

Abstract
Background:
Implantation of joint prosthesis, either in the knee or in the hip, may cause some problems such as an infection, so that a timely treatment is essential. In this respect, discovering a marker detecting the incidence of an infection is one of the requirements of arthroplasty. The present study was conducted to determine variations of two markers in arthroplasty and infection incidence in Iranian patients.
Materials and Methods:
This prospective study was carried out in Isfahan’s educational treatment centers from 2009 to 2011 on patients undergoing total knee arthroplasty (TKA) and total hip arthroplasty (THA) surgical operations. The erythrocyte sedimentation rate (ESR) was measured by Sed rate device (Lena) and C-reactive protein (CRP) by autoanalyzer device (Erba) with the unit of ng/dL. The patients underwent ESR and CRP tests the day before operation, the day of operation, and 1, 2, 5, and 15 days and 1, 3, 6, and 12 months after operation.
Results:
Mean ESR increased during the first 5 days then decreased gradually lasting for 3 months. After 1 year it increased to a level higher than before the operation. The variations in ESR values were 19.1 ± 12.9 before the operation and 21.14 ± 10.8 after 1 year with significant difference (P < 0.001). The level of CRP had an upward trend from the first day after operation and reached its maximum on the second day, then had a downward trend up to 1 month after the operation; however, it did not reach its preoperative level during 1 year.
Conclusion:
ESR and CRP and their variations can be suitable factors to detect probable infections in patients undergoing TKA and THA operations.
Keywords: C-reactive protein, erythrocyte sedimentation rate, total knee arthroplasty, total hip arthroplasty
INTRODUCTION
Due to the high prevalence of arthritis among people, total replacement of knee and hip joints is rather common. The most prevalent arthritis is osteoarthritis, which is caused by aging, congenital anomalies, and a history of trauma. Other candidates for this operation are those with fracture in knee or hip joints, rheumatoid arthritis, and aseptic necrosis.[1]
Although such operations have resulted in a great relief for patients, they may be accompanied with serious complications such as infections affecting the result of operation and patient’s condition.
Timely diagnosis of an infection can be effective in treatment of the infection. One way of early diagnosis of infections is the use of C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) markers.[1]
ESR is a hematological condition, which increases when one’s body is affected by an infection, inflammation, major stressors, and autoimmune diseases. This is a time-dependent test measured according to sedimentation rate of red blood cells and its unit is mm/h.[2]
CRP is a protein produced in the liver due to an inflammation in the body. CRP test can be used as a high sensitive test to detect infections.[2]
The studies done in different countries, including Sweden, Korea, America, and Turkey,[1,2,3,4,5,6,7,8,9] on normalization process of ESR and CRP after total knee arthroplasty (TKA) and total hip arthroplasty (THA) operations have reported different facts and figures. However, no study has been conducted in this regard in Iran. Given that ESR and CRP are markers of infections, patients unusual normalization process of ESR and CRP must be followed up and assessed again using bone scan[10] or other methods such as puncture and culture and ultimately, surgical operation. Conducting the present study was necessary because few studies have been done in this regard, there is no relevant study in Iran, and the number of TKA and THA operations done in Isfahan’s educational treatment centers is high. In this respect, the present study was conducted to determine variations in ESR and CRP in TKA and THA operations in patients going to Isfahan’s educational treatment centers from 2009 to 2011. So far, numerous studies have been conducted in different parts of the world on ESR and CRP as markers of infection in patients, but have shown contradictory results. According to these different results, it seems that race and relevant factors such as level of public health and environmental factors affect the process. Therefore, the present study was conducted to determine variations in these two markers in arthroplasty and incidence of infection in patients.
MATERIALS AND METHODS
This prospective study was carried out in Isfahan’s educational treatment centers from 2009 to 2011. The study population was patients undergoing TKA and THA surgical operations, with no history of inflammatory, infectious, and chronic diseases. The exclusion criteria of the study were patients' failure to go to the centers for further followups, patient’s death prior to completion of the study, impossibility of patient’s follow-up due to immigration and moving to another place and lack of access to patients, prosthetic fracture, and those with proved infection.
The ESR was measured through infrared technique using Sed rate device (Lena). The CRP was measured through turbidimetry using autoanalyzer device (Erba) and its unit is ng/dL.
The patients underwent ESR and CRP tests the day before operation, the day of operation, and 1, 2, 5, and 15 days and 1, 3, 6, and 12 months after operation. The patients with unusual normalization process of ESR and CRP, especially complaining patients, underwent bone scan and followed up for 1 year in order to detect the incidence of infection. Consequently, the patients with proved infection were excluded from the study.
The collected and revised data were analyzed using SPSS18 software. The statistical test used for comparing mean ESR and CRP in different temporal intervals was repeated measures analysis of variance (ANOVA).
RESULTS
In this study, 80 patients who were candidates for TKA and THA operations were examined, of whom 35 patients were candidates for TKA and 45 others were candidates for THA. The mean age of the patients was 63.3 ± 10.7 years with the range of 31–79 years. Furthermore, the mean age of patients who were candidates for TKA and THA was 65.9 ± 8.6 and 61.3 ± 11.8 years, respectively. Based on a t test, mean age of the two groups did not differ significantly (P = 0.053).
Regarding gender distribution, 27 patients (33.8%) were male and 53 patients (66.3%) were female. Number of male patients in TKA and THA groups was 8 and 19 (22.9% vs. 42.2%), respectively, although the Chi-square test did not show any significant difference in this regard (P = 0.07).
Table 1 shows mean variations in the level of ESR on the day before operation (day zero), the day of operation, and 1, 2, 5, and 15 days and 1, 3, 6, and 12 months after operation for all patients in separate groups. According to table 1, the mean ESR had an upward trend during the first 5 days and then decreased gradually. This reduction trend lasted up to 3 months; however, after 1 year it increased to a level higher than that of before operation. Analysis by repeated measures ANOVA test showed that variations in ESR of all the patients before operation and after 1 year were significantly different (P < 0.001). However, the analysis by paired t test showed no significant difference in the level of mean ESR before operation and after 1 year (P = 0.12). Table 1 also shows mean ESR before the operation up to 1 year after the operation for both groups in isolation. The mean ESR of both groups increased during the first 5 days and then decreased. Analysis by repeated measures ANOVA test showed that variations in ESR of TKA and THA groups were not significantly different (P = 0.48). Figure 1 shows variations in ESR before operation up to 1 year after operation. Figure 2 also shows variations in ESR in both the groups. It must be mentioned that age and gender of the patients did not affect the variations in ESR (P > 0.05).
Table 1.
Variation of mean±SD of ESR befrore and after surgery
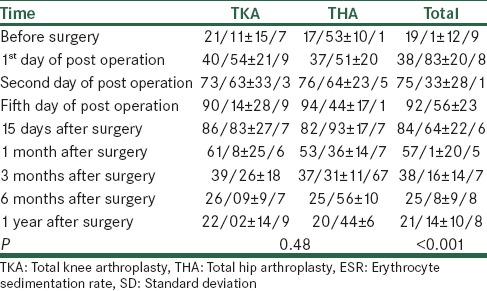
Figure 1.
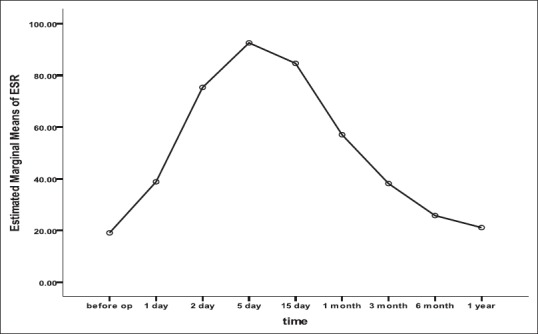
variations in ESR before operation up to 1 year after operation in all patients
Figure 2.
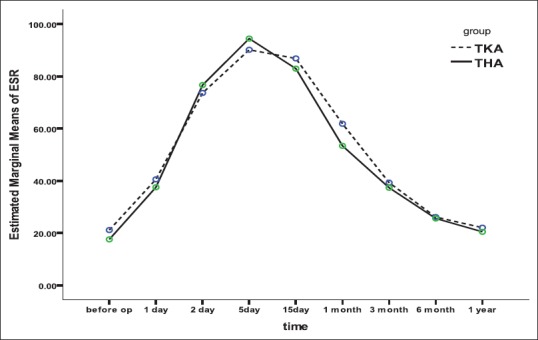
variations in ESR in both the groups(TKA, THA)
The level of CRP had an upward trend from the first day after operation and reached its maximum on the second day, then had a downward trend up to 1 month after the operation; however, it did not reach its preoperative level during 1 year.
The mean CRP values before TKA operation up to 1 year after the operation for all patients are shown in Table 2. Based on the table, CRP before operation up to 1 year after the operation was 4.07 ± 2.9 and 13.9 ± 9.6, respectively. The analysis of data by repeated measures ANOVA showed that the variations in CRP changed significantly within 1 year (P < 0.001). Figure 3 also shows variations in CRP within 1 year. According to the results, the mean CRP variation before operation up to 1 year followed a similar trend in both groups as there was no significant difference between groups in this regard based on repeated measures ANOVA (P = 0.41). Figure 4 shows variations in CRP for both groups in isolation. It is noteworthy that age and gender of the patients did not affect the variations in CRP (P > 0.05).
Table 2.
Variation of mean±SD of CRP befrore and after surgery
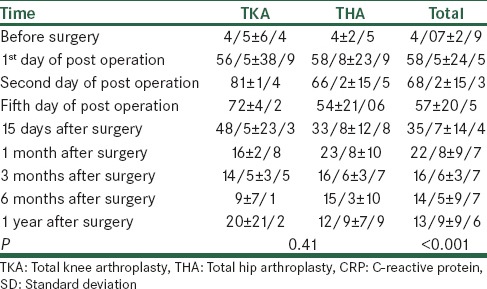
Figure 3.
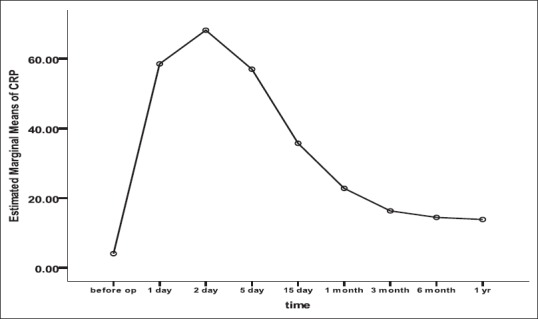
variations in CRP within 1 year in all patients.
Figure 4.
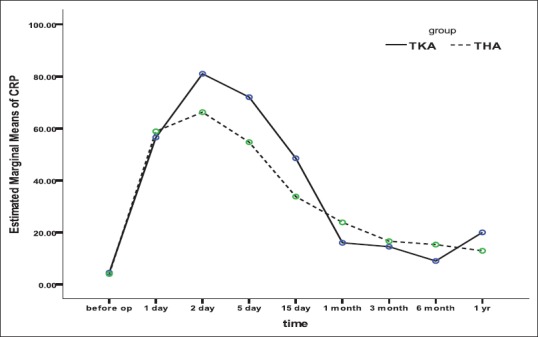
variations in CRP for both groups in isolation.
During the study, normalization process of ESR and CRP was abnormal in four (5%) patients who underwent bone scan. The result of the bone scan of two patients was negative, however, the positive result in two other patients proved the presence of infection during the operation, of which, one patient had undergone TKA operation and the other had undergone THA operation, and there was no significant difference between both the groups based on Fisher’s exact test (P = 1). Regarding gender distribution, 33.8% of patients were male and 66.3% of patients were female. Percentage of male patients in TKA and THA groups was 22.9% and 42.2%, respectively. The gender distribution did not show any significant difference between the groups. Considering lack of significant difference between both groups in terms of age and gender distribution, confounding effect of these two factors was neutralized, so the two groups were comparable.
DISCUSSIONS
A prospective study done in the University of British Columbia on 151 patients who were supposed to undergo revision TKA treatment, examined the presence of an infection through measuring ESR and CRP, in which, 45 patients were proved to have infection. In the above study, ESR with sensitivity of 0.93, specificity of 0.86, and accuracy of 0.86 and CRP with sensitivity of 0.91, specificity of 0.86, and accuracy of 0.88 were proved to be effective in detecting infections. Therefore, ESR and CRP can provide appropriate information on the presence of or absence of an infection before surgical interventions in patients who undergo knee arthroplasty due to feeling pain in this area.[3]
In a study done in an academic center in Spain on the patients who had undergone TKA and THA operations, their level of CRP was measured before operation and 1, 2, 3, 15, 42, and 150 days after operation, in which, the maximum level was related to 2 days after operation, total CRP in TKA patients was higher than that in THA patients, and returning to the preoperative normal level lasted 150 days. However, mean CRP was high up to the 42nd day and the conclusion was made based on the fact that if the increase in CRP continues up to 3 days after operation, it may be a marker of surgical problems such as infections.[4]
A study done in Turkey on 28 patients who had undergone joint replacement operation (TKA and THA) due to osteoarthritis showed maximum level of CRP 2 days after operation and its returning to the normal level on the 21st day in THA patients and after 60 days in TKA patients. In the above study, ESR reached its maximum 5 days after operation and returned to the preoperative level after 3 months and 9 months in THA and TKA operations, respectively.[5]
A study done in Sweden on four types of elective orthopedic surgeries examined the level of ESR and CRP and their normalization rate in primary THA, revision THA, and unicondylar TKA. The study showed that CRP reached its maximum on the 3rd day of revision arthroplasty and on the 2nd day in unicondylar TKA and it returned to the normal level on the 21st day. Furthermore, ESR reached its maximum after 5 days and it returned to the normal level on the 42nd day in patients without surgical complications.[6]
Another study in Scotland compared the level of CRP in patients who had undergone THA and TKA operations before and after operations, in which, maximum level of CRP was detected 2 days after operation and CRP in TKA operation was significantly higher than that in THA operation. The normalization rate of CRP in THA and TKA patients was equal.[7]
In a study done in Korea, levels of ESR and CRP were examined before operation and 2, 4, 5, 7, 14, 40, and 90 days after operation in patients who had undergone unilateral and bilateral TKA. In the above study, the level of CRP increased after 2 days and returned gradually to the normal level up to 40 days and the level of ESR reached its maximum on the 5th day and returned to the normal level after 90 days. In patients who underwent TKA of the contralateral joint, after recovery from the first operation, CRP variations were similar to those of patients who underwent TKA for the first time, or underwent unilateral TKA, however, CRP level was higher in bilateral TKA than that of unilateral TKA patients. The level of ESR in the bilateral operation within 2 days after operation was higher than that of the other two groups; however, from the 3rd day after operation, variations in ESR of all groups were similar to each other. There were two reduction peaks in CRP level, of which, one happened on the 14th day and the other happened on the 40th day after operation. The ESR level increased from the first day after operation, reached its maximum on the 5th day, and returned to preoperative level on the 90th day. The study also showed that process of variation in ESR and CRP is apart from each other. The level of CRP increased more quickly than that of ESR. Compared with variation of ESR, the rate of variations in CRP in all the patients was higher; the extent of abnormal variations was lower and the correlation between its levels before and after operation was lower.[8]
Another study done in Thailand on 49 patients who had undergone TKA due to osteoarthritis examined variations in CRP and ESR during days before operation and 0, 2, 6, and 14 days, and 26 weeks after operation. The result was that the level of CRP increased on the first day after operation and returned to its normal level within 6 weeks after operation. ESR level also increased within 2 weeks after operation and returned to its normal level within 26 weeks after operation.[9]
It has been observed that ESR and CRP in minor surgical operations such as arthroscopy are not suitable criteria for detecting infections; however, they can be effective in major surgeries.[11]
The objective of the present study was to determine and compare variations in ESR and CRP in TKA and THA operations in patients going to Isfahan’s educational treatment centers from 2009 to 2011. In this study, 45 patients who underwent TKA and 35 patients who underwent THA operation were examined. The mean age of the patients was 63.3 ± 10.7 years with a range of 31–79 years. Furthermore, the mean age of patients who were candidates for TKA and THA was 65.9 ± 8.6 and 61.3 ± 11.8 years, respectively. The mean age of the two groups did not differ significantly. Given a lack of significant difference between both the groups, the confounding effect of these factors was more likely neutralized, so the two groups were comparable.
According to the obtained results, the mean ESR had an upward trend during the first 5 days and then decreased gradually. This reduction trend lasted for 3 months; however, after one year it increased to a level higher than that of before operation. Variations in ESR in all patients before operation and after one year were significantly different; however, they were not significantly different between TKA and THA groups.
The level of CRP had an upward trend from the first day after operation and reached its maximum on the second day, then had a downward trend up to one month after the operation; however, it did not reach its preoperative level during 1 year.
Moreover, the results showed that joint replacement such as knee and hip arthroplasty increases ESR and CRP markers, although both markers reached their normal level after a while. However, given that these two markers increase in inflammations and infections, patients with high ESR and CRP that do not follow the normalization process according to the available curve, especially symptomatic patients, must be studied. Puncture, culture, and bone scan are methods to detect infections in patients undergoing joint replacement. In general, ESR and CRP and their variations can be suitable factors to detect probable infections in patients undergoing TKA and THA operations. Considering the results of the present study, further studies are required in this regard.
Footnotes
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Rashiq S, Finegan BA. The effect of spinal anesthesia on blood transfusion rate in total joint arthroplasty. Can J Surg. 2006;49:391–6. [PMC free article] [PubMed] [Google Scholar]
- 2.Honsawek S, Deepaisarnsakul B, Tanavalee A, Sakdinakiattikoon M, Ngarmukos S, Preativatanyou K, et al. Relationship of serum IL-6, C-reactive protein, erythrocyte sedimentation rate, and knee skin temperature after total knee arthroplasty: A prospective study. Int Orthop. 2011;35:31–5. doi: 10.1007/s00264-010-0973-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Greidanus NV, Masri BA, Garbuz DS, Wilson SD, McAlinden MG, Xu M, et al. Use of erythrocyte sedimentation rate and c-reactive protein level to diagnose infection before revision total knee arthroplasty. A prospective evaluation. J Bone Joint Surg Am. 2007;89:1409–16. doi: 10.2106/JBJS.D.02602. [DOI] [PubMed] [Google Scholar]
- 4.Herro FA, Lozano RL, Muoz AS. Descriptive analysis of CRP after uncomplicated THA and TKA. Acta Orto Max. 2008;22:80–4. [Google Scholar]
- 5.Bilgen O, Atici T, Durak K, Karaeminoğullari, Bilgen MS. C-reactive protein values and erythrocyte sedimentation rates after total hip and total knee arthroplasty. J Int Med Res. 2001;29:7–12. doi: 10.1177/147323000102900102. [DOI] [PubMed] [Google Scholar]
- 6.Larsson S, Thelander U, Friberg S. C-reactive protein (CRP) levels after elective orthopedic surgery. Clin Orthop Relat Res. 1992;275:237–42. [PubMed] [Google Scholar]
- 7.White J, Kelly M, Dunsmuir R. C-reactive protein level after total hip and total knee replacement. J Bone Joint Surg Br. 1998;80:909–11. doi: 10.1302/0301-620x.80b5.8708. [DOI] [PubMed] [Google Scholar]
- 8.Park KK, Kim TK, Chang CB, Yoon SW, Park KU. Normative Temporal values of CRP and ESR in unilateral and staged bilateral TKA. Clin Orthop Relat Res. 2008;466:176–88. doi: 10.1007/s11999-007-0001-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hashmi FR, Barlas K, Mann CF, Howell FR. Staged bilateral hip or knee arthroplasties. J Orthop Surg (Hong Kong) 2007;15:159–62. doi: 10.1177/230949900701500206. [DOI] [PubMed] [Google Scholar]
- 10.Geep B. Detection of low grade prosthetic joint Infection using TC-99-antigranulocyte SPECT/CT. Eur J Nucl Med Mol Imaging. 2010;37:1751–9. doi: 10.1007/s00259-010-1431-3. [DOI] [PubMed] [Google Scholar]
- 11.Parvizi J, Ghanem E, Sharkey P, Aggarwal A, Burnett RS, Barrack RL. Diagnosis of infected total knee: Findings of a multicenter database. Clin Orthop Relat Res. 2008;466:2628–33. doi: 10.1007/s11999-008-0471-5. [DOI] [PMC free article] [PubMed] [Google Scholar]