

Abstract
Background
Gestational diabetes mellitus (GDM) occurs in 2–6 % of all pregnancies. We investigated whether area level deprivation is associated with a higher risk for GDM and whether GDM detection rates in deprived regions changed after the introduction of charge-free GDM screening in Germany in 2012.
Methods
We analyzed population-based data from Bavaria, Germany, comprising n = 587,621 deliveries in obstetric units between 2008 and 2014. Area level deprivation was assessed municipality-based using the Bavarian Index of Multiple Deprivation (BIMD), divided into quintiles and assigned to each mother based on her residential address. We estimated annual odds ratios (ORs) for GDM diagnosis by BIMD quintile with adjustment for maternal obesity, maternal age, migration background and single mother status.
Results
Women from the most deprived regions were less likely to be diagnosed with GDM before introduction of charge-free GDM screening (OR = 0.76 [95 % confidence interval: 0.66, 0.86] compared to least deprived areas), in 2008. In contrast, high area level deprivation was associated with significantly increased risk of GDM diagnosis in 2013 (OR [95 % confidence interval] = 1.15 [1.02, 1.29]). The OR was also elevated, although not significantly, in 2014 (OR [95 % confidence interval] = 1.05 [0.93, 1.18]).
Conclusions
The prevalence of GDM seems to have been underreported in women from highly deprived areas before introduction of the charge-free GDM screening in Germany. In fact, women living in deprived regions seem to have an increased risk for GDM and may profit from access to charge-free GDM screening.
Keywords: Gestational diabetes mellitus, Area level deprivation, Bavarian index of multiple deprivation, Charge-free screening
Background
Gestational diabetes mellitus (GDM) occurs in 2–6 % of all pregnancies in industrialized countries [1] with an increasing prevalence in recent years [2, 3]. In 2010, the World Health Organization (WHO) presented new diagnostic criteria for the classification of GDM [4] which Germany adopted in 2011. Based on the new criteria GDM was diagnosed if at least one of the values for fasting, 1-h, and 2-h plasma glucose concentration as measured in a 75-g oral glucose tolerance test exceeded diagnostic thresholds, while at least two elevated values were required for GDM diagnosis before 2011. Apart from that, every pregnant woman in Germany without pre-existing diabetes has been offered a charge-free GDM screening since 2012, whereas formerly the optional test had to be paid for by the mother.
Maternal obesity is the major risk factor for GDM [5] but there are also other potential determinants such as gestational weight gain, maternal age, parity, family history of diabetes, ethnicity or life-style habits [6–10]. At an area level, it was reported that living in neighbourhoods with a high prevalence of fast food restaurants was significantly associated with an increased risk of GDM [11]. Maternal socioeconomic status (SES) might be another potential risk factor. In general, SES can be assessed either at individual level (e. g. based on educational level) or from area-based socioeconomic measures such as deprivation indices. There have been a number of studies on the association between individual level SES and GDM, yielding inconsistent results [12]. The association of area level deprivation and GDM has been rarely investigated, however, and the sparse literature provided rather inconsistent results. While neighbourhood deprivation was not found to be associated with GDM risk in data from Southwest England, higher glucose values at GDM diagnosis were observed in Canadian women living in highly deprived areas [13, 14].
Interestingly, high area level deprivation has already been found to be associated with increased risk for obesity [15] and type 2 diabetes [16, 17], particularly in women [18].
Here, we had the opportunity to analyze a large population-based dataset from Bavaria, Germany, which allowed investigating the association between area level deprivation and GDM risk. Additionally, we were able to assess the impact of the introduction of a charge-free GDM screening [19] on this association.
Methods
Data were extracted from a standard dataset regularly collected for national benchmarking of obstetric units in terms of clinical performance. The BAQ (Bayerische Arbeitsgemeinschaft für Qualitätssicherung - Bavarian Institute for Quality Assurance in hospital care) conducts corresponding regional evaluations for Bavaria, Germany. Data are transferred electronically to the BAQ office after personally identifying characteristics have been removed and replaced by an anonymous unique reference number. Amongst others, these data contain information on maternal age, weight and height, postal code of the mother’s residential address, GDM, and pre-gestational diabetes as previously described [20, 21]. GDM was diagnosed by the women’s gynaecologists who are assumed to follow the official guidelines from the German Diabetes Association. These guidelines were revised in 2011 following the WHO’s new diagnostic criteria [4]. Information on maternal weight and gestational age at first prenatal care visit was extracted by midwives and nurses from the mother’s pregnancy booklet (issued to every pregnant woman in Germany for complete documentation of all antenatal care visits) and augmented with additional information upon hospital admission. Mother’s height and weight recorded at first visit (median gestational age: 8 completed weeks) were used to derive her body mass index (BMI). The BAQ data do not contain variables on individual level SES apart from fairly rough surrogates such as smoking during pregnancy or migration background.
We assessed area level deprivation using the Bavarian Index of Multiple Deprivation (BIMD) [22] derived from official statistics and methods used in the UK for assessment of regional deprivation [23]. The BIMD including seven subdomains of deprivation (income, employment, education, municipal revenue, social capital, environment, security) was computed for all 2,056 Bavarian municipalities. We categorized the municipalities by BIMD quintiles, with the first quintile designating the least deprived and the fifth quintile the most deprived municipalities. Assignment of BIMD quintile to each mother was done based on postal code of her residential address.
According to current German maternity guidelines established in 2012, every pregnant woman without pre-existing diabetes is offered a glucose-challenge test between the 24th and 27th gestational week. In a second step, women with increased glucose values in the glucose-challenge test will be tested by an oral glucose tolerance test for diagnosis of GDM. The charges of this two-step procedure are now fully covered by the women’s health insurance, whereas formerly the test had to be paid for by the mother. To compare periods before and after its introduction we considered the data of all deliveries in Bavarian obstetric units from 2008 to 2014 (n = 645,774). Of these, 4,564 women with known pre-gestational diabetes were excluded. The BIMD could not be assigned to a further 53,589 women because the postal codes of their residential addresses referred to a location outside Bavaria or were missing, thus leaving a final sample size of n = 587,621. We used logistic regression to estimate odds ratios (ORs) and corresponding 95 % confidence intervals (CIs) with GDM as the outcome variable and BIMD quintiles as the explanatory variable (lowest deprivation as reference) separately for each year from 2008 to 2014. All models were calculated both crude and adjusted for maternal obesity (BMI ≥ 30 kg/m2) at first visit, maternal age (<35 compared to ≥ 35 years), migration background and single mother status, as these were significant predictors in unadjusted analyses. Likewise we assessed associations between GDM and all subdomains of the BIMD (as a continuous variable).
Statistical analyses were performed with SAS (version 9.3, SAS Institute Inc., Cary, NC, USA) and R (version 3.0.3, https://cran.r-project.org).
Results
The proportion of women with a diagnosis of GDM increased from 3.4 % in 2008 to 4.0 % in 2014 (Table 1), resulting in a relative increase in prevalence of about 17 %. Maternal obesity, age, migration background and single mother status were significantly associated with GDM in both 2008 and 2014 (p < 0.05), while smoking during pregnancy and parity (multiparous compared to primiparous) were not (data not shown). In contrast to GDM, the relative increase in prevalence for any of these factors was 11 % (as observed for obesity) or lower.
Table 1.
Description of the study population in 2008 and 2014
| Year 2008 (n = 81,129) | Year 2014 (n = 92,589) | |
|---|---|---|
| Gestational diabetes mellitus | n = 2,745 (3.4 %) | n = 3,682 (4.0 %) |
| Obese (BMI > 30 kg/m2) | n = 8,819 (10.9 %) | n = 11,169 (12.1 %) |
| Age > 35 years | n = 21,163 (26.1 %) | n = 25,615 (27.7 %) |
| Migration background | n = 14,401 (17.8 %) | n = 17,772 (19.2 %) |
| Single mother | n = 7,731 (9.9 %) | n = 6,864 (8.2 %) |
| Multiparous woman | n = 40,635 (50.1 %) | n = 45,219 (48.8 %) |
| Smoking during pregnancy | n = 5,457 (6.7 %) | n = 4,262 (4.6 %) |
| BIMD quintile 1 (least deprived) | n = 10,306 (12.7 %) | n = 12,716 (13.7 %) |
| BIMD quintile 2 | n = 9,679 (11.9 %) | n = 10,329 (11.2 %) |
| BIMD quintile 3 | n = 23,948 (29.5 %) | n = 27,831 (30.1 %) |
| BIMD quintile 4 | n = 13,198 (16.3 %) | n = 14,829 (16.0 %) |
| BIMD quintile 5 (most deprived) | n = 23,998 (29.6 %) | n = 26,884 (29.0 %) |
BIMD Bavarian Index of Multiple Deprivation
The rate of GDM diagnosis increased in 2011, when the new definition was established in Germany, in all BIMD quintiles and dropped slightly in 2012 when the universal two-step GDM screening was introduced (Fig. 1). However, the GDM prevalence remained at a considerably higher level compared to before 2011 in women from deprived areas, but not in women from regions with low level deprivation. Women from the most deprived areas were less likely to be diagnosed with GDM in 2008 (OR [95 % CI] = 0.76 [0.66, 0.86] for the fifth quintile compared to the first quintile in adjusted analyses, Table 2). In contrast, a higher area level deprivation was significantly associated with increased risk of GDM diagnosis in 2013 (OR [95 % CI] = 1.15 [1.02, 1.29] for the fifth quintile compared to the first quintile). The OR was also elevated, although not significantly, in 2014 (OR [95 % CI] = 1.05 [0.93, 1.18]). Further analyses suggested that these trends over time were at least partly based on changes in areas with low employment rates, as employment deprivation was the only BIMD subdomain associated with both lower GDM risk by trend in 2008 (OR [95 % CI] = 0.98 [0.94, 1.02]) and significantly higher risk in 2014 (OR [95 % CI] = 1.05 [1.02, 1.09], Table 3).
Fig. 1.
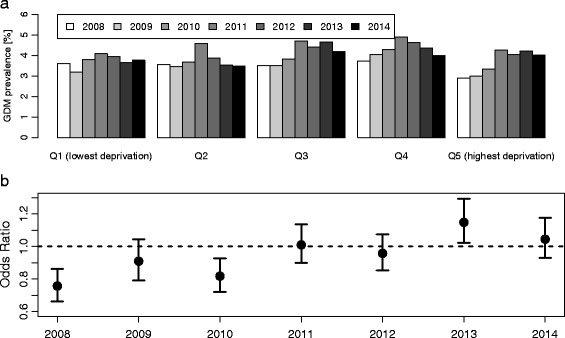
Yearly rates of gestational diabetes mellitus (GDM) diagnoses from 2008 to 2014 (numbers of pregnancies without pre-gestational diabetes in brackets) in Bavaria, Germany, by deprivation quintiles (Q1-Q5, plot a), and yearly odds ratios with corresponding 95 % confidence intervals for Q5 compared to reference Q1 (plot b, all estimates adjusted for maternal obesity, age, migration background and single mother status). In 2011, the criteria for GDM diagnosis were revised in Germany following WHO recommendations. In 2012, charge-free GDM screening, following a two-step procedure, was established in Germany
Table 2.
Odds ratios [95 % confidence intervals] for gestational diabetes mellitus by Bavarian Index of Multiple Deprivation (BIMD) quintile in 2008 and 2014 (based on n = 81,129 and n = 92,589 observations, respectively) as categorical variables, and by maternal obesity, age, migration background and single mother status, both crude and mutually adjusted
| BIMD | 2008, crude | 2008, adjusted | 2014, crude | 2014, adjusted |
|---|---|---|---|---|
| Quintile 1 (least deprived) | Reference | Reference | Reference | Reference |
| Quintile 2 | 0.99 [0.85, 1.15] | 0.99 [0.85, 1.15] | 0.92 [0.80, 1.06] | 0.93 [0.81, 1.08] |
| Quintile 3 | 0.97 [0.86, 1.10] | 0.92 [0.81, 1.04] | 1.12 [1.001, 1.24] | 1.07 [0.95, 1.20] |
| Quintile 4 | 1.04 [0.90, 1.19] | 1.01 [0.88, 1.16] | 1.06 [0.94, 1.20] | 1.09 [0.96, 1.24] |
| Quintile 5 (most deprived) | 0.79 [0.70, 0.90] | 0.76 [0.66, 0.86] | 1.07 [0.96, 1.19] | 1.05 [0.93, 1.18] |
| Maternal obesity | 3.07 [2.81, 3.35] | 3.19 [2.92, 3.49] | 3.53 [3.28, 3.80] | 3.71 [3.43, 4.00] |
| Maternal age ≥35 years | 1.54 [1.42, 1.67] | 1.56 [1.44, 1.69] | 1.64 [1.53, 1.75] | 1.69 [1.57, 1.82] |
| Migration background | 1.44 [1.32, 1.56] | 1.52 [1.39, 1.67] | 1.60 [1.49, 1.71] | 1.68 [1.55, 1.82] |
| Single mother status | 1.56 [1.34, 1.81] | 1.46 [1.25, 1.71] | 1.31 [1.14, 1.50] | 1.27 [1.10, 1.46] |
Significant associations (p < 0.05) are shown in bold face
Table 3.
Odds ratios [95 % confidence intervals] for gestational diabetes mellitus by Bavarian Index of Multiple Deprivation (BIMD) domains in 2008 and 2014 (based on n = 81,129 and n = 92,589 observations, respectively), both crude and adjusted for maternal obesity, age, migration background and single mother status
| BIMD domain | 2008, crude | 2008, adjusted | 2014, crude | 2014, adjusted |
|---|---|---|---|---|
| Income deprivation | 0.84 [0.80, 0.87] | 0.84 [0.80, 0.88] | 0.91 [0.88, 0.95] | 0.92 [0.89, 0.96] |
| Employment deprivation | 1.00 [0.96, 1.04] | 0.98 [0.94, 1.02] | 1.07 [1.03, 1.10] | 1.05 [1.02, 1.09] |
| Educational deprivation | 0.88 [0.84, 0.91] | 0.88 [0.84, 0.91] | 0.97 [0.94, 1.003] | 0.98 [0.94, 1.01] |
| Municipal revenue deprivation | 0.92 [0.88, 0.96] | 0.93 [0.89, 0.97] | 0.94 [0.91, 0.97] | 0.96 [0.93, 0.999] |
| Social capital deprivation | 0.87 [0.83, 0.90] | 0.88 [0.84, 0.91] | 0.97 [0.93, 0.999] | 0.99 [0.95, 1.02] |
| Environment deprivation | 1.10 [1.06, 1.14] | 1.08 [1.03, 1.12] | 1.11 [1.08, 1.15] | 1.08 [1.04, 1.12] |
| Security deprivation | 1.09 [1.05, 1.13] | 1.08 [1.04, 1.12] | 1.06 [1.03, 1.10] | 1.06 [1.02, 1.10] |
Significant associations (p < 0.05) are shown in bold face
Discussion
Our data show that area level deprivation is associated with GDM prevalence in a subtle way: Women from highly deprived areas were less likely to be diagnosed with GDM than women from less deprived regions before introduction of the charge-free GDM screening, but vice versa after 2012.
Hence, it appears likely that GDM was largely underreported in women from deprived areas before 2012. We therefore assume that living in deprived regions, especially with high unemployment rates, is indeed associated with a slightly increased risk for GDM as observed in our data from 2013 (significantly) and 2014 (not significantly). This is in accordance with previous studies related to type 2 diabetes [16–18]. Our findings further indicate that particularly women from deprived areas may profit from charge-free GDM screening. Although the screening fees were only about 10–25 €, we assume that this may already have constituted a financial barrier for an unemployed single woman in Germany receiving state benefits of only 364 € (“Hartz IV”) monthly in 2011. This would agree well with findings from other studies, indicating that especially people with low SES tended to avoid or delay physician visits after a practice charge for physicians (10 € per calendar quarter) was introduced in Germany in 2004 [24], and that financial barriers may be relevant for participation in colorectal cancer screening [25, 26].
In general, the trends of GDM prevalence in our data appear plausible, although they could only partly be explained by concomitant increases in the prevalence of risk factors such as maternal obesity or increased maternal age. Indeed, we observed an increase in the prevalence of both risk factors in our data, which is in line with long-term temporal trends in Germany [27, 28]. However, we think that it appears likely that the marked increase in GDM prevalence in 2011 in our data was due to the revision of the GDM diagnosis criteria in Germany in the same year, which may have particularly improved the detection of milder GDM cases (as only one instead of two elevated blood glucose values was deemed sufficient for GDM diagnosis). The lower prevalence in the following years may be due to introduction of the glucose-challenge pre-test in 2012, which is known to miss about 20 % of all GDM cases [29]. Interestingly, we observed almost no such decrease in prevalence in women from mostly deprived areas, possibly indicating that the introduction of charge-free screening levelled out the numbers missed by pre-testing in this subgroup. We are, however, hesitant to overinterpret GDM prevalence rates from 2011 and 2012, as changes introduced in these years may not have been immediately adopted by physicians [30] thus possibly leading to regional differences in this respect. Unfortunately, we are not aware of any other study reporting temporal trends of GDM prevalence in Germany before and after 2011–2012 to support our assumptions.
A major strength of the presented results is seen in the large number of pregnancies available for analysis. However, the data were collected for purposes not related to the study hypothesis. Data quality is high as completeness of the data is monitored annually across obstetric units as an integral part of benchmarking health-care provision: The BAQ, providing the data for our study, is part of an established national program to generate annual statistics depicting an individual obstetric units’ deviations from national targets. This program has been run within all federal states over the last three decades. Quality assurance data from the UK and the USA have similarly been analysed in other studies on determinants of pregnancy outcomes [31–35].
Unfortunately, the BAQ data do not contain a valid indicator of the mother’s SES so that we were not able to distinguish between the associations of individual and area level deprivation on GDM prevalence. It should further be noted that the BIMD quintiles were calculated based on the number of municipalities, as opposed to the population size of each municipality. Therefore, the proportions of pregnant women were not equally distributed across BIMD quintile. This was similar to previous studies [17, 18], however, and we do not think that this might constitute a potential source of severe bias.
In summary, our findings indicate that women living in highly deprived areas have a higher risk of developing GDM, and that even moderate charges may constitute an obstacle for participation in GDM screening. Thus, access to charge-free GDM screening and to appropriate treatment may be an important step towards more equality in pregnancy-related health care.
Acknowledgments
Funding
The work was supported by grants from the Kompetenznetz Diabetes mellitus (Competence Network for Diabetes mellitus), funding from the German Federal Ministry of Education and Research (BMBF) to the German Center for Diabetes Research (DZD e.V.), and by iMed–the Helmholtz Initiative on Personalized Medicine.
The funders had no impact on design, conduct and reporting of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Availability of data and materials
Upon request, the BAQ can offer onsite-access to external researchers to the data analyzed at the BAQ office in Munich, Germany.
Authors’ contributions
The authors’ responsibilities were as follows: AB (guarantor) formulated the study hypothesis together with WM, performed the statistical analyses and contributed to the first and final draft of the manuscript. DK, AGZ, NL and WM contributed to interpretation of the study results and to the first and final draft of the manuscript. NL was responsible for provision and interpretation of the data.
Competing interests
Nothing to declare.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethics approval or informed consent of patients was not necessary because this was a secondary analysis of anonymous routine data.
Abbreviations
- BAQ
Bayerische Arbeitsgemeinschaft für Qualitätssicherung
- BIMD
Bavarian index of multiple deprivation
- BMI
Body mass index
- CI
Confidence interval
- GDM
Gestational diabetes mellitus
- OR
Odds ratio
- SES
Socioeconomic status
- WHO
World Health Organization
References
- 1.American Diabetes Association Standards of medical care in diabetes--2011. Diabetes Care. 2011;34(Suppl 1):S11–61. doi: 10.2337/dc11-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Poston L. Maternal obesity, gestational weight gain and diet as determinants of offspring long term health. Best Pract Res Clin Endocrinol Metab. 2012;26(5):627–639. doi: 10.1016/j.beem.2012.03.010. [DOI] [PubMed] [Google Scholar]
- 3.Dabelea D, Snell-Bergeon JK, Hartsfield CL, Bischoff KJ, Hamman RF, McDuffie RS, Kaiser Permanente of Colorado GDMSP Increasing prevalence of gestational diabetes mellitus (GDM) over time and by birth cohort: Kaiser Permanente of Colorado GDM Screening Program. Diabetes Care. 2005;28(3):579–584. doi: 10.2337/diacare.28.3.579. [DOI] [PubMed] [Google Scholar]
- 4.Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, Dyer AR, Leiva A, Hod M, Kitzmiler JL, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi: 10.2337/dc09-1848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Farren M, Daly N, O’Higgins AC, McKeating A, Maguire PJ, Turner MJ. The interplay between maternal obesity and gestational diabetes mellitus. J Perinat Med. 2015;43(3):311–317. doi: 10.1515/jpm-2014-0272. [DOI] [PubMed] [Google Scholar]
- 6.Cleary-Goldman J, Malone FD, Vidaver J, Ball RH, Nyberg DA, Comstock CH, Saade GR, Eddleman KA, Klugman S, Dugoff L, et al. Impact of maternal age on obstetric outcome. Obstet Gynecol. 2005;105(5 Pt 1):983–990. doi: 10.1097/01.AOG.0000158118.75532.51. [DOI] [PubMed] [Google Scholar]
- 7.Savitz DA, Janevic TM, Engel SM, Kaufman JS, Herring AH. Ethnicity and gestational diabetes in New York City, 1995–2003. BJOG. 2008;115(8):969–978. doi: 10.1111/j.1471-0528.2008.01763.x. [DOI] [PubMed] [Google Scholar]
- 8.Cypryk K, Szymczak W, Czupryniak L, Sobczak M, Lewinski A. Gestational diabetes mellitus - an analysis of risk factors. Endokrynol Pol. 2008;59(5):393–397. [PubMed] [Google Scholar]
- 9.Hedderson MM, Gunderson EP, Ferrara A. Gestational weight gain and risk of gestational diabetes mellitus. Obstet Gynecol. 2010;115(3):597–604. doi: 10.1097/AOG.0b013e3181cfce4f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ruiz-Gracia T, Duran A, Fuentes M, Rubio MA, Runkle I, Carrera EF, Torrejon MJ, Bordiu E, Valle LD, Garcia de la Torre N, et al. Lifestyle patterns in early pregnancy linked to gestational diabetes mellitus diagnoses when using IADPSG criteria. The St Carlos gestational study. Clin Nutr. 2016;35(3):699–705. doi: 10.1016/j.clnu.2015.04.017. [DOI] [PubMed] [Google Scholar]
- 11.Kahr MK, Suter MA, Ballas J, Ramin SM, Monga M, Lee W, Hu M, Shope CD, Chesnokova A, Krannich L, et al. Geospatial Analysis of Food Environment Demonstrates Associations with Gestational Diabetes. Am J Obstet Gynecol. 2016;214(1):110.e1–9. [DOI] [PMC free article] [PubMed]
- 12.Dode MA, dos Santos IS. Non classical risk factors for gestational diabetes mellitus: a systematic review of the literature. Cad Saude Publica. 2009;25(Suppl 3):S341–359. doi: 10.1590/s0102-311x2009001500002. [DOI] [PubMed] [Google Scholar]
- 13.Janghorbani M, Stenhouse EA, Jones RB, Millward BA. Is neighbourhood deprivation a risk factor for gestational diabetes mellitus? Diabet Med. 2006;23(3):313–317. doi: 10.1111/j.1464-5491.2006.01774.x. [DOI] [PubMed] [Google Scholar]
- 14.Sampson L, Dasgupta K, Ross NA. The association between socio-demographic marginalization and plasma glucose levels at diagnosis of gestational diabetes. Diabet Med. 2014;31(12):1563–1567. doi: 10.1111/dme.12529. [DOI] [PubMed] [Google Scholar]
- 15.Heslehurst N. Identifying ‘at risk’ women and the impact of maternal obesity on National Health Service maternity services. Proc Nutr Soc. 2011;70(4):439–449. doi: 10.1017/S0029665111001625. [DOI] [PubMed] [Google Scholar]
- 16.Maier W, Holle R, Hunger M, Peters A, Meisinger C, Greiser KH, Kluttig A, Volzke H, Schipf S, Moebus S, et al. The impact of regional deprivation and individual socio-economic status on the prevalence of Type 2 diabetes in Germany. A pooled analysis of five population-based studies. Diabet Med. 2013;30(3):e78–86. doi: 10.1111/dme.12062. [DOI] [PubMed] [Google Scholar]
- 17.Grundmann N, Mielck A, Siegel M, Maier W. Area deprivation and the prevalence of type 2 diabetes and obesity: analysis at the municipality level in Germany. BMC Public Health. 2014;14:1264. doi: 10.1186/1471-2458-14-1264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Maier W, Scheidt-Nave C, Holle R, Kroll LE, Lampert T, Du Y, Heidemann C, Mielck A. Area level deprivation is an independent determinant of prevalent type 2 diabetes and obesity at the national level in Germany. Results from the National Telephone Health Interview Surveys 'German Health Update' GEDA 2009 and 2010. Plos One. 2014;9(2):e89661. doi: 10.1371/journal.pone.0089661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kleinwechter H, Schäfer-Graf U, Bührer C, Hoesli I, Kainer F, Kautzky-Willer A, Pawlowski B, Schunck K, Somville T, Sorger M, et al. Gestational diabetes mellitus (GDM) diagnosis, therapy and follow-up care: Practice Guideline of the German Diabetes Association (DDG) and the German Association for Gynaecologyand Obstetrics (DGGG) Exp Clin Endocrinol Diabetes. 2014;122(7):395–405. doi: 10.1055/s-0034-1366412. [DOI] [PubMed] [Google Scholar]
- 20.Beyerlein A, Lack N, von Kries R. Within-population average ranges compared with institute of medicine recommendations for gestational weight gain. Obstet Gynecol. 2010;116(5):1111–1118. doi: 10.1097/AOG.0b013e3181f1ad8b. [DOI] [PubMed] [Google Scholar]
- 21.Beyerlein A, Schiessl B, Lack N, von Kries R. Associations of gestational weight loss with birth-related outcome: a retrospective cohort study. BJOG. 2011;118(1):55–61. doi: 10.1111/j.1471-0528.2010.02761.x. [DOI] [PubMed] [Google Scholar]
- 22.Maier W, Fairburn J, Mielck A. Regional deprivation and mortality in Bavaria. Development of a community-based index of multiple deprivation. Gesundheitswesen. 2012;74(7):416–425. doi: 10.1055/s-0031-1280846. [DOI] [PubMed] [Google Scholar]
- 23.Noble M, Wright G, Smith G, Dibben C. Measuring multiple deprivation at the small-area level. Environ Plan A. 2006;38(1):169–185. doi: 10.1068/a37168. [DOI] [Google Scholar]
- 24.Rückert IM, Böcken J, Mielck A. Are German patients burdened by the practice charge for physician visits ('Praxisgebuehr')? A cross sectional analysis of socio-economic and health related factors. BMC Health Serv Res. 2008;8:232. doi: 10.1186/1472-6963-8-232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Klabunde CN, Vernon SW, Nadel MR, Breen N, Seeff LC, Brown ML. Barriers to colorectal cancer screening: a comparison of reports from primary care physicians and average-risk adults. Med Care. 2005;43(9):939–944. doi: 10.1097/01.mlr.0000173599.67470.ba. [DOI] [PubMed] [Google Scholar]
- 26.Green AR, Peters-Lewis A, Percac-Lima S, Betancourt JR, Richter JM, Janairo MP, Gamba GB, Atlas SJ. Barriers to screening colonoscopy for low-income Latino and white patients in an urban community health center. J Gen Intern Med. 2008;23(6):834–840. doi: 10.1007/s11606-008-0572-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Scholz R, Voigt M, Schneider KT, Rochow N, Hagenah HP, Hesse V, Straube S. Analysis of the German perinatal survey of the years 2007–2011 and comparison with data from 1995–1997: maternal characteristics. Geburtshilfe Frauenheilkd. 2013;73(12):1247–1251. doi: 10.1055/s-0033-1350830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mensink GB, Schienkiewitz A, Haftenberger M, Lampert T, Ziese T, Scheidt-Nave C. Overweight and obesity in Germany: results of the German health interview and examination survey for adults (DEGS1) Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013;56(5–6):786–794. doi: 10.1007/s00103-012-1656-3. [DOI] [PubMed] [Google Scholar]
- 29.Naylor CD, Sermer M, Chen E, Farine D. Selective screening for gestational diabetes mellitus. Toronto Trihospital Gestational Diabetes Project Investigators. N Engl J Med. 1997;337(22):1591–1596. doi: 10.1056/NEJM199711273372204. [DOI] [PubMed] [Google Scholar]
- 30.Görig T, Schneider S, Bock C, Maul H, Kleinwechter H, Diehl K. Screening for gestational diabetes mellitus in Germany: a qualitative study on pregnant womens attitudes, experiences, and suggestions. Midwifery. 2015;31(11):1026–1031. doi: 10.1016/j.midw.2015.07.001. [DOI] [PubMed] [Google Scholar]
- 31.Park S, Sappenfield WM, Bish C, Salihu H, Goodman D, Bensyl DM. Assessment of the Institute of Medicine Recommendations for Weight Gain During Pregnancy: Florida, 2004–2007. Maternal Child Health J. 2011;15(3):289–301. [DOI] [PubMed]
- 32.Donahue SM, Kleinman KP, Gillman MW, Oken E. Trends in birth weight and gestational length among singleton term births in the United States: 1990–2005. Obstet Gynecol. 2010;115(2 Pt 1):357–364. doi: 10.1097/AOG.0b013e3181cbd5f5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Khashan AS, Kenny LC. The effects of maternal body mass index on pregnancy outcome. Eur J Epidemiol. 2009;24(11):697–705. doi: 10.1007/s10654-009-9375-2. [DOI] [PubMed] [Google Scholar]
- 34.Bhattacharya S, Campbell DM, Liston WA. Effect of body mass index on pregnancy outcomes in nulliparous women delivering singleton babies. BMC Public Health. 2007;7:168. doi: 10.1186/1471-2458-7-168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bodnar LM, Siega-Riz AM, Simhan HN, Himes KP, Abrams B. Severe obesity, gestational weight gain, and adverse birth outcomes. Am J Clin Nutr. 2010;91(6):1642–48. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Upon request, the BAQ can offer onsite-access to external researchers to the data analyzed at the BAQ office in Munich, Germany.