

Abstract
Introduction
Fractional exhaled nitric oxide (FENO) is a biomarker of airway inflammation in asthma. The measurement of FENO is utilized to assist in the diagnosis and treatment of children with asthma, especially for those treated with inhaled corticosteroids.
Objectives
The aims of this study were to evaluate the correlations between FENO and atopic status, blood eosinophil levels, FCER2 mutation, and asthma control in Vietnamese children.
Subjects and methods
This was a prospective and descriptive study approved by the local Ethical Board. All children with uncontrolled asthma, seen in the National Hospital of Pediatrics (Hanoi, Vietnam), were included. Exhaled breath FENO, blood eosinophils, skin prick test, total IgE, asthma control test (ACT), and FCER2 gene polymorphism were performed at inclusion. They were followed up at 3 months to evaluate clinical status, FENO levels, and ACT.
Results
Forty-two children with uncontrolled asthma with a mean age of 10±3 years (6–16 years) were included. The male/female ratio was 2.5/1. The mean FENO levels were 26±25 ppb. FENO was significantly higher in patients with a positive skin prick test for respiratory allergens (P<0.05). FENO was significantly correlated with blood eosinophil levels (r=0.5217; P=0.0004). Five of the 32 subjects (15.6%) had a mutation of FCER2 gene (rs28364072 SNP). In this group, the levels of FENO were highest (37±10 ppb; P<0.05). The levels of FENO were significantly decreased after 3 months of treatment (17±8 ppb vs 26±25 ppb; P<0.05). Significant correlations between inhaled corticosteroid doses and FENO levels occurred at 1 and 3 months (r=0.415, P=0.007; r=0.396, P=0.010; respectively). There were no correlations between FENO levels, ACT, and daily use of salbutamol. After 3 months, asthma remained uncontrolled in 22.2% of children.
Conclusion
The measurement of FENO levels is a useful and feasible tool to predict clinical, biological, and asthma control in Vietnamese children.
Keywords: nitric oxide, FENO, eosinophils, asthma, FCER2, ICS
Video abstract
Introduction
Asthma is a diverse disease with many phenotypes, characterized by chronic airway inflammation, bronchial hyperresponsiveness, and smooth muscle contraction. In addition, the severity of airway obstruction increases secondary to secretions, decreased airway pliability, and mucosal edema. The present treatment paradigm is the use of bronchodilators for symptoms and inhaled corticosteroids (ICS) to reduce and control inflammation. As recommended by Global Initiative for Asthma (GINA),1 the assessment of asthma control is based on frequency of asthma symptoms, use of medication for asthma crisis and symptoms, activity inhibition, and severity of airway obstruction. However, this assessment does not directly reflect the severity of airway inflammation, the crucial key for appropriate asthma control.
Nitric oxide (NO) is a biomarker of airway inflammation. It is mainly synthesized by inducible nitric oxide synthase (iNOS) in epithelial cells and eosinophils in the airways of patients with asthma. The levels of NO in exhaled air (fractional exhaled nitric oxide [FENO]) is significantly increased in some of the phenotypes in asthma and can be detected with portable devices by using chemical electrolytic technique.2 The measurement of FENO is a noninvasive, easy to perform, and safe method for assessing airway inflammation in asthma. Since the early 1990s when FENO was first measured, many studies have shown close correlations between FENO levels and eosinophil counts in peripheral blood, sputum, bronchoalveolar lavage fluid, and in biopsied lung tissue.3,4 Therefore, FENO can be used as a relevant biomarker of airway inflammation in management of some cases of asthma. The measure of FENO also helps to predict asthma exacerbations, ICS response, and compliance to ICS.5 Recently, FENO measurement has been recommended by GINA in monitoring patients with asthma.1
In practice, clinical phenotyping of asthma in children is complex and dependent on the interaction between gene expression and environmental exposure (epigenetics). Two groups of genes have been focused upon in asthma, one is involved in the clinical phenotype of asthma patients and the other is involved in drug response. Previous studies demonstrated that in asthma patients, FCER2 has been significantly associated with poor lung function, high levels of IgE, risk of severe exacerbations, and need for high dose ICS.6,7 However, the correlation between FCER2 gene polymorphism with biomarkers of airway inflammation such as blood eosinophil or FENO level has not been clearly demonstrated. In addition, in developing countries, such as in Vietnam, the role of FENO and genetic polymorphism in asthma, especially in children with asthma, has not been well studied. Lastly, although ICS are the drug of choice for long-term treatment of uncontrolled asthma, the adherence of asthmatic children to ICS is very low in Vietnam.8
This study was planned to demonstrate the correlations between FENO and atopic status, blood eosinophil, FCER2 gene mutation, and the level of asthma control in Vietnamese children with uncontrolled asthma.
Subjects and methods
Subjects
Children with asthma and symptoms who presented to the Consultation Department or Department of Immunology, Allergy, and Rheumatology of the National Hospital of Pediatrics (Hanoi, Vietnam) from July 2014 to August 2015 were included in the present study parents/guardians signed an Institutional Review Board-approved consent forms on the patients’ behalf.
Inclusion criteria
All subjects with uncontrolled asthma, who were between the ages of 6–17 years, and not on medicine for at least a month, were included if they were able to perform spirometry, FENO measurement, and skin prick test (SPT). The diagnosis of asthma was based on the criteria recommended by GINA for children over 5 years.1
Exclusion criteria
Study subjects having one of the following were excluded: significant other chronic or acute disease, or severe asthma exacerbations needing systemic corticosteroid therapy (oral or injection) at inclusion.
Methods
Study design
This study was a prospective and descriptive study. All subjects with uncontrolled asthma were treated at inclusion as recommended by GINA. They were followed for 3 months. This study was approved by the Ethical Review Board of the National Hospital of Pediatrics (Hanoi, Vietnam).
Asthmatic children who met inclusion criteria were classified into four different levels of asthma severity for management (intermittent asthma: short-acting beta agonist [SABA] as needed; mild asthma: low dose ICS + SABA as needed; moderate asthma: moderate to high dose ICS + SABA as needed; severe asthma: moderate to high dose ICS + long-acting beta agonist + SABA as needed). ICS response and asthma control were evaluated by physicians as recommended: controlled, partially controlled, or uncontrolled asthma. Asthma control test (ACT) was used as a self-assessment by study subjects ≥12 years old or their parents (<12 years old). Usage of SABA was recorded in the diary by day and time for analyses.
Data collection
All data on medical and family history, clinical examination, and measures of FENO, spirometry, skin tests, blood eosinophils, and genetic polymorphism of study subjects were collected for statistical analyses. ACT was used for children over 12 years old with five scoring questions and four scoring questions for children <12 years old combined with three questions for their parents.
Laboratory techniques
Complete blood count with eosinophil value (%) was analyzed by automatic machines (XT-4000i-SYSMEX; Kope, Japan). IgE concentration in peripheral blood was quantified by chemical luminescence technique (COBASC 501; Hitachi, Japan).
SPT (Stallergenes; London, UK): negative control was 0.9% saline solution; positive control was 1 mg/mL of histamine. Six respiratory allergens including Dermatophagoides pteronyssinus, Dermatophagoides farinae, Blomia tropicalis, and hairs and epidermis of dogs, cats, and cockroaches were tested. Percutaneous skin test was considered positive when the wheal size exceeded the negative control by 3 mm.
Lung function testing (spirometry) was done by Koko (Inspire, Hertford, UK). The reversibility of forced expiratory volume in 1 second (FEV1) was evaluated after 15 minutes of using 200 µg salbutamol. The test was positive when there was an increase of FEV1 of FEV1 ≥12% and >200 mL.
Measuring exhaled NO concentration was done by Hypair NO (Medisoft, Sorinnes, Belgium) with expiratory air flow of 50 mL/sec. The mean value of two correctly performed measures was used for analyses. FENO levels were classified as recommended by the American Thoracic Society for children (<20 ppb: normal; 20–35 ppb: increased; >35 ppb: highly increased).5
Rs28364072 polymorphism in FCER2 gene was genotyped at the Laboratory for Molecular Biomedicine belonging to the School of Medicine and Pharmacy at Vietnam National University–Hanoi, using DNA extracted from peripheral blood leukocytes with a routine salting out procedure. Polymerase chain reaction method was used to amplify the alleles of the FCER2 gene, using the following forward and reverse primers: 5′-TCATAGCTCCAGCAGAGAACAC-3′ and 5′-GCCAAGACTCACCCTTCTAATCT-3′. The FCER2 gene amplified regions were then sequenced by using the BigDye®Terminator v3.1 Cycle Sequencing Kit on ABI 3500 Series Genetic Analyzer (Thermo Fisher Scientific, Waltham, MA, USA), and SNP alleles were identified by employing the BioEdit Version 7.1.9 (Abbott Laboratories, Carlbad, California, USA) for sequence alignment and analyses. Population allele and genotype frequencies were estimated based on the Hardy–Weinberg principles.
Statistical analyses
SPSS 22.0 software (IBM Corporation, Armonk, NY, USA) was used to analyze these data. Qualitative variables were expressed as numbers or percentage. Quantitative variables were presented as mean ± standard deviation. Standard distribution was tested by the Skewness-Kurtosis technique. Regression test was used to measure the correlation between FENO and quantitative variables with the correlation coefficient r of Pearson for standard distribution variables and of Spearman for nonstandard distribution variables. Mann–Whitney U test was used to evaluate the correlation between FENO and asthma control levels. The multiple correlations (FENO and allergens) were performed with Kruskal–Wallis test.
Results
Clinical and functional characteristics of study subjects
From July 2014 to August 2015, 42 subjects with the mean age of 10±3 years were included in the present study (Figure 1). There were 28.6% females and 71.4% males. Eighty-one percent of study subjects were atopic (Table 1) and 61.9% of study subjects had a familial history of allergy. Of the subjects, 57.1% had mild asthma and 42.9% moderate asthma. The results of spirometry demonstrated that the mean FEV1 was slightly reduced compared to predicted values (84±22%; Table 1). The mean FENO was 26±25 ppb. FENO levels of subjects with moderate asthma were significantly higher than subjects with mild asthma (38±34 ppb vs 17±10 ppb; Table 1).
Figure 1.

Study flow chart of recruitment and randomization.
Abbreviations: FENO, fractional exhaled nitric oxide; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroids; SABA, short-acting beta agonist.
Table 1.
Clinical and functional characteristics of study subjects
| Variables (n=42) | Mean ± SD |
|---|---|
| Age, years | 10±3 |
| Female (Male), % | 28.6 (71.4) |
| Height, cm | 134.8±13.5 |
| Weight, kg | 33.9±10.4 |
| BMI, kg/m2 | 18.4±3.2 |
| Personal atopic history, % | 81 |
| Eczema, % | 19 |
| Allergic rhinitis, % | 73.8 |
| Allergic conjunctivitis, % | 11.9 |
| Urticaria, % | 2.6 |
| Drug or food allergy, % | 11.5 |
| Familial atopic history*, % | 61.9 |
| Asthma severity | |
| Intermittent, % | 0 |
| Mild, % (n=24) | 57.1 |
| Moderate, % (n=18) | 42.9 |
| Severe, % | 0 |
| Asthma crisis at inclusion | |
| Yes, % | 52.5 |
| No, % | 47.5 |
| FVC, % of predicted | 86±18 |
| FEV1, % of predicted | 84±22 |
| FEV1/FVC, % | 94±12 |
| Salbutamol reversal test** | |
| Positive, % | 47.6 |
| Negative,% | 52.4 |
| FENO, ppb | 26±25 |
| Mild asthma subjects, ppb | 17±10 |
| Moderate asthma subjects, ppb | 38±34*** |
Notes:
Eczema, allergic rhinitis, allergic conjunctivitis, urticaria, drug or food allergy
gain of FEV1 ≥12%
significant difference vs mild asthma with P=0.0063
Abbreviations: SD, standard deviation; BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FENO, fractional exhaled nitric oxide.
Concentration of FENO compared between SPT-positive and –negative subjects
The concentrations of FENO when compared between subjects with positive SPT results and negative results are presented in Figure 2 and Table 2. FENO in subjects with positive SPT (with at least one respiratory allergen) was significantly higher than in those with negative SPT (24±12 ppb vs 5±2 ppb; P<0.05; Figure 2). The concentrations of FENO were not significantly different between those sensitive to the different allergens (Table 2).
Figure 2.
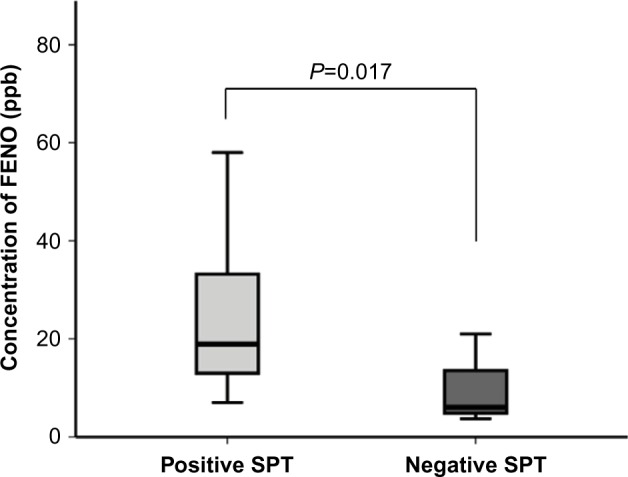
Concentration of FENO associated with skin prick test (SPT) being positive or negative.
Notes: Results are in response to a Student’s t-test.
Abbreviation: FENO, fractional exhaled nitric oxide.
Table 2.
Concentrations of FENO in subjects who tested positive to different allergens
| Respiratory allergens | n | FENO (ppb) | P |
|---|---|---|---|
| Dermatophagoides pteronyssinus + | 22 | 24±15 | NS |
| Dermatophagoides farinae + | 23 | 24±14 | NS |
| Blomia tropicalis + | 13 | 19±12 | NS |
| Dog hairs + | 2 | 31±9 | NS |
| Cat hairs + | 4 | 27±9 | NS |
| Cockroaches + | 8 | 21±13 | NS |
Abbreviations: FENO; fractional exhaled nitric oxide; NS, nonsignificant difference between each allergen.
Correlation between FENO levels and blood eosinophil counts
The correlation between FENO and percentage of blood eosinophils is presented in Figure 3. There was a moderate and significant correlation between the concentration of FENO and blood eosinophil percentage and absolute value (r=0.468, P=0.002; r=0.522, P=0.0004; respectively).
Figure 3.
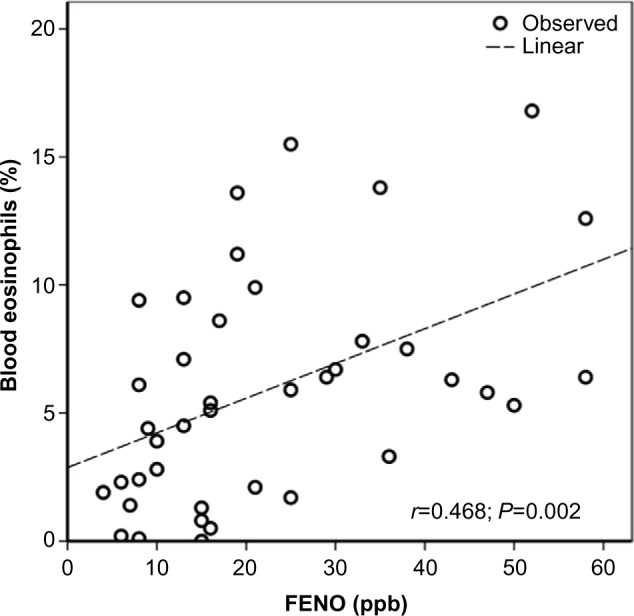
Correlation between FENO levels and blood eosinophils (n=40).
Notes: Results are in response to a regression analysis.
Abbreviation: FENO, fractional exhaled nitric oxide.
Concentration of FENO associated with FCER2 gene polymorphism
The concentration of FENO associated with FCER2 gene polymorphism is presented in Table 3. The concentration of FENO in homozygous variant rs28364072 (CC) of FCER2 gene was significantly higher than homozygous wild type (TT) and heterozygous (TC) (37±10 ppb vs 22±15 ppb and 19±7 ppb; P<0.05 and P<0.05; respectively; Table 3).
Table 3.
Concentration of FENO associated with rs28364072 variation of FCER2 gene
| rs28364072 variation | n | FENO (ppb) | P |
|---|---|---|---|
| Homozygous variant (CC) | 5 | 37±10 | P<0.05* |
| Homozygous wild type (TT) | 17 | 22±15 | NS |
| Heterozygous (TC) | 10 | 19±7 | NS |
Note:
Significant difference vs TT and TC
Abbreviations: FENO; fractional exhaled nitric oxide; NS, nonsignificant difference between TT and TC.
Correlations between FENO and ACT, ICS doses, and daily use of SABA
The correlations between FENO and ACT, ICS doses, and daily use of SABA are presented in Table 4. There were no significant correlations between FENO and ACT and daily use of SABA puffs (Table 4). There was a moderate and significant correlation between FENO and ICS doses at first day of inclusion and after 1–3 months (r=0.396 – 0.428; P=0.005–0.010; Table 4).
Table 4.
Correlation between FENO and ACT, ICS doses, and daily use of SABA
| Parameters | FENO (ppb)
|
|||||
|---|---|---|---|---|---|---|
| 1st day after inclusion | 1st month into therapy | 3rd month into therapy | ||||
|
| ||||||
| r | P | r | P | r | P | |
| ACT scores | 0.080 | 0.815 | 0.061 | 0.771 | 0.093 | 0.665 |
| ICS doses | 0.428 | 0.005 | 0.415 | 0.007 | 0.396 | 0.010 |
| SABA puffs | 0.088 | 0.585 | 0.092 | 0.567 | 0.020 | 0.903 |
Abbreviations: FENO; fractional exhaled nitric oxide; ACT, asthma control test; ICS, inhaled corticosteroids; SABA, short-acting beta agonist.
Variation of FENO concentration at 3 months after starting therapy
The variation of FENO concentration at inclusion, 1 month, and 3 months into therapy is presented in Figure 4. There was no significant difference between FENO concentration at inclusion and after 1 month of treatment (26±25 ppb vs 19±16 ppb; P=0.261; Figure 4). There was a significant difference of FENO concentration at inclusion and 3 months into therapy (26±25 ppb vs 17±8 ppb; P=0.034; Figure 4).
Figure 4.
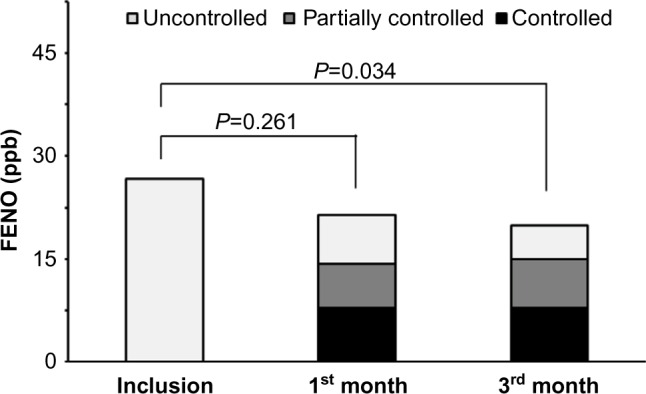
Variation between FENO concentrations from inclusion and after 1 and 3 months of therapy.
Abbreviation: FENO, fractional exhaled nitric oxide.
Discussion
The results of our study showed that 1) the levels of FENO in children with uncontrolled asthma were significantly higher than normal values; 2) FENO levels were significantly higher in subjects with moderate asthma, positive SPT, and FCER2 gene mutation; 3) there were significant correlations between FENO levels and blood eosinophil counts and ICS doses; and 4) there were significant decreases of FENO levels after 3 months of treatment with ICS.
In the present study, only children with mild-to-moderate uncontrolled asthma were included. Most of them (81%) were atopic, as defined by having positive skin tests, and had a family history of allergic disease (61.9%; Table 1). This result is consistent with previous studies, which demonstrated that over 50% of children with asthma had allergic symptoms.6,7 The mean concentration of FENO in study subjects was above the upper limit of normal range for healthy children.5 The highest levels of FENO were higher in subjects with positive skin tests (Figure 2), but were not dependent on the type of allergen the subject tested positive to (Table 2). Thus, FENO levels are independent of the specific allergen even though they are elevated in those with a positive skin test to an allergen (24±12 ppb vs 5±2 ppb; P<0.01; Figure 1). The results also showed that the level of FENO in moderate asthma was significantly higher than in mild asthma (Table 1). This result suggests that FENO concentrations might predict the severity of asthma as demonstrated previously.9,10
The results of our study demonstrated that there was a moderate and significant correlation between FENO and blood eosinophils (Figure 3). The correlation between FENO and blood eosinophil counts has been demonstrated in previous studies.11,12 Strunk et al showed that, in asthma patients, FENO levels were correlated with blood eosinophils and IgE levels.3 Our study showed similar results about the correlation between FENO and blood eosinophils, but in our study there was no correlation between FENO and IgE levels (r=0.09; P=0.609; data not shown). An increase of eosinophils in sputum is a specific biomarker of asthma; however, sputum eosinophil count is not available for many clinics and laboratories, especially in developing countries, because it is hard to obtain adequate samples that truly reflect the airway and the induction of sputum, preparation, staining, and reading is time-consuming and requires training and quality assurance.13
Unlike sputum eosinophils, FENO is an easy test to perform, requires minimal training and quality assurance, and similarly to sputum eosinophils it is a relevant biomarker for diagnosis, determining asthma stability and response to therapy. FENO is not a mediator, but an indirect marker of type 2 inflammation.14 High levels of FENO in exhaled breath and high levels of iNOS expression in the airway epithelial cells suggest eosinophilic airway inflammation.5 As noted above, the benefits of FENO are that the test is noninvasive, not expensive, easy to use, and results are obtained within a minute.15 For this reason, FENO is used along with other biomarkers such as blood eosinophil counts, IgE concentration, and periostin levels to categorize asthma phenotypes for individualized or personalized management.16
Analyses of FCER2 gene polymorphism showed that 15.6% (5/32) of children with asthma in our study had the homozygous variant (CC) of rs28364072 (Table 3). Interestingly, the levels of FENO in asthma subjects with rs28364072 homozygous variant (CC) were significantly higher than homozygous wild type (TT) and heterozygous (TC) variant (37±10 ppb vs 22±15 ppb and 19±7; P<0.05 and P<0.05; respectively; Table 3). A previous study demonstrated that the minor allele of T2206C (rs28364072) in FCER2 was significantly associated with poor lung function response in asthmatic patients.17 The multivariable association of the FCER2 SNPs with IgE levels has shown that variants in T2206C (rs28364072) were significantly associated with increases in IgE levels at 4 year, and also increased the risk of severe exacerbations in patients using ICS,18,19 but not in subjects with asthma control on ICS.18 The T2206C (rs28364072) variants were also associated with increased daily ICS doses.19 However, the correlation between FCER2 gene polymorphism and the level of FENO in exhaled breath has not been well demonstrated. The results of our study showed that FENO levels in asthmatic children with rs28364072 homozygous variant were significantly higher than in other variants (Table 3). In the present study, due to the small number of asthma subjects with FCER2 gene mutation (n=5) and also the small sample size (n=42), we could not define a specific FENO level that correlated with FCER2 gene mutation. Nonetheless our data suggest that high levels of FENO might predict a risk of having an FCER2 gene mutation. Obviously more studies should be done to confirm our suspicion.
Actually, many studies have attempted to associate gene expression with drug response in asthma. Particularly, FCER2 gene coding for low affinity IgE receptor has been investigated for associations with ICS response and asthma severity. Tantisira et al18 showed that the SPN - rs28364072 was related to the use of albuterol and also increased the number of exacerbations in asthmatics treated with ICS. In the present study, among 42 asthmatic children, 32 subjects had FCER2 sequencing and five subjects had a mutation (Table 3). These five children were well controlled with ICS after 3 months of treatment and had significantly decreased FENO levels (25±3 ppb at 3 months and 14±3 ppb at 1 month vs 40±7 ppb at inclusion; data not presented in the results).
As stated by the American Thoracic Society,5 FENO predicts the likelihood of response to ICS more consistently than spirometry, bronchodilator response, peak flow variation, or airway hyperresponsiveness to methacholine. Hence, high level of FENO in children with asthma is a reliable marker for airway inflammation mediated by eosinophils, and suggests a robust response to ICS, which in our study was fluticasone. Consistent with this is that after 3 months of treatment with ICS, FENO levels were significantly reduced (Figure 4) and this was most obvious in patients with the highest FENO levels at initial assessment when off of therapy (Table 4). Moreover, there was a significant correlation between levels of FENO and total doses of ICS (P=0.002; data not shown) required for control, which is consistent with previous studies.20
In the present study, the ACT was used to determine the levels of asthma control. Monthly, the study subjects went to hospital for clinical examination, medical history, treatment adherence, and ACT scoring. Unfortunately, the results of the present study failed to demonstrate a significant correlation between FENO levels and ACT scores and the daily uses of SABA (Table 4). Final results of the present study demonstrated that at the 3rd month, out of all the subjects with uncontrolled asthma at inclusion (n=42, 100%), 59.5% were controlled, 18.5% were partially controlled, and 22% were uncontrolled. This result was similar to a previous published study in adult Vietnamese asthma.21 In summary, the use of FENO is useful to predict FCERC2 gene mutation, ICS response, and asthma control in children with asthma in a developing country, such as Vietnam, where the use of FENO is easy and inexpensive.22
Conclusion
The level of FENO is a feasible biomarker to predict clinical and biological status of children with asthma. High levels of FENO are helpful for screening asthma subjects for the possibility of the FCER2 gene mutation and ICS response. Decreasing level of FENO is a good indicator for asthma control. Therefore, measuring FENO is a very useful tool in the management of patients with asthma, especially in developing countries, such as in Vietnam.
Acknowledgments
The authors would like to thank the Vietnamese National University–Hanoi; Project QG.14.59 for the grant that contributed to gene analyses.
Footnotes
Disclosure
The authors declare no conflicts of interest in this work.
References
- 1.Global Initiative for Asthma (GINA) 2014. Available from: http://ginasthma.org/archived-reports/
- 2.Alving K, Weitzberg E, Lundberg JM. Increase amount of nitric oxide in exhaled air of asthmatics. Eur Respir J. 1993;6(9):1368–1370. [PubMed] [Google Scholar]
- 3.Strunk RC, Szefler SJ, Phillips BR, et al. Relationship of exhaled nitric oxide to clinical and inflammatory marker of persistent asthma in children. J Allergy Clin Immunol. 2003;112(5):883–892. doi: 10.1016/j.jaci.2003.08.014. [DOI] [PubMed] [Google Scholar]
- 4.Payne DN, Adcock IM, Wilson NM, Oates T, Scallan M, Bush A. Relationship between exhaled nitric oxide and mucosal eosinophilic inflammation in children with difficult asthma, after treatment with oral prednisolone. Am J Respir Crit Care Med. 2001;164(8 Pt 1):1376–1381. doi: 10.1164/ajrccm.164.8.2101145. [DOI] [PubMed] [Google Scholar]
- 5.Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi: 10.1164/rccm.9120-11ST. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pearce N, Pekianen J, Beasley R. How much asthma is really attributable to atopy? Thorax. 1999;54(3):268–272. doi: 10.1136/thx.54.3.268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Douwes J, Gibson Pekianen P, Pearce N. Non-eosinophilic asthma: importance and possible mechanisms. Thorax. 2002;57(7):643–648. doi: 10.1136/thorax.57.7.643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sy DQ, Thanh Binh MH, Quoc NT, et al. Prevalence of asthma and asthma-like symptoms in Dalat Highlands, Vietnam. Singapore Med J. 2007;48(4):294–303. [PubMed] [Google Scholar]
- 9.Just J, Gouvis-Echraghi R, Rouve S, Wanin S, Moreau D, Annesi-Maesano I. Two novel, severe asthma phenotypes identified during childhood using a clustering approach. Eur Respir J. 2012;40(1):55–60. doi: 10.1183/09031936.00123411. [DOI] [PubMed] [Google Scholar]
- 10.Mahut B, Trinquart L, Le Bourgeois M, et al. Multicentre trial evaluating alveolar NO fraction as a marker of asthma control and severity. Allergy. 2010;65(5):636–644. doi: 10.1111/j.1398-9995.2009.02221.x. [DOI] [PubMed] [Google Scholar]
- 11.Jatakanon A, Lim S, Kharitonov SA, Chung KF, Barnes PJ. Correlation between exhaled nitric oxide, sputum eosinophils, and methacholine responsiveness in patients with mild asthma. Thorax. 1998;53(2):91–95. doi: 10.1136/thx.53.2.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Warke TJ, Fitch PS, Brown V, et al. Exhaled nitric oxide correlates with airway eosinophils in childhood asthma. Thorax. 2002;57(5):383–387. doi: 10.1136/thorax.57.5.383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Haldar P, Brightling CE, Hargadon B, et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N Engl J Med. 2009;360(10):973–984. doi: 10.1056/NEJMoa0808991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chibana K, Trudeau JB, Mustovich AT, et al. IL-13 induced increases in nitrite levels are primarily driven by increases in inducible nitric oxide synthase as compared with effects on arginases in human primary bronchial epithelial cells. Clin Exp Allergy. 2008;38(6):936–946. doi: 10.1111/j.1365-2222.2008.02969.x. [DOI] [PubMed] [Google Scholar]
- 15.Smith AD, Cowan JO, Filsell S, et al. Diagnosing asthma: comparisons between exhaled nitric oxide measurements and conventional tests. Am J Respir Crit Care Med. 2004;169(4):473–478. doi: 10.1164/rccm.200310-1376OC. [DOI] [PubMed] [Google Scholar]
- 16.Woodruff PG, Modrek B, Choy DF, et al. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am J Respir Crit Care Med. 2009;180(5):388–395. doi: 10.1164/rccm.200903-0392OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rogers AJ, Tantisira KG, Fuhlbrigge AL, et al. Predictors of poor response during asthma therapy differ with definition of outcome. Pharmacogenomics. 2009;10(8):1231–1242. doi: 10.2217/PGS.09.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tantisira KG, Silverman ES, Mariani TJ, et al. FCER2: a pharmacogenetic basis for severe exacerbations in children with asthma. J Allergy Clin Immunol. 2007;120(6):1285–1291. doi: 10.1016/j.jaci.2007.09.005. [DOI] [PubMed] [Google Scholar]
- 19.Koster ES, Maitland-van der Zee AH, Tavendale R, et al. FCER2 T2206C variant associated with chronic symptoms and exacerbations in steroid-treated asthmatic children. Allergy. 2011;66(12):1546–1552. doi: 10.1111/j.1398-9995.2011.02701.x. [DOI] [PubMed] [Google Scholar]
- 20.Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med. 2005;352(21):2163–2173. doi: 10.1056/NEJMoa043596. [DOI] [PubMed] [Google Scholar]
- 21.Duong-Quy S, Hua-Huy T, Doan-Quynh N, et al. A study of exhaled NO (FENO) measurement used to determine asthma control, dose of inhaled corticosteroid and cost in a developing country. Eur Respir J. 2015;46(Suppl 59):5013. [Google Scholar]
- 22.Duong-Quy S, Hua-Huy T, Tran-Mai-Thi HT, Le-Dong NN, Craig TJ, Dinh-Xuan AT. Study of Exhaled Nitric Oxide in Subjects with Suspected Obstructive Sleep Apnea: A Pilot Study in Vietnam. Pulm Med. 2016;2016:3050918. doi: 10.1155/2016/3050918. [DOI] [PMC free article] [PubMed] [Google Scholar]