls MVPA.[28, 55] One of the primary reasons for this was the limited attention the STEPs framework has towards “girl-specific” strategies, with only a single strategy targeting girls solely. Additional work is required to identify other, more salient, strategies that ASP providers can easily use to help increase girls’ MVPA.
This study has a number of strengths: the group randomization, delayed treatment design, large number of ASPs, large number of children measured over time, 3 year study timeframe, objective measure of PA, and diversity of program settings, organizations, and enrollment size. However, there are several limitations that need to be considered when interpreting these findings. First, all the programs were operated in one geographical location in a southeastern state. Thus, the findings may not generalize to programs operating in other states. Second, while the study included 20 ASPs, this sample size at the group level is limited in testing site-level analyses to identify site-level characteristics related to children’s MVPA. Thus, future studies should attempt to measure the PA and site-level characteristics within a larger sample of ASPs.
In conclusion, the STEPs approach was unable to fully achieve the 30 minutes of MVPA standard. However, it was able to make changes in time spent in MVPA and sedentary for both intervention groups. Future studies attempting to achieve the 30 minute MVPA standard should evaluate new, or augment existing, strategies to determine what works best in this setting to reach the standard.
Supplementary Material
Online Supplemental Figure 1. Minutes spent in moderate-to-vigorous physical activity for boys and girls by afterschool program across the three study measurement occasions (spring 2013, 2014, and 2015).
Highlights.
Afterschool programs struggle to meet the 30 min/day moderate-to-vigorous standard
Few intervention studies have attempted to meet the physical activity standard
Over 2 years, improvements can be made towards achieving the activity standard
Effectiveness of the intervention varied by gender and how many years received
Tailoring at program level is required to achieve the activity standard
Acknowledgments
None
Funding: Research reported in this publication was supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number R01HL112787. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Potential conflicts of interest: The authors declare that there are no conflicts of interest
Clinical Trials.gov NCT02144519
References
- 1.Afterschool Alliance. America After 3 PM: A Household Survey on Afterschool in America. Washington, DC: Afterschool Alliance; 2014. [Google Scholar]
- 2.First lady announces two new commitments to healthy eating and physical activity afterschool. [ http://www.afterschoolalliance.org/afterschoolsnack/printPage.cfm?idBlog=6FD1B2AD-215A-A6B3-02AAB84B1F59DA3F; http://ahealthieramerica.org/media/news-releases/#5482,news]
- 3.Beets MW, Wallner M, Beighle A. Defining standards and policies for promoting physical activity in afterschool programs. Journal of School Health. 2010;80:411–417. doi: 10.1111/j.1746-1561.2010.00521.x. [DOI] [PubMed] [Google Scholar]
- 4.Moore JB, Program: Move More North Carolina Recommended Standards for After-School Physical Activity. Health Education and Behavior. 2009;36:637–639. doi: 10.1097/PHH.0b013e3181ca2634. [DOI] [PubMed] [Google Scholar]
- 5.Moore JB, Schneider L, Lazorick S, Shores KA, Beighle A, Jilcott SB, Newkirk J. Rationale and development of the Move More North Carolina: Recommended Standards for After-School Physical Activity. J Public Health Manag Pract. 2010;16:359–366. doi: 10.1097/PHH.0b013e3181ca2634. [DOI] [PubMed] [Google Scholar]
- 6.California Department of Education. California After School Physical Activity Guidelines. Sacramenta, CA: California Department of Education; 2009. p. 52. 52. [Google Scholar]
- 7.U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Washington, D.C.: U.S. Department of Health and Human Services; 2008. [Google Scholar]
- 8.Beets MW, Rooney L, Tilley F, Beighle A, Webster C. Evaluation of policies to promote physical activity in afterschool programs: are we meeting current benchmarks? Prev Med. 2010;51:299–301. doi: 10.1016/j.ypmed.2010.07.006. [DOI] [PubMed] [Google Scholar]
- 9.Beets MW, Shah R, Weaver RG, Huberty J, Beighle A, Moore JB. Physical Activity in Afterschool Programs: Comparison to Physical Activity Policies. J Phys Act Health. 2015;12:1–7. doi: 10.1123/jpah.2013-0135. [DOI] [PubMed] [Google Scholar]
- 10.Gortmaker SL, Lee RM, Mozaffarian RS, Sobol AM, Nelson TF, Roth BA, Wiecha JL. Effect of an After-School Intervention on Increases in Children’s Physical Activity. Med Sci Sports Exerc. 2012;44:450–457. doi: 10.1249/MSS.0b013e3182300128. [DOI] [PubMed] [Google Scholar]
- 11.Herrick H, Thompson H, Kinder J, Madsen KA. Use of SPARK to promote after-school physical activity. J Sch Health. 2012;82:457–461. doi: 10.1111/j.1746-1561.2012.00722.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Iversen CS, Nigg C, Titchenal CA. The impact of an elementary after-school nutrition and physical activity program on children’s fruit and vegetable intake, physical activity, and body mass index: Fun 5. Hawaii Med J. 2011;70:37–41. [PMC free article] [PubMed] [Google Scholar]
- 13.Nigg C, Battista J, Chang JA, Yamashita M, Chung R. Physical activity outcomes of a pilot intervention using SPARK active recreation in elementary after-school programs. Journal of Sport & Exercise Psychology. 2004;26:S144–S145. [Google Scholar]
- 14.Nigg CR, Geller K, Adams P, Hamada M, Hwang P, Chung R. Successful Dissemination of Fun 5: A Physical Activity and Nutrition Program for Children. Translational Behavioral Medicine. 2012;2:276–285. doi: 10.1007/s13142-012-0120-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Robinson TN, Matheson DM, Kraemer HC, Wilson DM, Obarzanek E, Thompson NS, Alhassan S, Spencer TR, Haydel KF, Fujimoto M, et al. A randomized controlled trial of culturally tailored dance and reducing screen time to prevent weight gain in low-income African American girls: Stanford GEMS. Arch Pediatr Adolesc Med. 2010;164:995–1004. doi: 10.1001/archpediatrics.2010.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sharpe EK, Forrester S, Mandigo J. Engaging Community Providers to Create More Active After-School Environments: Results From the Ontario CATCH Kids Club Implementation Project. J Phys Act Health. 2011;8(Suppl 1):S26–31. doi: 10.1123/jpah.8.s1.s26. [DOI] [PubMed] [Google Scholar]
- 17.Wilson DK, Van Horn ML, Kitzman-Ulrich H, Saunders R, Pate R, Lawman HG, Hutto B, Griffin S, Zarrett N, Addy CL, et al. Results of the “Active by Choice Today” (ACT) randomized trial for increasing physical activity in low-income and minority adolescents. Health Psychol. 2011;30:463–471. doi: 10.1037/a0023390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dzewaltowski DA, Rosenkranz RR, Geller KS, Coleman KJ, Welk GJ, Hastmann TJ, Milliken GA. HOP’N after-school project: an obesity prevention randomized controlled trial. Int J Behav Nutr Phys Act. 2010;7:90. doi: 10.1186/1479-5868-7-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gutin B, Yin Z, Johnson M, Barbeau P. Preliminary findings of the effect of a 3-year after-school physical activity intervention on fitness and body fat: The Medical College of Georgia Fitkid Project. International Journal Of Pediatric Obesity: IJPO: An Official Journal Of The International Association For The Study Of Obesity. 2008;3(Suppl 1):3–9. doi: 10.1080/17477160801896457. [DOI] [PubMed] [Google Scholar]
- 20.Yin Z, Moore JB, Johnson MH, Vernon MM, Gutin B. The impact of a 3-year after-school obesity prevention program in elementary school children. Child Obes. 2012;8:60–70. doi: 10.1089/chi.2011.0085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hastmann TJ, Bopp M, Fallon EA, Rosenkranz RR, Dzewaltowski DA. Factors Influencing the Implementation of Organized Physical Activity and Fruit and Vegetable Snacks in the HOP’N After-School Obesity Prevention Program. Journal of Nutrition Education and Behavior. 2013;45:60–68. doi: 10.1016/j.jneb.2012.06.005. [DOI] [PubMed] [Google Scholar]
- 22.Kelder S, Hoelscher DM, Barroso CS, Walker JL, Cribb P, Hu S. The CATCH Kids Club: a pilot after-school study for improving elementary students’ nutrition and physical activity. Public Health Nutrition. 2005;8:133–140. doi: 10.1079/phn2004678. [DOI] [PubMed] [Google Scholar]
- 23.Naylor PJ, Nettlefold L, Race D, Hoy C, Ashe MC, Wharf Higgins J, McKay HA. Implementation of school based physical activity interventions: a systematic review. Prev Med. 2015;72:95–115. doi: 10.1016/j.ypmed.2014.12.034. [DOI] [PubMed] [Google Scholar]
- 24.Beets MW, Glenn Weaver R, Turner-McGrievy G, Huberty J, Ward DS, Freedman DA, Saunders R, Pate RR, Beighle A, Hutto B, Moore JB. Making healthy eating and physical activity policy practice: the design and overview of a group randomized controlled trial in afterschool programs. Contemp Clin Trials. 2014;38:291–303. doi: 10.1016/j.cct.2014.05.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Beets MW, Weaver RG, Turner-McGrievy G, Huberty J, Ward DS, Pate RR, Freedman D, Hutto B, Moore JB, Beighle A. Making policy practice in afterschool programs: a randomized controlled trial on physical activity changes. Am J Prev Med. 2015;48:694–706. doi: 10.1016/j.amepre.2015.01.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bloom HS, Bos JM, Lee SW. Using cluster random assignment to measure program impacts. Statistical implications for the evaluation of education programs. Eval Rev. 1999;23:445–469. doi: 10.1177/0193841X9902300405. [DOI] [PubMed] [Google Scholar]
- 27.Murrary DM. Design and analysis of group-randomized trials. New York: Oxford University Press; 1998. [Google Scholar]
- 28.Webber LS, Catellier DJ, Lytle LA, Murray DM, Pratt CA, Young DR, Elder JP, Lohman TG, Stevens J, Jobe JB, et al. Promoting physical activity in middle school girls: Trial of Activity for Adolescent Girls. Am J Prev Med. 2008;34:173–184. doi: 10.1016/j.amepre.2007.11.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Stevens J, Murray DM, Catellier DJ, Hannan PJ, Lytele LA, Elder JP, Young DR, Simons-Morton DG, Webber LS. Design of the trial of activity in adolescent girls (TAAG) Contemporary Clinical Trials. 2005;26:223–233. doi: 10.1016/j.cct.2004.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cohen JFW, Richardson S, Austin SB, Economos CD, Rimm EB. School Lunch Waste Among Middle School Students Nutrients Consumed and Costs. American Journal of Preventive Medicine. 2013;44:114–121. doi: 10.1016/j.amepre.2012.09.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cohen JFW, Smit LA, Parker E, Austin SB, Frazier AL, Economos CD, Rimm EB. Long-Term Impact of a Chef on School Lunch Consumption: Findings from a 2-Year Pilot Study in Boston Middle Schools. Journal of the Academy of Nutrition and Dietetics. 2012;112:927–933. doi: 10.1016/j.jand.2012.01.015. [DOI] [PubMed] [Google Scholar]
- 32.Wansink B, Just DR, Hanks AS, Smith LE. Pre-Sliced Fruit in School Cafeterias Children’s Selection and Intake. American Journal of Preventive Medicine. 2013;44:477–480. doi: 10.1016/j.amepre.2013.02.003. [DOI] [PubMed] [Google Scholar]
- 33.Beets MW, Weaver RG, Moore JB, Turner-McGrievy G, Pate RR, Webster C, Beighle A. From Policy to Practice: Strategies to Meet Physical Activity Standards in YMCA Afterschool Programs. American Journal of Preventive Medicine. 2014;46:281–288. doi: 10.1016/j.amepre.2013.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Huberty JL, Beets MW, Beighle A, Balluff M. Movin After School: A community-based support for policy change in the afterschool environment. Childhood Obesity. 2010;6:337–341. [Google Scholar]
- 35.Beets MW, Webster C, Saunders R, Huberty JL. Translating policies into practice: a framework for addressing childhood obesity in afterschool programs. Health Promotion Practice. 2013;14:228–237. doi: 10.1177/1524839912446320. [DOI] [PubMed] [Google Scholar]
- 36.Israel BA, Schulz AJ, Parker EA, Becker AB. Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health. 1998;19:173–202. doi: 10.1146/annurev.publhealth.19.1.173. [DOI] [PubMed] [Google Scholar]
- 37.Collins LM, Murphy SA, Bierman KL. A conceptual framework for adaptive preventive interventions. Prev Sci. 2004;5:185–196. doi: 10.1023/b:prev.0000037641.26017.00. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Brazendale K, Chandler JL, Beets MW, Weaver RG, Beighle A, Huberty JL, Moore JB. Maximizing children’s physical activity using the LET US Play principles. Prev Med. 2015;76:14–19. doi: 10.1016/j.ypmed.2015.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Weaver RG, Hutto B, Saunders R, Moore JB, Turner-McGrievy G, Huberty J, Ward DS, Pate R, Beighle A, Freedman D, Beets MW. Making Healthy Eating and Physical Activity Policy Practice: Process evaluation of a group randomized controlled intervention targeting healthy eating and physical activity in afterschool programs. Health Education Research. 2015;30:849–865. doi: 10.1093/her/cyv052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Weaver RG, Moore JB, Huberty J, Freedman DA, Turner-McGrievy G, Beighle A, Ward DS, Pate R, Saunders R, Brazendale K, et al. Process Evaluation of Making HEPA Policy Practice: A Group Randomized Trial. Health Promotion Practice. doi: 10.1177/1524839916647331. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Beets MW, Huberty J, Beighle A. Physical Activity of Children Attending Afterschool Programs Research- and Practice-Based Implications. Am J Prev Med. 2012;42:180–184. doi: 10.1016/j.amepre.2011.10.007. [DOI] [PubMed] [Google Scholar]
- 42.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of Obesity and Trends in Body Mass Index Among US Children and Adolescents, 1999–2010. Jama-Journal of the American Medical Association. 2012;307:483–490. doi: 10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bailey RC, Olson J, Pepper SL, Porszaz J, Barstow TJ, Cooper DM. The level and tempo of children’s physical activities: An observational study. Med Sci Sports Exerc. 1995;27:1033–1041. doi: 10.1249/00005768-199507000-00012. [DOI] [PubMed] [Google Scholar]
- 44.Baquet G, Stratton G, Van Praagh E, Berthoin S. Improving physical activity assessment in prepubertal children with high-frequency accelerometry monitoring: a methodological issue. Preventive Medicine. 2007;44:143–147. doi: 10.1016/j.ypmed.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 45.Vale S, Santos R, Silva P, Soares-Miranda L, Mota J. Preschool children physical activity measurement: importance of epoch length choice. Pediatr Exerc Sci. 2009;21:413–420. doi: 10.1123/pes.21.4.413. [DOI] [PubMed] [Google Scholar]
- 46.Vale S, Silva P, Santos R, Soares-Miranda L, Mota J. Compliance with physical activity guidelines in preschool children. J Sports Sci. 2010;28:603–608. doi: 10.1080/02640411003702694. [DOI] [PubMed] [Google Scholar]
- 47.Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc. 2011;43:1360–1368. doi: 10.1249/MSS.0b013e318206476e. [DOI] [PubMed] [Google Scholar]
- 48.Kim Y, Beets MW, Pate RR, Blair SN. The effect of reintegrating Actigraph accelerometer counts in preschool children: Comparison using different epoch lengths. Journal of Science and Medicine in Sport. 2013;16:129–134. doi: 10.1016/j.jsams.2012.05.015. [DOI] [PubMed] [Google Scholar]
- 49.Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci. 2008;26:1557–1565. doi: 10.1080/02640410802334196. [DOI] [PubMed] [Google Scholar]
- 50.Matthews CE, Chen KY, Freedson PS, Buchowski MS, Beech BM, Pate RR, Troiano RP. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am J Epidemiol. 2008;167:875–881. doi: 10.1093/aje/kwm390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Trost SG, Rosenkranz RR, Dzewaltowski D. Physical activity levels among children attending after-school programs. Med Sci Sports Exerc. 2008;40:622–629. doi: 10.1249/MSS.0b013e318161eaa5. [DOI] [PubMed] [Google Scholar]
- 52.Geraci M, Bottai M. Linear quantile mixed models. Statistics and Computing. 2014;24:461–479. [Google Scholar]
- 53.Cradock AL, Barrett JL, Giles CM, Lee RM, Kenney EL, deBlois ME, Thayer JC, Gortmaker SL. Promoting Physical Activity With the Out of School Nutrition and Physical Activity (OSNAP) Initiative A Cluster-Randomized Controlled Trial. Jama Pediatrics. 2016;170:155–162. doi: 10.1001/jamapediatrics.2015.3406. [DOI] [PubMed] [Google Scholar]
- 54.Beets MW, Weaver RG, Turner-McGrievy G, Moore JB, Webster C, Brazendale K, Chandler J, Khan M, Saunders R, Beighle A. Are We There Yet? Compliance with Physical Activity Standards in YMCA Afterschool Programs. Child Obes. 2016 doi: 10.1089/chi.2015.0223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Sutherland R, Campbell E, Lubans DR, Morgan PJ, Okely AD, Nathan N, Wolfenden L, Wiese J, Gillham K, Hollis J, Wiggers J. ‘Physical Activity 4 Everyone’ school-based intervention to prevent decline in adolescent physical activity levels: 12 month (mid-intervention) report on a cluster randomised trial. Br J Sports Med. 2015 doi: 10.1136/bjsports-2014-094523. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Online Supplemental Figure 1. Minutes spent in moderate-to-vigorous physical activity for boys and girls by afterschool program across the three study measurement occasions (spring 2013, 2014, and 2015).