

Abstract
Objectives:
To describe the family profile of child abuse and neglect (CAN) subjects in Saudi Arabia.
Methods:
Data were collected retrospectively between July 2009 and December 2013 from patients’ files, which were obtained from the Child Protection Centre (CPC) based in King Abdulaziz Medical City, Riyadh, Saudi Arabia. Four main sets of variables were examined: demographics of victim, family profile, parental information, and information on perpetrator and forms of abuse.
Results:
The charts of 220 CAN cases were retrospectively reviewed. Physical abuse was the most common form of abuse (42%), followed by neglect (39%), sexual abuse (14%), and emotional abuse (4%). Children with unemployed fathers were 2.8 times as likely to experience physical abuse. Children living in single/step-parent households were 4 times as likely to experience physical abuse. Regarding neglect children living in larger households (≥6) were 1.5 times as likely to be neglected by their parents as were children living in smaller households (<6). Regarding sexual abuse, male children were 2.9 times as likely to be abused as were female children.
Conclusions:
The recent acknowledgment of CAN as a public health problem in Saudi Arabia suggests that time will be needed to employ effective and culturally sensitive prevention strategies based on family risk factors.
Child maltreatment (CM) is a universal problem with significant consequences for children, families, and communities. According to the public health approach, CM is preventable through identifications of its roots and implementation of effective solutions and prevention programs rather than simply reacting to it occurrence. In a 2002 report, the World Health Organization (WHO) described the roots of CM as a complex interplay of individual, relationship, community, societal, cultural, and environmental factors. Although some risk factors are likely unique to a particular type of CM, the various types of CM share a number of risk factors, particularly those related to the family. Numerous studies have examined the characteristics of families and various other factors that could compromise parenting practices; thus, predisposing children to child abuse and neglect (CAN). Exposure to violence at home is major factor, which has been found to be associated with being a victim, or perpetrator of abuse in adulthood.1 Other factors that may possibly contribute to CAN include parents’ age and level of education, family size and structure, single parenting and divorce, and the presence of illness and disability within the household.2-5 One study examined CAN in blended households, or households wherein a non-related parental figure resides, and concluded that the risk of physical and sexual abuse is higher compared with other household types.6 Several studies in the Middle East have confirmed similar familial factors that predispose families to CAN. A study conducted in Kuwait highlighted that students of divorced parents had higher scores on measures of psychological and physical abuse.7 In the Kingdom of Saudi Arabia (KSA) in 2013, Al-Eissa et al8 conducted a prevalence study of adolescents’ exposure to violence and maltreatment by adult caregivers in the home using the International Society for the Prevention of Child Abuse and Neglect (ISPCAN) screening tool-child (home version). They found that adolescents experienced significantly greater rates of all types of violence/maltreatment when they lived with their mother, or father only (versus with both), and even greater rates were observed when they lived in a blended household.8 Nonetheless, some have argued that the exact connection between family profile and CAN has not received the necessary attention in the pediatric literature and thus requires further exploration.9 To fully understand the etiology of CAN in the KSA, professionals must focus on the unique dynamics of the family structures and values in the country, with a particular focus on the context in which CAN is most likely to occur. However, we have little knowledge of such context in the KSA, research on the family profile of abused children in the KSA is scarce, making it an area in urgent need of exploration. In the present study, we describe the family profiles of CAN cases in the KSA, particularly in terms of family size, parents’ employment status, marital status, and age and the children’s relationship to the perpetrator.
Methods
Cases of CAN evaluated by the Child Protection Centre (CPC) at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia, were included in this study. King Abdulaziz Medical City, Riyadh is a National Guard health facility that provides health care services to the National Guard soldiers, officers, employees, and their families. The total served population is approximately 100,000, and the CPC evaluates between 60 and 90 potential CAN cases per year. The CPC is considered one of the largest, oldest, and most established centers in the country, and thus, it facilitates a larger study sample. Only those cases involving children <18 years of age who were evaluated by the CPC between July 2009 and December 2013 were included in the final analysis. Other inclusion criteria included having at least 80% of the demographic, parents, and perpetrator data available. Missing data in the file were excluded from the analysis.
Scientific and ethical approval was obtained from the Scientific Research Committee, King Abdullah International Medical Research Center, Riyadh, Saudi Arabia, which also approved the subsequent amendments for the researcher to access the patients’ files.
Procedures
Data were collected retrospectively from the case files of the CPC. Initially, data was extracted from the electronic National Family Safety Registry (NFSR). However, some of the required information was missing from the NFSR, adjustments had to be made to obtain necessary information for all eligible cases. We also performed chart reviews to supplement the data from the registry. Overall, 220 cases registered in the NFSR between 2009 and 2013 and completed data in the chart were included in the final analysis.
A number of steps were taken to ensure confidentiality of the data. Each case was assigned a unique identification when his/her information was entered into the database for this study. These data were furthermore stored in a locked cabinet, or a password-protected database on computers in locked rooms at the CPC.
Measures
Four main sets of variables were assessed: 1) demographic information of the child, 2) family profile information, 3) information of the parents (age, marital status, education level, employment status, and presence of illness or disability), and 4) information of the perpetrator and form of abuse. Information of the parents was subdivided to obtain specific information for each parent. Data was structured in this manner to identify the risk factors associated with CAN, and is reflective of the format used by the NFSR. Furthermore, the risk factors assessed were similar to those identified by the Office on Child Abuse and Neglect, Children’s Bureau, US Department of Health and Human Services.10
Data analysis
We first conducted a descriptive analysis by describing children by their sociodemographic status (age and gender), family size, each parent’s level of education and employment status, parents’ marital status, and types of abuse experienced. The perpetrators were divided into 2 categories - “parents” and “others”. We conducted Chi-square test for comparison of case information between types of perpetrators of child abuse and neglect. We conducted a logistic regression analysis, calculating odds ratios (ORs), and corresponding 95% confidence intervals (CIs) for each of the potential explanatory variables in relation to the outcome. A significance level of 0.05 was used for all statistical tests. Data entry and analysis were performed using the Statistical Package of Social Sciences version 21.0 (SPSS Inc., Chicago, IL, USA).
Results
The charts of 220 cases of CAN were reviewed. Tables 1 & 2 show the demographic information and family profile of the children and their parents. Specifically, victims’ mean age was 6.72 ± 4.61 years, 55% were male, 30% had ≥4 siblings, and 25% lived in a family of ≥6 people (including parents). Physical abuse was the most common form of abuse, accounting for 42% of all cases, followed by childhood neglect (39%), sexual abuse (14%), and emotional abuse (4%). Regarding parents’ information, only 16.8% of fathers and 19.5% of mothers, completed a high school education or more (Table 2). Among children who had experienced physical abuse, parents were the perpetrators in 34% of the cases. In contrast, parents were responsible for 56% of the neglect cases. In sexual abuse cases, parents and others (including family members other than parents and strangers) were the perpetrators of 4% and 34% of cases, respectively (Figure 1).
Table 1.
Demographic information of 220 child abuse and neglect victims in Saudi Arabia.
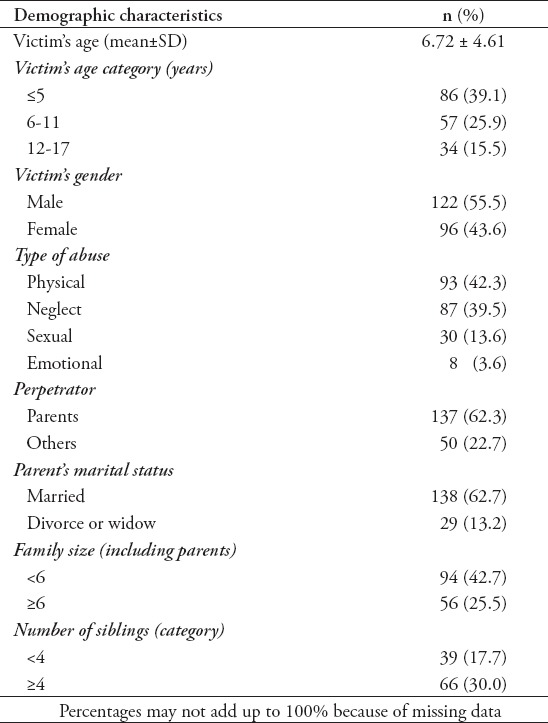
Table 2.
Information of the parents of 220 child abuse and neglect victims in Saudi Arabia.
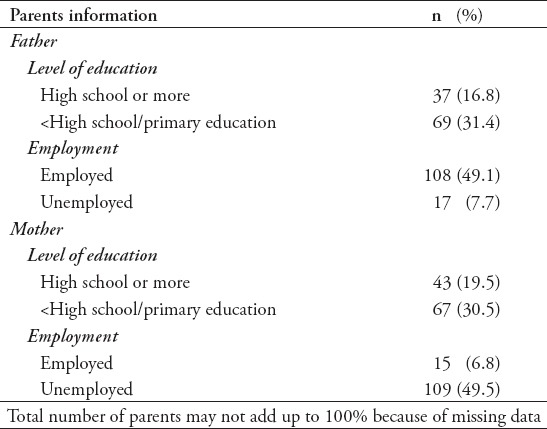
Figure 1.
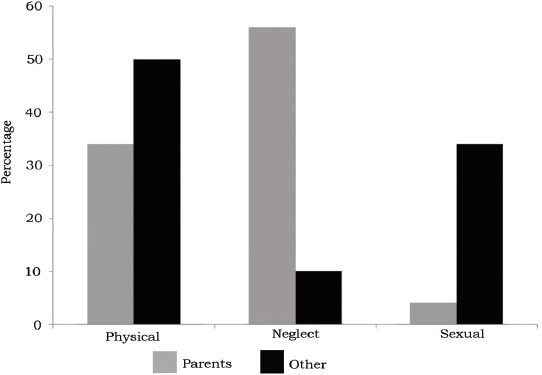
Differences in types of child abuse and neglect by perpetrator.
As shown in Table 3, parent perpetrators were more common among young children (mean age 5.9 years; p=0.018), male victims (p=0.045), large families (≥6 people; p=0.032), and in neglect cases (p=0.000). In contrast, other perpetrators were common among the older age group (mean age 7.8 years), female victims, and cases of sexual abuse. The mean age of perpetrators was significantly higher among others than among parents (p=0.012). With respect to the level of education, parent perpetrators were more likely than with other perpetrator with an education level of less than high school, or no education (p=0.023). In addition, parent perpetrators were more likely to be unemployed compared with other perpetrators (p=0.015).
Table 3.
Comparison of case information between types of perpetrators of 220 child abuse and neglect in Saudi Arabia.
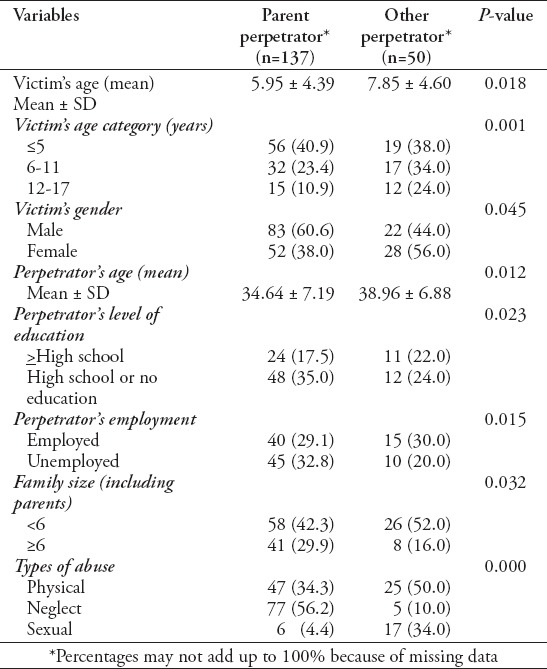
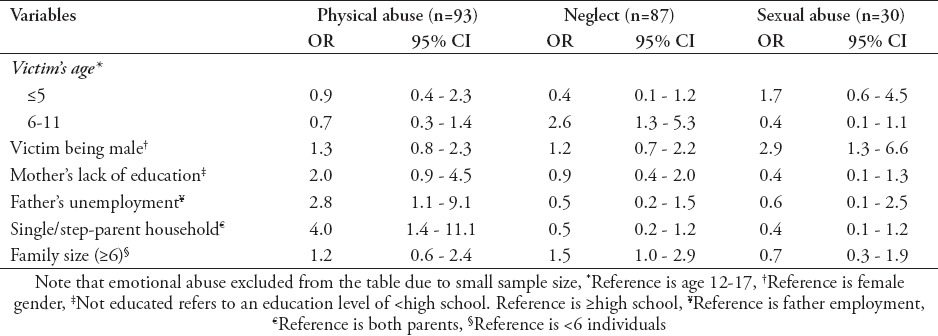
Table 4 shows the ORs for factors associated with physical abuse, childhood neglect, and sexual abuse. We found that children of unemployed father were 2.8 times as likely to be victims of physical abuse. Furthermore, victims from single/step-parent households were 4.0 times as likely to be physically abused were victims from households containing both parents. With respect to childhood neglect, victims living in a large family (≥6) were 1.5 times as likely to be neglected by their parents compared with children living in a small household (<6). Regarding sexual abuse, male victims were 2.9 times as likely to be abused as with female victims.
Table 4.
Factors associated with child abuse and neglect in Saudi Arabia.
Discussion
Child abuse and neglect is heavily intertwined with cultural beliefs and family dynamics. In the last decade, the KSA has witnessed major progress in the field of child protection, including increased awareness, greater capacity building, and the issuing of laws and legislations. Specifically, a law aimed at the prevention of violence and abuse and a child rights law were approved in August 2013 and November 2014. It is expected that the implementation of these laws in the near future will improve services and follow-up of case management. In this context, knowing the family profile of victims of violence may help better understand this epidemic and provide better services. However, given that CAN was barely recognized as a public health issue in the KSA within the last 2 decades,11 most cases continue to go unrecognized, or under reported. In our study, the most common form of abuse reported in the CPC was physical abuse (42% of the cases), whereas in most developed countries, the most common was psychological abuse.12 These results suggested a possible under-recognition and lack of reporting on milder cases in the KSA. We also found that more than half (62%) of perpetrators were parents (with others making up only 23% of perpetrators). These results are similar to the studies from the United States13 and United Kingdom,14 where parents were found to be the offenders in most CAN cases. In summary, the characteristics of the families of CAN victims appeared to be somewhat similar across the countries from different continents and with different economic statuses. A significant relationship was found between the types of abuse and perpetrators. Neglect was most common among victims whose parents were the perpetrators, whereas physical and sexual abuse were most prominent when others were the perpetrators. We also found that boys were significantly more likely to be abused compared with girls, particularly for sexual abuse. The higher incidence of sexual abuse for boys was unexpected. According to the World Health Report,15 girls, in contrast to boys, have been noted to have a higher risk of experiencing sexual abuse in most countries. Male children, on the other hand, are more likely to experience physical abuse, suggesting that they are being exposed to harsher physical punishment.15 Similarly, among Western populations, previous studies have reported that, although rates of CAN are similar for both gender, girls have a greater risk of child sexual abuse compared with boys.16,17 Global studies of this age group also tend to find higher self-reported prevalence and incidence of sexual abuse among adolescent females.18 Similar findings have been noted in less developed countries, with girls being at greater risk of neglect and sexual abuse and boys at greater risk of physical abuse.19 However, prevalence studies in the KSA noted similar findings with our study. Al-Eissa et al11 reported sexual abuse among adolescent boys to be higher than that among adolescent girls. There are several possible explanations for these findings in a patriarchal culture such as the KSA, including the possibility that sexual abuse among girls is regarded as too sensitive topic and thus, under reported. It is also possible that girls are more closely observed and are less outgoing compared with boys, thus, decreasing the opportunities for them to be sexually abused. Alternatively, sexual victimization of girls is more stigmatizing to a family compared with that of boys, which might have resulted in a fewer number of cases of sexually victimized girls being presented to the CPC for evaluation.11 According to the WHO report on violence and health,1 the age of the child is often cited as a predisposing factor for CAN; this is important to acknowledge, given that relevant care often depends on the age of the child. Furthermore, the World Report on Violence and Health15 highlighted that families with >4 children are 3 times as likely to experience CAN compared with families with fewer than 4 children. In our study, a quarter of the cases lived in households comprising ≥6 members, and these cases were 1.5 times as likely to experience childhood neglect as those not living in such households. This rate is comparable with that in previous population-based studies; indeed, evidence supports the increased risk of CAN in larger families from both financial and social perspectives, as the risk of family discord and financial challenges increases with larger families.3 Similarly, Wu et al20 reported that families with more than 2 children are 2.7 times as likely to experience CAN as are those with 2 children or less.
It is predictable that higher educational levels are equated with better employment opportunities, financial stability, and better living standards. The literature varies significantly in terms of the relationship between parents’ level of education and CAN. In some studies, there was no relationship between these variables,21 whereas others found a rather strong association.22 Regarding parents’ unemployment, the Fourth National Incidence Study of Child Abuse and Neglect (NIS-4, 2009-2010) reported that the rate of CAN among children of unemployed parents was 2-3 times that of children of employed parents. This is expected due to household income and socioeconomic status are likely to be highly influenced by parents’ unemployment.23,24 We similarly found that having an unemployed father was a strong predictor of CAN, which is comparable to Coohey’s25 report, wherein having a non-biological, unemployed father was a significant risk factor for CAN. Our study shows that children living in single/step-parent households are more likely to be physically abused compared with those living with both parents. A major concern is that the risk of exposure to all forms of CAN is greater for Saudi children living in single/step-parent households compared with children living with both parents. Other studies have noted that living in households that include members not genetically related to the child, such as single/step-parent households, are a risk factor for CAN.15 A study conducted in Kuwait explored the relationship between psychological and physical abuse and parental characteristics, and found that CAN was significantly correlated with parental divorce.7 Van Ijzendoorn et al3 also examined the relationship between step-parent and the incidence of CAN, and concluded that the absence of genetic ties increases the risk of CAN.3 Our findings are consistent with the findings of other national studies in the KSA, which revealed that single-parent households and the presence of step-parent may put children at increased risk of CAN.26 This finding was also noted in a larger prevalence survey among adolescents of the KSA.11
Study limitations
A major limitation of the sample was that it was restricted to an almost homogeneous sector of society, namely the KAMC, Riyadh; thus, our results are not reflective of the KSA population and our conclusions cannot be generalized. Furthermore, as a result of the novelty of the documentation and reporting system in the KSA, many gaps were found in the patients’ files, thus, leading to a considerable amount of missing information. Another possible limitation is the number of variables studied: that is, it might have been preferable to focus on one variable to gain a deeper understanding of its dynamics. This in turn raises questions of the suitability of the quantitative method of studying such social phenomena. Although identifying specific quantifiable variables that might have an impact on incidences of CAN is useful, it does not take into consideration, infinitely unquantifiable variables such as human behavior, morality, religious influences, and the perception of the self and others.
Child protection services are in their early stages in the KSA. There is a great demand for research in this area in order to provide a better understanding and aid in the development of appropriate interventions. This study only reflects a small sample of CAN in the KSA; as such, these findings do not represent the city, or the wider nation. Perhaps once further CPCs are established, expanding this research to cover the whole of the KSA would provide a better understanding of the problem. More specifically, based on our findings, there are numerous areas that need closer examination: a) early detection, reporting, and accurate documentation of CAN, b) legislations that would deter CAN, and c) working collaboratively with schools and social services to educate parents about effective childcare and discipline.
In conclusion, as CAN has only been recently recognized in the KSA, time will undoubtedly be required to employ effective, culturally sensitive prevention strategies. The present study was a modest attempt to try to understand what can compromise parenting and cause CAN within the Saudi household. Although this merely scratches the surface of a very complex problem within this unique society, it will serve as a platform on which to build in the future.
Acknowledgment
The authors would like to thank Ms. Nahrain Quiambao and Ms. Nourah AlKufeidy for the administrative support and assistance in the preparation of the manuscript.
Footnotes
Copyright.
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
References
- 1.Krug E, Dahlberg L, Mercy A, Zwi A, Lozano R. World report on violence and health. Geneva (CH): World Health Organization; 2002. [Google Scholar]
- 2.Barlett J, Easterbrooks M. Links between physical abuse in childhood and child neglect among adolescent mothers. Child Youth Serv Rev. 2012;34:2164–2169. [Google Scholar]
- 3.Van Ijzendoorn M, Euser E, Prinzie P, Juffer F, Bakermans-Kranenburg M. Elevated risk of child maltreatment in families with stepparents but not with adoptive parents. Child Maltreat. 2012;14:369–375. doi: 10.1177/1077559509342125. [DOI] [PubMed] [Google Scholar]
- 4.U.S. Department of Health and Human Services. Child maltreatment. Washington (DC): U.S. Government Printing Office; 2008. [cited on June 15, 2015]. Available from: http://archive.acf.hhs.gov/programs/cb/pubs/cm08/cm08.pdf . [Google Scholar]
- 5.Pilowsky D, Wickramaratne P, Nomura Y, Weissman M. Family discord, parental depression, and psychopathology in offspring:20-year follow-up. J Am Acad Child Adolesc Psychiatry. 2006;45:452–460. doi: 10.1097/01.chi.0000198592.23078.8d. [DOI] [PubMed] [Google Scholar]
- 6.McRee N. Child abuse in blended households: Reports from runaway and homeless youth. Child Abuse Negl. 2008;32:449–453. doi: 10.1016/j.chiabu.2007.09.007. [DOI] [PubMed] [Google Scholar]
- 7.Al-Fayez G, Ohaeri J, Gado O. Prevalence of physical, psychological and sexual abuse among a nationwide sample of Arab high school students: association with family characteristics, anxiety, depression, self-esteem, and quality of life. Soc Psychiatry Psychiatr Epidemiol. 2012;47:53–66. doi: 10.1007/s00127-010-0311-2. [DOI] [PubMed] [Google Scholar]
- 8.Al-Eissa MA, Albuhairan FS, Qayad M, Saleheen H, Runyan D, Almuneef M. Determining child maltreatment incidence in Saudi Arabia using the ICAST-CH: A pilot study. Child Abuse Negl. 2014;42:174–182. doi: 10.1016/j.chiabu.2014.08.016. [DOI] [PubMed] [Google Scholar]
- 9.Oliver W, Kuhns L, Pomeranz E. Family structure and child abuse. Clin Pediatr. 2006;45:111–118. doi: 10.1177/000992280604500201. [DOI] [PubMed] [Google Scholar]
- 10.Goldman J, Salus M, Wolcott D, Kennedy K. A coordinated response to child abuse and neglect: the foundation for practice. Chapter Five: What factors contribute to child abuse and neglect? Washington (DC): Office on Child Abuse and Neglect, Children’s Bureau, US Department of Health and Human Services; 2003. [cited on 2015 July 1]. Available at: https://www.childwelfare.gov/pubs/usermanuals/foundation/foundation.pdf . [Google Scholar]
- 11.Al-Eissa MA, Saleheen HN, AlMadani S, Albuhairan FS, Weber A, Fluke JD, et al. Determining prevalence of maltreatment among children in the Kingdom of Saudi Arabia. Child Care Health Dev. 2016;42:565–571. doi: 10.1111/cch.12325. [DOI] [PubMed] [Google Scholar]
- 12.Zolotor AJ, Runyan DK, Dunne MP, Jain D, Péturs HR, Ramirez C, et al. ISPCAN Child Abuse Screening Tool Children’s Version (ICAST-C): Instrument development and multi-national pilot testing. Child Abuse Negl. 2009;33:833–841. doi: 10.1016/j.chiabu.2009.09.004. [DOI] [PubMed] [Google Scholar]
- 13.Sedlak A, Mettenburg J, Basena M, Petta I, McPherson K, Greene A, et al. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to congress [Internet] US. Washington (DC): Department of Health and Human Services, Administration for Children and Families; 2010. [Cited on 2015 July 2015]. Available from: http://www.acf.hhs.gov/sites/default/files/opre/nis4_report_congress_full_pdf_jan2010.pdf . [Google Scholar]
- 14.May-Chahal C, Cawson P. Measuring child maltreatment in the United Kingdom: A study of the prevalence of child abuse and neglect. Child Abuse Negl. 2005;29:969–984. doi: 10.1016/j.chiabu.2004.05.009. [DOI] [PubMed] [Google Scholar]
- 15.The World Health Report on Violence and Health. Chapter 3: Child abuse and neglect by parents and other caregivers. Geneva: World Health Organization; 2002. [Cited on 2015 August 2015]. Available from: http://www.who.int/violence_injury_prevention/violence/global_campaign/en/chap3.pdf . [Google Scholar]
- 16.Andrews G, Corry J, Slade T, Issakidis C, Swanston H. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. Child Sexual Abuse. 2004;2:1851–1940. [Google Scholar]
- 17.U.S. Department of Health and Human Services. Administration on children, youth, and families. Washington, (DC): US Government Printing Office; 2014. [Google Scholar]
- 18.Stoltenborgh M, Van IJzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat. 2011;16:79–101. doi: 10.1177/1077559511403920. [DOI] [PubMed] [Google Scholar]
- 19.Pinheiro PS. World report on violence against children. New York: United Nations Secretary-General’s Study on Violence Against Children; 2006. [Cited on 2015 August 19, 2015]. Available from URL: http://www.unicef.org/lac/full_tex(3).pdf . [Google Scholar]
- 20.Wu SS, Ma CX, Carter RL, Ariet M, Feaver EA, Resnick MB, Roth J. Risk factors for infant maltreatment: a population-based study. Child Abuse Negl. 2004;28:1253–1264. doi: 10.1016/j.chiabu.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 21.Alokan F, Kemi B. The correlation between parents’ educational status and child abuse. Humanity & Social Sciences Journal. 2010;5:73–79. [Google Scholar]
- 22.Malik F. Determinants of child abuse in Pakistani families parental acceptance-rejection and demographic variables. International Journal of Business and Social Sciences. 2010;1:67–80. [Google Scholar]
- 23.Liao M, Lee A, Roberts-Lewis A, Hong J, Jiao K. Child maltreatment in China: An ecological review of the literature. Children Youth Serv Rev. 2011;33(9):1709–1719. [Google Scholar]
- 24.May-Chahal C, Cawson P. Measuring child maltreatment in the United Kingdom: A study of the prevalence of child abuse and neglect. Child Abuse Negl. 2005;29:969–984. doi: 10.1016/j.chiabu.2004.05.009. [DOI] [PubMed] [Google Scholar]
- 25.Coohey C. Physically abusive fathers and risk assessment. Child Abuse Negl. 2006;30:467–480. doi: 10.1016/j.chiabu.2004.10.016. [DOI] [PubMed] [Google Scholar]
- 26.Dufour S, Lavergne C, Larrivée MC, Trocmé N. Who are these parents involved in child neglect? A differential analysis by parent gender and family structure. Children Youth Serv Rev. 2008;30:141–156. [Google Scholar]