

Abstract
Introduction
Lithium overdose can be associated with cardiac toxicity, especially in those with underlying heart disease. Toxic levels of serum lithium are associated with cardiotoxic effects ranging from simple ECG disorders to dysrhythmias, cardiomyopathy and even acute myocardial infarction (AMI). This report describes a patient with AMI accompanied by high blood levels of lithium.
Case Presentation
A 62-year-old woman was admitted to the emergency department due to weakness and acute chest pain. Her ECG revealed ST elevation in leads DI, aVL and V5-6, with a ventricular rate of 80 bpm. Blood chemistry and complete blood count were within normal limits. The patient’s blood lithium level was measured as 2.3 mmol/L (N: 0.5 - 0.8 mmol/L), and her troponin I level was 0.892 ng/mL (N: 0 - 0.01 ng/mL). Coronary angiography produced normal findings, concurrent with the resolution of electrocardiographic abnormalities following elimination of lithium. The clinical course in the intensive care unit was uneventful and the patient was discharged on the seventh day.
Conclusions
Lithium intoxication should be considered in the differential diagnosis, especially in elderly patients on lithium therapy who are admitted to the emergency department with chest pain.
Keywords: Lithium, Overdose, Acute Myocardial Infarction, Cardiotoxicity
1. Introduction
Lithium is an alkaline compound which was introduced in early 1900s for psychiatric disorders and is currently used in the treatment of bipolar affective disorder and depression. However, acute overdoses can cause life-threatening conditions. Intoxications are relatively common due to the drug’s narrow therapeutic index. Its toxicity is characterized by neurological, gastrointestinal, renal, endocrine and cardiac problems (1). Patients with lithium intoxication (LI) are classified as acute, acute-on-chronic and chronic poisoning. Early symptoms of acute LI mostly involve gastrointestinal problems, such as nausea and vomiting, but chronic symptoms are generally neurological and include ataxia, tremor, speech impairment and altered level of consciousness. A review of the literature revealed several case reports in which both therapeutic and toxic levels of serum lithium were associated with cardiotoxic effects ranging from simple ECG disorders to cardiomyopathy, arrhythmias and even acute myocardial infarction (AMI) (2). This report presents a patient admitted to the hospital with acute chest pain and ST segment elevation associated with lithium therapy.
2. Case Presentation
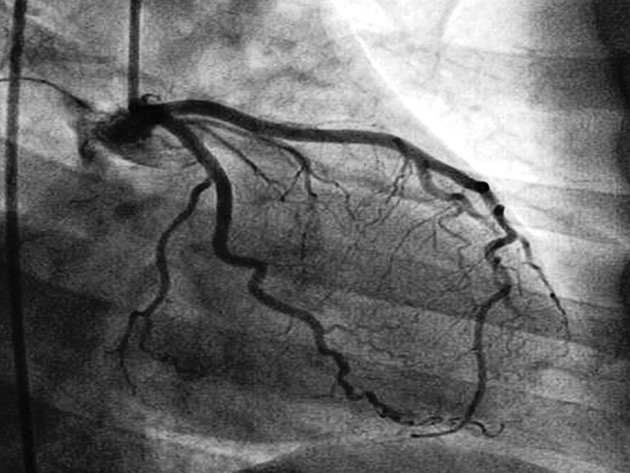
A 62-year-old woman was admitted to the emergency department suffering from weakness and acute chest pain during the preceding two hours. There were no records in the patient’s history of any chronic diseases, including renal failure or hypo/hyperthyroidism. In fact, she had no remarkable medical history, except for being put on lithium 400 mg/day and duloxetine 20 mg/day, a week earlier, due to bipolar disorder. Physical examination disclosed tremor in both hands and bilateral nystagmus. The patient’s arterial blood pressure was 90/60 mmHg, with a heart rate of 78 bpm, a respiratory rate of 22 bpm, and a transcutaneous SaO2 of 97%. Surface electrocardiography revealed ST elevation in leads DI, aVL and V5-6, with a ventricular rate of 80 bpm (Figure 1). Blood chemistry, including renal function tests and complete blood count were within normal limits. The patient’s blood lithium level was measured as 2.3 mmol/L (therapeutic range 0.5 to 0.8 mmol/L), and her troponin I level was 0.892 ng/mL (N: 0–0.01 ng/mL). Echocardiographic findings, including myocardial wall motions, pulmonary arterial pressure and ejection fractions were normal. The patient was admitted to the coronary intensive care unit. A subsequent coronary angiography performed within one hour of admission provided normal results (Figure 2). This was concurrent with a resolution of electrocardiographic abnormalities accompanied by elimination of lithium, which suggested that the observed ECG changes were linked to LI. The patient’s lithium level, measured on the seventh day, was found to be within normal limits (0.6 mmol/L). The clinical course in the intensive care unit was uneventful, with the patient being provided medical treatment and then discharged.
Figure 1. Surface ECG exhibits 1-mm ST Elevation in Leads DI, aVL and 3-mm Elevation in V4-6.
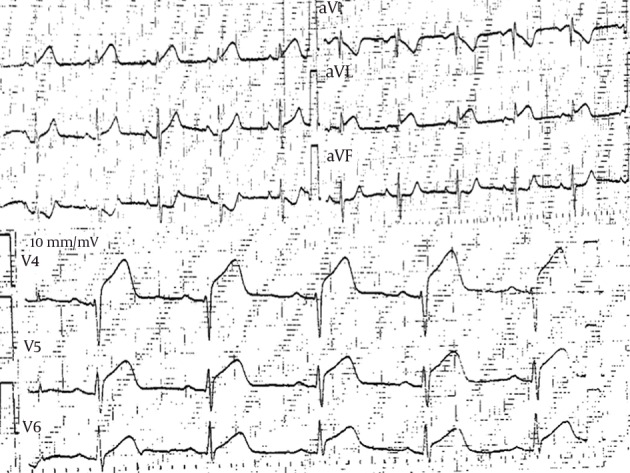
Figure 2. Coronary Angiography Revealed Normal Coronary Arteries.
3. Discussion
Acute chest pain is among the most common complaints encountered in emergency settings. In such cases, thorough and systematic evaluation are of vital importance to ensure expedient life-saving interventions. Diagnosis is based on the combination of a patient’s entire medical history, physical examination and laboratory investigations. After ruling out cardiac and life-threatening conditions, the medical history should be carefully evaluated and use of medications should not be overlooked.
This report describes a patient with acute chest pain whose ECG suggested AMI while being treated with lithium carbonate, resulting in a threefold serum level increase above normal range. Lithium-associated cardiotoxic effects can be seen even in therapeutic doses (3). Cardiac effects due to LI include prolonged QT interval, atrioventricular block, sinus arrest and ventricular dysrhythmias (4). Lithium causes toxicity through several mechanisms, including depletion of intracellular potassium and displacement of intracellular calcium. These effects have been reported to cause a decreasing depolarization rate and ECG changes resembling hypokalemia, due to the interchangeability of lithium with intracellular potassium (5). Through these mechanisms, lithium triggers certain ECG changes, such as QT prolongation, T-wave abnormalities and ST changes that masquerade as AMI (6). Even though there are numerous reports of such ECG changes in the literature, cases with ST elevation are rare. Kayrak and colleagues found ST segment elevation in inferior derivations as a result of lithium intoxication. As in our case, the myocardial wall motions and coronary angiography were found to be normal in echocardiography. The patients’ ECG readings returned to normal after hemodialysis (7). The ST elevation was attributed to the cardiotoxic effect of lithium. We did not perform hemodialysis in our case. Since the patient had a normal coronary angiography and lacked myocardial wall motion irregularities, takotsubo cardiomyopathy was ruled out.
Cases of LI are classified in terms of severity as acute, acute-on-chronic and chronic poisoning. Linakis et al. pointed out that these kind of ECG disorders are encountered in chronic LI (8), which contrasts with the present case in that lithium therapy had only lasted for one week. LI is reported more commonly in women than men, which is also the case in this paper. In addition, lithium is poorly tolerated by women and the elderly (9). Risk factors predisposing individuals to toxicity include diminished renal excretion of lithium due to advanced age-related renal impairment and lithium retention, secondary to nonsteroidal anti-inflammatory drugs, thiazide diuretics and the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) (10). There was no underlying cause that would raise blood lithium levels in our patient.
The recommended therapies in acute LI include hemodialysis and whole bowel irrigation (10, 11). The primary route of lithium elimination is renal (via glomerular filtration). Between 70% and 80% is reabsorbed in the proximal tubule. Hydration treatment in LI can decrease lithium reabsorption from the proximal tubule and increases its excretion. During initial therapy, replacement of fluids up to twice as much as the body’s normal requirement are to be given as normal saline (6). Accordingly, the patient was first administered fluid intravenously in the emergency department. This treatment was followed by gradually lowered lithium levels, which returned to normal in a few days. Resolution of electrocardiographic abnormalities in accordance with elimination of lithium suggests that ECG changes are linked to LI. These findings can be misinterpreted as cardiac ischemia, and thus physicians staffed in primary care should be cautious on this issue.
3.1. Conclusion
LI should be considered in the differential diagnosis, especially in elderly patients on lithium therapy who present to the emergency department with chest pain.
References
- 1.Hopkins HS, Gelenberg AJ. Serum lithium levels and the outcome of maintenance therapy of bipolar disorder. Bipolar Disord. 2000;2(3 Pt 1):174–9. doi: 10.1034/j.1399-5618.2000.020304.x. [DOI] [PubMed] [Google Scholar]
- 2.Puhr J, Hack J, Early J, Price W, Meggs W. Lithium overdose with electrocardiogram changes suggesting ischemia. J Med Toxicol. 2008;4(3):170–2. doi: 10.1007/BF03161196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Farag S, Watson RD, Honeybourne D. Symptomatic junctional bradycardia due to lithium intoxication in patient with previously normal electrocardiogram. Lancet. 1994;343(8909):1371. doi: 10.1016/s0140-6736(94)92512-7. [DOI] [PubMed] [Google Scholar]
- 4.Serinken M, Karcioglu O, Korkmaz A. Rarely seen cardiotoxicity of lithium overdose: complete heart block. Int J Cardiol. 2009;132(2):276–8. doi: 10.1016/j.ijcard.2007.08.058. [DOI] [PubMed] [Google Scholar]
- 5.Canan F, Kaya A, Bulur S, Albayrak ES, Ordu S, Ataoglu A. Lithium intoxication related multiple temporary ecg changes: A case report. Cases J. 2008;1(1):156. doi: 10.1186/1757-1626-1-156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Singer I, Rotenberg D. Mechanisms of lithium action. N Engl J Med. 1973;289(5):254–60. doi: 10.1056/NEJM197308022890508. [DOI] [PubMed] [Google Scholar]
- 7.Kayrak M, Ari H, Duman C, Gul EE, Ak A, Atalay H. Lithium intoxication causing ST segment elevation and wandering atrial rhythms in an elderly patient. Cardiol J. 2010;17(4):404–7. [PubMed] [Google Scholar]
- 8.Linakis J, Woolf A. Clinical features of acute versus chronic lithium overdose. Vet Human Toxicol. 1989;31(370) [Google Scholar]
- 9.Vestergaard P, Amdisen A. Lithium treatment and kidney function. A follow-up study of 237 patients in long-term treatment. Acta Psychiatr Scand. 1981;63(4):333–45. doi: 10.1111/j.1600-0447.1981.tb00682.x. [DOI] [PubMed] [Google Scholar]
- 10.Smith SW, Ling LJ, Halstenson CE. Whole-bowel irrigation as a treatment for acute lithium overdose. Ann Emerg Med. 1991;20(5):536–9. doi: 10.1016/s0196-0644(05)81610-5. [DOI] [PubMed] [Google Scholar]
- 11.Waring WS. Delayed cardiotoxicity in chronic lithium poisoning: discrepancy between serum lithium concentrations and clinical status. Basic Clin Pharmacol Toxicol. 2007;100(5):353–5. doi: 10.1111/j.1742-7843.2007.00054.x. [DOI] [PubMed] [Google Scholar]