

Abstract
Background
In neurological diseases, winging of the scapula occurs because of serratus anterior muscle dysfunction due to long thoracic nerve palsy, or trapezius muscle dysfunction due to accessory nerve palsy. Several sports can cause long thoracic nerve palsy, including archery and tennis. To our knowledge, this is the first report of long thoracic nerve palsy in an aquatic sport.
Objective
The present study is a rare case of winging of the scapula that occurred during synchronized swimming practice.
Methods
The patient's history with the present illness, examination findings, rehabilitation progress, and related medical literature are presented.
Results
A 14-year-old female synchronized swimmer had chief complaints of muscle weakness, pain, and paresthesia in the right scapula. Upon examination, marked winging of the scapula appeared during anterior arm elevation, as did floating of the superior angle. After 1 year of therapy, right shoulder girdle pain and paresthesia had disappeared; however, winging of the scapula remained.
Conclusions
Based on this observation and the severe pain in the vicinity of the second dorsal rib, we believe the cause was damage to the nerve proximal to the branch arising from the upper nerve trunk that innervates the serratus anterior.
Keywords: winging of the scapula, accessory nerve palsy, long thoracic nerve palsy, synchronized swimming
Introduction
Winging of the scapula is a condition in which the medial border of the scapula is raised from the chest wall, resulting in a wing-like protrusion of the scapula. Scapular winging has been observed in scoliosis, deltoid contracture, Sprengel's deformity, and infraspinatus muscle atrophy. It can also occur in dislocation of the shoulder, as well as after muscle rupture or muscular dystrophy associated with trauma.1 2 Frequently, winging of the scapula occurs because of denervation of the serratus anterior muscle due to long thoracic nerve palsy, or because of the denervation of the trapezius muscle due to accessory nerve palsy.3 4 5 6 7 The severity of winged scapula is variable, and although pain is not seen in every case, it will most often resolve with time, even when there is complete loss of muscle function.
The cause of long thoracic nerve palsy may be traumatic or atraumatic.8 Lesions to the long thoracic nerve may occur due to numerous and varied causes.9 Generally, however, injury to the long thoracic nerve can follow excessive upper-limb stretching, and may result from traction and/or compression between its cervical origin and its distal terminal branches in the serratus anterior muscle, the anatomical structure and innervation of which have been thoroughly described. Excessive upper-limb stretching during sports activities appears to be a significant factor.10 11 12 13 14
A wide range of sports have been reported to cause long thoracic nerve palsy, including archery, tennis, and basketball.4 6 7 15 16 17 18 19 20 21 To our knowledge, this is the first report of long thoracic nerve palsy in aquatic sports (Table 1).
Table 1. Cases of long thoracic nerve palsy due to sports, as reported in the literature.
| Author | Year | Age | Sex | Cause | Period until Improvement (mo) |
|---|---|---|---|---|---|
| Gregg et al5 | 1979 | 23 | M | Tennis | 1 |
| 47 | F | Tennis | 6 | ||
| 32 | M | Ballet | 14 | ||
| 23 | M | Soccer | 12 | ||
| 20 | M | Ice hockey | 12 | ||
| 27 | M | Bowling | 7 | ||
| 27 | M | Golf | 11 | ||
| 22 | M | Gymnastics | 4 | ||
| 11 | M | Weightlifting | 4.5 | ||
| Sakamoto et al16 | 1981 | 14 | M | Basketball | 6 |
| Isayama et al17 | 1982 | 20 | M | Archery | 1 |
| Yasuda et al18 | 1982 | 12 | F | Portball | Began recovering in 2 y |
| Foo et al28 | 1983 | 18 25 |
M F |
Tennis Archery |
12 Unknown |
| Ohno et al19 | 1984 | 21 | F | Gymnastics | 7 |
| Fukuzawa et al20 | 1985 | 14 13 |
M F |
Basketball Volleyball |
6 5 |
| Shimizu3 | 1990 | 20 | M | Archery | Recovering |
| Toizumi et al15 | 1997 | 16 | M | Javelin | 7 |
| Ebata et al23 | 2005 | 27 | M | Weightlifting | Unknown |
| Present case | 2013 | 14 | F | Synchronized swimming | Began recovering in 1 y |
Note: Previous studies have reported patients with long thoracic nerve palsy due to sports other than aquatic sports.
Synchronized swimming is a sport in which athletes are subjectively scored on technical merit and artistic expression during their aquatic performance. In the present study, we report a rare case of winging of the scapula that occurred during synchronized swimming practice.
Case Report
The subject was a 14-year-old female synchronized swimmer with chief complaints of muscle weakness, pain, and paresthesia in the right scapula. She had no history of neurological or muscular disease.
History of Present Illness
In mid-July 2011, while performing the butterfly stroke during synchronized swimming practice, the subject experienced severe pain in the vicinity of the second dorsal rib, as well as dislocation of the right glenohumeral joint. Thereafter, she discontinued practice and underwent an orthopedic examination several days later.
Physical Findings upon Initial Examination
Right arm manual muscle testing (MMT) grades and right shoulder joint range of motion (ROM) are listed in Tables 2 and 3, respectively. In the left shoulder, MMT and joint ROM were normal. The subject experienced paresthesia in the right shoulder girdle. In addition, when the diagnostic wall press test (WPT) was performed (pressing hands against a wall in a leaning position), distinct winging of the right scapula was observed. Due to drooping of her right shoulder, it was immobilized in a sling for 2 to 3 months. In addition, she was diagnosed with isolated paralysis of the serratus anterior muscle based on electromyography results.
Table 2. Results of the right arm manual muscle test before and after therapy.
| Initial examination | One year after beginning therapy | |
|---|---|---|
| Shoulder flexion | 2 | 4 |
| Shoulder abduction | 2 | 4 |
| Shoulder extension | 1 | 3 |
| Scapular elevation | 1 | 2 |
Table 3. Results of the right shoulder joint range of motion examination before and after therapy.
| Initial examination | One year after beginning therapy | |||
|---|---|---|---|---|
| Passive (degrees) | Active (degrees) | Passive (degrees) | Active (degrees) | |
| Shoulder flexion | 10° | 5° | 130° | 130° |
| Shoulder abduction | 20° | 10° | 90° | 90° |
| Shoulder extension | 5° | 0° | 40° | 25° |
Exercise Therapy
At 4 months postinjury, the subject discontinued shoulder immobilization and began rehabilitation. Rehabilitation initially consisted of passive flexion, extension, abduction, and external and internal rotation of the right glenohumeral joint; this was followed by gradual transition to active movement, and ultimately progressed to resistance exercises. In addition, the muscles surrounding the right shoulder were stretched and massaged. Two or three rehabilitation sessions were performed per week, with each session lasting ∼30 minutes.
Progress
One year after beginning therapy, the right shoulder girdle pain and paresthesia had disappeared. MMT and joint ROM improved, although not completely. The subject's MMT and ROM grades 1 year after beginning therapy are listed in Tables 2 and 3, respectively. However, when shoulder abduction was 0 degree, downward rotation of the right scapula was prominent. Furthermore, WPT resulted in a distinct dorsal protrusion of the scapula, and winging of the scapula remained (Fig. 1).
Fig. 1.

Winging of the scapula is apparent when the patient is pushing forward. The arrows show winging of the scapula.
Discussion
The long thoracic nerve is primarily derived from the merging of the ventral rami of branches from the fifth, sixth, and seventh cranial nerves (hereafter, “C5,” “C6,” and “C7,” respectively); this nerve consists of pure motor fibers, which innervate the serratus anterior muscle.4 6 21 22 23 24 25 There are many variations in the components of the long thoracic nerve. However, generally, the upper long thoracic nerve trunk, which is formed by C5 and C6, innervates the upper portion of the serratus anterior muscle. C7, which constitutes the lower long thoracic nerve trunk, merges with the upper trunk to form the common trunk, and then innervates the middle and lower portions of the serratus anterior muscle. The course of the long thoracic nerve is characterized by certain features. C5 and C6, which form the upper nerve trunk, primarily run through the anterior and middle scalene muscles; in 24 to 33% of cases, the middle scalene muscle is penetrated (Fig. 2).26 27 When the common trunk of the long thoracic nerve descends behind the brachial plexus, it angulates over the second rib, runs downward along the thoracic wall, and innervates the middle and lower portions of the serratus anterior muscle; its total length is ∼24 cm.3 21 22 28
Fig. 2.
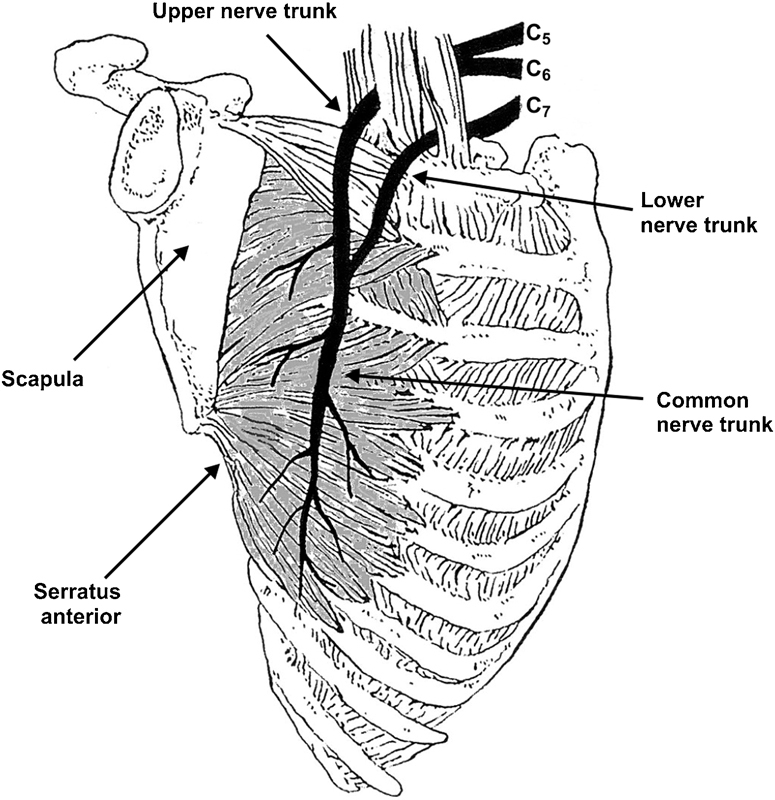
Diagram of the long thoracic nerve in a cadaver. The serratus anterior muscle consists of upper, middle, and lower portions. The upper portion is supplied mainly by the C5 nerve root. The long thoracic nerve, consisting of the C6 and C7 nerve roots, innervates the middle and lower portions. Image modified from Toizumi et al15 with the permission from Igaku-shoin.
Based on this anatomical course, there are sites where tight facial bands of tissue may cause a “bow-string” effect that could induce long thoracic nerve palsy. Furthermore, there is also a possibility of traction injury of the nerve between the middle scalene muscle and the lower portion of the serratus anterior muscle.5 15 22 29 30
Hamada et al21 showed that the upper portion of the serratus anterior muscle runs in a posterior direction, the middle portion in a posteromedial direction, and the lower portion in a posterosuperior direction. Therefore, the upper, middle, and lower portions of the serratus anterior muscle control the anterior tilt, abduction, and upward/internal rotation of the scapula, respectively. The serratus anterior muscle was considered to stabilize the scapula as follows: the upper portion of the serratus anterior muscle attaches the superior angle of the scapula to the first and second ribs, the middle portion attaches the medial border of the scapula to the thorax, and the lower portion attaches the inferior angle to the thorax. Therefore, when the superior angle is attached to the thorax and the medial border and inferior angle of the scapula are floating, it is inferred that the nerve distal to the branch that arises from the upper nerve trunk and innervates the serratus anterior is damaged. When the superior angle is also floating, it is inferred that there is damage to the nerve proximal to the branch described above. Winging of the scapula associated with paralysis of the serratus anterior muscle is prominent during anterior arm elevation. The middle portion of the serratus anterior muscle controls scapular abduction, while the lower portion controls upward and interior rotation; in paralysis of the serratus anterior muscle, these portions do not function, resulting in characteristic adduction and downward rotation of the scapula. In other words, the upper portion of the serratus anterior muscle is innervated by branches that arise directly from the upper long thoracic nerve trunk, which is composed primarily of C5 and C6, while the middle and lower portions of the serratus anterior muscle are innervated by the common trunk. Therefore, winging of the scapula only occurs if there is paralysis of the middle or lower portions of the serratus anterior muscle.
The present case demonstrated prominent winging of the scapula during anterior arm elevation, as well as floating of the superior angle. Based on this observation and the severe pain near the second dorsal rib, we believe the cause was damage to the nerve proximal to the branch that arises from the upper nerve trunk and innervates the serratus anterior muscle.
The case reported herein presented with severe pain and dysfunction of the serratus anterior muscle while swimming the butterfly stroke during synchronized swimming practice. The cause of these symptoms was considered to be compression of the long thoracic nerve between the scapula and ribs during posterior rotation of the arm. However, despite identical movements of the left and right arms in the butterfly stroke, the left serratus anterior muscle was completely undamaged. Therefore, it is inferred that frequent use of the dominant right arm in sports and activities of daily living can result in traction injury to the long thoracic nerve.
Conclusion
We reported a case of long thoracic nerve palsy and winging of the scapula that occurred during synchronized swimming practice. It was apparent that some improvement was evident at a 1-year follow-up examination, but full recovery was not evident. This case shows that severe functional loss can remain and therefore timely follow-up is necessary to monitor for signs of reinnervation. Otherwise, surgical exploration and microsurgical nerve decompression repair or nerve transfer might be indicated. Methods to consider for monitoring of reinnervation are clinical examination, muscle magnetic resonance imaging to determine resolution of denervation edema, and electromyogram of the serratus to detect reinnervation.
Acknowledgments
I would like to express my sincere gratitude to the subject in this report for understanding the significance of the case and her willingness to participate. I am also deeply grateful to everyone else involved in this report.
Editorial support, in the form of development, collating author comments, copyediting, fact checking, and referencing, was provided by Editage, a division of Cactus Communications Pvt. Ltd. and funded by the author.
Footnotes
Conflict of Interest The author does not have any conflict of interest to declare.
References
- 1.Tsuchisawa N, Fujino H, Miyaoka H. Case report of osteochondroma presenting with winging of the scapula [in Japanese] J East Jpn Orthop Traumatol. 2004;16:158–161. [Google Scholar]
- 2.Wataya M, Maeda K, Sakamoto T, Ohwada O, Iioka K. Treatment of a patient complaining of shoulder pain associated with winging of the scapula [in Japanese] Hokkaido J Phys Ther. 1994;11:30–32. [Google Scholar]
- 3.Shimizu J. Case report of long thoracic nerve palsy presenting with winging of the scapula associated with archery practice [in Japanese] Clin Nephrol. 1990;30:873–876. [Google Scholar]
- 4.Johnson J TH, Kendall H O. Isolated paralysis of the serratus anterior muscle. J Bone Joint Surg Am. 1955;37-A(3):567–574. [PubMed] [Google Scholar]
- 5.Gregg J R Labosky D Harty M et al. Serratus anterior paralysis in the young athlete J Bone Joint Surg Am 197961(6A):825–832. [PubMed] [Google Scholar]
- 6.Toda N. Long thoracic nerve palsy [in Japanese] Jpn J Surg. 1992;11:505–508. [Google Scholar]
- 7.Fiddian N J, King R J. The winged scapula. Clin Orthop Relat Res. 1984;(185):228–236. [PubMed] [Google Scholar]
- 8.Harada M, Mura N, Takahara M, Naruse T, Ogino T. Long thoracic nerve palsy caused by fence picket penetration from axillary region to neck [in Japanese] Tohoku J Orthop Traumatol. 2007;51(1):106–109. [Google Scholar]
- 9.Vastamäki M, Kauppila L I. Etiologic factors in isolated paralysis of the serratus anterior muscle: a report of 197 cases. J Shoulder Elbow Surg. 1993;2(5):240–243. doi: 10.1016/S1058-2746(09)80082-7. [DOI] [PubMed] [Google Scholar]
- 10.Nasu H, Yamaguchi K, Nimura A, Akita K. An anatomic study of structure and innervation of the serratus anterior muscle. Surg Radiol Anat. 2012;34(10):921–928. doi: 10.1007/s00276-012-0984-1. [DOI] [PubMed] [Google Scholar]
- 11.Prescott M U, Zollinger R W. Alar scapula: an unusual surgical complication. Am J Surg. 1944;65(1):98–103. [Google Scholar]
- 12.Takagishi K. Tokyo: Medical View Co. Ltd.; 2006. Long thoracic nerve palsy; pp. 234–240. [Google Scholar]
- 13.Iceton J, Harris W R. Treatment of winged scapula by pectoralis major transfer. J Bone Joint Surg Br. 1987;69(1):108–110. doi: 10.1302/0301-620X.69B1.3029135. [DOI] [PubMed] [Google Scholar]
- 14.Izumi S, Kasumi F. Preventing and dealing with intraoperative trouble [in Japanese] J Clin Surg. 1989;44:1342–1369. [Google Scholar]
- 15.Toizumi T, Kondo S, Mitsubashi N. et al. Case report of long thoracic nerve palsy in a javelin thrower [in Japanese] J Jpn Clin Orthop Assoc. 1997;32:1341–1344. [Google Scholar]
- 16.Sakamoto K, Fujimaki E, Maruyama T, Kimura T, Kuriyama S. Case report of isolated paralysis of the serratus anterior muscle in a basketball player [in Japanese] Higashi Nihon Supootsu Ikenkaishi. 1981;2:27–30. [Google Scholar]
- 17.Isayama T, Takagishi N, Takeshita M. Five cases of winging of the scapula due to long thoracic nerve palsy [in Japanese] Shoulder Joint. 1982;6:40–42. [Google Scholar]
- 18.Yasuda T, Morimoto K, Terao A. Long thoracic nerve palsy due to sports injury [in Japanese] Neurol Med. 1982;17:513–514. [Google Scholar]
- 19.Ohno T, Ishii Y, Kawaji W. Case report of paralysis of the anterior serratus muscle during calisthenics [in Japanese] Tohoku Arch Orthop Surg Traumatol. 1984;27:383–384. [Google Scholar]
- 20.Fukuzawa K, Uemura S, Maruyama T, Fujimaki E, Sakamoto K. Two cases of isolated paralysis of the serratus anterior in the young athlete [in Japanese] Jpn J Physical Fit Sports Med. 1985;34:569. [Google Scholar]
- 21.Hamada J, Ogawa K, Akita K. The long thoracic nerve and serratus anterior muscle: dissection and clinical practice [in Japanese] Shoulder Joint. 2010;34(3):861–865. [Google Scholar]
- 22.Horwitz M T, Tocantins L M. An anatomical study of the role of the long thoracic nerve and the related scapula bursae in the pathogenesis of local paralysis of the serratus anterior muscle. Anat Rec. 1938;71:375–385. [Google Scholar]
- 23.Ebata A, Kokubun N, Miyamoto T, Hirata K. Case report of long thoracic nerve palsy in which muscle training was considered to be involved in bilateral winging of the scapula [in Japanese] Clin Nephrol. 2005;45(4):308–311. [PubMed] [Google Scholar]
- 24.Takagishi K. Tokyo: Nakayama Shoten; 2006. The shoulder joint and shoulder girdle; pp. 306–311. [Google Scholar]
- 25.Wood V E, Frykman G K. Winging of the scapula as a complication of first rib resection: a report of six cases. Clin Orthop Relat Res. 1980;(149):160–163. [PubMed] [Google Scholar]
- 26.Yazar F, Kilic C, Acar H I, Candir N, Comert A. The long thoracic nerve: its origin, branches, and relationship to the middle scalene muscle. Clin Anat. 2009;22(4):476–480. doi: 10.1002/ca.20794. [DOI] [PubMed] [Google Scholar]
- 27.Hamada J, Igarashi E, Akita K, Mochizuki T. A cadaveric study of the serratus anterior muscle and the long thoracic nerve. J Shoulder Elbow Surg. 2008;17(5):790–794. doi: 10.1016/j.jse.2008.02.009. [DOI] [PubMed] [Google Scholar]
- 28.Foo C L, Swann M. Isolated paralysis of the serratus anterior. A report of 20 cases. J Bone Joint Surg Br. 1983;65(5):552–556. doi: 10.1302/0301-620X.65B5.6643557. [DOI] [PubMed] [Google Scholar]
- 29.Gozna E R, Harris W R. Traumatic winging of the scapula. J Bone Joint Surg Am. 1979;61(8):1230–1233. [PubMed] [Google Scholar]
- 30.Hester P, Caborn D N, Nyland J. Cause of long thoracic nerve palsy: a possible dynamic fascial sling cause. J Shoulder Elbow Surg. 2000;9(1):31–35. doi: 10.1016/s1058-2746(00)90007-7. [DOI] [PubMed] [Google Scholar]