

Abstract
Background
We aimed to compare indicators of Parkinson disease (PD) progression between patients first prescribed either selegiline or rasagiline as their antiparkinsonian drugs (APDs) on the basis of real-life data.
Methods
Pharmacy data on members of a large Israeli health maintenance organization, treated as patients with PD during 2001–2012 and prescribed selegiline or rasagiline as their first APD, were analyzed. The first APD was selegiline for 349 patients (2001–2006) and rasagiline for 485 patients (2007–2012). Time from monoamine oxidase type B inhibitor prescription until initiating treatment with dopamine agonists (DAs) or levodopa was compared between the groups using Cox regression adjusted to sex and age at initiation of APD.
Results
The selegiline group was significantly older at first monoamine oxidase type B inhibitor purchase. In a similar follow-up time (3.0 [1.7] year for selegiline group, 3.1 y [1.4] for rasagiline group), the time to initiation of levodopa treatment did not differ between the 2 groups (adjusted hazard ratio [HR], 1.06; 95% confidence interval [CI], 0.86–1.31). The time to initiation of DA treatment was longer in the selegiline group (adjusted HR, 1.93; 95% CI, 1.49–2.53). For those who were treated with DA before levodopa (n = 276), the time to initiation of levodopa treatment was longer in the rasagiline group (adjusted HR, 0.77; 95% CI, 0.56–1.07).
Conclusions
The similarity in time to levodopa in both groups suggests no differences between selegiline and rasagiline in their effect on the natural history of PD. A possible interaction effect between rasagiline and DA might exist. A better symptomatic profile of selegiline more than that of rasagiline in the earlier stages of PD may explain the difference between the 2 groups in time to DA initiation.
Key Words: Parkinson disease, selegiline, rasagiline, observational study, disease progression
Medical treatment of Parkinson disease (PD) is symptomatic.1,2 Levodopa3 and, to a lesser extent, dopamine agonists (DAs)2 are currently the most effective symptomatic treatment. However, levodopa use is commonly delayed, especially in younger patients, because of the associated development of motor complications (eg, motor response fluctuations and dyskinesias). Several guidelines suggest initiating antiparkinsonian medical treatment with monoamine oxidase isoenzyme type B inhibitors (MAO-BIs) and delay levodopa when justified.1,4 Monoamine oxidase isoenzyme type B inhibitors are considered in some but not all reports as being a potential disease-modifying therapy.5 Selegiline and rasagiline have been the only Food and Drug Administration (FDA)–approved MAO-BIs for the past 15 years. Both are relatively selective and irreversible, with some significant differences, mainly in their metabolites: amphetamine derivatives from selegiline and aminoindane from rasagiline.6 Rasagiline has been marketed strongly on the basis of this difference.5 Selegiline was approved for use by the FDA in 1996 and in Israel in 1998. Rasagiline was approved for use by the FDA in 2006 and in Israel as part of the Israeli “National Health Basket” in 2007. Both are provided to patients with PD with minimal personal payment if it is first prescribed within 3 years since diagnosis. Rasagiline has gradually replaced selegiline in clinical practice since 2007, mostly as a result of marketing industry policy and based on several large-scale, placebo-controlled clinical trials.5,7–11 The time interval between the commencement of rasagiline or selegiline treatment as the first antiparkinsonian drug (APD) and the initiation of dopaminergic treatment as a marker of symptoms progression have never been studied before. Furthermore, the symptomatic effect of selegiline6,12 and rasagiline8–11 has never been compared in a real-life study but was rather compared solely in an indirect meta-analysis of placebo-controlled randomized clinical trials.13
The present study used the pharmacy database of the second largest health maintenance organization (HMO) in Israel (Maccabi Healthcare Services [MHS]) that covers approximately 25% of the Israeli population. All newly prescribed MAO-BI patients for the years 1998–2012 who were naive to other APDs and met the algorithm-based criteria for being a patient with PD14 were identified. Their records were checked retrospectively to detect the time that DA or levodopa was first purchased. Because selegiline was prescribed until 2006 and mostly rasagiline was prescribed since then, it was possible to study the relationships between the individual MAO-BI and the time to the initiation of dopaminergic therapy in real-life high-quality data collected for a period of 15 years.
METHODS
Participants (Exposure Groups)
The MAO-BIs study group was identified from a pharmacy-based PD cohort for 1998-2008 that had been created by Chillag-Talmor et al14 and then extended until December 31, 2012. Individual data included all APD purchased by the patients during the study period. Classification of the PD diagnosis as being “definite,” “probable,” or “possible” was based on the patterns of drug consumption, the patient's age, and the length of the follow-up period.14
Because rasagiline gradually replaced selegiline after its introduction in Israel in mid-2006, the study population was divided into 2 groups such that each had 6 years of follow-up. Specifically, the selegiline group included patients who began selegiline monotherapy between January 01, 2001, and December 31, 2006. The rasagiline group included patients who began rasagiline monotherapy between January 01, 2007, and December 31, 2012. Follow-up for the selegiline group began from the date of the first selegiline purchase and ended at the date of death or December 31, 2006, whichever occurred first. Follow-up for the rasagiline group began from the date of the first rasagiline purchase and ended at the date of death or December 31, 2012, whichever occurred first. Patients who switched from 1 treatment to the other during the study period were excluded.
This is a retrospective study on the basis of pharmacologic data retrieved from the computerized database of a large HMO. Data on sex, date of birth, and status at HMO (active/deceased/left with dates) were gathered from other MHS databases and linked. The study was approved by the institutional review boards of both Tel Aviv Medical Center and MHS.
Statistical analysis
Kaplan-Meier curves were used to describe and compare cumulative time to event in the 2 study groups (selegiline users and rasagiline users). Measurements included the time from the first MAO-BI purchase until the initiation of DA treatment and to the initiation of levodopa treatment. Cox proportional hazard modeling was established to estimate adjusted hazard ratio (HR) and 95% confidence intervals (95% CIs) for the 2 study groups, where age at first purchase/treatment and sex were the covariates because of their known effects on disease progression.14–17 Sensitivity analysis included another event, either DA or levodopa treatment.
RESULTS
Participants' Characteristics
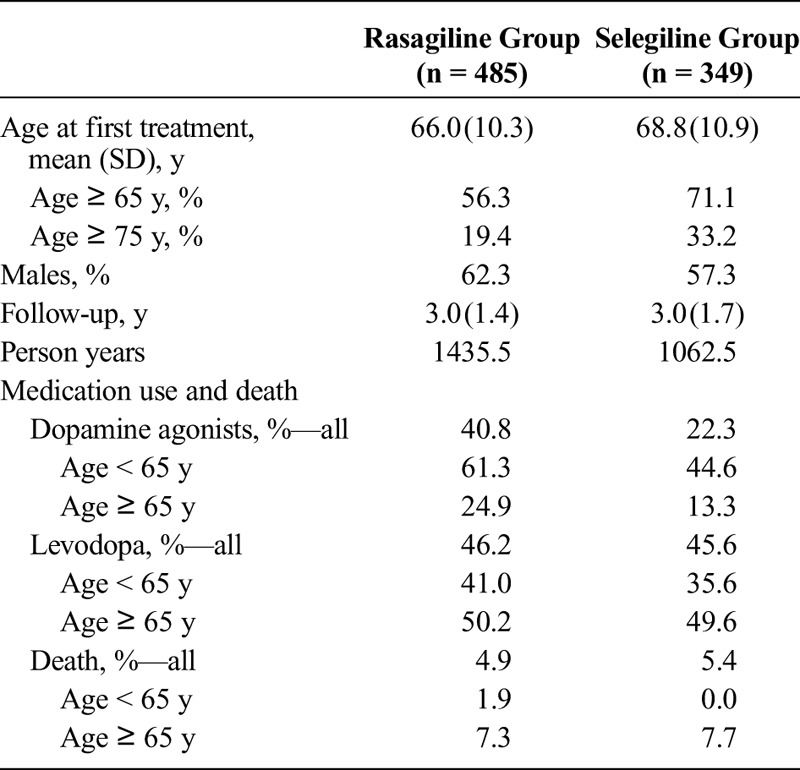
A total of 1009 treatment-naive patients with PD were identified as cases whose first APD was selegiline (n = 454) or rasagiline (n = 555). They were assessed by us as “definite,” “probable,” or “possible” PD cases.14 The possible PD cases were then excluded to reduce misclassification bias, and we were left with 349 cases who received selegiline and 485 who received rasagiline as their first APD. The 2 groups were compared (Table 1) using univariate analysis, which yielded that the length of follow-up was similar, but the mean age at first treatment differed significantly between the groups (P = 0.0001), with the rasagiline group being younger at first purchase. Comparison of the rates of medication use and death revealed that although the rates of levodopa use and death were similar for the 2 groups, the rates of DA use differed significantly between the groups (P < 0.0001, higher in the rasagiline group). Similarly, the rates of either DA or levodopa use were higher in the rasagiline group (63.5% vs 52.4%, P = 0.0014).
TABLE 1.
Characteristics of the Study Groups of Treatment-Naive PD Patients Starting on Rasagiline or Selegiline Monotherapy (N = 834)
Time to Endpoints
Figure 1 presents DA free survival from first purchase of MAO-BI in the 2 study groups, and Figure 2 presents levodopa free survival from first purchase of MAO-BI in the 2 study groups. Table 2 presents adjusted risks.
FIGURE 1.
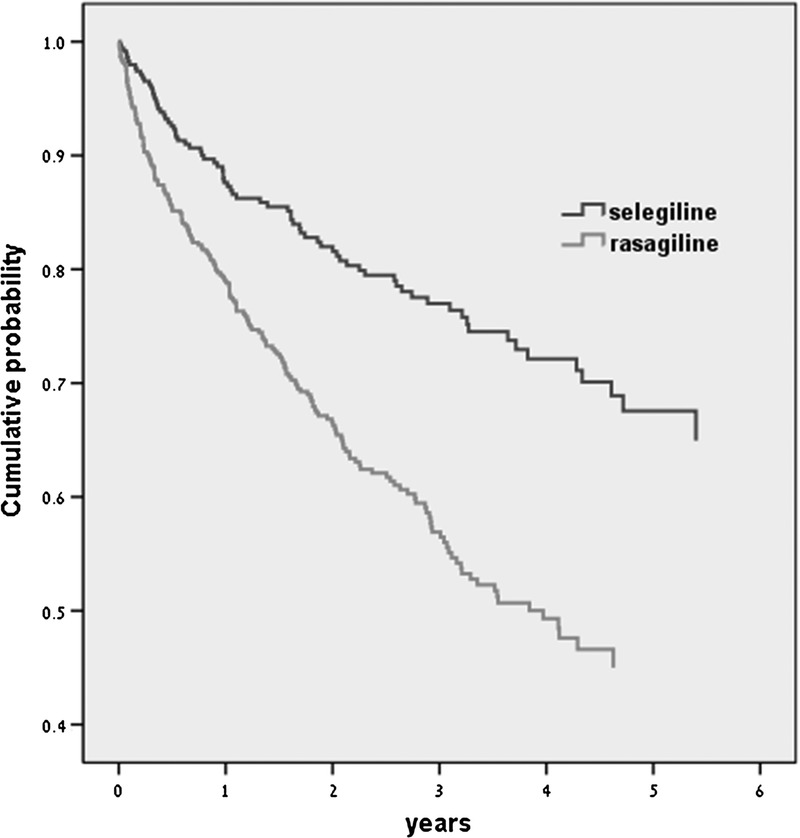
K-M curves; Time free of DA in rasagiline (n = 485) and selegiline (n = 349) groups (log-rank test P < 0.001).
FIGURE 2.
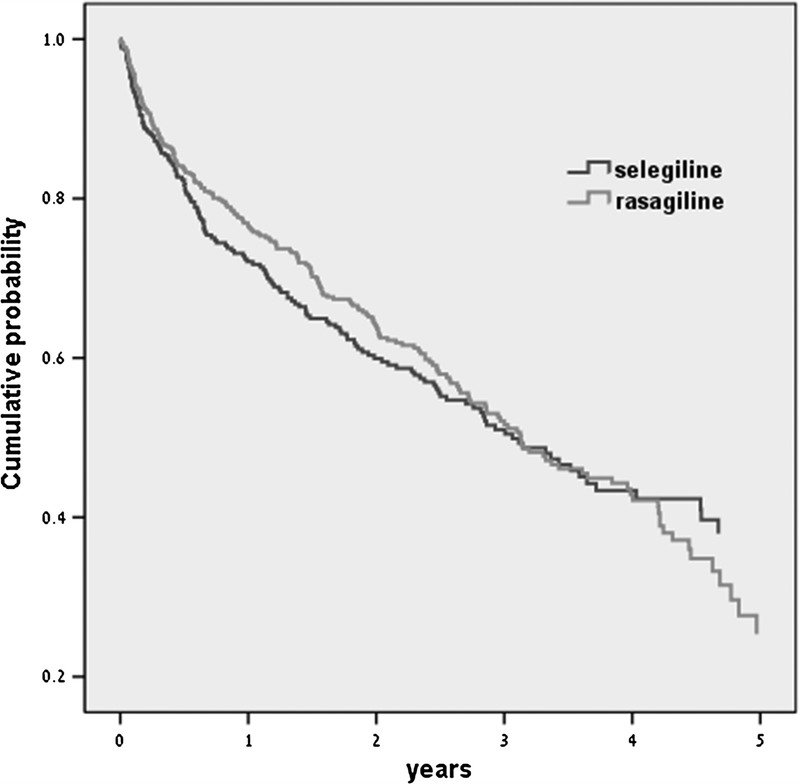
K-M curves; Time free of levodopa in rasagiline (n = 485) and selegiline (n = 349) groups (log-rank test P = ns).
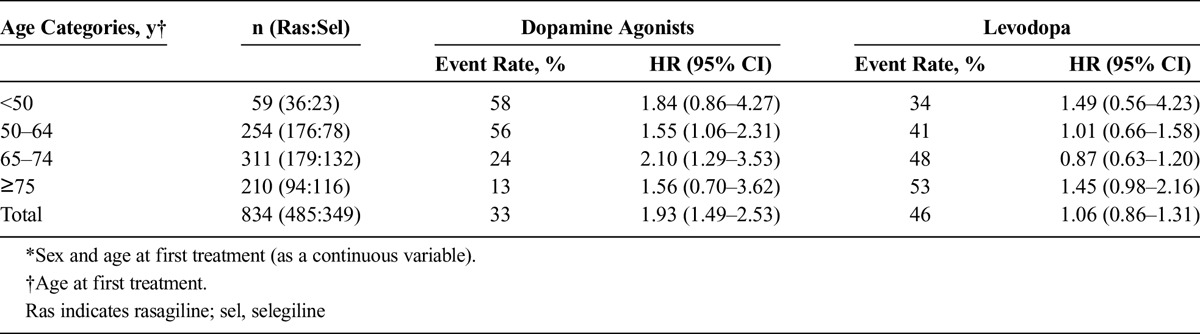
TABLE 2.
Adjusted* HR (95% CI) for the Rasagiline Group Compared With the Selegiline Group to Initiate Treatment With Dopamine Agonists or Levodopa
Time to DA
We found a significantly shorter time free of DA in the rasagiline group compared with the selegiline group for all age categories (log-rank test, P < 0.0001). The hazard to purchase DA was twofold higher for the rasagiline group compared with the selegiline group (HR, 1.93; 95% CI, 1.49–2.53). Stratification by age categories yielded a shorter time (ie, an increased HR) to initiate DA for the rasagiline group compared with the selegiline group in all 4 age categories as follows: HR of 1.84 for younger than 50 years, HR of 1.55 for age 50 to 64 years, HR of 2.10 for age 65 to 74 years, and HR of 1.56 for 75 years or older (P = nonsignificant [ns], P = 0.0273, P = 0.0038, and P = ns, respectively). Sex was a nonsignificant covariate in all models, whereas continuous age at first treatment was at least borderline significant in the age categories stratification models, except for 75 years or older.
Sensitivity Analysis: We restricted the study dates from January 01, 2004, to December 31, 2009, such that each group had 3 years of follow-up; specifically, the selegiline group included 236 patients who began selegiline monotherapy between January 01, 2004 and December 31, 2006, and the rasagiline group included 236 patients who began rasagiline monotherapy between January 01, 2007, and December 31, 2009. The comparisons in time to DA between the groups were in the same direction but with less significance (HR, 1.77; 95% CI, 1.10–2.91; P = 0.0207).
In addition, we evaluated the time to initiation of either DA or levodopa, and the results were similar to the time of initiation of DA alone for all age categories and by age group. We found a significantly shorter period free of either DA or levodopa in the rasagiline group compared with that of the selegiline group.
Time to Levodopa
We found no difference in time free of levodopa for all ages between the 2 study groups (log-rank test, P = ns). The hazard to initiate levodopa was similar for both groups (HR, 1.06; 95% CI, 0.86-1.31). Stratification by age categories yielded an increased but nonsignificant hazard to purchase levodopa in the rasagiline group in the youngest and oldest age categories: HR of 1.49 for younger than 50 years and HR of 1.55 for 75 years or older (P = ns and P = 0.0647, respectively). For those who were treated with DA before levodopa (n = 276 cases), we found some decreased risk in the rasagiline group compared with the selegiline group to initiate levodopa (HR, 0.77, 95% CI, 0.56–1.07, P = 0.1233). Although for those who were not treated with DA before levodopa (n = 558 cases), the time to initiate levodopa was similar in the rasagiline and selegiline groups (HR, 1.07; 95% CI, 0.81–1.40; P = 0.6489).
Sensitivity Analysis: When the possible PD cases were included in our analysis (with 6 years of follow-up for each group), increasing the sample size from 834 to 1009, the comparisons in time to DA or levodopa between the rasagiline and the selegiline groups were in the same direction but with greater significance.
DISCUSSION
Rasagiline and selegiline have never been compared in a head-to-head randomized controlled trial (RCT), and this is the first attempt to evaluate and compare retrospectively in a real-life setting the relationship between the type of MAO-BI given to treatment-naive patients with PD and time to first purchase of DA or levodopa treatment in an observational community-based study.
Overall, our results indicated a similar time to levodopa for patients treated with either rasagiline or selegiline as their initial MAO-BI. A stratification by age at first treatment revealed some nonsignificantly increased HR of approximately 50% for the rasagiline group to first initiate levodopa compared with the selegiline group among the younger (<50 years) and oldest (>75 years) subgroups. Interestingly, for those who were treated with DA before levodopa, we found some decreased risk of 23% in the rasagiline group compared with the selegiline group to initiate levodopa.
The clinical effectiveness of rasagiline and selegiline was evaluated by reviewing short-term randomized, placebo-controlled trials in patients with early PD, with changes in the Unified Parkinson Disease Rating Scale as endpoint.13,18 The results of analysis of 5 studies with selegiline and 4 studies with rasagiline yielded a similar level of efficacy,13 whereas an earlier indirect meta-analysis reported an advantage for rasagiline over selegiline when the Unified Parkinson Disease Rating Scale total score was the objective measure of symptomatic effect.18
Considering the essential difference between the pharmacological spectrum of selegiline and rasagiline,5 the results of the present study demonstrated that the group treated with selegiline as initial MAO-BI stayed without DA for a longer period compared with the rasagiline group; the hazard to initiate DA was twice as high in the rasagiline group compared with the selegiline group. This finding applied to the 4 age categories, although with some difference in HR values.
In Israel, neurologists, primary care physicians, and gerontologists are all making the diagnosis of PD. The younger the patient, the more likely a neurologist will be the one to make the final diagnosis and to initiate treatment.
These findings may possibly be explained by a change in the clinical practice of physicians in Israel in prescribing DA.
Specifically, they have followed a more conservative approach of delaying the initiation of DA as of 2001–2006, compared with customarily prescribing DA earlier in the course of the disease between 2007 and 2012. The change in prescription behavior might be the result of recent studies that demonstrated DA as having some antidepressant effects,19,20 in addition to their proven effect on the motor aspects of the disease.21 Another hypothetical explanation for the earlier use of DA in the second period of the present study is the physicians' belief that DAs have a disease-modifying effect of slowing PD progression. This idea has been suggested in the past,22,23 but it had never been supported by scientific data.23 To explore this possibility, we have looked at the last 3 years of the selegiline group, 2004–2006, and compared them with the first 3 years in the rasagiline group, 2007–2009, assuming that physicians' belief with regard to drug effect will not change sharply at 1 year. This sensitivity analysis of shorter time spans of 3 years yielded similar results as for the 6 years, which, to our understanding, might indicate that physicians' beliefs are less likely the preferred explanation. Another possible explanation for the longer period until DA implementation in the selegiline-treated group is its better symptomatic effect that could delay the need for dopaminergic treatment.
A symptomatic effect of both MAO-BIs has been well demonstrated in prospective RCTs for both drugs in the early stages of PD.6 The possible effect of MAO-BIs on disease progression, their role in the pathological process, and their symptomatic effect have been a matter of debate since the first large-scale RCT almost 25 years ago, when the results of the 1991 DATATOP study demonstrated the beneficial effect of selegiline in delaying the need for levodopa treatment in naive patients with PD.24 Several observations over the years have supported a disease-modifying effect of MAO-BIs, such as delaying the appearance of freezing or motor response fluctuations,25 but no conclusive results have ever been reached. Consequently, the FDA refused to add that effect to rasagiline's official labeling.26 It could be argued that prescribing DA later in the selegiline group might indicate a better disease-modifying effect and that having no difference in time to levodopa reflects no difference between the 2 drugs in their role on disease progression. However, a possible interaction effect between rasagiline and DA for better symptomatic or disease-modifying effect is suggested on the basis of the finding that the time to levodopa was longer in the rasagiline-treated group when compared with the selegiline-treated group in the subgroup who was given DA before levodopa.
The present analysis of extensive community data has considerable advantage more than the earlier short-term controlled, small-scale clinical trials on the drugs' effectiveness. Our study population better represents the general population and differs from the highly selected group of patients usually enrolled in RCT studies. Our endpoints are clinically relevant and reflect doctors' practice in the use of 2 MAO-BIs. Indeed, time to dopaminergic therapy was based on clinical decisions of hundreds of neurologists in Israel who made that decision solely according to the patient's clinical need and not motivated to delay its prescription for any academic or industry-oriented reasons. The quality of such studies is heavily dependent on the completeness and accuracy of the databases that are used; our pharmacy data source is a highly accurate and complete database, which is closely monitored and considered highly reliable, because it is maintained for administrative purposes and has major financial implications.
The disadvantages of our study include the following: purchase of drugs does not accurately represent actual drug use and measure may include a lag time to treatment initiation of up to 1 year. In addition, no clinical information about disease severity was available. The choice of type of APD treatment was made by the physicians on the basis of national and international guidelines and recommendations, on adverse effects of the drugs to certain patients, as well as on marketing efforts on the part of the pharmaceutical companies.
To conclude, this is the first attempt to compare the effect of 2 commercially available MAO-BIs by evaluating the time to initiating dopaminergic treatment as a marker. The present large-scale study demonstrated a similar effect of rasagiline and selegiline with regard to the time to first purchasing of levodopa. The results suggest some possible advantage for selegiline, either because of better symptomatic effect or superiority in its disease-modifying effect, although such conclusions should be taken with caution, and additional studies will be needed to explore this issue in head-to-head RCTs. A possible interaction effect between rasagiline and DA for better symptomatic or disease-modifying effect is suggested.
Other endpoints, such as time to motor response fluctuations, first fall, dementia, or time to death, should also be studied to further explore the effect of specific MAO-BI on PD progression.
Footnotes
Conflicts of Interest and Source of Funding: The authors have no conflicts of interest to declare.
C.P. was involved in study conceptualization and design, data analysis and interpretation, and writing the article. H.S. contributed in data arrangement, primary data analysis, and writing. V.R. helped in data arrangement and in writing and revising the article. T.G. was part of study conceptualization, literature review, and revision of article. B.E. assisted in study conceptualization and critical revision of the article. J.D. did the data retrieval and helped in revising the article. N.G. was part of study conceptualization and design, interpretation, and writing the article.
REFERENCES
- 1.Connolly BS, Lang AE. Pharmacological treatment of Parkinson disease: a review. JAMA 2014;311:1670–1683. [DOI] [PubMed] [Google Scholar]
- 2.Stowe RL, Ives NJ, Clarke C, et al. Dopamine agonist therapy in early Parkinson's disease. Cochrane Database Syst Rev 2008;2:CD006564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.LeWitt PA. Levodopa for the treatment of Parkinson's disease. N Engl J Med 2008;359:2468–2476. [DOI] [PubMed] [Google Scholar]
- 4.Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson's disease (2001): treatment guidelines. Neurology 2001;56:S1–S88. [DOI] [PubMed] [Google Scholar]
- 5.LeWitt PA. MAO-B inhibitor know-how; back to the pharm. Neurology 2009;72:1352–1357. [DOI] [PubMed] [Google Scholar]
- 6.Olanow CW. MAO-B inhibitors in Parkinson's disease. Adv Neurol 1993;60:666–716. [PubMed] [Google Scholar]
- 7.Ives NJ, Stowe RL, Marro J, et al. Monoamine oxidase type B inhibitors in early Parkinson's disease: meta-analysis of 17 randomised trials involving 3525 patients. BMJ 2004;329:593–600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Olanow CW, Rascol O, Hauser R, et al. A double-blind, delayed-start trial of rasagiline in Parkinson's disease. N Engl J Med 2009;361(13):1268–1278. [DOI] [PubMed] [Google Scholar]
- 9.Parkinson Study Group. A controlled, randomized, delayed-start study of rasagiline in early Parkinson disease. Arch Neurol 2004;61:561–566. [DOI] [PubMed] [Google Scholar]
- 10.Hauser RA, Lew MF, Hurtig HI, et al. Long-term outcome of early versus delayed rasagiline treatment in early Parkinson's disease. Mov Disord 2009;24:564–573. [DOI] [PubMed] [Google Scholar]
- 11.Rascol O, Fitzer-Attas CJ, Hauser R, et al. A double-blind, delayed-start trial of rasagiline in Parkinson's disease (the ADAGIO study): prespecified and post-hoc analyses of the need for additional therapies, changes in UPDRS scores, and non-motor outcomes. Lancet Neurol 2011;10:415–423. [DOI] [PubMed] [Google Scholar]
- 12.Palhagen S, Heinonen E, Hagglund J, et al. Selegiline slows the progression of the symptoms of Parkinson disease. Neurology 2006;66:1200–1206. [DOI] [PubMed] [Google Scholar]
- 13.Marconi S, Zwingers T. Comparative efficacy of selegiline versus rasagiline in the treatment of early Parkinson's disease. Eur Rev Med Pharmacol Sci 2014;18:1879–1882. [PubMed] [Google Scholar]
- 14.Chillag-Talmor O, Giladi N, Linn S, et al. Use of a refined drug tracer algorithm to estimate prevalence and incidence of Parkinson's disease in a large Israeli population. J Parkinsons Dis 2011;1:35–47. [DOI] [PubMed] [Google Scholar]
- 15.de Lau LML, Breteler MMB. Epidemiology of Parkinson's disease. Lancet Neurol 2006;5:525–535. [DOI] [PubMed] [Google Scholar]
- 16.Wirdefeldt K, Adami HO, Cole P, et al. Epidemiology and etiology of Parkinson's disease: a review of the evidence. Eur J Epidemiol 2011;26:S1–58. [DOI] [PubMed] [Google Scholar]
- 17.Chillag-Talmor O, Giladi N, Linn S, et al. Estimation of Parkinson's disease survival in Israeli men and women, using health maintenance organization pharmacy data in a unique approach. J Neurol 2013;260:62–70. [DOI] [PubMed] [Google Scholar]
- 18.Jost WH, Friede M, Schnitker J. Indirect meta-analysis of randomized placebo-controlled clinical trials on rasagiline and selegiline in the symptomatic treatment of Parkinson's disease. Basal Ganglia 2012;2:S17–26. [Google Scholar]
- 19.Leentjens AF. The role of dopamine agonists in the treatment of depression in patients with Parkinson's disease: a systematic review. Drugs 2011;71:273–286. [DOI] [PubMed] [Google Scholar]
- 20.Troeung L, Egan SJ, Gasson N. A Meta-analysis of randomised placebo-controlled treatment trials for depression and anxiety in Parkinsons disease. PLoS One 2013;8:e79510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Montastruc JL, Rascol O, Senard JM. Treatment of Parkinson's disease should begin with a dopamine agonist. Mov Disord 1999;14:725–730. [DOI] [PubMed] [Google Scholar]
- 22.Whone AL, Watts RL, Stoessl AJ, et al. Slower progression of Parkinson's disease with ropinirole versus levodopa: The REAL-PET study. Ann Neurol 2003;54:93–101. [DOI] [PubMed] [Google Scholar]
- 23.Olanow CW, Kieburtz K, Schapira AH. Why have we failed to achieve neuroprotection in Parkinson's disease? Ann Neurol 2008;64:S101–110. [DOI] [PubMed] [Google Scholar]
- 24.Parkinson Study Group. Impact of deprenyl and tocopherol treatment on Parkinson's disease in DATATOP patients requiring levodopa. Ann Neurol 1996;39:37–45. [DOI] [PubMed] [Google Scholar]
- 25.Schapira AH. Monoamine oxidase B inhibitors for the treatment of Parkinson's disease: a review of symptomatic and potential disease-modifying effects. CNS Drugs 2011;25:1061–1071. [DOI] [PubMed] [Google Scholar]
- 26.Suchowersky O, Gronseth G, Perlmutter J, et al. Practice Parameter: neuroprotective strategies and alternative therapies for Parkinson disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2006;66:976–982. [DOI] [PubMed] [Google Scholar]