

Abstract
Aim:
The aim of the study is to evaluate the effect of ceramic type, thickness, and time of irradiation on degree of polymerization of dual-cure resin cement.
Materials and Methods:
Dual-cure resin cement (SoloCem) was used to prepare disk-shaped samples (0.5 mm thick × 5 mm diameter). Study group samples (n = 5) were light-cured for 40, 60, and 80 s through all ceramic leucite-reinforced (Cergo Kiss), lithium disilicate-reinforced (IPS e.max), and monolithic zirconia-reinforced (Ziecon) of three thicknesses (2, 3, and 4 mm). Negative control group samples were cured through metal disks and positive control samples were cured without the presence of ceramic. The degree of conversion (DC) was evaluated by Fourier transform infrared spectrometer. The recorded data were subjected to one-way analysis of variance, followed by post hoc analysis (Tukey HSD).
Results and Conclusion:
Greatest light transmission and DC were seen through Cergo Kiss, followed by IPS e.max Press and Ziecon, with insignificant difference between the latter two. The attenuation of light irradiance increased with increasing thickness of ceramic disks, with statistically significant values between 3 and 4 mm. Increasing time of irradiation to cure dual-cure resin cement did not always result in greater degree of polymerization.
Keywords: All-ceramic, degree of conversion, dual-cure resin cement, Fourier transform infrared spectrometer
INTRODUCTION
Retention of ceramic inlays, which is crucial for its success, depends on the cavity design and the effectiveness of the adhesive luting cement which fixes the restoration to the tooth structure.
Resin cements can be activated chemically or via visible light or by both chemical and light cure (dual-cure). Dual-cure resin cements were developed with the objective of combining the favorable characteristics of self- and light-activated cements.[1]
Polymerization of dual-cured resin cement may be affected if the curing light does not reach the cement; thus, dual-cured cement needs to rely on an autopolymerizing component.[2] Mechanical properties of dual-cured resin agents depend on the intensity of light irradiation and the light attenuation through different materials.[3] The degree of light attenuation depends on the characteristics of the overlying restoration such as optical behavior of the restorative material,[4,5,6] crystalline structure, grain size, defects, intrinsic porosity, thickness, layering technique,[7,8,9] and shade,[5,6] which interfere with light transmittance. Besides formulation[6] and opacity[10] of the indirect restorative material, other factors that interfere with the radiant exposure that reaches the cement layer are the distance between the curing light and cement layer,[11] the type of light source, their intensity, and the exposure time.[10,12]
The degree of polymerization of dual-cured resin cement is a measure of the percentage of carbon–carbon double bonds that have been converted to single bonds to form a polymeric resin. There are various methods to evaluate the degree of polymerization among which Fourier transform infrared (FTIR) spectroscopy is the best method as it offers a direct approach to evaluate the depth of cure.[5]
To the best of our knowledge, there has been no study which has evaluated the effect of three factors, i.e., ceramic type, thickness, and irradiation on degree of polymerization of recently introduced dual-cured resin cement, SoloCem. The purpose of this study is to evaluate the effect of ceramic type, thickness, and irradiation time on the degree of polymerization of recently introduced dual-cure resin cement.
MATERIALS AND METHODS
All ceramic disks of lithium disilicate ceramic (IPS e.max Press), leucite-reinforced ceramic (Cergo Kiss), and monolithic zirconia (Ziecon) were fabricated in B2 shade in 2, 3, and 4 mm thickness.
To simulate the condition of cementing an indirect restoration using dentin reflectance, a human incisor tooth was used. The root of the tooth was removed using a diamond disk. The incisor tooth was then embedded in acrylic resin with the buccal surface facing out.
There were 13 groups of 15 samples each, out of which 9 were experimental groups, 3 negative control groups, and 1 positive control group. The dual-cure resin cement samples of each group were cured through:
Groups I, II, and III (n = 15) – lithium disilicate ceramic disk (IPS e.max Press) of 2, 3, and 4 mm thickness, respectively
Groups IV, V, and VI (n = 15) – glass silicate ceramic disk (Cergo Kiss) of 2, 3, and 4 mm thickness, respectively
Groups VII, VIII, and IX (n = 15) – monolithic zirconia disk (Ziecon) of 2, 3, and 4 mm thickness, respectively,
Groups X, XI, and XII (n = 15) – metal disk of 2, 3, and 4 mm thickness, respectively, which served as negative control
Group XIII (n = 15) – Mylar strip which served as positive control group.
Each group was further subdivided into subgroups (n = 5) depending on the time of irradiation, i.e., 40, 60, and 80 s.
Before the fabrication of samples, the light transmission value of each thickness and type of ceramic was measured by placing the disk on the aperture of a handheld radiometer (Demetron 100, SDS/Kerr) and recording the average of resultant light readings through the disk in mW/cm2.
The samples were fabricated from self-adhesive, dual-cure resin cement – SoloCem (Coltene/Whaledent). For this, standard cylindrical ring stainless steel molds were fabricated with dimensions 5 mm inner diameter × 10 mm outer diameter × 0.5 mm depth. Separate positioning rings were fabricated to stabilize the ceramic disk and prevent displacement of the sample mold during preparation. Its inner diameter matched the outer diameter of the ceramic disk.
The resin cement was mixed and placed into the sample mold following the manufacturer recommendations. Mylar strip was placed on the bottom and top of the cement. Ceramic disk of that particular group was then placed on top of the resin cement sample, and the cement was light activated with curing unit held in direct contact with ceramic or metal disk for time duration specified for that particular group [Figure 1]. Curing light intensity was standardized at 600 mW/cm2 for each sample preparation using a light-cure unit with a radiometer (Spectrum 800, QTH light, Dentsply, Baar, Switzerland).
Figure 1.
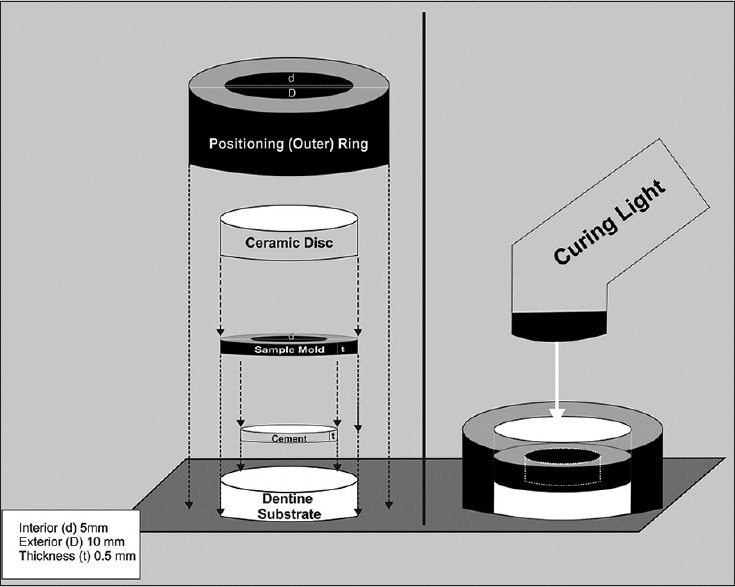
Experimental study set up
Immediately after light curing, the specimens were stored in light proof containers in a relatively high humidity at 37°C for 24 h.
The polymerized resin cement was removed from the molds to perform the infrared spectroscopic analysis using an FTIR.[13]
The mean value of degree of conversion % (DC) was calculated as a mean of five readings corresponding to five samples and was subjected to statistical analysis.
The statistical analysis was done using SPSS Version 15.0 (IBM Corp, Armonk, NY, USA). Data were analyzed using analysis of variance to determine the significance of the ceramic thickness, type, and time of irradiation on polymerization. Bonferroni post hoc test was used to rank the significant variables. A multivariate assessment was done using three-way ANOVA to determine which factor had the maximum influence.
RESULTS
Light transmission values of various ceramic and metal disks are displayed in Table 1. Table 2 shows the mean DC of different groups and thicknesses at different time intervals.
Table 1.
Transmission of light through ceramic and metal disks
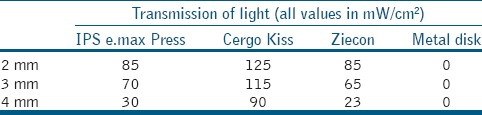
Table 2.
Mean degree of conversion values (%) and standard deviation for different groups and thickness at different time intervals
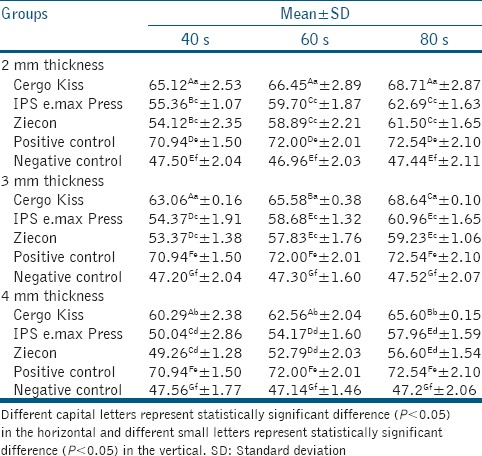
The maximum DC was seen in the positive control group and minimum in the negative control group.
Among the experimental groups, Cergo Kiss had maximum DC, followed by IPS e.max and Ziecon, at all thicknesses and time intervals. However, the difference in DC of IPS e.max Press and Ziecon was statistically insignificant.
For all the three materials, statistically, no significant difference between 2 and 3 mm thickness was observed at different time intervals. However, a statistically significant (P < 0.05) difference between 2 and 4 mm samples and 3 and 4 mm samples was observed at all the time intervals.
With Cergo Kiss, for 2 mm samples, none of the differences were significant statistically. For 3 mm specimens, all the three comparisons were significant statistically (P < 0.05); however for 4 mm samples, difference between 40 and 80 s samples and 60 and 80 s samples was significant (P < 0.05). With IPS e.max Press and Ziecon, all the three comparisons were significant statistically (P < 0.05) for 4 mm evaluation; however, in 2 and 3 mm specimens, the comparison between 60 and 80 s was not significant statistically.
DISCUSSION
The null hypothesis of this study was rejected as there was a difference in the DC of the dual-cured resin cement when irradiated through different ceramic disks of different thicknesses, for different time durations.
Among the three all-ceramic materials used, Cergo Kiss (leucite-reinforced) showed the maximum light transmission, hence the highest DC.
The superior DC seen by Cergo Kiss at all thicknesses is because the microstructure of the leucite-reinforced glass ceramic which is less dense and is characterized by single crystal formation of leucite crystals, without interlocking between crystal.[9] This ceramic contains between 35% and 45% volume leucite as crystalline phase[14] and 9% porosity.[15] Lithium disilicate ceramics, on the other hand, contain about 65% volume lithium disilicate as the main crystalline phase, with about 1% porosity.[15]
Moreover, in the lithium disilicate glass ceramic (IPS e.max), the main crystalline phase consists of elongated lithium disilicate crystals building a scaffold of many small interlocking needle-like crystals that are randomly oriented. A second crystalline phase consisting of lithium orthophosphate is of a much lower volume.[9] Thus, IPS e.max Press, with its higher degree of crystalline content and less porosity, has a greater scattering effect and appears relatively opaque to visible light. Although no study has been done till date using Cergo Kiss, studies of Ilie and Hickel[9] and Borges et al.[16] have compared other leucite-reinforced ceramics, lithium disilicate ceramic, and zirconia. They have also shown superior light transmission by leucite-reinforced ceramics, which is in accordance with the results of our study.
Zirconia ceramics have high refractive indices, low absorption coefficients, and high opacity in the UV/vis spectrum.[17] Studies of Borges et al.[16] and Kesrak and Leevailoj[18] have shown that DC of dual-cure resin cements polymerized under zirconia to be lower than lithium disilicate ceramics.
On the contrary, in our study, the difference in light transmission and DC of IPS e.max Press and Ziecon (monolithic zirconia-reinforced) was not significant. This was due to the high translucency zirconia which was used in our study. The translucency of this zirconia was due to yttria-stabilized zirconia which crystallizes into cubic structures.[19] In addition, the highly translucent zirconia was developed by decreasing the light-scattering sources, such as alumina particles (0.25 weight%).[20] Along with the composition, scattering of light is also generated by voids and porosities, crystal number, and size. Although the manufacturers have kept it a trademark secret, it may be speculated that the improvement in light transmittance might be attributable to the smaller grain size.[21]
On comparing the DC of the resin cement through different thicknesses of ceramics, it was seen that the results were not significant between 2 and 3 mm ceramic disks, whereas a significant decrease in the conversion was seen when the thickness was increased to 4 mm for all the ceramics. This was due to the attenuation in irradiance with increasing specimen thickness as the self-curing components are not able to compensate for the low light intensity that reaches the resinous material. Kilinc et al.[22] stated that the critical ceramic thickness that adversely affects resin cement microhardness is 3 mm.
Our results were corroborated by the findings of other studies which showed gradual reduction in KHNs with increasing ceramic thicknesses.[6,18,23,24]
With Cergo Kiss, the nonlinear relationship between curing and curing time may be explained by the typical autoacceleration/autodeceleration stages of a polymerization reaction,[25] in which the chain flexibility and molecular mobility decrease while the complete polymerization of the material is avoided[26] due to the limitation of diffusion in the reaction medium.[27]
With IPS e.max Press and Ziecon, the difference in the DC of the cement at 2 and 3 mm thickness at different times of irradiation was attributed to the fact that the velocity of the photoinitiation polymerization reaction is limited and an unrestricted increase in irradiation will not be able to accelerate this process[9] which corroborates with the findings of Ilie and Hickel.[9]
At 4 mm thickness, the DC increased significantly when time of irradiation was increased from 40 s to 60 s and then to 80 s. Light overexposure was able to compensate for the light attenuation caused by these ceramic disks.
Multivariate assessment revealed that ceramic type played the most significant role on the degree of polymerization followed by the time of irradiation and ceramic thickness.
CONCLUSION
Within the limitations of the study, it can be concluded that the DC is affected by type of ceramic, thickness above 3 mm, and time of irradiation, with ceramic type having the maximum influence. As intensity of light through the ceramic disks decreases, the degree of polymerization of dual-cure resin cement decreases. Increasing time of irradiation to cure dual-cure resin cement did not always result in greater degree of polymerization.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ozcan M, Zambonι S, Valandro F, Bottino M, Bagis B. Microhardness of dual-polymerized resin cement around a translucent fiber post in the intraradicular environment. J Conserv Dent. 2011;14:370–3. doi: 10.4103/0972-0707.87200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Reza F, Lim SP. Effects of curing mode of resin cements on the bond strength of a titanium post: An intraradicular study. J Conserv Dent. 2012;15:123–6. doi: 10.4103/0972-0707.94576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Meng X, Yoshida K, Atsuta M. Influence of ceramic thickness on mechanical properties and polymer structure of dual-cured resin luting agents. Dent Mater. 2008;24:594–9. doi: 10.1016/j.dental.2007.06.014. [DOI] [PubMed] [Google Scholar]
- 4.Cardash HS, Baharav H, Pilo R, Ben-Amar A. The effect of porcelain color on the hardness of luting composite resin cement. J Prosthet Dent. 1993;69:620–3. doi: 10.1016/0022-3913(93)90293-w. [DOI] [PubMed] [Google Scholar]
- 5.Rasetto FH, Driscoll CF, Prestipino V, Masri R, von Fraunhofer JA. Light transmission through all-ceramic dental materials: A pilot study. J Prosthet Dent. 2004;91:441–6. doi: 10.1016/S0022391304001106. [DOI] [PubMed] [Google Scholar]
- 6.Soares CJ, da Silva NR, Fonseca RB. Influence of the feldspathic ceramic thickness and shade on the microhardness of dual resin cement. Oper Dent. 2006;31:384–9. doi: 10.2341/05-51. [DOI] [PubMed] [Google Scholar]
- 7.Peixoto RT, Paulinelli VM, Sander HH, Lanza MD, Cury LA, Poletto LT. Light transmission through porcelain. Dent Mater. 2007;23:1363–8. doi: 10.1016/j.dental.2006.11.025. [DOI] [PubMed] [Google Scholar]
- 8.Lee IB, An W, Chang J, Um CM. Influence of ceramic thickness and curing mode on the polymerization shrinkage kinetics of dual-cured resin cements. Dent Mater. 2008;24:1141–7. doi: 10.1016/j.dental.2008.03.015. [DOI] [PubMed] [Google Scholar]
- 9.Ilie N, Hickel R. Correlation between ceramics translucency and polymerization efficiency through ceramics. Dent Mater. 2008;24:908–14. doi: 10.1016/j.dental.2007.11.006. [DOI] [PubMed] [Google Scholar]
- 10.Rasetto FH, Driscoll CF, von Fraunhofer JA. Effect of light source and time on the polymerization of resin cement through ceramic veneers. J Prosthodont. 2001;10:133–9. doi: 10.1111/j.1532-849x.2001.00133.x. [DOI] [PubMed] [Google Scholar]
- 11.Uctasli S, Hasanreisoglu U, Wilson HJ. The attenuation of radiation by porcelain and its effect on polymerization of resin cements. J Oral Rehabil. 1994;21:565–75. doi: 10.1111/j.1365-2842.1994.tb01171.x. [DOI] [PubMed] [Google Scholar]
- 12.Usumez A, Ozturk AN, Usumez S, Ozturk B. The efficiency of different light sources to polymerize resin cement beneath porcelain laminate veneers. J Oral Rehabil. 2004;31:160–5. doi: 10.1046/j.0305-182x.2003.01219.x. [DOI] [PubMed] [Google Scholar]
- 13.Archegas LR, de Menezes Caldas DB, Rached RN, Soares P, Souza EM. Effect of ceramic veneer opacity and exposure time on the polymerization efficiency of resin cements. Oper Dent. 2012;37:281–9. doi: 10.2341/11-134-L. [DOI] [PubMed] [Google Scholar]
- 14.Denry IL, Rosenstiel S. Phase transformations in feldspathic dental porcelains. In: Fischman G, Clare A, Hench L, editors. Bioceramics: Materials and Applications. Westerville, OH, USA: The American Ceramic Society; 1995. pp. 149–56. [Google Scholar]
- 15.Guazzato M, Albakry M, Ringer SP, Swain MV. Strength, fracture toughness and microstructure of a selection of all-ceramic materials. Part I. Pressable and alumina glass-infiltrated ceramics. Dent Mater. 2004;20:441–8. doi: 10.1016/j.dental.2003.05.003. [DOI] [PubMed] [Google Scholar]
- 16.Borges GA, Agarwal P, Miranzi BA, Platt JA, Valentino TA, dos Santos PH. Influence of different ceramics on resin cement Knoop hardness number. Oper Dent. 2008;33:622–8. doi: 10.2341/07-155. [DOI] [PubMed] [Google Scholar]
- 17.Vagkopoulou T, Koutayas SO, Koidis P, Strub JR. Zirconia in dentistry: Part 1. Discovering the nature of an upcoming bioceramic. Eur J Esthet Dent. 2009;4:130–51. [PubMed] [Google Scholar]
- 18.Kesrak P, Leevailoj C. Surface hardness of resin cement polymerized under different ceramic materials. Int J Dent. 2012;2012:317509. doi: 10.1155/2012/317509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yamashita I, Kudo I, Tsukuma K. Development of highly transparent zirconia ceramics. TOSOH Res Technol Rev. 2012;56:11–6. [Google Scholar]
- 20.Ritter RG. Use of high translucency zirconia in the aesthetic zone. Dent Today. 2013;32:116, 118–9. [PubMed] [Google Scholar]
- 21.Yang Y, Huang H, Gao L, Zhang F. Investigation of a new 3Y-stabilized zirconia with an improved optical property for applications as a dental ceramic. J Ceram Process Res. 2011;12:473–6. [Google Scholar]
- 22.Kilinc E, Antonson SA, Hardigan PC, Kesercioglu A. The effect of ceramic restoration shade and thickness on the polymerization of light- and dual-cure resin cements. Oper Dent. 2011;36:661–9. doi: 10.2341/10-206-L. [DOI] [PubMed] [Google Scholar]
- 23.el-Badrawy WA, el-Mowafy OM. Chemical versus dual curing of resin inlay cements. J Prosthet Dent. 1995;73:515–24. doi: 10.1016/s0022-3913(05)80109-x. [DOI] [PubMed] [Google Scholar]
- 24.Zhang X, Wang F. Hardness of resin cement cured under different thickness of lithium disilicate-based ceramic. Chin Med J (Engl) 2011;124:3762–7. [PubMed] [Google Scholar]
- 25.Atai M, Watts DC, Atai Z. Shrinkage strain-rates of dental resin-monomer and composite systems. Biomaterials. 2005;26:5015–20. doi: 10.1016/j.biomaterials.2005.01.022. [DOI] [PubMed] [Google Scholar]
- 26.Watts DC. Reaction kinetics and mechanics in photo-polymerised networks. Dent Mater. 2005;21:27–35. doi: 10.1016/j.dental.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 27.Lovell LG, Newman SM, Bowman CN. The effects of light intensity, temperature, and comonomer composition on the polymerization behavior of dimethacrylate dental resins. J Dent Res. 1999;78:1469–76. doi: 10.1177/00220345990780081301. [DOI] [PubMed] [Google Scholar]