

Abstract
Background
Statins are used for treatment of hypercholestremia. Common adverse reports associated with use of statins are generalized bodyache, rhabdomyolysis, muscles weakness and gastrointestinal disorders. The current work is an attempt to explain how smooth muscles of gastrointestinal tissues are affected by the current statins (Simvastatin, atorvastatin, fluvastatin and rosuvastatin).
Methods
Effects of the current statins were studied on spontaneous activity of isolated rabbits’ jejunal preparations. Different molar concentrations (10−12–10−2M) of the statins were applied on spontaneously contracting rabbits’ jejunal preparations. As statins relaxed spontaneous activity, so we tested the statins on KCl (80 mM) induced contractions in similar test concentrations. Positive relaxant statins were tested again through construction of Calcium Concentration Response Curves (CCRCs) in the absence and presence of the statins using verapamil, a standard calcium channel blocker. CCRCs of statins were compared with CCRCs of verapamil.
Results
Simvastatin, atorvastatin, fluvastatin and rosuvastatin relaxed the spontaneous and KCl-induced contractions. IC50 for simvastatin on spontaneous rabbit’s jejunal preparations is −5.08 ± 0.1 Log 10 M. Similarly, IC50 for KCl-induced contractions is −4.25 ± 0.01 Log 10 M. Mean IC50 (Log 10 M) for atorvastatin on spontaneous rabbit’s jejunal preparations and KCl-induced contractions are −5.19 ± 0.07 and −4.37 ± 0.09, respectively. Fluvastatin relaxed spontaneous activity of rabbits’ jejunal preparations with an IC50 (Log 10 M) −4.5 ± 0.03. Rosuvastatin relaxed spontaneous as well as KCl (80 mM) induced contractions with respective IC50 (Log 10 M) −3.62 ± 0.04 and −4.57 ± 0.06. In case of CCRCs, tissues pre-treated with 4.6 μg/ml of simvastatin, have IC50 = −1.84 ± 0.03 [log (Ca++) M] vs control IC50 = −2.54 ± 0.04 [log (Ca++) M]. Similarly, atorvastatin, fluvastatin and rosuvastatin produced significant right shift in IC50 for CCRCs (P ≤ 0.05). In case of verapamil, IC50 for control curves is −2.45 ± 0.06 [log (Ca ++) M], while IC50 in presence of verapamil (0.1 μM) is −1.69 ± 0.05 [log (Ca ++) M]. Statins produced right shift in the IC50 of CCRCs. The effects of statins are like that of effects of verapamil, a standard calcium channel blocker.
Conclusions
Our findings suggest that current statins have calcium antagonistic effects that act on voltage gated calcium channels that may provide a rationale for cause muscle weakness and gastrointestinal disorders.
Keywords: Statins, Simvastatin, Atorvastatin, Fluvastatin, Rosuvastatin, Voltage gated calcium channels, Verapamil
Background
There are very hot discussions about the safety profile and role of statins use in low risk cardiovascular patients. Even stake holders in health professions ask for an impartial review of statins especially in patients who are at low risk [1]. Statins are therapeutically effective lipid lowering drugs, which are used to reduce blood cholesterol in patients with hypercholestremia [2]. Statins reduce the development of atherosclerosis and prevent formation of atheromatous lesion [3]. Statins inhibit the enzyme HMG-CoA reductase and prevents the de novo synthesis of cholesterol as well [4]. Statins decrease intracellular cholesterol level, which increases the LDL receptors that can combine and internalize circulating LDLs. Consequently plasma cholesterol level is reduced by inhibiting cholesterol synthesis and raise catabolism of LDLs [5]. It is explicit that statins decrease cholesterol in addition to have pleotropic action [6]. Three lipid lowering drugs i.e. lovastatin, simvastatin and pravaststin were approved for marketing in 1990 [7, 8]. Statins valuable effects were seen in cardiac patients [9]. With passage of time, its adverse effects started appearing. Following administration of normal doses, statins are quickly absorbed and gain peak plasma concentrations within 4 h. They are metabolised by Cytochrome P450, which is composed of 30 isoenzymes. [10, 11]. Fluvastatin is metabolized through CYP2C9 and drugs like fluconazole and diclofenac (inhibitors of CYP2C9) interact to raise plasma levels of the statins [12]. Common adverse effects of statins are muscle pain and weakness, which can progress to rhabdomyolysis [13, 14]. Myositis, myalgia and cataract [15] are mostly caused by fluvastatin and simvastatin. Cerivastatin was withdrawn from market because of myotoxicity produced in most of the patients [16]. Most common unwanted effects of statin on gastrointestinal system are constipation, dyspepsia, abdominal pain, nausea, vomiting, heartburn and flatulence [15]. Smooth muscles’ contraction of GIT is due to calcium influx, which is regulated by calmodulin mechanism. Stimulating fibres in myosin filaments cause to develop attractive forces between actin and myosin filaments which is responsible for smooth muscles contractions. Total cholesterol level in human body is decreased by regulating cholesterol quantity in intestinal wall due to reducing Acetyl Co acyltransferase enzyme [17]. Statins also deregulate calcium channels that stimulate differentiated phenotype of vascular smooth muscle cells, as a consequence, reactivate calcium influx pathway and also upregulate L-type calcium channels, where calcium channel blocker effect is synergized in vascular cells [18]. But this upregulation takes time to develop and was studied in cell lines. It was also observed in animal study that using long term statins in hypertensive animals normalized blood pressure and wall of blood vessels [19]. Perhaps, this may be attributed to reports which say that smooth muscles’ cell migration, proliferation and invasion was inhibited by statins due to preventing isoprenoid pathways that subsequently inhibit Rhoprenylation of smooth muscles’ cells [20]. As there are reports for GI upsets with statins in start of therapy, hence we designed current study to test the direct effects of statins on isolated rabbits’ jejunal preparations. Thus our objective was to check the current statins for possible inhibitory effects on voltage gated calcium channels that may describe possible rationale for gastrointestinal disorders.
Study setting
The study was carried out in Department of Pharmacology, Institute of Basic Medical Sciences, Khyber Medical University, Peshawar, Khyber Pakhtunkhwa, Pakistan.
Methods
Effects of current statins on isolated rabbits’ jejunal preparation
The aim of the current work is to find out possible effects of some current statins (simvastatin, atorvastatin, fluvastatin and rosuvastatin) on isolated rabbits’ jejunal preparations.
Drugs and standards
Analytical grade chemicals were used in the experiments. Acetylcholine was purchased from BDH, Poole, England, which was used for maintenance of isolated tissues. Raw materials of rosuvastatin and atorvastatin as calcium salts were obtained from Ferozsons Laboratories Pvt. Ltd. Nowshera, Pakistan. Raw material of simvastatin was taken from Polyfine Pharmaceutical Industry, Peshawar. Fluvastatin of Novartis Pharma were purchased from local market of Peshawar, Pakistan. Raw materials, which had poor solubility in Tyrode’s solutions, were suspended in 0.01 % Carboxy Methyl Cellulose (CMC). However, a negative control of 0.01 % of CMC in deionized water was run to rule out any possible effects of CMC. All solutions and suspensions were freshly prepared on the same days of experiments.
Animals
Local breed rabbits weighing (1.5–2.0 kg; either sex) were used in the experiments. They were kept in animal house under controlled environment at Institute of Basic Medical Sciences, Khyber Medical University, Peshawar, Pakistan. The animals ware fasted overnight before the days of experiments. They had free access to water. The study protocols were approved by the Advanced Study & Research Board and Ethical Board (Approval No. Dir/KMU/-EB/SE/000138) of the Khyber Medical University, Peshawar, Pakistan.
Data recording
Intestinal responses were recorded using Force Transducer (Model No: MLT 0210/A Pan Lab S.I), connected through an amplifier FE 221 attached with four channels Power Lab (Model No: 4/25 T) AD Instruments, Australia. Lab Chart 7 was used to record and interpret the intestinal responses of isolated jejunal preparations.
Physiological solutions used in the experiments
Normal Tyrode’s solution, Potassium Normal (Ca++ free) Tyrode’s solution and Potassium Rich (Ca++ free) Tyrode’s solutions were used in the experiments. All solutions were prepared in deionized water on the same day of experiments.
Effects of statins on spontaneous rabbits’ jejunal preparations
Abdomens of overnight fasted rabbits were opened. Their jejunums were removed and placed in petri dishes containing Tyrode’s solution. The tissues were maintained with constant supply of carbogen gas (95 % O2, 5 % CO2) [21]. Pieces of about 1.5 cm were cut from the jejunums and mounted in organ bath containing Tyrode’s solution already maintained with carbogen gas (95 % O2, 5 % CO2) on 37 ± 1 °C. The composition of Tyrode’s solution was (mM) KCl 2.7, NaH2PO4 0.4, NaCl 136.9, Glucose 5.6, MgCl2 1.1, CaCl2 1.8, NaHCO3 11.9 on pH 7.4. Test concentrations of current statins were prepared in deionized water as mentioned above. The statins were added in cumulative manner to the organ bath in test concentrations Log10 (1 × 10−12–1 × 10−3) M which entail their plasma levels. The test samples were applied in a period of 1 min gap. Effects on spontaneous jejunal preparations were recorded as per our reported procedures [22, 23]. Earlier, tissues were stabilized for a period of 30 min before testing the statins.
Effects of statins on KCl (80 mM)-induced contractions
As KCl-depolarizes the tissues and keep the tissues in sustained contractions, hence any relaxing effects are usually, but not necessarily, regarded as to follow voltage gated calcium channels. So we tested the statins on KCl-induced contraction in similar equimolar concentrations Log10 (1 × 10−12–1 × 10−3) M in cumulative manners. Their effects are recorded [22, 24]. IC50 were calculated using Graph Pad Prism.
Effects of statins on calcium concentration response curves (CCRCs)
For confirmation of involvement of voltage gated calcium channels, we constructed CCRCs in a range of calcium concentration 1 × 10−4–256 × 10−4 M in absence and presence of different concentrations of statins as per our reported practice [23, 25, 26]. Verapamil was used as standard calcium channel blocker [23, 25–27]. Briefly describing the procedure, the tissues were maintained in Tyrode’s solution. After stabilization of tissues, the tissues were exposed to a series of wash with Tyrode’s Normal (calcium free) solution followed by exposure to K-Rich Tyrode’s solution. K-Rich Tyrode’s solution composition was (mM) NaCl 91.04, KCl 50, NaH2 PO4 0.42, MgCl2 1.05, EDTA 0.1, NaHCO3 11.90 and glucose 5.55. This lead to decalcification of tissues. The temperature was maintained on 37 ± 1 °C. Control CCRCs were constructed in absence of statins. Then CCRCs were constructed in presence of different concentrations of statins following an incubation period of 1 h. Similarly, curves were constructed in absence and presence of verapamil, a standard calcium channel blocker. The CCRCs were compared for any possible right shift.
Statistical analysis
Effects of test concentrations of statins on isolated rabbits’ jejunal preparations were plotted versus respective concentrations of statins as dose repose curves using Graph Pad Prism. Effects were expressed as % of control maximum for spontaneous as well as KCl-induced contractions. For CCRCs, control curves were drawn in Graph Pad Prism. CCRCs were also drawn in presence of respective statins concentrations. Data were analysed using nonlinear regression (curve fit) method with built in equation for sigmoidal dose response using Graph Pad Prism. Two way ANNOVA was used to determine the significances of concentration versus responses at 95 % CI with P < 0.05.
Results
Effects of statins on spontaneous and KCl-induced contractions are shown in Fig. 1. Effects of simvastatin on spontaneous activity of rabbits’ jejunal preparations and KCl (80 mM) induced contractions are shown in Fig. 1a. Decrease in spontaneous activity is evident on concentration −6.15 Log 10[Simvastatin] M. IC50 value on spontaneous rabbits’ jejunal preparations is −5.08 ± 0.1 Log 10[Simvastatin] M. Relaxant effects of simvastatin was maximum (65 %) of control maximum on concentration −3.4 Log10[Simvastatin] M. Similarly, KCl-induced contractions were relaxed in concentration −5.2 Log 10[Simvastatin]M. Mean IC50 value of simvastatin for KCl induced contraction Log 10[Simvastatin] M was −4.25 ± 0.01 (Table 1). Similarly, atorvastatin effects on spontaneous activity of rabbits’ jejunal preparations and KCl (80 mM) induced contractions are shown in Fig. 1b. Decrease in spontaneous activity was evident on concentration −4.3 Log[Atorvastatin] M. Mean IC50 value on spontaneous rabbit’s jejunal preparations and KCl-induced contractions are −5.19 ± 0.07 Log 10[atorvastatin] M and −4.37 ± 0.09 Log 10[atorvastatin]M. Relaxant effect on KCl induced contractions was maximum (70 %) in concentration −3.3 Log 10[atorvastatin] M.
Fig. 1.
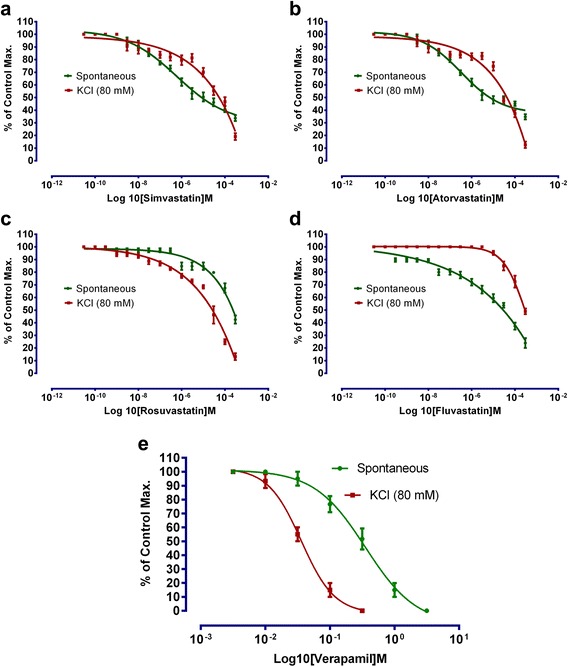
To show the effect of a simvastatin, b atorvastatin, c rosuvastatin, d fluvastatin, and e verapamil on spontaneous and KCl-induced contractions. (Effects is expressed as percent of control maximum, n = 5)
Table 1.
To show the effects of current statins on spontaneous and 80mM KCl-induced contractions in isolated rabbits’ jejunal preparations (n = 5)
| Types of contractions | Mean Log Molar IC50 of statins (Mean ± SD) | ||||
|---|---|---|---|---|---|
| Simvastatin | Atorvastatin | Rosuvastatin | Fluvastatin | Verapamil | |
| Spontaneous contractions | −5.08 ± 0.1 | −5.19 ± 0.07 | −3.62 ± 0.04 | −4.5 ± 0.03 | −0.5 ± 0.01 |
| KCl-induced contractions | −4.25 ± 0.01 | −4.37 ± 0.09 | −4.57 ± 0.06 | −3.52 ± 0.02 | −1.43 ± 0.04 |
Fluvastatin effects on spontaneous activity of rabbits’ jejunal preparations and KCl (80 mM) induced contractions are shown in Fig. 1d with respective mean IC50 values of −3.63 ± 0.04 Log 10[fluvastatin] M and −3.52 ± 0.02. Spasmolytic effect of fluvastatin was maximum on concentration −3.3 Log 10[fluvastatin]M. Rosuvastatin relaxed spontaneous as well as KCl (80 mM) induced contractions with respective mean IC50 (Log 10[rosuvastatin]M) of −3.62 ± 0.04 and −4.57 ± 0.06 Fig. 1c. Decrease in spontaneous activity started in concentration −5.2 Log 10[rosuvastatin]M. Maximum relaxing effects on spontaneous and KCl-induced contractions were respectively 70 and 40 % on −3.39 Log 10[rosuvastatin]M. Verapamil relaxed both spontaneous and KCl-induced contractions with respective IC50 (Log 10[Verapamil]M) values of −0.5 ± 0.01 and −1.43 ± 0.04 (Fig. 1e).
Calcium channel blocking activity on Rabbits’ jejunal preparations
Contractions in smooth muscles occur due to calcium influx. Two types of Ca2+ channel are involved i.e. voltage dependent and receptor-linked Ca2+channels. Intestinal contractions are due to cytosolic free calcium levels which passes through voltage gated calcium channels in sarcoplasmic reticulum [21, 25, 28, 29]. It has been reported that KCl opens the voltage gated calcium channels. Thus an agent which relaxes the KCl-induced contractions is considered to have calcium channel blocking activity. But as reported that positive relaxing effects on KCl-induced contraptions not always follow inhibition of voltage gated calcium channels, hence, construction of calcium concentration response curves will testify with a right shift in the tissues or otherwise [30].
As statins (simvastatin, atorvastatin, fluvastatin and rosuvastatin) in different concentrations showed relaxing properties both on spontaneous and KCl-induced contractions, hence, we constructed CCRCs. Calcium chloride curves in the absence (control) and presence of test samples of simvastatin, atorvastatin, fluvastatin and rosuvastatin are shown in Fig. 2. According to Fig. 2a, IC50 for control curve, in case of simvastatin, is −2.54 ± 0.04 [log (Ca ++) M]. While tissues pre-treated with 4.6 μg/ml of simvastatin, have IC50 = −1.84 ± 0.03 [log (Ca ++) M]. Similarly, IC50 for atorvastatin, control curve is−2.48 ± 0.06 [log (Ca ++) M]. In presence of 23.1 μg/ml of atorvastatin, IC50 = −1.99 ± 0.04 [log (Ca ++) M] (Fig. 2b). IC50 ([log (Ca ++) M]) value for control and in presence of 9.6 μg/ml of fluvastatin are −2.11 ± 0.05 and −1.56 ± 0.03, respectively (Fig. 2c). In presence of rosuvastatin 6.6 μg/ml value of IC50 = −2.17 ± 0.03, while for control IC50 = −2.44 ± 0.03 [log (Ca ++) M] Fig. 2d. IC50 values are shown in Table 2. In case of verapamil, IC50 [log (Ca ++) M] for control curves is −2.45 ± 0.06, while IC50 in presence of verapamil (0.1 μM = 45.46 μg/ml) is −1.69 ± 0.05 [log (Ca ++) M] (Fig. 2e). It is evident from Fig. 2 and Table 2 that all statins produced a right shift in IC50 for CCRCs. The effects of statins are like that of effects of verapamil, a standard calcium channel blocker with a right shift [22, 23, 25].
Fig. 2.
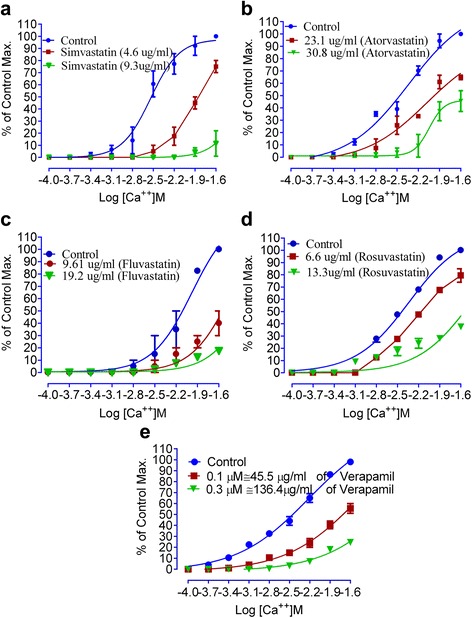
To show the effect of a simvastatin, b atorvastatin, c fluvastatin, d rosuvastatin, and e verapamil on calcium chloride curve compared to that of the respective controls
Table 2.
To represent the IC50 values in absence (control) and presence (test concentrations) of test statins
| Statins | CCRCs specifications | IC50 Log [Ca++]M |
|---|---|---|
| Simvastatin | Control | −2.54 ± 0.04 |
| Test concentration 4.6 μg/ml | −1.84 ± 0.03** | |
| Atorvastatin | Control | −2.48 ± 0.06 |
| Test concentration 23.1 μg/ml | −1.99 ± 0.04** | |
| Test concentration 30.8 μg/ml | −1.68 ± 0.03** | |
| Fluvastatin | Control | −2.11 ± 0.05 |
| Test concentration 9.61 μg/ml | −1.56 ± 0.03** | |
| Rosuvastatin | Control | −2.44 ± 0.03 |
| Test concentration 6.6 μg/ml | −2.17 ± 0.03** | |
| Verapamil | Control | −2.45 ± 0.06 |
| Test concentration 0.1 μM | −1.69 ± 0.05** |
** P < 0.05; test vs respective control
Discussion
The findings of the study prove our assumptions that statins may have inhibitory effects on voltage gated calcium channels. These findings can be interpreted in multiple ways. Like, if statins are used in combination with other calcium channel blockers, especially for management of hypertension in obese who may have hypercholestremia where statins may be advised for management of concomitant hypercholestremia. Then what could be the possible effects like additive or synergistic, is yet to be answered on evidence based practice of medicine. As it has been reported earlier that rhabdomyolysis and myositis occur with use of statins and whereas there are reports of upregulation of L type calcium channels in cell lines, hence, this study further confirms that statins inhibit the voltage gated calcium channels. This requires reassessment for dosimetry of statins, particularly, in clinical environments where combination of statins and calcium channel blockers are prescribed together. More, chances of muscles’ weaknesses or rhabdomyolysis should be reassessed in absence and presence of a calcium channel blockers to prove its clinical relevance. More, the use of statins may also be questioned for clinical conditions where maximum doses of statins are recommended. Thus the findings of the studies suggest that simvastatin and fluvastatin shifted the calcium curves to right in relatively in less amount i.e. 4.6 μg/ml and 9.61 μg/ml respectively. While Rosuvastatin and atorvastatin shifted the curves in presence of 6.6 μg/ml and 23.1 μg/ml respectively. Logically speaking, chances of adverse effects should be less with fluvastatin as it shifted the curves to right in relatively high concentration. Nevertheless, the tested statins follow inhibition of voltage gated calcium channels that warrants for reassessment of its dosimetry particularly in presence of other voltage gated calcium channel blockers like verapamil, diltiazem, amlodipine and nifedipine in true clinical environments. Perhaps, reassessing the doses of statins may be helpful to avoid rhabdomyolysis or myositis that mostly appear in shape of adverse effects of the statins rather than to go for its withdrawal or blaming drugs that are already in the market for a good cause.
Conclusions
Our findings suggest that current statins have relaxant activity on smooth muscles that follow inhibitory effect on voltage gated calcium channels that may explain the possible rationale for gastrointestinal disorders and muscle weakness that is reported with statins.
Acknowledgements
The authors also want to thank the Pharmaceutical Industries for providing the test samples of statins.
Funding
The authors want to thank the Higher Education Commission of Pakistan for providing fund (Grant No:20-1723/R&D/10) for establishing laboratory of Pharmacology at Institute of Basic Medical Sciences at Khyber Medical University, Peshawar.
Availability of data and materials
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
Authors’ contributions
RB carried out experimental work as M.Phil Scholar. Also prepared the 1st draft of manuscript. NA extensively revised the manuscript. He is also designed the study. AK helped experimental work. MN helped in experimental work. MSF helped in experimental work. GS helped in experimental work. SU helped in literature review and preparation of manuscript. WA helped in interpretation and preparing the manuscript. All authors approved the final version of manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical Board of the Khyber Medical University, Peshawar accorded approval of the study protocols via approval No. Dir/KMU/-EB/SE/000138.
Abbreviations
- M
Molar
- Log10[statin] M
Molar concentration of statin expressed as log10
- hrs
Hours
- GIT
Gastrointestinal tract
Contributor Information
Niaz Ali, Phone: +92-91-9217730, Email: niazpharmacist@yahoo.com.
Robina Begum, Email: Robinakmu2013@gmail.com.
Muhammad Saleh Faisal, Email: drsalehfaisal@gmail.com.
Aslam Khan, Email: aslamkhan_mkd@yahoo.com.uk.
Muhammad Nabi, Email: mnabipharmacist@gmail.com.
Gulfam Shehzadi, Email: gulfam.shehzadi@yahoo.com.
Shakir Ullah, Email: shakir_pharmacist@yahoo.com.
Waqar Ali, Email: waqarmohmadzai@yahoo.com.
References
- 1.Parish E, Bloom T, Godlee F. Statins for people at low risk. 2015. [DOI] [PubMed] [Google Scholar]
- 2.Stancu C, Sima A. Statins: mechanism of action and effects. J Cell Mol Med. 2001;5:378–387. doi: 10.1111/j.1582-4934.2001.tb00172.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Glynn RJ, Danielson E, Fonseca FA, Genest J, Gotto AM, Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med. 2009;360:1851–1861. doi: 10.1056/NEJMoa0900241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tobert JA. Lovastatin and beyond: the history of the HMG-CoA reductase inhibitors. Nat Rev Drug Discov. 2003;2:517–526. doi: 10.1038/nrd1112. [DOI] [PubMed] [Google Scholar]
- 5.Lennernäs H, Fager G. Pharmacodynamics and pharmacokinetics of the HMG-CoA reductase inhibitors. Clin Pharmacokinet. 1997;32:403–425. doi: 10.2165/00003088-199732050-00005. [DOI] [PubMed] [Google Scholar]
- 6.Liao JK, Laufs U. Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol. 2005;45:89. doi: 10.1146/annurev.pharmtox.45.120403.095748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grundy SM. HMG-CoA reductase inhibitors for treatment of hypercholesterolemia. N Engl J Med. 1988;319:24–33. doi: 10.1056/NEJM198807073190105. [DOI] [PubMed] [Google Scholar]
- 8.Hunninghake DB. HMG CoA reductase inhibitors. Curr Opin Lipidol. 1992;3:22–28. doi: 10.1097/00041433-199202000-00005. [DOI] [PubMed] [Google Scholar]
- 9.Brown G, Albers JJ, Fisher LD, Schaefer SM, Lin J-T, Kaplan C, Zhao X-Q, Bisson BD, Fitzpatrick VF, Dodge HT. Regression of coronary artery disease as a result of intensive lipid-lowering therapy in men with high levels of apolipoprotein B. N Engl J Med. 1990;323:1289–1298. doi: 10.1056/NEJM199011083231901. [DOI] [PubMed] [Google Scholar]
- 10.Schachter M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: an update. Fundam Clin Pharmacol. 2005;19:117–125. doi: 10.1111/j.1472-8206.2004.00299.x. [DOI] [PubMed] [Google Scholar]
- 11.Rao S, Prasad T, Mohanta G, Manna P. An overview of statins as hypolipidemic drugs. Int J Pharm Sci Drug Res. 2011;3:178–183. [Google Scholar]
- 12.Transon C, Leemann T, Vogt N, Dayer P. In vivo inhibition profile of cytochrome P450TB (CYP2C9) by (±)‐fluvastatin. Clin Pharmacol Ther. 1995;58:412–417. doi: 10.1016/0009-9236(95)90054-3. [DOI] [PubMed] [Google Scholar]
- 13.Golomb BA, Evans MA. Statin adverse effects. Am J Cardiovasc Drugs. 2008;8:373–418. doi: 10.2165/0129784-200808060-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Evans M, Rees A. Effects of HMG-CoA reductase inhibitors on skeletal muscle. Drug Saf. 2002;25:649–663. doi: 10.2165/00002018-200225090-00004. [DOI] [PubMed] [Google Scholar]
- 15.Mlodinow SG, Onysko MK, Vandiver JW, Hunter ML, Mahvan TD. Statin Adverse Effects Sorting out the evidence. J Fam Prac. 2014;497+.Academic OneFile. Web. 7 Sept. 2016. [PubMed]
- 16.Rosenson RS. Current overview of statin-induced myopathy. Am J Med. 2004;116:408–416. doi: 10.1016/j.amjmed.2003.10.033. [DOI] [PubMed] [Google Scholar]
- 17.Greenwood B, Davison J. The relationship between gastrointestinal motility and secretion. Am J Physiol Gastrointest Liver Physiol. 1987;252:G1–G7. doi: 10.1152/ajpgi.1987.252.1.G1. [DOI] [PubMed] [Google Scholar]
- 18.Clunn GF, Sever PS, Hughes AD. Calcium channel regulation in vascular smooth muscle cells: synergistic effects of statins and calcium channel blockers. Int J Cardiol. 2010;139:2–6. doi: 10.1016/j.ijcard.2009.05.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Doyon M, Hale TM, Huot-Marchand J-E, Wu R, de Champlain J. Does atorvastatin induce aortic smooth muscle cell apoptosis in vivo? Vasc Pharmacol. 2011;54:5–12. doi: 10.1016/j.vph.2010.10.001. [DOI] [PubMed] [Google Scholar]
- 20.Corsini A, Mazzotti M, Raiteri M, Soma MR, Gabbiani G, Fumagalli R, Paoletti R. Relationship between mevalonate pathway and arterial myocyte proliferation: in vitro studies with inhibitors of HMG-CoA reductase. Atherosclerosis. 1993;101:117–125. doi: 10.1016/0021-9150(93)90107-6. [DOI] [PubMed] [Google Scholar]
- 21.Gilani AH, Bukhari IA, Khan RA, Khan A, Ullah F, Ahmad VU. Cholinomimetic and calcium channel blocking activities of Carthamus oxycantha. Phytother Res. 2005;19:679–683. doi: 10.1002/ptr.1727. [DOI] [PubMed] [Google Scholar]
- 22.Ali N. Brine shrimp cytotoxicity of crude methanol extract and antispasmodic activity of α-amyrin acetate from Tylophora hirsuta Wall. BMC Complement Altern Med. 2013;13:135. doi: 10.1186/1472-6882-13-135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ali N, Shah SWA, Ahmed G, Shah I, Shoaib M, Junaid M, Ali W. Acute toxicity and antispasmodic activities of Achillea wilhelmsii C. Koch. Pak J Pharm Sci. 2014;27:309–315. [PubMed] [Google Scholar]
- 24.A-u K, Gilani AH. Antispasmodic and bronchodilator activities of Artemisia vulgaris are mediated through dual blockade of muscarinic receptors and calcium influx. J Ethnopharmacol. 2009;126:480–486. doi: 10.1016/j.jep.2009.09.010. [DOI] [PubMed] [Google Scholar]
- 25.Ali N, Shah S, Shah I. Preliminary phytochemical screening and antispasmodic activity of Artemisia macrocephala Jacquem. J Young Pharm. 2011;3:125–128. doi: 10.4103/0975-1483.80300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ali N, Ahmed G, Shah SWA, Shah I, Ghias M, Khan I. Acute toxicity, brine shrimp cytotoxicity and relaxant activity of fruits of callistemon citrinus curtis. BMC Complement Altern Med. 2011;11:99. doi: 10.1186/1472-6882-11-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mazimba O, Majinda RR, Motlhanka D. Antioxidant and antibacterial constituents from Morus nigra. 2011. [Google Scholar]
- 28.Ali N, Shah I, Shah SWA, Ahmed G, Shoaib M, Junaid M, Ali W, Ahmed Z. Antioxidant and relaxant activity of fractions of crude methanol extract and essential oil of Artemisia macrocephala jacquem. BMC Complement Altern Med. 2013;13:96. doi: 10.1186/1472-6882-13-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ali N, Shah SWA, Shah I, Ahmed G, Ghias M, Khan I, Ali W. Anthelmintic and relaxant activities of Verbascum Thapsus Mullein. BMC Complement Altern Med. 2012;12:29. doi: 10.1186/1472-6882-12-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gilani AH, Khan AU, Jabeen Q, Subhan F, Ghafar R. Antispasmodic and blood pressure lowering effects of Valeriana wallichii are mediated through K+ channel activation. J Ethnopharmacol. 2005;100:347–352. doi: 10.1016/j.jep.2005.05.010. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.