

Abstract
Aims:
To compare the canal transportation, centering ability, and remaining dentin thickness of WaveOne and ProTaper systems using cone beam computed tomography.
Subjects and Methods:
Forty extracted human single-rooted premolars were used in the present study. Preinstrumentation scanning of all teeth was taken; canal curvatures were calculated, and the samples were randomly divided into two groups, with twenty samples in each group; one group was instrumented with WaveOne system and the other group with ProTaper rotary system. Postinstrumentation scans were performed, and the two scans were compared to determine canal transportation, centering ability, and remaining dentin thickness at 3 mm, 6 mm, and 9 mm from the root apex.
Statistical Analysis Used:
Student's unpaired t-test.
Results:
Using Student's unpaired t-test, results were as follows: for canal transportation, Group 1 showed significant difference at 3 mm and 6 mm and insignificant difference at 9 mm while Group 2 showed insignificant difference in all the three regions. For centering ability and remaining dentin thickness, Group 1 showed insignificant difference at 3 mm and 9 mm while significant difference at 6 mm was obtained. When comparison of remaining dentin thickness was done at three levels using two groups WaveOne and ProTaper, there was no significant difference between two groups.
Conclusions:
(1) WaveOne single reciprocation file system respected better canal anatomy better than ProTaper. (2) Individually, centering ability of WaveOne was better at 3 mm, 6 mm, and 9 mm levels. (3) However, ProTaper individually was better centered at 3 mm (apical third) and 9 mm (coronal 3rd) levels than 6 mm level (middle third).
Keywords: Centering ability, dentin thickness and cone beam computed tomography, ProTaper, transportation, WaveOne
INTRODUCTION
Successful endodontic therapy depends on effective debridement and shaping of the root canal system without deviating from the original anatomy. Ideally, during root canal preparation, the instruments should always confirm to and retain the original shape of the canal to maximize the cleaning effectiveness and minimize unnecessary weakening of tooth structure to achieve the optimal result. When curvatures are present, preparation becomes difficult and there is a tendency for all preparation techniques to divert the prepared canal away from the original axis.
Transportation of the root canal is a frequent mishap during the instrumentation of curved root canals. Transportation in the apical third of the root canal promotes the harboring of debris and residual microorganisms as a result of insufficient cleaning of the root canals and destruction of the integrity of the root. The etiology associated with an increased risk of canal transportation includes insufficiently designed access cavities, use of inflexible instruments, instrumentation technique, tip design, insufficient irrigation during mechanical enlargement, degree and radius of a canal curvature, unseen canal curvatures in two-dimensional (2D) radiography, and skill of operator.[1]
ProTaper features a convex triangular cross-section. They have a noncutting modified guiding tip along with a variable taper.[2] Recently, a new reciprocating WaveOne single-file system has been introduced by Dentsply. The system is designed to be used with a reciprocating motion motor. These files are made of a special nickel-titanium (NiTi) alloy called M-Wire that is created by an innovative thermal treatment process.[3,4]
In the past, methods for assessment of canal transportation, remaining dentin thickness, and centering ability included radiographic method, serial sectioning technique, photographic assessment, scanning electron microscope, and computer manipulation technique. These methods were invasive in nature and accurate repositioning of pre- and post-instrumented specimens was difficult, whereas radiographic method provides 2D images of 3D objects.[5,6]
Recently, a nondestructive technology has been advocated for pre- and post-instrumentation evaluations of canal. Cone beam computed tomography (CBCT) utilizes a cone-shaped X-ray beam and an area detector that captures a cylindrical volume of data in one acquisition. Advantages of CBCT are that it can render cross-sectional and 3D images that are highly accurate, high resolution, fully quantifiable and provides repeatable results.[7,8,9]
Considering the above-mentioned factors, this study was conducted to evaluate and compare the canal transportation, centering ability, and remaining dentin thickness after instrumentation with ProTaper and WaveOne rotary systems using CBCT.
SUBJECTS AND METHODS
Forty extracted human premolar teeth were included and stored in normal saline. All the samples were standardized to 18 mm length by decoronation using a steel disc.[10] Access cavity was made using round carbide bur and working length was determined.
Angle of curvature was assessed according to the criteria described by Schneider.[11] Teeth were radiographed using radiovisiography in buccolingual direction. A line was drawn parallel to long axis of the canal. The second line was drawn from the apical foramen to intersect with the first at the point where the canal began to leave the long axis of the tooth. Thus, the acute angle formed was measured and the angle of curvature was determined. Teeth with a degree of curvature ranging between 10° and 24° were included in the study.[12]
The specimens were embedded in self-cure acrylic resin, and then all teeth were scanned by CBCT before instrumentation. The images were stored and randomly divided into two groups of twenty each.
Group 1: Canals were prepared using WaveOne files.
Group 2: Canals were prepared using ProTaper rotary files.
The specimens were scanned by CBCT after instrumentation. The centering ability, canal transportation, and Remaining Dentine Thickness (RDT) were evaluated at 3 mm, 6 mm, and 9 mm from the root apex. The images were stored for further comparison between pre- and post-instrumentation data using CBCT (Kodak 9000 DICOM Software CS 9000 3D). Figure 1 showing superimposition of pre and post instrumentation images by using wavone at 3mm, 6mm & 9mm, while Figure 2 showing superimposition of pre and post instrumentation images by using protaper at 3mm, 6mm & 9mm.
Figure 1.
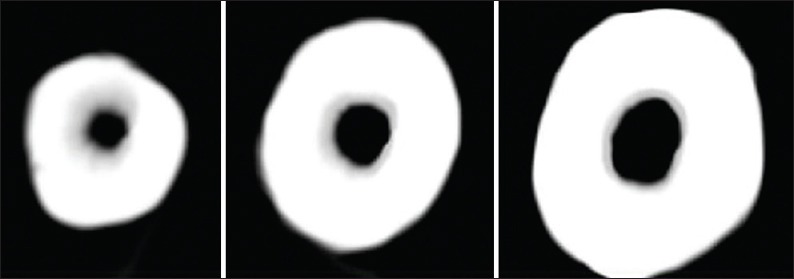
Group 1 (Waveone) superimposition of images at 3mm, 6mm & 9mm
Figure 2.
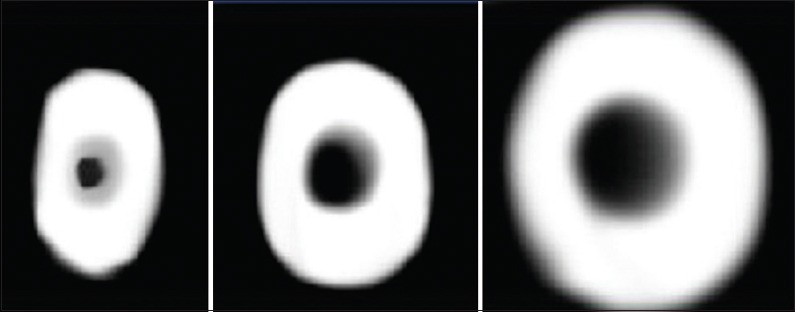
Group 2 (Protaper) superimposition of images at 3mm, 6mm & 9mm
The formula introduced by Gambill et al.[13] was used to measure the degree of canal transportation.
([a1 − a2] – [b1 − b2]).
where a1 and a2 are the shortest distance from the mesial edge of the root to the mesial edge of the uninstrumented and instrumented canal, respectively; b1 and b2 are the distance from distal edge of the root to the distal edge of the uninstrumented canal and instrumented canal, respectively. The result of “0” indicates no canal transportation and other than “0” means that transportation has occurred.
The following formula was used for the calculation of centering ability.
(a1 − a2)/(b1 − b2) or (b1 − b2)/(a1 − a2).
If the numbers are not equal, the lower figure was considered as the numerator and a result of “1” indicates perfect centering. The RDT was determined by subtracting the uninstrumented canal from the instrumented canal.
RESULTS
The data obtained were statistically analyzed using Student's unpaired t-test for intergroup comparison. Evaluation of canal transportation was done at three levels between two groups [Graphs 1–3]. A statistically significant difference was observed at 3 mm and 6 mm in Group 1. No statistically significant difference was found at 9 mm in Group 1. No statistically significant difference was obtained at all the three levels in Group 2.
Graph 1.
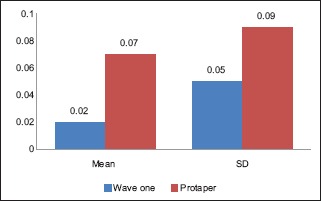
Bar chart showing the comparison of canal transportation at 3mm for both groups
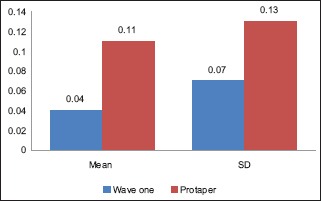
Graph 3.
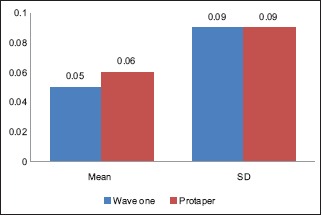
Bar chart showing the comparison of canal transportation at 9mm for both groups
Graph 2.
Bar chart showing the comparison of canal transportation at 6mm for both groups
Evaluation of centering ability was done between two groups. A statistically significant difference was observed at 6 mm in Group 1. No statistically significant difference was found at 3 mm and 9 mm in Group 1. Group 2 had no statistically significant difference at all the levels.
There was no statistically significant difference between the two groups with respect to remaining root dentin at 3 mm, 6 mm, and 9 mm.
DISCUSSION
Cleaning and shaping of the root canal comprise the most important phase of endodontic treatment. The aim of root canal preparation is to form a continuous tapered canal with the narrowest diameter at the apical foramen and the widest at the orifice to allow effective irrigation and filling without deviating from the original trajectory.[14]
An ideal instrumentation should have equal dentin removal from the canal walls so that it could avoid excessive thinning of root structure. However, the presence of curvatures may pose difficulty in root canal instrumentation. Ledge formation, blockage, perforation, and apical transportation are undesirable mishaps that can occur during preparation of curved root canals.
Cleaning and shaping of the root canal are carried by various instruments. Carbon steel which was used previously for root canal instrumentation has the drawback of susceptibility to fracture, tarnish, and corrosion. To overcome these failures, stainless steel has been introduced in the field of endodontics and it has long clinical success rate but has disadvantage of less flexibility. Various studies have shown that the incidence of transportation and straightening of the root canal are common with the use of stainless steel.[12]
The advent of NiTi rotary instruments has revolutionized root canal preparation. NiTi rotary files are manufactured from the NiTi alloy, which was developed by Buehler et al.[15] in 1963 at the Naval Ordinance Lab. NiTi files possess an elastic memory that enables the file to return to its original shape without deformation and have better ability to remain centered within the canal during instrumentation as compared to stainless steel files thus minimizing the straightening of the canal.
In the present study, canals prepared with ProTaper showed statistically significant difference (P < 0.05) for root canal transportation at apical third and middle levels which may be attributed to the progressive taper along the cutting surface, indicating a tendency to straighten curved canals and reduction in instrument flexibility. However, anon statistical significant (P < 0.05) difference was observed at coronal level. Apical transportation of more than 300 µm can have a negative impact on the seal of the obturation.[16] The results are obtained in conformity to Javaheri and Javaheri,[17] who found ProTaper to produce more apical transportation than any other instrument. The results are also in accordance to Bonaccorso et al.[18]
In the present study, canals prepared with WaveOne showed no statistically significant difference (P > 0.05) for canal transportation at all levels. Reasons for showing minimum canal transportation are the reciprocating movement which minimizes torsional and flexural stresses and reduces the taper lock. The results are in correlation to Yoo and Cho,[19] who also found WaveOne to produce lesser canal transportation than ProTaper.
When comparing canal transportation at apical and middle third among both the groups, a statistical significant (P < 0.05) difference was observed. However, anon statistical significant (P < 0.05) difference was observed between both the groups at coronal level.
In the analysis of centering ability, low value indicated that the preparation was centered in the canal. WaveOne showed better canal centered in all the three levels while ProTaper showed least-centered preparation at 6 mm (P < 0.05). These differences could be attributed to different instrumentation techniques. The least-centered preparation with ProTaper could be due to its reduced flexibility, increased tip stiffness and progressive taper of the instrument. Deviation from the original canal curvature can lead to excessive, inappropriate dentin removal and straightening of the canal and creation of a ledge in the dentinal wall. The results are in accordance to Goldberg et al.[4] Our results are also in confirmation to Yang et al.,[20] who found constant taper produced good centering ability compared to instruments with progressive taper. No statistically significant difference was found at 3 mm and 9 mm levels between the groups with regard to centering ability. However, a statistically significant difference was observed at 6 mm.
No statistically significant difference (P > 0.05) was seen for remaining root dentine at apical level between both the groups, which may be attributed to the noncutting modified safety tip. However, root dentine was significantly thinner at the middle third and coronal levels for ProTaper group. Progressively tapered design along with triangular convex cross-sectional design may have led to aggressive cutting. If root canals were excessively enlarged, weakening of the root structure and strip perforation results. Ozgur Uyanik et al.[21] have concluded that ProTaper removed the greatest amount of dentin. Comparing for remaining dentin thickness at all three levels in both the groups showed no statistically significant difference (P > 0.05).
Instrument selection and technique play important role in retaining original shape of the canal to maximize the cleaning effectiveness and minimize unnecessary weakening of tooth structure to achieve the optimal result.
CONCLUSIONS
Within the limitations of the present study, WaveOne single reciprocation file respected original canal anatomy better than ProTaper.
Better-centered canals was prepared with WaveOne at all three levels.
Canals prepared with ProTaper were better centered at the apical third and coronal third levels.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ingle JI, Himel VT, Hawrish CE, Glickman GN. Endodontic cavity preparation. In: Ingle JI, Bakland LK, editors. Endodontic. Ontario, Canada: BC Decker; 2002. p. 502. [Google Scholar]
- 2.Paqué F, Musch U, Hülsmann M. Comparison of root canal preparation using RaCe and ProTaper rotary Ni-Ti instruments. Int Endod J. 2005;38:8–16. doi: 10.1111/j.1365-2591.2004.00889.x. [DOI] [PubMed] [Google Scholar]
- 3.Berutti E, Paolino DS, Chiandussi G, Alovisi M, Cantatore G, Castellucci A, et al. Root canal anatomy preservation of WaveOne reciprocating files with or without glide path. J Endod. 2012;38:101–4. doi: 10.1016/j.joen.2011.09.030. [DOI] [PubMed] [Google Scholar]
- 4.Goldberg M, Dahan S, Machtou P. Centering ability and influence of experience when using WaveOne® single-file technique in simulated canals. Int J Dent. 2012;2012:206321. doi: 10.1155/2012/206321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dowker SE, Davis GR, Elliott JC. X-ray microtomography: Nondestructive three-dimensional imaging forin vitro endodontic studies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:510–6. doi: 10.1016/s1079-2104(97)90155-4. [DOI] [PubMed] [Google Scholar]
- 6.Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34:476–84. doi: 10.1046/j.1365-2591.2001.00422.x. [DOI] [PubMed] [Google Scholar]
- 7.Garip Y, Günday M. The use of computed tomography when comparing nickel-titanium and stainless steel files during preparation of simulated curved canals. Int Endod J. 2001;34:452–7. doi: 10.1046/j.1365-2591.2001.00416.x. [DOI] [PubMed] [Google Scholar]
- 8.Arora A, Taneja S, Kumar M. Comparative evaluation of shaping ability of different rotary NiTi instruments in curved canals using CBCT. J Conserv Dent. 2014;17:35–9. doi: 10.4103/0972-0707.124127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maitin N, Arunagiri D, Brave D, Maitin SN, Kaushik S, Roy S. An ex vivo comparative analysis on shaping ability of four NiTi rotary endodontic instruments using spiral computed tomography. J Conserv Dent. 2013;16:219–23. doi: 10.4103/0972-0707.111318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sanchez JA, Duran-Sindreu F, Matos MA, Carabaño TG, Bellido MM, Castro SM, et al. Apical transportation created using three different patency instruments. Int Endod J. 2010;43:560–4. doi: 10.1111/j.1365-2591.2010.01710.x. [DOI] [PubMed] [Google Scholar]
- 11.Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32:271–5. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- 12.Fayyad DM, Sabet NE, El-Said Mahmoud Abd EH. Computed tomographic evaluation of the apical shaping ability of hero shaper & Revo-S. Quintessence Int. 2012;6:119–24. [Google Scholar]
- 13.Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369–75. doi: 10.1016/S0099-2399(96)80221-4. [DOI] [PubMed] [Google Scholar]
- 14.Grossman LI. Endodontic practice. 10th ed. Lea and Febigger; 1982. p. 297. [Google Scholar]
- 15.Buehler WJ, Wiley RC, Gilfrich JV. Effect of low- temperature phase changes on mechanical properties of alloys near composition. J Applied Phys. 1963;34:1475–7. [Google Scholar]
- 16.Gergi R, Rjeily A, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, pathfile, protaper system, and stainless steel hand k-files by using computed tomography. J Endod. 2010;36:904–7. doi: 10.1016/j.joen.2009.12.038. [DOI] [PubMed] [Google Scholar]
- 17.Javaheri HH, Javaheri GH. A comparison of three Ni-Ti rotary instruments in apical transportation. J Endod. 2007;33:284–6. doi: 10.1016/j.joen.2006.05.004. [DOI] [PubMed] [Google Scholar]
- 18.Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod. 2009;35:883–6. doi: 10.1016/j.joen.2009.03.007. [DOI] [PubMed] [Google Scholar]
- 19.Yoo YS, Cho YB. A comparison of the shaping ability of reciprocating NiTi instruments in simulated curved canals. Restor Dent Endod. 2012;37:220–7. doi: 10.5395/rde.2012.37.4.220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yang GB, Zhou XD, Zheng YL, Zhang H, Shu Y, Wu HK. Shaping ability of progressive versus constant taper instruments in curved root canals of extracted teeth. Int Endod J. 2007;40:707–14. doi: 10.1111/j.1365-2591.2007.01296.x. [DOI] [PubMed] [Google Scholar]
- 21.Ozgur Uyanik M, Cehreli ZC, Ozgen Mocan B, Tasman Dagli F. Comparative evaluation of three nickel-titanium instrumentation systems in human teeth using computed tomography. J Endod. 2006;32:668–71. doi: 10.1016/j.joen.2005.12.015. [DOI] [PubMed] [Google Scholar]