

ABSTRACT
Objective
Compulsive exercise is a well‐known feature in eating disorders. The Exercise and Eating Disorder (EED) self‐report questionnaire was developed to assess aspects of compulsive exercise not adequately captured by existing instruments. This study aimed to test psychometric properties and the factor structure of the EED among women with eating disorders and a control group.
Method
The study included 449 female participants, including 244 eating disorders patients and 205 healthy controls. The patient group consisted of 32.4% (n = 79) AN patients, 23.4% (n = 57) BN, 34.4% (n = 84) EDNOS and 9.8% (n = 24) with BED diagnosis.
Results
The analyses confirmed adequate psychometric properties of the EED, with a four‐factor solution: (1) compulsive exercise, (2) positive and healthy exercise, (3) awareness of bodily signals, and (4) weight and shape exercise. The EED discriminated significantly (p < .001) between patients and controls on the global score, subscales, and individual items. Test‐retest reliability was satisfactory (r = 0.86). Convergent validity was demonstrated by high correlations between the EED and the Eating Disorder Examination Questionnaire (EDE‐Q; r = 0.79).
Discussion
The EED is the first clinically derived, self‐report questionnaire to assess compulsive exercise among ED patients. The EED offers assessment that has broader clinical utility than existing instruments because it identifies treatment targets and treatment priorities. © 2015 Wiley Periodicals, Inc. (Int J Eat Disord 2015; 48:983–993).
Keywords: eating disorders, compulsive exercise, physical activity, questionnaire
Introduction
Compulsive/excessive exercise is a well‐known feature in eating disorders. It has been reported as an important factor to consider in all stages of the illness, and has been identified as a predictor of poor outcome.1, 2, 3 In the DSM‐IV and DSM 5 criteria, the phrase “excessive exercise” is described in relation to fear of gaining weight for anorexia nervosa (AN) and as a compensatory behavior to control weight for bulimia nervosa (BN). Exercise is defined as excessive when interfering with important activities, occurring at inappropriate times and settings, and continuing despite injuries and/or medical complications.4
Meyer and Taranis5 have described challenges in this research field as a consequence of great variation and inconsistency in use of terms and definitions. Similar to other researchers,6, 7 they have highlighted the lack of a consensus definition of compulsive/excessive exercise. Measurement has largely focused on motivation, i.e., exercise motivated by shape/weight concern/control, and the amount of exercise.6, 8, 9 Across different inpatient samples, 39 to 45.5% of patients have been classified as compulsive/excessive exercisers.6, 9
Improving our knowledge and understanding of compulsive exercise among clinical samples of eating disorders is an important and clinically relevant research direction. In addition to exercise motivated by shape and weight concerns, research has elucidated the role of exercise in affect regulation in clinical samples,10, 11 and emerging evidence suggests the importance of withdrawal symptoms and negative consequences of not exercising.3, 12, 13 It has been stated that “compulsive” is a more appropriate term than “excessive” when describing exercise in patients with eating disorders.5, 14 These authors differentiated between a quantity dimension (excessive) measured by frequency, intensity and duration, and the qualitative dimension related to compulsivity.
Different assessments have measured different constructs related to excessive/compulsive exercise. The Obligatory Exercise Questionnaire (OEQ) was developed to measure exercise attitudes and activities.15 A revised version (OEQ‐R) covers emotional elements, behavioral elements and exercise preoccupation.16 The Eating and Exercise Behavior Questionnaire17 focuses on behavioral control of obesity, with one scale covering exercise behavior. The Commitment to Exercise Scale18 was developed to tap feelings of well‐being, maintenance, and exercise regimes. The Reasons for Exercise Inventory (REI)19 includes four subscales to assess management of fitness and health, attractiveness and weight loss, emotional regulation, and social interaction. Another perspective in the measurement of excessive exercise is linked to theories of addiction or dependence on exercise. For example, the Exercise Dependence Questionnaire20 and Exercise Dependence Scale‐Revised (EDS‐R)21 both represent this tradition. In the EDS‐R, all the criteria for dependence in the DSM‐IV were included and linked to exercise behavior. The Exercise Addiction Inventory22 is a short version related to addiction models of understanding exercise. Within this framework, eating disorders are theoretically linked to secondary dependency of exercise. Other models have focused on primary factors related to the maintenance of compulsive exercise within a cognitive‐behavioral framework. In 2011, for example, preliminary results were published from a validation study of a new questionnaire entitled the compulsive exercise test (CET).23 The content of this questionnaire stems from a multidimensional view of eating disorders. All of these questionnaires were validated in nonclinical samples.
In our clinical practice, we experienced a lack of correspondence between the challenges reported by the eating disorder patients and available questionnaires, and no questionnaires have been developed in clinical eating disorder units. Restriction of exercise and regulation of rest and meals are elements in treatment programs. It is necessary to understand how emotional and behavioral aspects influence the relationship between exercise and other symptoms in treatment. We aimed to develop an instrument for clinical purposes that addressed aspects of excessive exercise not adequately captured by existing questionnaires. Specifically, we attempted to fill a gap in the assessment literature by covering clinically relevant constructs such as negative emotions, or consequences if exercise was delayed or interrupted,18, 24 the ability to perceive and/or interpret body signals (e.g., hunger, satiety and fatigue) despite being emaciated,25 and changes in body perception when exercise was restricted. Based on existing research and clinical observations, a new questionnaire, the Exercise and Eating Disorder (EED), was developed. A pilot study showed promising preliminary results,13 and subsequent revisions to the EED in 2009 made necessary further validation. More information about the pilot study is provided in the method section. The specific aims of this study were to (1) test the psychometric properties of the revised version of the EED in a female clinical sample and a control group, (2) to test the factor structure, and (3) to determine a classification scheme based on the EED global score to yield an estimate of severity, which may be useful in clinical decision‐making.
Method
Participants and Procedure
The study included 449 female participants, 244 eating disorder patients (inpatients and outpatients), and 205 healthy controls. The patients were recruited from an eating disorder unit between the beginning of 2009 and the end of 2013. Questionnaires, which included informed consent, were administered at the beginning of treatment in accordance with routine assessment procedures at intake. Exclusion criteria in the patient group were not fulfilling criteria for an eating disorder diagnosis (n = 8) and pregnancy (n = 1). Patients were diagnosed by licensed psychologists or psychiatrists. Diagnoses were based on clinical interviews in accordance with diagnostic criteria,26 as supported by the Eating Disorder Examination Questionnaire (EDE‐Q)27 and the Eating Disorder Inventory (EDI‐2).28 Preliminary diagnoses were discussed in meetings with a minimum of two specialists prior to reaching a final consensus diagnosis. The patient sample consisted of 32.4% (n = 79) AN patients, 23.4% (n = 57) BN, 34.4% (n = 84) with an eating disorder not otherwise specified (EDNOS) and 9.8% (n = 24) with a binge eating disorder (BED) diagnosis. In the AN group, 77.2% (n = 61) were diagnosed as restrictive subtype, and 22.8% (n = 18) as binge‐eating/purging subtype. Because there were so few patients in the bulimic subtype, the AN group was collapsed into one group for the analyses. All BN patients were classified as BN‐purging type. The reported duration of eating disorder in the patient group (n = 240) was on average 10.3 years, with a range from 1 to 40 years. Patients were weighed in‐person, but height and weight of controls were self‐reported on the EDE‐Q. Patients were on average significantly older [t (447) = 7.34, p < 0.001] than controls, but the average BMI between groups was not significant [t (440) = −1.61, p < 0.09]. Group differences in age and BMI are presented in Table 1. The mean (SD) for patients on EDE‐Q Global scores was 3.76 (1.42), and for controls it was 1.60 (1.17), t (440) = 17.22, p < .001.
Table 1.
Characteristics of participants
| All Patients n = 244 | AN n = 79 | BN n = 57 | EDNOS n = 84 | BED n = 24 | Controls n = 205 | Differencea, b | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | F valuea, b | p values | Bonferroni Post hoc | |
| Age | 27.1 (9.5) | 23.4 (7.3) | 27.7 (9.3) | 27.6 (9.9) | 36.1 (8.9) | 21.4 (6.3) | 52.30a | a*** | AN vs. BN and EDNOS* |
| (years) | 13.92b | b*** | BED vs. BN** | ||||||
| Range | 16–59 | 16–50 | 16–50 | 16–55 | 24–59 | 16–59 | BED vs. AN and EDNOS*** | ||
| n =242c | n = 56c | n = 83c | n = 203c | ||||||
| BMI | 22.4 (9.4) | 15.4 (1.8) | 22.6 (4.0) | 22.6 (6.5) | 44.5 (7.4) | 23.6 (3.6) | 63.70a | a NS | AN vs. BN, EDNOS and BED*** |
| 213.11b | b*** | BED vs. BN and EDNOS*** | |||||||
| Range | 8.7–62.1 | 8.7–17.6 | 17.5–35.0 | 17.5–48.0 | 33.1–62.1 | 17.3–37.6 |
AN: anorexia nervosa; BN: bulimia nervosa; EDNOS: eating disorder not otherwise specified; BMI: body mass index; NS: not significant.
Independent t test two tailed: Age: t (447) = 7.34, BMI: t (440) = −1.61, between patient group and control group.
One way ANOVA between diagnostic groups, df (3, 240) (age), df (3, 238). Bonferroni post hoc test, only significant relationships are reported.
Reduced N is due to missing BMI data in individuals.
p values: * p < 0.05, ** p < 0.01, and *** p < 0.001.
All secondary female students from a community high school and from different faculties at two University Colleges in the region were invited to participate as a control group. The high school offers education in seven different programs such as science, economics, design and crafts, media and communication, etc. Together with students from different programs (driving instruction, multimedia, finance and administration, animal science, nature management, nursing, and physiotherapy), the control group provided a representative sample of this student population. Questionnaires were administrated by teachers in high school, by the first author (MD) in the University College, and were completed during regular classes (autumn 2013, and beginning of 2014). A total of 219 female students attending school on the data collection days were invited to participate, only four students chose not to participate. Fourteen of these female students reported having an eating disorder and, therefore, were excluded from the study, leaving a total of 205 students. To investigate the test‐retest reliability, 69 controls completed the questionnaire a second time after one week. The questionnaires were pairwise coded for T1 and T2. The actual participants received both questionnaires at the same time, completing one on the actual day (T1) and the other (T2) one week later. These participants received a negligible lottery ticket (value $4, without any guaranty of winning) as a compensation for their participation.
The study was approved by the local Data Access Committee and the Regional Committee for Medical and Health Research Ethics. All patients have provided written informed consent before participation. Information from the control group participants was anonymous. Consent from the control group was organized and completed in accordance to advice received from the Regional Committee for Medical and Health Research Ethics. Both written and oral information were given to the participants. They were informed that completing and returning the questionnaire was equivalent to giving consent to participate in the study. Because of anonymity of the data, it was not possible to withdraw the consent later.
Development of the EED Questionnaire
Based on systematized clinical data, discussions in the multidisciplinary team and existing research, the first version of the EED was developed in 2005.13 It consisted of 20 statements on a 6‐point Likert scale from zero to five (never, rarely, sometimes, often, usually, and always). The scale is reversed for statements with positive meaning. The questionnaire was developed to cover different dimensions of exercise. Originally, the items were divided thematically into three subscales: (1) intentions to exercise, (2) consequences of not exercising, and (3) bodily signals; based on clinical experience, without performing a factor analysis. Because the response scale is reversed on positive statements, higher scores of the EED indicate more compulsivity and unhealthy exercise. The phrase “physically active” was used in statements to capture low intensity activity. Questions about workouts per week ranged from no workouts to more than five per week.
Results from the pilot study13 (50 eating disorder patients and 51 controls) showed good internal reliability, and significant discrimination between groups (sum score and subscales). Afterwards, three statements were rewritten, one because it did not discriminate between patients and controls and two statements because their meaning overlapped with other items. Three questions exploring quantity dimensions were included. The questions were similar to those used in The HUNT study, which is a longitudinal population health study in Norway.29 There are five alternatives for reporting frequency of exercise from “never” to “almost every day.” There are three alternatives for intensity from “I take it easy without breaking into a sweat or losing my breath” to “I push myself to near exhaustion,” and four response alternatives for duration of each exercise session from “<15 min” to “[mt]1 h.” These questions have been validated.29 Feedback from patients have shown that one of the new statements was difficult to understand (I feel/notice pain). Preliminary analysis showed that another statement (I'm physically active to be the first or best performer) had a considerably negative influence on reliability of the actual subscale and did not discriminate significantly between groups. These two statements have been excluded, and all analyses are performed on EED with 18 items. The same 6‐point Likert scale, which was reversed in positive statements, was kept in the revised version of the EED. To make interpretation easier, mean scores were reported in the validated version. The EED global score was calculated as a mean score of all items because of the different number of items in subscales.
The Eating Disorder Examination – Questionnaire 6.0 (EDE‐Q)
The EDE‐Q is a validated and well‐known self‐report questionnaire based on the Eating Disorder Examination interview, and investigates key eating disorder attitudes and behavior of the last 28 days.27 It consists of Global score and four subscales: Dietary restraint, Weight concern, Shape concern and Eating concern. Norwegian norms for EDE‐Q have been established.30 In this study, differences in Global score between patients and controls are reported. To measure convergent validity with the EED, a Global score above 2.530 and the exercise frequency (item # 18 of the EDE‐Q) were used to investigate the severity grading of the EED. The EDE‐Q cut‐off score of 2.5 was calculated by the mean value and one standard deviation in the Norwegian norms.30 The exercise item was “exercising more than 5 times per week during the last 28 days to control weight and shape.”27 The Cronbach's alpha coefficient for the whole sample in this study was 0.96, for patients 0.94, and controls 0.95.
Statistical Analyses
Statistical analyses were carried out using the SPSS version 21. Kolomorgov‐Smirnow test did not show normality of all EED data. To achieve consistent presentation of the data, results of parametric tests were reported (independent and paired t‐tests, one way ANOVA, Pearson's correlation). Nonparametric analyses were also performed. Any discrepancies between parametric and nonparametric results were reported. A Principal component analysis (PCA) was performed to explore the factor structure of the EED, including Kaiser‐Meyer‐Olkin measure of sampling adequacy (KMO), correlation matrix, two criteria for retaining factors (Kaisers and Scree plot) and oblique rotation (direct oblim), because correlations between factors could be expected. Chronbach alphas were calculated to investigate internal consistency. Univariate analyses adjusting for age differences between groups were performed. Effect size was calculated for comparative analyses, Cohens d for t test and eta squared ( 2) for ANCOVA analyses. Values of ≥0.70 were used as the criterion for acceptable level of internal consistency, significance levels were set at p < 0.05, and accepted level of factor loading at 0.4.
Missing Data
Missing data on single items of the EED were replaced by a calculated mean on the actual subscale for each participant. The proportion of missing EED data was 0.37%. EDE‐Q data from six patients were missing. These patients were excluded from analyses including EDE‐Q data. Missing data, which were not replaced by the mean, were marked clearly to show the different Ns in the actual analyses. This is reported in text and tables.
Results
Psychometric Properties of the EED
Mean (SD), group differences and 95% Confidence interval (CI) are presented in Table 2. As shown in the table, the EED discriminated significantly (p < .001) between groups. Analyses adjusted for age differences did not affect the significance level. Adjusted mean differences and 95% CI are presented in Table 2. The subscales of the EED are established through a PCA, and more information is provided later in the result section.
Table 2.
Differences in items, subscales and global score of the EED, with effect size, patients versus controls
| Items, Subscales, and Global Score | Patients n = 244 Mean (SD) | Controls n = 205 Mean (SD) | t (447) p values | Diffa | 95%CI | Effect Size Cohens d | Diffb Adjusted for Age | 95%CI |
|---|---|---|---|---|---|---|---|---|
| Compulsive exercise | ||||||||
| I am physically active to avoid dealing with negative emotions. | 2.45 (1.70) | 1.27 (1.18) | 8.46*** | 1.18 | 0.90–1.46 | 0.82 | 1.43 | 1.15–1.71 |
| It feels wrong if I can't be physically active every day. | 2.34 (1.85) | 1.00 (1.18) | 9.96*** | 1.33 | 1.04–1.63 | 0.87 | 1.50 | 1.19–1.81 |
| If I haven't been physically active I don't eat. | 1.84 (1.70) | 0.37 (0.82) | 11.38*** | 1.47 | 1.22–1.73 | 1.10 | 1.67 | 1.40–1.93 |
| If I haven't been physically active, I can't relax. | 2.20 (1.78) | 0.81 (1.15) | 9.70*** | 1.39 | 1.12–1.73 | 0.93 | 1.57 | 1.27–1.87 |
| If I haven't been physically active, I get a bad conscience. | 3.23 (1.76) | 2.05 (2.06) | 6.65*** | 1.19 | 0.83–1.54 | 0.63 | 1.33 | 0.96–1.70 |
| If I haven't been physically active, my body feels big. | 2.99 (1.77) | 1.77 (1.50) | 7.89*** | 1.23 | 0.91–1.53 | 0.75 | 1.34 | 1.01–1.66 |
| If I haven't been physically active, my body feels disgusting. | 2.95 (1.80) | 1.51 (1.45) | 9.32*** | 1.44 | 1.14‐1.75 | 0.89 | 1.61 | 1.28‐1.93 |
| I listen to my body. | 3.12 (1.30) | 1.64 (1.15) | 12.70*** | 1.48 | 1.25–1.71 | 1.21 | 1.51 | 1.27–1.58 |
| Subscale 1 mean score | 2.64 (1.40) | 1.30 (0.95) | 11.75*** | 1.35 | 1.12–1.57 | 1.13 | 1.49 | 1.26–1.73 |
| Positive and healthy exercise | ||||||||
| I enjoy being physical active. | 2.32 (1.58) | 1.76 (1.33) | 3.97*** | 0.56 | 0.30–0.84 | 0.38 | 0.53 | 0.24–0.82 |
| I like to exercise with other people. | 2.75 (1.57) | 1.64 (1.28) | 8.03*** | 1.11 | 0.84–1.38 | 0.77 | 1.01 | 0.73–1.30 |
| I am physically active to be healthy. | 2.16 (1.61) | 1.37 (1.26) | 5.64*** | 0.79 | 0.52–1.06 | 0.54 | 0.81 | 0.52‐1.10 |
| Subscale 2 mean score | 2.41 (1.36) | 1.59 (1.11) | 6.85*** | 0.81 | 0.58–1.04 | 0.66 | 0.78 | 0.54–1.03 |
| Awareness of bodily signals | ||||||||
| I notice when I get tired. | 1.68 (1.40) | 1.19 (1.14) | 4.04*** | 0.49 | 0.25–0.73 | 0.64 | 0.63 | 0.38–0.88 |
| I notice when I get thirsty. | 1.61 (1.58) | 0.92 (1.05) | 5.38*** | 0.69 | 0.44–0.95 | 0.52 | 0.78 | 0.51–1.05 |
| I notice when I get hungry. | 2.33 (1.63) | 0.88 (1.10) | 10.92*** | 1.45 | 1.19–1.71 | 1.05 | 1.62 | 1.35–1.90 |
| I notice when I feel fit/in shape. | 1.82 (1.34) | 1.05 (1.07) | 6.67*** | 0.77 | 0.54–1.00 | 0.64 | 0.88 | 0.64–1.12 |
| Subscale 3 mean score | 1.86 (1.18) | 1.01 (0.90) | 8.49*** | 0.86 | 0.66–1.05 | 0.81 | 0.98 | 0.77–1.19 |
| Weight and shape exercise | ||||||||
| I am physically active to become thin. | 3.20 (1.74) | 2.25 (1.50) | 6.24*** | 0.97 | 0.65–1.26 | 0.53 | 1.10 | 0.78–1.42 |
| I am physically active to burn calories I have eaten. | 2.87 (1.79) | 1.36 (1.31) | 10.17*** | 1.51 | 1.22–1.81 | 0.97 | 1.69 | 1.38–2.00 |
| I am physically active for appearance reasons. | 2.92 (1.79) | 2.42 (1.40) | 3.24*** | 0.50 | 0.19–0.80 | 0.32 | 0.75 | 0.44–1.06 |
| Subscale 4, mean score | 3.00 (1.60) | 2.01 (1.20) | 7.37*** | 1.00 | 0.73–1.26 | 0.71 | 1.18 | 0.90–1.46 |
| EED Global score | 2.49 (0.96) | 1.40 (0.65) | 13.88*** | 1.09 | 0.94–1.24 | 1.09 | 1.21 | 1.05–1.37 |
t test for independent samples, two tailed. p values: *** p < 0.001.
Diff: Mean difference between patients and controls and 95%.confidence interval (CI).
Diff: Mean difference between patients and controls adjusted for age. 95%CI: 95% confidence interval.
Cohens d: Small effect size = 0.2, medium = 0.5, and large = 0.8.
In patients, age and BMI were significantly negatively related (Pearson's r, two‐tailed) to EED Global score, r = −0.21, p < 0.01 (age), and r = −0.27, p < 0.01 (BMI). These correlations indicated that the EED Global score increased with lower BMI and younger age in patients. In the control group, the tendency was the same regarding age, but opposite regarding BMI.
In Table 3, the EED Global and subscale scores, and the effect size eta squared ( adjusted for age difference) in diagnostic groups are presented. The analyses are adjusted for age differences, without changing the original result.
Table 3.
EED scores (Global score and subscales) in diagnostic groups
| AN n = 79 Mean (SD) | BN n = 57 Mean (SD) | EDNOS n = 84 Mean (SD) | BED n = 24 Mean (SD) | F | Differencea p values | Bonferroni post hoc p values | Effect size Eta squared Adjusted for age η 2 | |
|---|---|---|---|---|---|---|---|---|
| EED | 2.54 (1.03) | 2.63 (0.98) | 2.52 (0.89) | 1.87 (0.63) | 4.00 | ** | BED vs. AN and EDNOS* | 0.03 |
| Global score | BED vs. BN** | |||||||
| EED | 2.75 (1.53) | 2.88 (1.34) | 2.63 (1.33) | 1.72 (0.89) | 4.42 | ** | BED vs. AN, BN** | |
| Compulsive | BED vs. EDNOS* | 0.04 | ||||||
| EED | 2.24 (1.48) | 2.44 (1.25) | 2.44 (1.30) | 2.79 (1.35) | 1.07 | NS | NS | 0.01 |
| Positive and healthy | ||||||||
| EED | 2.12 (1.16) | 1.72 (1.28) | 1.95 (1.11) | 1.00 (0.82) | 6.29 | *** | BED vs. AN*** | 0.05 |
| Bodily signals | BED vs. EDNOS** | |||||||
| EED | 2.81 (1.62) | 3.37 (1.61) | 3.06 (1.49) | 2.53 (1.63) | 2.13 | NS | NS | 0.03 |
| Weight and shape |
One way ANOVA F(3, 240). AN: anorexia nervosa, BN: bulimia nervosa, EDNOS: eating disorder not otherwise specified. BED: binge eating disorder.
In Bonferroni post hoc test, only significant relationships are reported.
p values: * p < 0.05, ** p < 0.01, and *** p < 0.001. NS: Not significant.
Effect size ‐ Eta squared η 2: small effect size = 0.02, medium = 0.13, and large = 0.26.
Reliability Testing
The Chronbach's alpha coefficient of the Global EED in the whole sample was 0.90. Subscale coefficients of the whole sample and patients are presented in Table 5. In controls, the Chronbach's alpha coefficients in subscales ranged from 0.81 to 0.85. All subscale items were tested for effect on α if each item was deleted, and none of the items affected the α‐level to a considerable level. The factors for corrected item‐total correlation ranged from 0.56 to 0.84. The results indicated an acceptable level of consistency.
Table 5.
PCA of the EED for the whole sample (N = 449) and patients (n = 244)
| Rotated Factor Loadings | ||||
|---|---|---|---|---|
| Factors and Items Factor 1 Compulsive Exercise | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
| If I haven't been physically active, I can't relax. | 0.96/0.95 a | −0.02 | −0.01 | −0.10 |
| It feels wrong if I can't be active every day. | 0.90/0.87 | −0.08 | −0.00 | −0.02 |
| If I haven't been physically active I don't eat. | 0.87/0.85 | 0.07 | −0.10 | −0.05 |
| If I haven't been physically active, I get a bad conscience. | 0.71/0.68 | 0.03 | 0.12 | 0.15 |
| If I haven't been physically active my body feels disgusting. | 0.65/0.58 | 0.04 | −0.00 | 0.32 |
| I am physically active to avoid dealing with negative emotions. | 0.61/0.57 | −0.17 | ‐.20 | 0.13 |
| If I haven't been physically active my body feels big. | 0.60/0.51 | 0.06 | 0.06 | 0.41/0.50 |
| I listen to my body. | 0.37/0.46 | 0.23 | −0.38 | 0.12 |
| Factor 2 | ||||
| Positive and healthy exercise | ||||
| I enjoy being physically active. | −0.23 | 0.89/0.85 | −0.00 | 0.08 |
| I am physically active to be healthy. | 0.04 | 0.85/0.84 | −0.06 | −0.14 |
| I like to exercise with other people. | 0.13 | 0.84/0.84 | 0.01 | −0.018 |
| Factor 3 | ||||
| Awareness of bodily signals | ||||
| I notice when I am thirsty. | −0.04 | 0.02 | −0.86/0.83 | 0.01 |
| I notice when I feel fit/in shape | −0.05 | 0.09 | −0.81/0.79 | 0.05 |
| I notice when I get tired. | −0.03 | −0.10 | −0.79/0.71 | −0.03 |
| I notice when I am hungry. | 0.12 | 0.04 | −0.77/0.82 | −0.02 |
| Factor 4 | ||||
| Weight and shape related exercise | ||||
| I am physically active to become thin. | −0.02 | 0.07 | −0.01 | 0.94/0.97 |
| I am physically active for appearance reasons. | 0.01 | −0.16 | −0.01 | 0.85/0.82 |
| I am physically active to burn calories I have eaten. | 0.29 | 0.09 | −0.11 | 0.64/0.76 |
| Eigenvalue | 7.53/7.25 | 3.05/2.98 | 1.66/1.84 | 0.91/0.93 |
| % of variance | 41.81/40.25 | 16.95/16.54 | 9.22/10.23 | 5.06/5.18 |
| Chronbach's alpha | 0.93/0.93 | 0.84/0.82 | 0.83/0.80 | 87/0.89 |
Factor loadings above 0.4 is marked in bold.
Patient group: Values are presented underscored in italic numbers.
Test‐Retest Reliability (N = 69)
Between test (T1) and retest (T2), the Pearson's correlation factor on Global score was .86 and ranged from .68 to .90 in subscales. Mean global scores (SD) were 1.41 (0.71) at T1 and 1.41 (0.70) at T2. No significant differences (paired sample t test, two‐tailed) were found between the two points of measurement on Global score t (68) = 0.22, p < 0.84, or subscales. Values in subscale 1 (compulsive) were t (68) = 1.00, p < 0.33, subscale 2 (positive): t (68) = −1.89, p < 0.07, subscale 3 (bodily signals): t (68) = 0.00, p = 1.00, and subscale 4 (weight and shape): t (68) = 0.49, p < 0.64. The nonparametric test (Wilcoxon test) showed similar results except for subscale 2: z = −2.3, p < 0.05, indicating significant difference between T1 and T2. The overall results indicated a satisfactory level of stability of the EED, despite the limited discrepancy of results on subscale 2.
Convergent and Discriminant Validity
Correlations between global score and subscales of the EED and EDE‐Q are presented in Table 4. Higher correlations were found between EED subscales representing compulsive elements of exercise and EDE‐Q weight/shape over concern than the other EED subscales. These associations indicated both convergent and discriminant validity between exercise measured by EED and symptoms of eating disorders measured by EDE‐Q.
Table 4.
Correlations between EED and EDE‐Q global scores and subscale scores
| EED Global Score | EED Compulsive | EED Positive and Healthy | EED Bodily Signals | EED Weight and Shape | |
|---|---|---|---|---|---|
| EDE‐Q Global score Whole sample (n = 443)a | 0.79** | 0.70** | 0.36** | 0.39** | 0.65** |
| EDE‐Q Global score Patient group (n = 238)a | 0.66** | 0.55** | 0.27** | 0.25** | 0.59** |
| EDE‐Q Global score Controls (n = 205) | 0.73** | 0.67** | 0.14* | 0.16* | 0.64** |
Pearson's r (two‐tailed). **Correlation significant at the 0.01 level. *Correlation significant at the 0.05 level.
EED: Exercise and Eating Disorders. EDE‐Q: Eating Disorder Examination Questionnaire.
Reduced N is due to missing EDE‐Q data in six patients.
Factor Structure of the EED, PCA
Results for the total sample indicated that all KMO values for statements were above 0.72. The KMO measure verified sampling adequacy (MSA = 0.91).31 Bartlett's test of sphericity X 2 (153) = 5717.388, p < 0.001, indicated sufficiently large correlations between items for performing a PCA. Analyses of Kaisers criterion and scree plot showed that both a three and a four‐factor solution could be justified. There were three factors with an eigenvalues above 1, and a fourth factor just below 1 (0.91). The inflexion point of the scree plot indicated a four‐factor structure. Changing from three to four factors, communality values increased from an average of 0.68 to 0.73, explained variance increased from 67.8 to 73.0%, and three items in factor 1 established the fourth factor. In the patient and control group, MSA values (respectively, 0.88 and 0.85) and Bartlett's test of sphericity (p < 0.001) were acceptable. A summary of the PCA analyses and Chronbach's alpha coefficient in subscales is presented for the whole sample and patient group in Table 5. Factor structure was similar for the control group, except for one item, and the eigenvalue of the fourth factor increased to 1.21. Through evaluation of statistical and clinical arguments, the final conclusion was to retain four factors. Items of each factor were investigated to see how they captured common themes and clinically relevant dimensions. The three items in the fourth factor were related to exercise for weight and appearance reasons, which have been looked on as an important factor both clinically and theoretically. Eating disorder patients regularly report exercising for weight and appearance reasons. The other factors covered dimensions related to compulsivity, healthy exercise, and awareness of bodily signals. As shown in the table, the loading of one statement (if I haven't been physically active, my body feels big) was above 0.40 in two factors. It was kept in the factor with the highest loading. Another statement, “I listen to my body,” was retained because it has clinical relevance31 and higher loading above 0.40 in the patient group, despite loading below 0.4 in the total sample.
Clinical Guide of Severity Grading of the EED Scale
To make interpretation of the EED for clinicians and the communication with patients easier, we have estimated a clinical severity scale. This scale is based on quartile groups of the EED global score in the patient group.
The results yielded the following classification based on global EED score: Group 1, global score <1.80 (no symptoms of compulsive exercise); Group 2, global score 1.80 − 2.39 (low severity); Group 3, global score 2.40 − 3.19 (moderate severity) and Group 4, global score > 3.20 (high severity). In Figure 1, the expected positive associations between EED severity groups and high level exercise for patients are shown. High level of exercise was defined as the highest alternative (frequency, intensity, and duration) of amount of exercise in the EED, together with exercising more than 5 times a week (EDE‐Q, # 18). The same tendency (see Fig. 1), was found in those with an EDE‐Q Global score above 2.5, 79.7% (n = 188), and in diagnostic groups, except for the BED group. None of the 24 BED patients reported a high level exercise.
Figure 1.
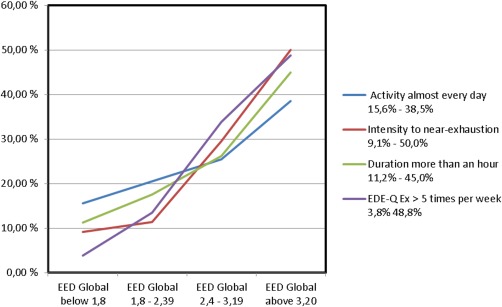
EED Global score divided into four severity groups (approximately quartiles). Activity measures of the EED and the exercise measure of the EDE‐Q (# 18 per week). Percentage of patients in each severity group are presented.
Discussion
All analyses confirmed adequate psychometric properties of the EED and a four‐factor solution. These results showed adequate test‐retest reliability and discriminant validity between patients and healthy controls across different dimensions of compulsive exercise. Analyses showed that this discrimination between groups was not affected by age differences. Convergent validity was demonstrated by the high correlations between compulsive exercise measured by the EED and eating disorder symptoms measured by the EDE‐Q. Findings indicate that the EED can be a useful assessment in eating disorder patients.
The EED is the first clinically derived, self‐report questionnaire developed specifically for use in treatment settings for eating disorder patients. Considerable debate surrounds the issue of how exercise should be addressed in treatment for eating disorders.32, 33 The EED may prove to be a useful contribution as an assessment tool tapping clinically relevant dimensions of compulsive exercise within a broader perspective than captured by existing questionnaires. To identify treatment goals and plan treatment, it is important to recognize and understand the different dimensions related to compulsive exercise among patients.
Consistent with existing research, the results confirmed that exercising to control weight, shape, and appearance are important features of excessive exercise.34, 35 The results also supported the complex and multidimensional nature of exercise in eating disorders, which is consistent with C. Meyer's cognitive‐behavioral maintenance model of compulsive exercise.3 The subscale that explained the greatest part of the variance in the EED scale was related to what we have defined as the compulsive elements of exercising. The compulsive scale consisted of elements, which are theorized to maintain this behavior. Exercising to avoid difficult emotions and the concern about consequences if exercise is restricted, postponed or interrupted are primary features of the compulsive scale on the EED. The importance of compulsive attitudes has also been highlighted in research related to a conceptual model of understanding the relationship between EEDs.36 Addiction models of excessive exercise report that withdrawal symptoms related to negative affect such as guilt, anxiety, and depression are involved in maintenance.37 In the EED, consequences of not exercising are included that are related to eating disorder symptoms, such as difficulty with regular meals and changes in perceived body image when they do not exercise. These elements are important to understand the complex nature of exercise in clinical samples of eating disorder patients, and they may directly affect treatment.
The two other subscales are related to healthy issues of exercise, which also is important. The positive effects of healthy exercise are well‐known, and it has been reported that healthy exercise may be a positive factor in treatment of eating disorder patients.10, 38 The ability to notice bodily signals is a component not focused on in other questionnaires. Awareness of physical signals, such as fatigue, thirst, etc., is a precondition for attending to these needs and regulating exercise in a healthy way. Hilde Bruch has highlighted difficulties with perceiving and interpreting bodily signals as a symptom of AN patients. In this study, these difficulties also appeared in the other diagnostic groups. When interpreting these two subscales, it is important to remember that the response scales are reversed, and low score indicates healthy exercise and good ability to recognize bodily signals, a high score indicates the opposite.
Correlations indicated that higher scores of the EED were associated with lower BMI and younger age in patients. The AN patients were on average younger and had a lower BMI than BN and EDNOS patients, but the age range was wide across groups. Analyses adjusting for age showed that age was a factor to consider, though it did not change the results. Our lack of differences between diagnostic groups in the patient sample diverged from a study that found the highest prevalence of compulsive exercise among AN patients compared to BN and EDNOS.6 However, similar levels of excessive exercise across diagnostic groups has been previously shown.39 Differences across studies may depend on different levels of compulsive exercise across samples, but it may also be due to differences in definitions and measures.5 In our sample, only BED patients were shown to have significantly lower scores on the global scale and two subscales (compulsive exercise and awareness of bodily signals). However, these results should be interpreted with caution because of the low number of BED patients in the sample. Still, it is in accordance with our clinical experience, that these patients express less compulsivity concerning exercise.
Compulsive exercise is not a symptom of all eating disorder patients, and the reported prevalence of compulsive exercise in other clinical samples has been estimated between 399 and 45.5%.6 It is not possible to compare these prevalence rates directly to the EED because different measures were employed. Yet, the proportion of patients with EED global score above 2.4 (estimated groups of moderate and high severity) was 50.8%, which falls in the same range as prior research. The estimated classification of severity (from “no symptoms of compulsive exercise” to “high severity”) based on EED global score in the patients is meant to assist clinical work with patients. This scale should be interpreted as gradually increasing severity, not strictly separate groups, giving an indication of how much attention is needed in treatment. However, it is important to have a more overall perspective too. Consistent with other research,40, 41 a continuum model, may highlight the dynamic nature of features like compulsive exercise and related topics. Convergent validity was demonstrated by correlations between the severity groups and increasingly higher levels of exercise. This supports the clinical relevance of the severity grading of the global EED score, and emphasizes the importance of evaluating both qualitative (attitudes and thoughts related to compulsivity) and quantitative measures of compulsive exercise in eating disorders. In accordance with other research, the qualitative measures are regarded as the clinically most important aspect of exercise behavior3, 14 and the amount or frequency of exercise is considered supplemental information in our clinic. An evaluation as to whether the amount of exercise is harmful or not depends on the individual's health and fitness level, and may also depend on prior history of exercise behavior.
Strengths and Limitations
A satisfactory sample size and acceptable number of patients in diagnostic groups strengthens this study.
Several limitations are important to consider. First, despite showing convergent validity with the EDE‐Q, the EED has not been validated against another exercise questionnaire. The exclusion of male students prohibits conclusions regarding gender differences. Patients were recruited from one eating disorder unit; and findings may not generalize to generalist treatment settings or community samples of eating disorders. Another limitation is lack of structured diagnostic reliability testing. However, well‐experienced ED clinicians made the diagnoses. The BED patients were quite few and that made the results in this group more uncertain. In our sample, the patients were on average older than controls. These differences were adjusted for by statistical analyses. The EED is based on self‐reported data, and bias associated with over‐and under‐reporting is possible. The same concern applies to the self‐reported weight and the possibility of unreported ED by participants in the control group.
Exercising despite pain and injury is a part of the DSM‐5 criteria of excessive exercise,4 and the importance has also been confirmed in research and clinical observations.23 This study reported psychometric data for the second version of the EED (version 2). Future versions of the EED will be designed to incorporate an item specific to awareness of physical pain and a timeframe of 4 weeks will be used to provide greater understanding of when changes occur. Additional research is also necessary to determine whether the EED captures changes through treatment, to investigate its potential predictive validity in determining outcome and to clarify relationships with other comorbidity and related symptomology. Comparing EED scores of compulsive exercisers with and without eating disorders and with athletes and other groups of physically active persons may also be interesting issues for future research.
Conclusion
The results of this study confirm the EED (version 2) as a valid and reliable measure of compulsive exercise in eating disorder patients. This brief, self‐report, easy‐to‐administer questionnaire includes 18 items divided into four subscales, which yield clinically relevant information that tap different dimensions of this phenomenon.
Acknowledgments
The authors wish to thank research staff member Hilde Kristin Vatterholm for all assistance and good work in the data colleting phase, and Deborah L. Reas, PhD for her great contribution in the writing of this article.
This article was published online on January 30, 2015. An error was subsequently identified. This notice is included in the online and print versions to indicate that both have been corrected April 25, 2015.
Conflict of interest: The authors are responsible for the writing and the content of this article and no conflicts of interest are reported.
References
- 1. Penas‐Lledo E, Vaz Leal FJ, Waller G. Excessive exercise in anorexia nervosa and bulimia nervosa: Relation to eating characteristics and general psychopathology. Int J Eat Disord 2002;31:370–375. [DOI] [PubMed] [Google Scholar]
- 2. Strober M, Freeman R, Morrell W. The long‐term course of severe anorexia nervosa in adolescents: Survival analysis of recovery, relapse, and outcome predictors over 10‐15 years in a prospective study. Int J Eat Disord 1997;22:339–360. [DOI] [PubMed] [Google Scholar]
- 3. Meyer C, Taranis L, Goodwin H, Haycraft E. Compulsive exercise and eating disorders. Eur Eat Disord Rev 2011;19:174–189. [DOI] [PubMed] [Google Scholar]
- 4. American Psychiatric A. Diagnostic and Statistical Manual of Mental Disorders, 5th ed Arlington: APA, 2013. [Google Scholar]
- 5. Meyer C, Taranis L. Exercise in the eating disorders: Terms and definitions. Eur Eat Disord Rev 2011;19:169–173. [DOI] [PubMed] [Google Scholar]
- 6. Dalle Grave R, Calugi S, Marchesini G. Compulsive exercise to control shape or weight in eating disorders: Prevalence, associated features, and treatment outcome. Compr Psychiatry 2008;49:346–352. [DOI] [PubMed] [Google Scholar]
- 7. Davis C, Katzman DK, Kaptein S, Kirsh C, Brewer H, Kalmbach K, et al. The prevalence of high‐level exercise in the eating disorders: Etiological implications. Compr Psychiatry 1997;38:321–326. [DOI] [PubMed] [Google Scholar]
- 8. Mond JM, Hay PJ, Rodgers B, Owen C. An update on the definition of “excessive exercise” in eating disorders research. Int J Eat Disord 2006;39:147–153. [DOI] [PubMed] [Google Scholar]
- 9. Shroff H, Reba L, Thornton LM, Tozzi F, Klump KL, Berrettini WH, et al. Features associated with excessive exercise in women with eating disorders. Int J Eat Disord 2006;39:454–461. [DOI] [PubMed] [Google Scholar]
- 10. Bratland‐Sanda S, Sundgot‐Borgen J, Ro O, Rosenvinge JH, Hoffart A, Martinsen EW. Physical activity and exercise dependence during inpatient treatment of longstanding eating disorders: An exploratory study of excessive and non‐excessive exercisers. Int J Eat Disord 2010;43:266–273. [DOI] [PubMed] [Google Scholar]
- 11. Vansteelandt K, Rijmen F, Pieters G, Probst M, Vanderlinden J. Drive for thinness, affect regulation and physical activity in eating disorders: A daily life study. Behav Res Ther 2007;45:1717–1734. [DOI] [PubMed] [Google Scholar]
- 12. Bamber DJ, Cockerill IM, Rodgers S, Carroll D. Diagnostic criteria for exercise dependence in women. Br J Sports Med 2003;37:393–400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Danielsen M, Bratberg GH, Ro O. A pilot study of a new assessment of physical activity in eating disorder patients. Eat Weight Disord 2012;17:e70–77. [DOI] [PubMed] [Google Scholar]
- 14. Adkins EC, Keel PK. Does “excessive” or “compulsive” best describe exercise as a symptom of bulimia nervosa? Int J Eat Disord 2005;38:24–29. [DOI] [PubMed] [Google Scholar]
- 15. Thompson JK, Pasman L. The obligatory exercise questionnaire. Behav Ther 1991;14. [Google Scholar]
- 16. Steffen JJ, Brehm BJ. The dimensions of obligatory exercise. Eat Disord 1999;7:219–226. [Google Scholar]
- 17. Brandon JE, Loftin JM, Thompson B. The eating and exercise behavior questionnaire: A validity assessment. Health Educ 1988;19:6–10. [PubMed] [Google Scholar]
- 18. Davis C, Brewer H, Ratusny D. Behavioral frequency and psychological commitment: Necessary concepts in the study of excessive exercising. J Behav Med 1993;16:611–628. [DOI] [PubMed] [Google Scholar]
- 19. Cash TF, Novy PL, Grant JR. Why do women exercise? Factor analysis and further validation of the reasons for exercise inventory. Percept Motor Skills 1994;78:539–544. [DOI] [PubMed] [Google Scholar]
- 20. Ogden J, Veale D, Summers Z. The development and validation of the exercise dependence questionnaire. Addict Res 1997;5:343–356. [Google Scholar]
- 21. Downs DS, Hausenblas H, Nigg CR. Factorial validity and psychometric examination of the exercise dependence scale revised. Meas Phys Edu Exerc Sci 2004;8:19 [Google Scholar]
- 22. Griffiths MD, Szabo A, Terry A. The exercise addiction inventory: A quick and easy screening tool for health practitioners. Br J Sports Med 2005;39:e30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Taranis L, Touyz S, Meyer C. Disordered eating and exercise: Development and preliminary validation of the compulsive exercise test (CET). Eur Eat Disord Rev 2011;19:256–268. [DOI] [PubMed] [Google Scholar]
- 24. Yates A. Compulsive exercise and the eating disorders. Levittown PA: Masel, 1991. [Google Scholar]
- 25. Bruch H. Perceptual and conceptual disturbances in anorexia nervosa. Psychosom Med 1962;24:187–194. [DOI] [PubMed] [Google Scholar]
- 26. American Psychiatric A. Diagnostic and statistical manual of mental disorders. Washington DC: APA, 2013. [Google Scholar]
- 27. Fairburn CG, Beglin SJ The Eating Disorder Examination Questionnaire (EDE‐Q 6.0) In Fairburn CG, editors. Cognitive behavior therapy and eating disorders. New York: Guilford Press, 2008. [Google Scholar]
- 28. Garner DM. Eating Disorder Inventory‐2 Odessa, FL: Psychological Assessment Resources, 1991. [Google Scholar]
- 29. Kurtze N, Rangul V, Hustvedt BE, Flanders WD. Reliability and validity of self‐reported physical activity in the Nord‐trondelag health study: HUNT 1. Scand J Public Health 2008;36:52–61. [DOI] [PubMed] [Google Scholar]
- 30. Ro O, Reas DL, Lask B. Norms for the eating disorder examination questionnaire among female university students in Norway. Nord J Psychiat 2010;64:428–432. [DOI] [PubMed] [Google Scholar]
- 31. Field A. Discovering statistics using SPSS. London: SAGE Publications Ltd., 2009. [Google Scholar]
- 32. Bratland‐Sanda S, Rosenvinge JH, Vrabel KA, Norring C, Sundgot‐Borgen J, Ro O, et al. Physical activity in treatment units for eating disorders: Clinical practice and attitudes. Eat Weight Disord 2009;14:e106–e112. [DOI] [PubMed] [Google Scholar]
- 33. Hechler T, Beumont P, Marks P, Touyz S. How do clinical specialists understand the role of physical activity in eating disorders. Eur Eat Disord Rev 2005;13:125–132. [Google Scholar]
- 34. Fairburn CG, Cooper Z. The eating disorder examination In: Fairburn CG, Wilson GT, editors. Binge eating: Nature, assessment and treatment, 12th ed New York: Guilford Press, 1993, p. 317 ‐360. [Google Scholar]
- 35. Dalle GR, Calugi S, Marchesini G. Compulsive exercise to control shape or weight in eating disorders: Prevalence, associated features, and treatment outcome. Compr Psychiat 2008;49:346–352. [DOI] [PubMed] [Google Scholar]
- 36. Cook B, Hausenblas H, Tuccitto D, Giacobbi PR. Eating disorders and exercise: A structural equation modelling analysis of a conceptual model. Eur Eat Disord Rev 2011;19:216–225. [DOI] [PubMed] [Google Scholar]
- 37. Bamber D, Cockerill IM, Carroll D. The pathological status of exercise dependence. Br J Sports Med 2000;34:125–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Hausenblas HA, Cook BJ, Chittester NI. Can exercise treat eating disorders?. Exerc Sport Sci Rev 2008;36:43–47. [DOI] [PubMed] [Google Scholar]
- 39. Solenberger SE. Exercise and eating disorders: A 3‐year inpatient hospital record analysis. Eat Behav 2001;2:151–168. [DOI] [PubMed] [Google Scholar]
- 40. Elbourne KE, Chen J. The continuum model of obligatory exercise: A preliminary investigation. J Psychosom Res 2007;62:73–80. [DOI] [PubMed] [Google Scholar]
- 41. Espeset EM, Nordbo RH, Gulliksen KS, Skarderud F, Geller J, Holte A. The concept of body image disturbance in anorexia nervosa: An empirical inquiry utilizing patients' subjective experiences. Eat Disord 2011;19:175–193. [DOI] [PubMed] [Google Scholar]