

Dear Sir,
The world population reached about 7 billion nowadays. Half of the world's population is female. At the same, 50 years and over aged women are living approximately more than 470 million women in the world. Twenty-five percent of women have severe postmenopausal symptoms, which can seriously affect a woman's quality of life. In worldwide, millions of women live 30% to 40% of their lifetimes after the menopause. Large population-based studies have estimated the mean or median age of natural menopause in western women as 50 to 52 years.1 The median age at menopause in Europe ranges from 50.1 to 52.8 years and in Asia from 42.1 to 49.5 years. Among Korean women, common (46.7%) menopausal age was around 46 to 50, but some of them (39%) were 51 to 55 years.2 The population of Mongolia reached 3 million last years with 12% of them being women aged 50 and over. Mean age at menopause of Mongolian women is 49.7 years.
The combination of high altitude and extreme weather in Mongolia requires the average Mongolian to consume a high protein diet and fatty red meat, in fact, it is the highest in Central Asia.3 Even red meat has the source of protein and essential nutrients but it may increase the risk of cardiovascular disease. Besides, a high number of cardiovascular diseases are causes of obesity woman of menopausal age and unbalanced diet. Menopause is a normal physiologic and biological process, which is defined by the absence of menstrual periods for 12 consecutive months. The changes associated with menopause and the perimenopause occur when ovarian function diminishes and ceases.4,5 Many of women aware of the symptom of menopause which includes hot flushes, sweats, depression and mood changes, sleep disturbance, musculoskeletal pain, vaginal dryness and decreased sexual function (Table 1).4 In Mongolia, the most reported symptom is hot flashes and night sweat same as the Korean woman.3 The hot flashes and night sweats which resolve spontaneously in time, in contrast, atrophic symptoms affecting the vagina and lower urinary track are often progressive and less likely to resolve without intervention. In early perimenopause, the prevalence of urogenital symptoms occurs 4%, rising to 25% one year after menopause and reaching to 47% three years after menopause which affecting sexual function and quality of women's life.6 Postmenopausal hormone therapy is the treatment of first choice of alleviate symptoms of estrogen deficiency.7 Besides, effectively relieving climacteric symptoms and can also protect against some chronic diseases, such as osteoporosis and colorectal cancer. In Mongolia, we have limited medication and therapies in this field. Therefore, complete treatment and/or curing the certain symptoms are the challenging issues here. Probably the cause of a present issue is associated with the Mongolian economic situation and the pharmacologic organization does not comply with international standards of health management guideline absolutely. In addition, the special features of our country such as diversity of the culture differences, the economy, the geography, and our lifestyle may also affect the discussing issues.
Table 1. Life style and postmenopausal symptoms.
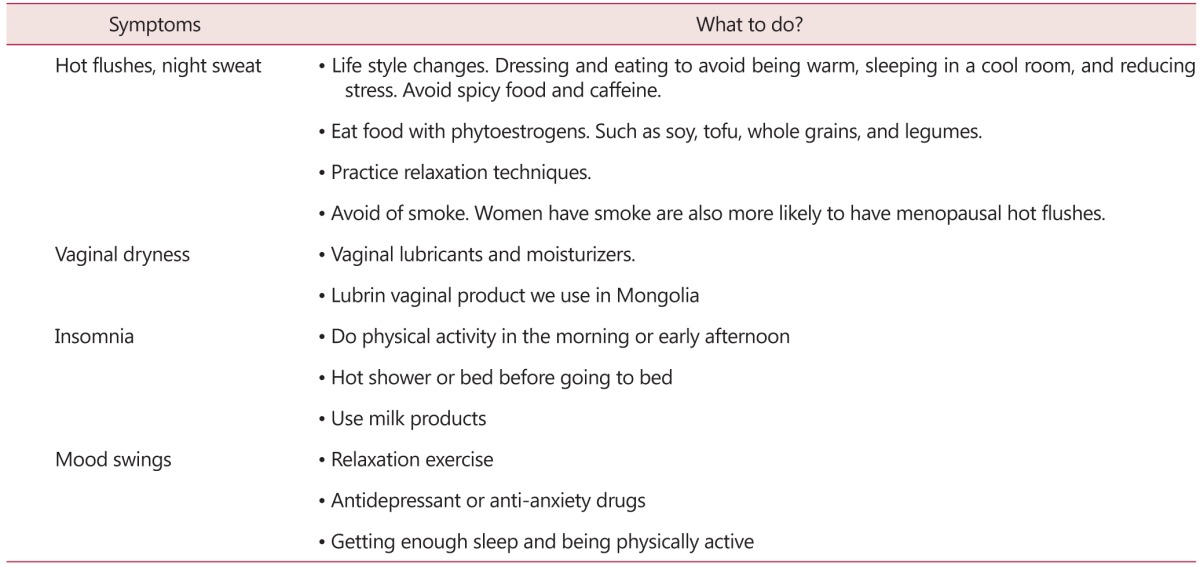
[Reprinted from " Menopause: diagnosis and management", by National Institute for Health and Care Excellence, 2015. Copyright 2015 by the National Institute for Health and Care Excellence. Reprinted with permission]
Whichever, we need to supply more appropriate medications and try to use the recommended therapies according to the international guidelines. It is important that information should be available to every woman so that they can make informed choices about their lifestyle around this time and potential treatments.4 Chae et al.2 showed us the most common menopausal symptom in Korean women was hot flushes and sweating. But most of the Korean women thought that menopausal symptom was aging process. Another Korean researcher conducted a research on the knowledge, attitude, symptoms and management of menopause in middle-aged women. They investigated that there is a significant correlation between the menopausal attitude and the management.8 Mongolian researchers investigated the relationship between serum follicle stimulating hormone (FSH), luteinizing hormone (LH) & estradiol levels and bone mineral density in postmenopausal 120 women which analyzed by enzyme-linked immunosorbent assay (ELISA). The results showed that when the woman getting older the mean serum estradiol level is decreased, in contrast, mean FSH and LH levels increased. Menopausal woman with estrogen receptor 1 (ER1) CC genotype is 2.7 hold the risk of osteoporosis.9
Menopausal hormone therapy is the broad term used to describe unopposed estrogen use (for women who have undergone hysterectomy) or combined estrogen-progestin therapy (EPT; for women with an intact uterus who need a progestin to prevent estrogen-associated endometrial hyperplasia.10 When systemic hormone therapy is needed to treat other menopausal symptoms, vaginal symptoms are generally satisfactorily resolved as well.11 Moreover, systemic hormone therapy may worsen or provoke stress incontinence.12,13 Hormone replacement therapy (HRT) should be recommended for the shortest period at the lowest dose. There are several ways that woman can take the hormone but in Mongolia taken orally is only approved. Rests of them are not occurred yet in Mongolian market and it is extremely limited now. HRT is important to woman avoid the fear of menopause symptoms.
Mongolian oriental medicine doctors prescribe traditional medicine. According to their theory, every illness is related to the kidney so all treatment includes the kidney medicine. Traditional medicine plants have their own ingredients and it is expressed by number after the drug name. For example Dashnamjil (bkra sis rnam rgyal), Sugmel-7, Sojed-11, Agar-35, Tanchen-25, Goyu-13. Early mentioned drugs are the mostly used in Mongolia.14
Presently, we mostly advise to women Premarin and Klimonorm estrogens to relieve the symptoms. Also, there are Tobolino and Clonidine, we use but not so often. Until last year, we just use copper intrauterine device (IUD) for preventing fertilization. But currently, we started to use hormonal IUD such as Mirena™. The non-hormonal drug, Klimafit 911 we use and this is herbal preparation which included in the group of homeopathic remedies that are used in the treatment of psycho-emotional disorders during menopause. Also, we use vitabiotics such as Menopause, and Osteocare liquid during the menopause. There are no reference data about all these medications. Only specialist doctors prescribe the medications.
In Mongolia, there is no proper guideline and management in menopausal women and there are have very few menopause specialists. Therefore, Mongolian Menopause and Andropause Society is working on the guideline and treatment plans based on international menopause society guidelines and standards, followed by setting up of a steady supply of HRT for health care services. In my opinion, the general knowledge of menopause and the postmenopausal syndrome in women is very low in Mongolia. Recently, diet, yoga and lifestyle widely publicized but very few women used to come for consultation and help. So we should provide more meaningful information by media, or lesson to improve woman's attitude, knowledge, behaviors and practice regarding the menopause. We need to communicate with government health agencies and proper organization to discuss treatment plans based on the standard and guidelines therapies.
Acknowledgement
This research was supported by High Value-added Food Technology development program, Ministry of agriculture, Food and Rural Affairs, Republic of Korea (114025-03-1-HD030).
Footnotes
Funding: This work was supported by the Soonchunhyang University Research Fund.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
References
- 1.Stanford JL, Hartge P, Brinton LA, Hoover RN, Brookmeyer R. Factors influencing the age at natural menopause. J Chronic Dis. 1987;40:995–1002. doi: 10.1016/0021-9681(87)90113-5. [DOI] [PubMed] [Google Scholar]
- 2.Chae HD, Choi SY, Cho EJ, Cho YM, Lee SR, Lee ES, et al. Awareness and experience of menopausal symptom and hormone therapy in korean postmenopausal women. J Menopausal Med. 2014;20:7–13. doi: 10.6118/jmm.2014.20.1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Unentsatsral L, Sukhee D, Tsogmaa B. Menopausal syndrome, hormone replacement therapy, prolactine hormone. Mongolian Med Sci. 2008;144:17–20. [Google Scholar]
- 4.National Institute for Health and Care Excellence. Menopause: diagnosis and management. London, UK: National Institute for Health and Care Excellence; 2015. [Cited by 2016 Feb 9]. Available from: https://www.nice.org.uk/guidance/ng23. [Google Scholar]
- 5.Avis NE, Crawford SL, Greendale G, Bromberger JT, Everson-Rose SA, Gold EB, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med. 2015;175:531–539. doi: 10.1001/jamainternmed.2014.8063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dennerstein L, Dudley EC, Hopper JL, Guthrie JR, Burger HG. A prospective population-based study of menopausal symptoms. Obstet Gynecol. 2000;96:351–358. doi: 10.1016/s0029-7844(00)00930-3. [DOI] [PubMed] [Google Scholar]
- 7.van der Mooren MJ, Kenemans P. Postmenopausal hormone therapy: impact on menopause-related symptoms, chronic disease and quality of life. Drugs. 2004;64:821–836. doi: 10.2165/00003495-200464080-00003. [DOI] [PubMed] [Google Scholar]
- 8.Kwak EK, Park HS, Kang NM. Menopause knowledge, attitude, symptom and management among midlife employed women. J Menopausal Med. 2014;20:118–125. doi: 10.6118/jmm.2014.20.3.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Unentsatsral L, Sarantuya J, Battogtokh Z. Correlation between reproductive hormonal level and osteoporosis among women in Mongolia. Cent Asian J Glob Health. 2015 doi: 10.5195/cajgh.2015.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.The North American Menopause Society. The 2012 hormone therapy position statement of: The North American Menopause Society. Menopause. 2012;19:257–271. doi: 10.1097/gme.0b013e31824b970a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kim HK, Kang SY, Chung YJ, Kim JH, Kim MR. The Recent Review of the Genitourinary Syndrome of Menopause. J Menopausal Med. 2015;21:65–71. doi: 10.6118/jmm.2015.21.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brown JS, Grady D, Ouslander JG, Herzog AR, Varner RE, Posner SF. Prevalence of urinary incontinence and associated risk factors in postmenopausal women Heart & Estrogen/Progestin Replacement Study (HERS) Research Group. Obstet Gynecol. 1999;94:66–70. doi: 10.1016/s0029-7844(99)00263-x. [DOI] [PubMed] [Google Scholar]
- 13.Hendrix SL, Cochrane BB, Nygaard IE, Handa VL, Barnabei VM, Iglesia C, et al. Effects of estrogen with and without progestin on urinary incontinence. JAMA. 2005;293:935–948. doi: 10.1001/jama.293.8.935. [DOI] [PubMed] [Google Scholar]
- 14.Oldokh S, Tserentsoo B, Bathuyag P. Mongolian traditional medicine. Ulaanbaatar: Bit Press; 2009. [Google Scholar]