

Abstract
Knee trauma and effusion are common Emergency Department presentations. This article outlines the clinician's sonographic approach to knee effusion detection and localisation. A case where lipohaemarthrosis was detected with ultrasound is demonstrated, and the characteristic appearance of this pathology discussed. The sonographic detection of the associated tibial fracture is also demonstrated.
Keywords: knee effusion, lipohaemarthrosis, tibial plateau fracture, trauma
Background
Knee pain and swelling are common presentations to the Emergency Department. Differential diagnoses includes trauma, inflammatory arthropathies, crystal deposition arthropathies, infection, osteoarthritis and overuse, and rarely tumour. 1 Traditionally, assessment in the Emergency Department involves taking a history, performing an examination (often limited by pain acutely) and arranging investigations. Imaging usually begins with a plain radiograph, and if necessary progresses to CT where bony injury is suspected, or MRI where complex ligamentous and meniscal injury is considered. 2 Joint aspiration is commonly performed to determine the origin of an effusion (particularly to exclude bacterial infection), and occasionally to relieve pain.
The increasing availability of ultrasound at the bedside in Emergency Departments enables the clinician with relatively basic ultrasound training to rapidly assess the joint, particularly for the presence or absence of effusion, as well as determining the best site at which to aspirate it. Hoppmann, et al. showed that fourth‐year medical students can learn to identify knee effusions with ultrasound following a brief introductory lecture and 15 minutes supervised hands‐on scanning practice. 3
Those with greater expertise in musculoskeletal ultrasound can assess the joint and surrounding structures for a far broader range of pathology, including inflammatory findings and their response to therapy; this is well described in the rheumatology literature. 4
Tibial plateau fractures may be subtle and can be missed on plain radiography. CT scan is the imaging investigation of choice if the diagnosis is uncertain, and also to characterise the position of bone fragments prior to operative intervention. The fracture is generally caused by lateral or medial force to the knee, or by axial compression. These fractures frequently require operative intervention. 5
When the tibial plateau fractures, both blood and fat (from the bone marrow) escape into the joint. This results in a joint effusion termed a lipohaemarthrosis. The fat forms a layer above the blood creating a linear fluid level. A horizontal beam lateral radiograph is recommended as this will optimise visualisation of the lipohaemarthrosis, which in itself is a very specific (although not particularly sensitive) sign of intra articular fracture. 6 Where there is little joint movement, the blood and serum may separate, with red cells settling below a layer of serum. Thus occasionally a double fluid level is present within a lipohaemarthrosis. A simple haemarthrosis from bleeding into the joint without disruption of the bony cortex does not contain the fat layer. Non traumatic joint effusion is most commonly anechoic throughout, although where there is purulent material or other intra articular debris the fluid may appear echogenic.
The case
A young man presented after falling off his surfboard and twisting his knee. He was unable to weight bear. Clinically it was felt this was likely to represent cruciate ligament injury, with an associated tense haemarthrosis. As his pain was severe the clinician involved was considering aspirating the effusion. This would not be routine practice as there is a small risk of introducing infection, but aspiration is occasionally performed to ease pain. An ultrasound of the knee was requested of one of the department's ultrasound qualified Emergency Physicians.
Technique – clinically assessing for knee effusion
Prior to performing an ultrasound the clinician sonologist initially assesses the patient clinically. History guides the clinician as to the likely aetiology, and then orthopaedic examination commonly proceeds in the “Look, Feel, Move, Special tests” sequence, searching for clues as to the pathology.
Inspecting a knee with a large effusion reveals the typical appearance of fullness in the suprapatellar regions both medially and laterally. Inspection may also suggest other traumatic pathology such as dislocation or fracture, prepatellar bursitis, or patellar tendon or quadriceps rupture.
Palpation may reveal the typical bouncy fluctuation of a large effusion. A moderate to large effusion can be demonstrated with the patellar tap sign, as the distended joint holds the patella off the femoral condyles, only to have the examiner ballot the two together on examination. For smaller effusions fluid displacement tests are used. In these fluid from one side of the joint is milked to the other where it may form a bulge and be more readily detected. 7
Technique – sonographically assessing for knee effusion
This is a very simple and easily learned approach to clinical ultrasound of the knee that aims only to detect and potentially drain effusion.
The suprapatellar scan of the knee in 30 degrees flexion has been found to be the most sensitive position to detect synovial fluid in knee joints. It is important however to assess the three major suprapatellar pouch recesses: midline suprapatellar, medial parapatellar and lateral parapatellar. This is particularly important when considering aspiration of an effusion, when assessing for the most accessible and largest pocket of fluid. 8 , 9
A linear transducer with musculoskeletal presets is usually selected, unless the leg is very large, when a curvilinear lower frequency transducer may be required (Figures 1–4).
Figure 1.

Positions for ultrasound probe when examining for knee effusion.
Figure 4.

A small anechoic knee effusion is demonstrated in from the midline suprapatellar approach. The normal concavity of the quadriceps tendon is maintained. The fluid lies anterior to the prepatellar fat pad that directly abuts the femur, and posterior to the anterior suprapatellar fat pad that lies behind the quadriceps tendon.
Figure 2.

Plain horizontal beam lateral radiograph of the knee with an effusion. Note the fullness of the suprapatellar pouch. 1 Quadriceps; 2 Effusion; 3 Femur; 4 Patella; 5 Patellar tendon; 6 Tibia; 7 Ultrasound transducer position in midline sagittal section.
Figure 3.

This is a panoramic ultrasound image of a similar effusion and demonstrates the image acquired with the transducer in the midline sagittal plane. 1 Subcutaneous fat; 2 Quadriceps; 3 Effusion; 4 Prefemoral fat pad; 5 Femur; 6 Patella; 7 Acoustic shadow.
An effusion is usually seen as a hypoechoic collection, however blood or purulent debris may create fine particulate material that makes the effusion more echogenic in appearance.
The patient should be supine, with the knee resting on a pillow or other support, at 30 degrees flexion.
Take a sagittal section of the knee in the midline, with the transducer just touching the superior pole of the patella distally. Move the probe proximally to assess the upper recesses of the suprapatellar pouch.
The next step is to explore the lateral and medial para and suprapatellar regions in transverse and longitudinal planes. An effusion bulges out between the lateral and medial borders of the patella and the femoral condyles (Figures 5–6).
Figure 5.
A tense haemarthrosis is seen, with marked distension of the suprapatellar pouch and the presence of fine particulate debris (consistent with blood in the context of trauma) in the effusion. Pyarthrosis may have a similar appearance, but can usually be distinguished clinically.
Figure 6.

This is a CT axial image taken toward the superior pole of the patella. It shows how a large effusion protrudes into the lateral and medial suprapatellar recesses between patella and femoral condyles.
Where the aim is aspiration the effusion is explored to determine its most most accessible point (usually the most superficial and the largest pocket of fluid). This is often at the lateral lower thigh, at a level parallel with the upper pole of the patella, just distal to the body of vastus lateralis. This correlates with the traditionally described superior lateral approach to knee aspiration (Figures 7–8).
Figure 7.

Where the effusion is small pressure on the opposing recess will displace fluid toward the examining ultrasound transducer.
Figure 8.

This is a transverse view of the lateral suprapatellar recess, just proximal to the patella. The fine particulate echogenic material in the large effusion is blood.
Where there is a small effusion, milking the joint by compressing the opposite side increases the amount of fluid available for aspiration on the procedural side.
Where there is debris in the joint it can be seen to swirl with probe pressure.
When the optimal site for aspiration is selected, it is marked and if the target is large a standard aseptic no touch technique is used for aspiration. Where the target effusion is smaller, real time ultrasound guided aspiration is preferred. Ensuring a sterile probe cover and full aseptic technique is essential.
More distal drainage sites (patellar and intrafrapatellar) may also be ultrasound guided.
The case
The suprapatellar pouch is distended with fluid, however an echogenic layer of fluid (fat) lies above the relatively anechoic blood. This is typical of lipohaemarthrosis (Figure 9).
Figure 9.

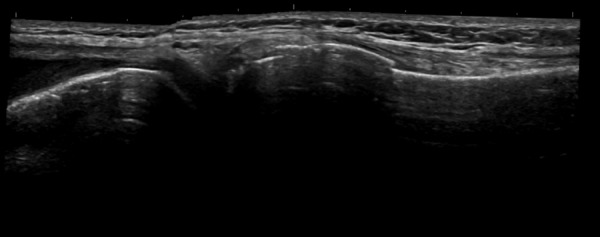
This is a panoramic midline sagittal ultrasound image of the suprapatellar region of the injured knee.
Fat is echogenic on ultrasound, and this is the appearance of a lipohaemarthrosis. The fat layer lying above the blood layer. This can also be demonstrated on plain radiography when a horizontal beam lateral view of the knee is taken. In the case of plain radiography the fat and blood create a fluid level where the fat is relatively radiolucent compared to blood (Figure 10). 10
Figure 10.

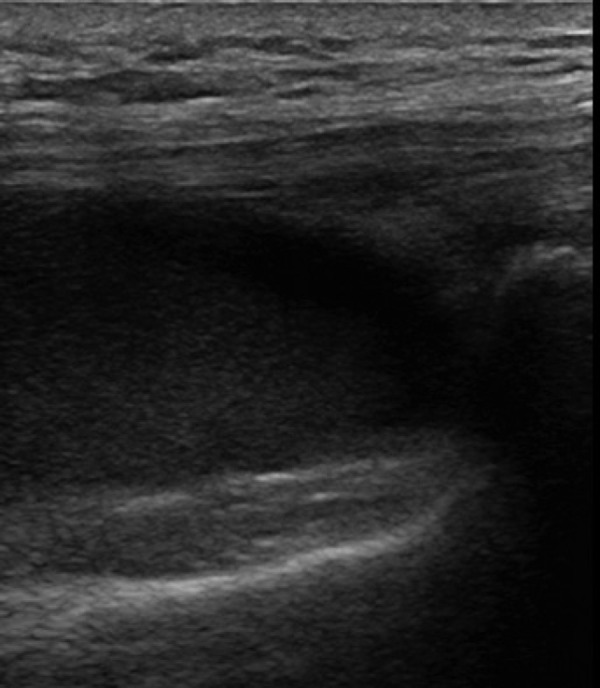
Here the lipohaemarthrosis is demonstrated in transverse section, in the medial parapatellar recess of the joint space. The synovial cavity is distended and a fluid level demonstrated.
Finding a lipohaemarthrosis strongly suggests intraarticular fracture, and further investigation to determine the site of fracture is mandated. In this case simply moving the transducer distally over the proximal tibia demonstrated a clear step in the cortex and the diagnosis of tibial plateau fracture was confirmed (Figures 11–12).
Figure 11.

Lateral knee plain film taken with horizontal beam, demonstrating the lipohaemarthrosis with radiolucent fat lying above the blood in the effusion.
Figure 12.
This ultrasound shows the distal femur, knee joint and proximal tibial. A clear step is seen in the tibial cortex confirming the presence of a tibial fracture.
Key Learning Points
Ultrasound to detect knee effusion is easily learned.
The patient should be supine with the knee resting on a pillow and flexed to 30 degrees.
Explore the suprapatellar bursa in the midline, then medially and laterally to define the size and character of the effusion and optimal site for aspiration.
While most effusions are hypoechoic, blood and pus may be echogenic, and in the case of lipohaemarthrosis a fluid level with echogenic fat will lie above the hypoechoic blood.
Finding a lipohaemarthrosis should trigger search for occult fracture.
Fractures can be demonstrated sonographically, by a step in the adjacent cortex. Associated haematoma and tenderness are usually present (Figure 13).
Figure 13.

CT further confirms the tibial plateau fracture.
Acknowledgement
The author wishes to thank Dr Tor Ercleve for the illustration included in this article.
Videos 1 & 2.

The first video demonstrates a large acute haemarthrosis. The fine particulate suspended debris is blood. Pressure with the probe compresses the tense effusion and the blood can be seen swirling around.
Video 1 URL: http://youtu.be/WN393spKHFA

The second video demonstrates a smaller haemarthrosis where clot has formed. Milking fluid from the opposite side of the knee makes the pocket of fluid on the side being examined larger.
Video 2 URL: http://youtu.be/CLkp7WFW1QQ
References
- 1. Johnson MW. Acute knee effusions: a systematic approach to diagnosis. Am Fam Physician 2000; 61 (8): 2391–400. [PubMed] [Google Scholar]
- 2. Koplas M, Schils J. The painful knee: choosing the right imaging test. Cleve Clin J Med 2008; 75 (5): 377–84. [DOI] [PubMed] [Google Scholar]
- 3. Hoppmann R1, Hunt P, Louis H, Keisler B, Richeson N, Rao V, Stacy J, Howe D. Medical student identification of knee effusion by ultrasound. Rheumatology, 2011. Epub 2011. [DOI] [PMC free article] [PubMed]
- 4. Vlad V, Iagnocco A. Ultrasound of the knee in rheumatology. Med Ultrasound 2012; 14 (4): 318–25. [PubMed] [Google Scholar]
- 5. Cole PJ, Watson T, Schatzker J. Tibial Plateau Fractures. In Browner B, Levine A, Jupiter J, Trafton P, editors. Skeletal Trauma, 4th edn, Saunders; 2009: p. 2074–2130 [Google Scholar]
- 6. Ferguson J, Knottenbelt J. Lipohaemarthrosis in knee trauma: an experience of 907 cases. Injury 1994; 25 (5): 311–12. [DOI] [PubMed] [Google Scholar]
- 7. Physiopedia; Effusion tests [Internet] [cited July 2014]. Available at http://www.physio‐pedia.com/Effusion_tests.
- 8. Mandl P, Brossard M, Aegerter P, Backhaus M, Bruyn GA, Chary‐Valckenaere I, et al. Ultrasound evaluation of fluid in knee recesses at varying degrees of flexion. Arthritis Care Res 2012; 64 (5): 773–79. [DOI] [PubMed] [Google Scholar]
- 9. Hong BY1, Lim SH, Cho YR, Kim HW, Ko YJ, Han SH, Lee JI. Detection of knee effusion by ultrasonography. Am J Phys Med Rehabil 2010; 89 (9): 715–21. [DOI] [PubMed] [Google Scholar]
- 10. Knipe H, Gaillard F. Lipohaemarthrosis. Radiopedia.org [Internet] [cited July 2014]. Available at http://radiopaedia.org/articles/lipohaemarthrosis.