

Abstract
Background:
The aim of this study is to compare the effects of laser therapy and shock wave therapy for symptoms treatment among patients with MPS in the upper trapezius muscle.
Materials and Methods:
In a clinical trial study, 46 patients were selected based on the clinical criteria and physiathrist diagnosis. Subjects were randomized into two groups as follows: Twenty individuals were assigned to exercise-medication-laser therapy group, and 26 to exercise-medication-shock wave therapy group. The pain was assessed based on visual analog scale (VAS), neck disability index (NDI), and SPADI in three stages: Before treatment, subsequently after treatment, and a month after treatment.
Results:
One man and 19 women, age group of 45.3 ± 7.7 years, were assigned into laser therapy group. Two men and 24 women, average age group of 42.3 ± 10.4 were assigned into shock wave therapy group. A significant difference was found among our study groups before treatment and after starting treatment for VAS, NDI, and SPDI indices, that is, two methods of treatments were effective (P < 0.001). However, among these two treatment methods, laser therapy provided higher effect on VAS and NDI as compared to the radial shock wave method (P < 0.05) in 2 weeks from starting the treatment (consequent to treatment).
Conclusion:
According to this study results, we can conclude that shock wave and laser therapy results on similar effect in long-term for relieve of pain and eliminating symptoms in patients with myofascial but laser provides a faster optimal results.
Keywords: Low level laser therapy, myofascial pain syndrome, neck disability index, shock wave, upper trapezius, visual analog scale
INTRODUCTION
Pain in the neck area considers a major medical-social issue and its occurrence alone or in conjunction with the upper parts pains was estimated to be present among 9–18% among the general population. Generally speaking, 1/3 of the population experience pain at least once during a lifetime. Myofascial pain syndrome (MPS) is a localize pain syndrome, which will recognized by tender spots and myofascial trigger points (MTP). The most prominent characteristic of MTrPs is presented of piercing tenderness in nodule, which are a part of taut band and fibrosis muscles.[1] With applying pressure to the point, pain, or paresthesia occurs in the searea or pain radiates into the neighboring areas and result in a series of outcomes such as local contraction of the muscle, limited range of motion (ROM), and muscle weakness. MPS is mostly seen in the time of evaluation and treatment of patients with chronic pain. Resulted pain caused by trigger point stimulation is topical or recurring, and increase with effected area tension, cold, or pressure. While the mechanism of trigger points is not fully understood, but it seems MPS forms by trauma, inflammation, and other causes.[2] Trigger points can be seen in any muscle or muscular group but they are usually seen in under higher stress muscles or in muscles which do not go under complete contraction and relaxation for long period of time. In upper body parts usually trapezius, lovatra scapola, and infraspinatus are mostly involved.[3] However, the upper trapezius is the most involved part. For treatment and eliminating of symptoms, many methods are used. The treatment includes stretching and deep massage, manipulation, ultrasound, electrotherapy, and needling (as acupuncture, dry, or numbing with injection). Laser therapy also uses as a treatment method for eliminating pain and increasing skin resistance. The analgesic effect of laser is by means of a mechanism or a combination of various mechanisms as follow: Increasing blood perfusion, collagen proliferation, peripheral nerve stimulation, anti-inflammatory, and direct analgesic effects. Shock wave therapy as a modern tool uses in MPS treatment[4] and Low level laser therapy (LLLT).[5] In physical therapy modalities, LLLT is one of the most recently employed treatments. LLLT has been applied in several rheumatoid and soft-tissue disorders with varying rates of success.[6,7,8] The efficacy of LLLT in MPS seems controversial.[9,10] The results of some placebo-controlled studies suggest that the low-power laser treatment may be useful for reducing the pain in cervical osteoarthritis,[11] medial and lateral epicondylitis,[12] and MPS.[5,13] On the other hand, a number of placebo-controlled, and randomized double blind studies have not been able to demonstrate any significant or convincing, clinically relevant effects over, placebo in the treatment of cervical MAS,[10,14] lateral epicondylitis,[15] rotator cuff tendinitis, and rheumatoid arthritis.[16] The effect of low level laser in treatment of MPS of neck is controversial. Some studies point to its effectiveness and some reject its benefit.[17,18] A study by Hakgüder et al. shows the effect of LLLT for decreasing symptoms of MPS. The study provided the evidences that LLLT recognized effective on eliminating the MPS symptoms.[5] However, the study by Dundar et al. on evaluation of laser therapy effect for trigger point treatment of neck did not find significant difference between the two study groups; group with low level laser recipients and placebo laser recipients. In fact, the laser therapy method was lagged to be effective.[17] Other treatment method is shock wave therapy, which done with electromagnetic stimulation and producing low level energy wave which may be effective on increasing blood flow in the treated area. Nowadays, various procedures are used for treatment that we can point to improving the muscles movement by means of decreasing passive muscle tone and increase muscle movement range.[9] Considering the conflicting results in performed studies on laser effect and lack of comparative research on LLLT and radial shock wave effect, our aim is to study and compare these two treatment method in patients with MPS and most involved parts, that is, upper trapezius.
MATERIALS AND METHODS
Noteworthy, the total number of participants were 52 which dropped to 46 due to the lack of interest for continue participation in latter stages. Forty six patients which were referred to physical medicine clinics and rehabilitation centers Isfahan from 2012 to 2013 were diagnosed with MPS of the upper trapezius. These patients were randomized into two groups; 20 assigned in exercise-medication-laser therapy and 26 assigned in exercise-medication-shock wave therapy group. The intensity of pain was simulated for these two groups. Participating criteria included the clinical diagnosis by MPS in upper trapezius based on active trigger points which recognized by reoccurrence of pain or increase pain by finger pressing and taut band touch. Other criteria included the tendency to participate in study and lack of specific characteristics to prohibit them to enter the study, visual analog scale (VAS) >5, duration of pain >1-month. Exclusion criteria included a history of fracture of the cervical spine or surgery of the neck, myelopathy or radiculopathy of neck, psychological illness or cognitive impairment, (taking corticosteroids oral) or intravenous or narcotics, pregnancy, and coagulopathy. As the result, the number of participants in each group turned out to be unequal. The patients in both groups underwent equal drug therapy and upper part of trapezius stretching. The exercises are given in 30 s interval for 3 times and the stretching repeated 3 times a day. All participants prescribed with similar medication and stretching exercises for 2 weeks. In the first group, 20 patients (26 point) underwent 10 sessions of LLLT in addition to stretching exercises and medication. The type of laser used: Indolaser device, type Ga-AL-As with 6 J/cm2, average power 100 mW, and for total of 3 min on each spot was used.
In the second group, 26 patients (32 point) had three session of radial shock wave therapy in addition to stretching exercises, and medication. Type of shock wave used: Standard electromagnetic device, DUOLITH SD1-shock waves with 1000 impulse and 3 J/m2 and 10 Hz frequency was used.
Evaluation VAS, neck disability index (NDI), and SPADI occurred in three stages, before treatment, consequently after treatment (in 2 weeks of starting treatment) and 4 weeks after completed the treatment. The results registered in relative checklists.
Measuring pain score based on visual analog scale
First of all, participants were requested to grade their pain based on 1–10 (3 and 4 for mild to medium, 5 for medium, 7 and 8 for intense, and 9 and 10 for very severe pain). The scores were recorded in a vertically graded diagram from 1 to 10.[19]
Neck disability index
It includes 10 part; pain intensity, personal care, lifting objects, reading, headache, concentration, work, driving, sleeping, and entertainments. There are six presumptions and patient must use one of these presumptions. The first presumption is given 0 and the last presumption had the score of 5. Ultimately, the percent of the obtained scores were found.[19]
The shoulder pain and disability index (SPADI) is a self-administered questionnaire that consists of two dimensions, one for pain and the other for functional activities. The pain dimension consists of five questions regarding the severity of an individual’s pain. Functional activities are assessed with eight questions designed to measure the degree of difficulty an individual has with various activities of daily living that require upper-extremity use.[19]
Data analysis was done by descriptive statistical methods (mean ± standard deviation), means difference test for independent groups, paired t-test, and variance analysis (one-way ANOVA) for comparing two groups and variance analysis with repeated measures ANOVA, and Pearson correlation coefficient with the use of SPSS version 20 software IBM SPSS CO. P <0.05 considered as significant statistically.
RESULTS
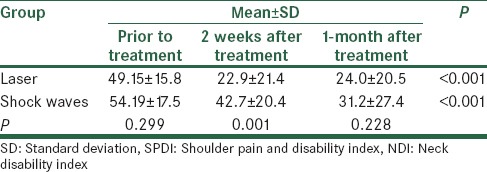
The study included 46 patients; laser therapy group included 1 man and 19 women average age of 45.3 ± 7.7 years, shock wave therapy group included 2 men and 24 women with average age 42.3 ± 10.4 years. There was no significant difference between the age range of participants in the both groups, and both groups considered analogous with regard to the age variable (P = 0.16). With regard to the gender variable, no significant difference was also found (P = 0.26). A significant difference was found among our study groups before treatment and after starting treatment for VAS, NDI, and SPDI indices, that is, both methods of treatments were effective (P = 0.0003) [Tables 1–3]. However, among these two treatment methods, laser therapy provided higher effect on VAS and NDI as compared to the other study methods (P = 0.008). In 2 weeks from starting the treatment (consequent to treatment). Nevertheless, evaluation after a month from treatment did not show a significant different in 2 treatment methods for 3 indices (P = 0.40). Moreover, both methods were equally effective on pain relieve and improving disability. According to the study results, we can concluded that shock wave therapy and laser therapy result on similar effect in long-term for relieve of pain and eliminating symptoms in patients with myofascial (P > 0.05), but laser provides a faster optimal results. The recent study showed there is no significant difference among treatment groups in some indicate such as SPDI and in fact, the effectiveness in eliminating the pain was identical for both groups (P > 0.05) [Tables 1–3].
Table 1.
Average VAS for two study groups in various times
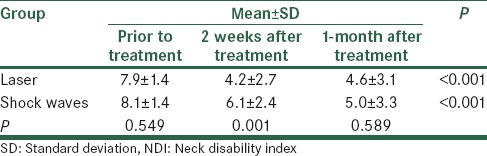
Table 3.
Average SPDI for two groups in various times
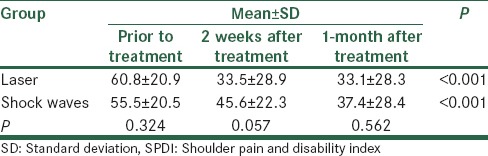
Table 2.
Average NDI for two groups in various times
DISCUSSION
In this study, we obtained positive results for effectiveness of 2 treatment methods; laser and shock wave therapy in elimination of pain based on VAS, NDI, and SPDI after applying treatment as compared to prior to treatments. In fact, for both groups, a significant improvement was observed. Similar to our study of Hakgüder et al. among two 30 participants groups; one was treated with low level laser and exercise and the second one with exercise, after 3 weeks, a significant elimination of pain was observed in the first group as compared to the second group with use of VAS measures. Therefore, low level laser considers effective in decreasing MPS.[5] A significant difference was observed for pain elimination consequent to treatment based on VAS, NDI, which all present a good evidence of effectiveness of these treatment methods in short-term. In addition, profound study showed between the two groups; laser and shock wave therapy, use of laser was more effective in short-term. Gur et al. studied the effect of LLLT in eliminating chronic MPS of neck among two groups of 30 individuals. The first group received low level laser and the second group had a placebo laser. The laser applied 2 weeks every day except for the last day of weeks. The evaluation was done in 2nd, 3rd, and 12 weeks. The first group showed a significant improvement in 2nd week of treatment (consequent to treatment) as compared to the control group for pain in time of rest, pain in time of movement, the number of trigger points, and VAS and NDI measures, but for the second group, the pain relieve was significant for 1st week only in rest time.[9] The results are in conformity with the results obtained from the recent studies. However, a printed study review by Chow et al. entitled effect of low laser (LLLT) on neck pain showed low level laser results on elimination of intense neck pain after treatment in a period of effectiveness of 22 weeks,[18] but no significant difference was observed after a month of treatment among our study groups. The shock wave therapy which works by means of electromagnetic induction mechanism and creating the waves with low energy level can be effective by increasing the blood circulation in under treatment location.[20,21] In the year 2012, in a study by Jeon, two groups of 15 individuals with MPS in upper trapezius were been studied. Fifteen patients underwent the transcutaneous electrical nerve stimulation (TENS) treatment conjoint with an injection in trigger point every week once. The second group underwent an extracorporeal shock wave lithotripsy (ESWL) once every 3 weeks. A significant difference was found for VAS in ESWL group as compared to TENS and injected group, but there was no significant difference in neck ROM.[22] In a prospective clinical trial by Dundar et al., he divided 64 patients with chronic neck pain into two groups in order to study the effect of LLLT. One group receive laser in trigger points and the second group receive placebo laser. Results were statistically significant for two groups before and after treatments in improvement signs, but no significant difference was found between these two groups.[17] Altan et al. investigated the effect of LLLT as compared to the placebo laser in patients with chronic myofascial pain (CMP) in the neck. The statistical analysis of their results showed a significant improvement after treatment as compared to prior to treatment and 12 weeks after treatment. However, the comparison of two groups showed no significant difference in Velter a flexion of neck consequently after treatment and 12 weeks after treatment. That is to say, there is no priority for laser therapy vs. placebo treatment in patients with CMPs in the neck.[10] The recent study showed there is no significant difference among treatment groups in some indicate such as SPDI, and in fact, the effectiveness in eliminating the pain was identical for both groups (P > 0.05). According to the study results, we can concluded that shock wave and laser therapy result on similar effect in long-term for relieve of pain and eliminating the symptoms in patients with myofascial (P > 0.05), but laser provides a faster optimal results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Hong CZ. In: Physical Medicine and Rehabilitation. 4th ed. Braddom RL, editor. Philadelphia: Elsevier Saunders; 2011. pp. 971–1002. [Google Scholar]
- 2.Travell JG, Simons DG. Myofascial Pain and Dysfunction. The Trigger Points Manual. 1st ed. Baltimore: Williams & Wilkins; 1998. [Google Scholar]
- 3.Childers MK, Feldman JB, Guo HM. In: Chronic Myofascial Pain (CMP). Essentials of Physical Medicine and Rehabilitation. 2nd ed. Frontera WR, Silver JK, Rizzo TD, editors. Philadelphia: Saunders & Elsevier; 2008. pp. 529–39. [Google Scholar]
- 4.Kuan TS. Current studies on myofascial pain syndrome. Curr Pain Headache Rep. 2009;13:365–9. doi: 10.1007/s11916-009-0059-0. [DOI] [PubMed] [Google Scholar]
- 5.Hakgüder A, Birtane M, Gürcan S, Kokino S, Turan FN. Efficacy of low level laser therapy in myofascial pain syndrome: An algometric and thermographic evaluation. Lasers Surg Med. 2003;33:339–43. doi: 10.1002/lsm.10241. [DOI] [PubMed] [Google Scholar]
- 6.Klein RG, Eek BC. Low-energy laser treatment and exercise for chronic low back pain: Double-blind controlled trial. Arch Phys Med Rehabil. 1990;71:34–7. [PubMed] [Google Scholar]
- 7.Vasseljen O, Jr, Høeg N, Kjeldstad B, Johnsson A, Larsen S. Low level laser versus placebo in the treatment of tennis elbow. Scand J Rehabil Med. 1992;24:37–42. [PubMed] [Google Scholar]
- 8.Heussler JK, Hinchey G, Margiotta E, Quinn R, Butler P, Martin J, et al. A double blind randomised trial of low power laser treatment in rheumatoid arthritis. Ann Rheum Dis. 1993;52:703–6. doi: 10.1136/ard.52.10.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gur A, Sarac AJ, Cevik R, Altindag O, Sarac S. Efficacy of 904 nm gallium arsenide low level laser therapy in the management of chronic myofascial pain in the neck: A double-blind and randomize-controlled trial. Lasers Surg Med. 2004;35:229–35. doi: 10.1002/lsm.20082. [DOI] [PubMed] [Google Scholar]
- 10.Altan L, Bingöl U, Aykaç M, Yurtkuran M. Investigation of the effect of GaAs laser therapy on cervical myofascial pain syndrome. Rheumatol Int. 2005;25:23–7. doi: 10.1007/s00296-003-0396-y. [DOI] [PubMed] [Google Scholar]
- 11.Ozdemir F, Birtane M, Kokino S. The clinical efficacy of low-power laser therapy on pain and function in cervical osteoarthritis. Clin Rheumatol. 2001;20:181–4. doi: 10.1007/s100670170061. [DOI] [PubMed] [Google Scholar]
- 12.Simunovic Z, Trobonjaca T, Trobonjaca Z. Treatment of medial and lateral epicondylitis – Tennis and golfer’s elbow – With low level laser therapy: A multicenter double blind, placebo-controlled clinical study on 324 patients. J Clin Laser Med Surg. 1998;16:145–51. doi: 10.1089/clm.1998.16.145. [DOI] [PubMed] [Google Scholar]
- 13.Ilbuldu E, Cakmak A, Disci R, Aydin R. Comparison of laser, dry needling, and placebo laser treatments in myofascial pain syndrome. Photomed Laser Surg. 2004;22:306–11. doi: 10.1089/pho.2004.22.306. [DOI] [PubMed] [Google Scholar]
- 14.Waylonis GW, Wilke S, O'Toole D, Waylonis DA, Waylonis DB. Chronic myofascial pain: Management by low-output helium-neon laser therapy. Arch Phys Med Rehabil. 1988;69:1017–20. [PubMed] [Google Scholar]
- 15.Vecchio P, Cave M, King V, Adebajo AO, Smith M, Hazleman BL. A double-blind study of the effectiveness of low level laser treatment of rotator cuff tendinitis. Br J Rheumatol. 1993;32:740–2. doi: 10.1093/rheumatology/32.8.740. [DOI] [PubMed] [Google Scholar]
- 16.Goats G, Flett E, Hunter JA, Stirling A. Low intensity laser and phototherapy for rheumatoid arthritis. Physiotherapy. 1996;82:311–20. [Google Scholar]
- 17.Dundar U, Evcik D, Samli F, Pusak H, Kavuncu V. The effect of gallium arsenide aluminum laser therapy in the management of cervical myofascial pain syndrome: A double blind, placebo-controlled study. Clin Rheumatol. 2007;26:930–4. doi: 10.1007/s10067-006-0438-4. [DOI] [PubMed] [Google Scholar]
- 18.Chow RT, Johnson MI, Lopes-Martins RA, Bjordal JM. Efficacy of low-level laser therapy in the management of neck pain: A systematic review and meta-analysis of randomised placebo or active-treatment controlled trials. Lancet. 2009;374:1897–908. doi: 10.1016/S0140-6736(09)61522-1. [DOI] [PubMed] [Google Scholar]
- 19.Damian M, Zalpour C. Trigger point treatment with radial shock waves in musicians with nonspecific shoulder-neck pain: Data from a special physio outpatient clinic for musicians. Med Probl Perform Art. 2011;26:211–7. [PubMed] [Google Scholar]
- 20.Wang CJ. Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res. 2012;7:11. doi: 10.1186/1749-799X-7-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Min H, Kim J, Jeong H. Extracorporeal shock wave therapy in myofascial pain syndrome of upper trapezius. Ann Rehabil Med. 2012;36:675–80. doi: 10.5535/arm.2012.36.5.675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jeon JH, Jung YJ, Lee JY, Choi JS, Mun JH, Park WY, et al. The effect of extracorporeal shock wave therapy on myofascial pain syndrome. Ann Rehabil Med. 2012;36:665–74. doi: 10.5535/arm.2012.36.5.665. [DOI] [PMC free article] [PubMed] [Google Scholar]