

Abstract
Background: Carpal coalition and metacarpal synostosis are uncommon congenital anomalies of the carpus and hand. Methods: A comprehensive review of the literature was performed to help guide surgical and non-surgical treatment of carpal coalition and metacarpal synostosis. Results: The embryology, epidemiology, medical and surgical management, and associated outcomes are detailed. Conclusions: Most patients with these disorders will likely benefit from conservative measures. Surgery should be considered in patients with pain and limitations in wrist and hand function.
Keywords: carpal coalition, synostosis, hand coalitions, congenital, lunotriquetral coalition
Introduction
Congenital carpal coalitions are often found incidentally after radiographic evaluation following trauma. As such, the true incidence of carpal coalitions is unknown, with several case series and reports providing the most current available data. In contrast to isolated congenital carpal coalitions, those occurring in association with syndromes have been well defined and demonstrate a wide array of anatomic variability. The coalition between the lunate and triquetrum has been the best described in the literature secondary to its higher incidence than other coalitions. As most isolated congenital coalitions are asymptomatic, treatment is often not required.
Although congenital carpal coalition is well described as a failure of segmentation, metacarpal synostosis is best described as a failure of differentiation causing a union between 2 adjacent metacarpals. Metacarpal synostosis has been most described between the ring and small fingers and oftentimes is symptomatic.
In an effort to help guide identification and treatment of these rare entities, this article will review relevant classification systems, associated syndromes, and treatment options that have been described in the literature.
Embryology
Embryologically, carpal coalitions arise from a failure of separation of the cartilaginous interzone of adjacent carpal bones. The interzone is made up of 3 layers: 2 denser zones that form the articular cartilage of the 2 bones and a central loose layer that becomes the synovium and intracapsular structures.36,48,53 The extent of coalition between carpal bones is determined by the amount of lack of development of the central zone. Patients with no development of the central zone will have a complete coalition whereas those with incomplete development will have a partial coalition. When describing a partial or incomplete bony union between adjacent carpal bones, many authors prefer the term incomplete coalition.19,36,52 This theory applies specifically to carpal bones in the same row and is not supported in coalitions of the pisiform and hamate. This joint is hypothesized to coalesce due to ossification of the distal portion of the flexor carpi ulnaris or through metaplasia of the pisohamate ligament into bone resulting in synostotic fusion and not true coalition.5,7,8,35,43,49
Unlike carpal coalitions, isolated metacarpal synostosis is thought to be due to a sporadic inheritance pattern causing failure of differentiation between adjacent metacarpals.4,32,56 However, recent data suggest that genetic inheritance may play a larger role than previously thought. With the help from genetic sequencing and splicing, an X-linked recessive inheritance pattern has been described. This pattern involves a nonsense mutation in exon 3 of FGF16 on chromosome Xq21.1.32
Epidemiology
As most patients with congenital carpal coalitions are asymptomatic and found incidentally, the true incidence of congenital carpal coalitions is unknown. The incidence of congenital carpal coalitions in the literature has varied from as low as 0.1% in Caucasians to as high as 8% in certain African tribes.7,20,24,48 The most frequent coalition described is between the lunate and triquetrum, and is twice as common in females then males.20
Metacarpal synostosis is relatively rare with a wide variation in patient presentation.4,16,23,40 As previously mentioned, the fourth and fifth metacarpal is most often affected. The incidence of metacarpal synostosis has ranged in the literature from 0.02% to 0.07%. As many names have been attributed to what has now been described as metacarpal synostosis, this range may not be all-inclusive.4
Classification Systems
Several classification systems have been described in an effort to help guide treatment of these 2 rare congenital anomalies. Case reports describing carpal coalitions date back to as early as 1779, with several subsequent reports following.12,55
DeVilliers Minnaar defined the first carpal coalition classification system in 1952. The Minnaar classification was developed when describing 12 cases of congenital coalition of the lunate and triquetrum of the South African Bantu.12 The classification includes 4 subtypes as described by Minnaar, and has been extended to help describe other carpal coalitions (see Table 1). Although this scheme has been used extensively for both luno-triquetral coalitions, as well as many others, it has several shortcomings. These limitations mainly apply to the identification and classification of associated anomalies.5,28 Specifically, anomalies are often seen with Minnaar types I and II and are not necessarily restricted just to the hand, as they can be seen in the lower extremity.6,28 Furthermore, it does not address the significant variability seen in nonosseous coalitions. To remedy these pitfalls, a classification was proposed by Burnett et al, who describe coalitions as either nonosseous or osseous.5 As incomplete coalitions are often more symptomatic, this classification likely has more clinical significance than the aforementioned system.5,45,48,49,50,58
Table 1.
Minnaar Classification.
| Type I | Incomplete fusion resembling a pseudarthrosis |
| Type II | Fusion with a notch of varying depth |
| Type III | Complete fusion of lunate and triquetrum alone |
| Type IV | Complete fusion associated with other carpal anomalies |
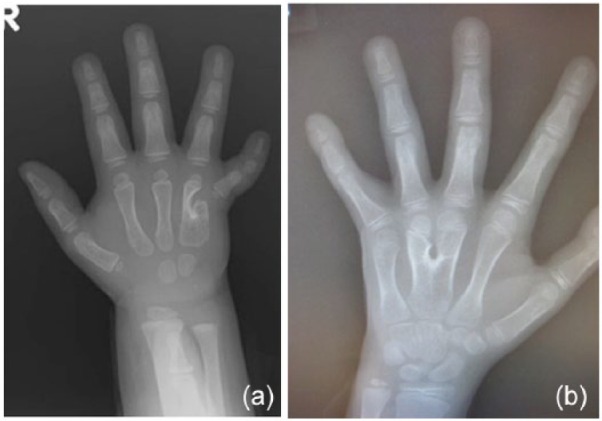
Despite several classifications being described in the literature, none have truly captured the involvement or lack of involvement of associated syndromes. Isolated coalitions without syndrome involvement have been described among the entire carpus and most often only involve 2 bones within the same row (see Figures 1a and 1b).7,20,29,33,36,41,45,47,49-51,58-60 In contrast, syndromic involvement often includes multiple bones in various patterns (see Figure 1c).
Figure 1.

(a) PA radiograph hand depicting a lunate-triquetrum coalition with a very subtle cleft between the 2 bones distally. The trapezium and trapezoid may have a partial coalition as well. (b) PA radiograph demonstrates a capitate-hamate coalition. (c) PA radiograph with multiple carpal coalitions, including capitate-hamate and scaphoid-trapezium.
Note. PA = posteroanterior.
Despite the rare incidence of metacarpal synostosis, several classification systems have been described.4 Buck-Gramcko and Wood described a classification scheme in 1993 (see Table 2).4 The classification uses the length of synostosis to characterize these rare entities in to 3 subsets. This scheme is simple to use; however, it does not offer guidelines for treatment. Thus, Foucher et al developed a different classification scheme in 2001.16 This newer classification uses the shape of the synostosis, degree of metacarpal hypoplasia, deformity of the digits distal to the synostosis, web involvement, and growth direction of the epiphysis.
Table 2.
Buck-Gramcko and Wood4 Classification.
| Type I | Coalition only at the base of the metacarpal |
| Type II | Synostosis extends up to half the length of the metacarpal |
| Type III | Synostosis extends more than half the length of the metacarpal |
Isolated Carpal Coalitions
An isolated complete coalition between the lunate and triquetrum remains the most common coalition described in the literature.10,50 As these coalitions tend to be asymptomatic, they are often discovered incidentally and do not require any treatment. In contrast, incomplete coalitions have recently been proven to be more symptomatic than their complete counterpart.48,52,49,50,58 This has been attributed to the development of a thin layer of articular cartilage, which is prone to degenerative wear and sometimes even fracture.50 In patients with symptomatic incomplete coalitions, lunate and triquetrum fusion provides acceptable results with little wrist dysfunction.52,24,50,58
Most isolated coalitions occur within the same carpal row. However, case reports and series have described coalitions between the hamate and pisiform.8 Although the first case reported was asymptomatic, most subsequent reports have portrayed ulnar-sided symptoms including pain and ulnar nerve paresthesias.2,5,18,35,49 Like incomplete coalitions, the nonosseous coalition that can develop between the hamate and pisiform has been reported to be more symptomatic than its osseous counterpart, especially in regard to ulnar neuropathy.5 Similarly, nonosseous hamate and pisiform coalitions are predisposed to degenerative arthritis and fracture.6,18 Like with many coalitions, nonoperative measures such as immobilization should be tried first. Should conservative measures fail, excision of the pisiform and the underlying coalition should be entertained.5,35,49
Metacarpal Synostosis
Isolated metacarpal synostosis can also be partial or complete. Typically, the synostosis is located between the ring and little finger metacarpals, but has also been described between the middle and ring fingers (see Figures 2a and 2b).4,23,27 This condition can be disabling because the affected finger is held in abduction. The abduction deformity limits finger motion and can cause the digit to catch on pockets. Should the deformity occur between the middle and ring, grasping objects becomes difficult, as they often will fall through the abduction deformity.4,23,27 To quantify the abduction deformity, the senior author attempted to describe the extent of deformity using standard posteroanterior (PA) radiographs of the hand with the affected finger in maximum adduction.23 When the deformity is between the ring and small fingers, the middle finger is used as a reference point. If the middle and ring fingers are affected, the angle between the proximal phalanges is used.23
Figure 2.
(a) PA radiograph of the hand with a metacarpal synostosis between the ring and small metacarpals. Note the abduction of the small finger. (b) PA radiograph with the metacarpal synostosis between the middle and ring finger metacarpals.
Note. PA = posteroanterior.
Because of the variability in metacarpal synostoses, treatment can vary substantially. However, most surgical techniques involve splitting the synostosis and then filling the newly created space with a spacer to separate the metacarpals.4,16,23,27,40 The senior author’s preferred filler is coralline hydroxyapatite (Interpore, Biomet, Parsippany, New Jersey).23 It is important to place the graft proximal to the growth plates to avoid growth arrest. This technique corrects the abduction deformity but does not take in to account the hypoplastic deformity of the fingers.23 As such, some impairment in motion and function will remain. Surgery should be considered on a case-by-case basis, as not all synostoses are amenable to separation with spacer placement.
Associated Syndromes
Several syndromes have been identified that are associated with carpal coalitions. These syndromes include arthrogryposis, diastrophic dwarfism, dyschondrosteosis, Ellis-van Creveld syndrome, fetal alcohol syndrome, hand-foot-genital syndrome, Holt-Oram syndrome, Nievergelt’s syndrome, oto-palato-digital (OPD) syndrome, symphalangism, and Turner syndrome. Syndromic coalitions often cross carpal rows, involve multiple carpal bones, and are seen with other anatomic anomalies both within the appendicular skeleton and other organ systems.10,47,52 Although syndromic coalitions are more involved, few, if any, require surgical intervention.
Arthrogryposis Multiplex Congenita
Arthrogryposis is a constellation of clinical findings with the most notable being multiple congenital contractures of differing body areas.1,34 The incidence of arthrogryposis is approximately 1 in every 3000 live births and is thought to be due to a limitation of motion in utero.3 The exact mechanism for this is unknown although some have attributed it to antibodies inhibiting fetal acetylcholine receptors.
Patients with arthrogryposis and upper extremity abnormalities will present with a rigid deformity of the wrist and hand. The deformity is often a flexed and ulnarly deviated hand, which routinely fails to respond well to conservative measures.14
Carpal coalitions occur frequently in arthrogryposis and have substantial variability. The proximal row is more commonly involved early and then is often followed by intercarpal involvement. Authors have theorized this pattern of involvement as being acquired instead of congenital. Given the extensive nature of the coalitions, the midcarpal joint is often eliminated.14 This can often be attributed to a coalition between the scaphoid and capitate. A coalition of these two carpal bones complicates the traditional surgical treatment of a proximal row carpectomy. Instead, previous authors have recommended a biplanar osteotomy to correct the flexion and ulnar deviation of the carpus prior to the toddler age reaching 5 years of age.14
Diastrophic Dwarfism
Diastrophic dwarfism is an autosomal recessive form of short-limbed dwarfism. The common mutation involves the sulfate transporter protein found on chromosome 5 and is more common in patients of Finnish decent. Similar to arthrogryposis, it has been hypothesized that carpal coalitions associated with this syndrome may be acquired instead of truly congenital. This is in part due to the higher incidence of coalitions, as patients get older. The radiographic appearances of carpal bones appear deformed and more mature than their normal counterparts.47 Management depends on the symptoms and expectations of the patient and their parents.
Dyschondrosteosis
Dyschondrosteosis is a rare inherited mesomelic dwarfism associated with bilateral Madelung deformities. Patients may also have associated variable carpal coalitions with limited forearm and wrist motion. Treatment options are often tailored toward the wrist deformity if symptomatic.
Ellis-van Creveld
Ellis-van Creveld syndrome is a rare autosomal recessive disorder with genetic defects in the EVC1 and EVC2 gene on chromosome 4p16.42,46 The syndrome is often referred to as chondro-ectodermal dysplasia. Characteristic features include short limb dwarfism and in over half of cases congenital heart defects. Other defects often include skin, teeth, hair, and nails.13,17,42,46,47 The incidence of the syndrome is 1 in 60 000 live births and affects boys and girls equally. Hand and wrist findings may include but are not limited to capito-hamate coalition, postaxial polydactyly, metacarpal synostosis, and clinodactyly.13 Although the patient may have significant carpus and hand involvement, treatment is often not necessary for the carpal coalition.
Fetal Alcohol Syndrome
Fetal alcohol syndrome has been recognized in children of mothers using alcohol during their pregnancy. Several consistent malformations have been described including those affecting the upper extremity. These can include radio-ulnar synostoses and capito-hamate coalitions either unilateral or bilaterally.31 Treatment is often conservative and based on symptoms.
Hand-Foot-Genital Syndrome
Hand-foot-genital syndrome is an autosomal dominant inherited syndrome characterized by hand and foot deformities with associated urogenital defects.54 Hand and wrist manifestations include hypoplastic hypothenar eminence, limited thumb opposition attributed to limited flexion, and carpal coalitions. Coalitions have been described between the scaphoid and trapezium.22,25,30,54
Holt-Oram Syndrome
Holt-Oram syndrome is an autosomal dominant inherited syndrome that affects the upper extremities and the heart. Patients with Holt-Oram syndrome will likely have an absent radius, atrial septal defect, and an abnormally shaped scaphoid with associated carpal coalitions.47 Some authors have reported a narrowing of the scaphoid and trapezium joint space with accessory carpal bones.47
Nievergelt’s Syndrome
Nievergelt’s syndrome is a rare form of mesomelic dwarfism. Although it often has an autosomal dominant inheritance, sporadic inheritance has also been documented. Classic features include limited motion of the elbow and forearm with associated carpal coalitions44: Similar manifestations may also be seen in the feet including clubfeet and metatarsal synostosis.44
OPD syndrome
OPD syndrome is a constellation of abnormalities affecting the ears, palate, and skeleton. The defining skeletal dysplasia affects the hands and feet predominantly. Carpal bones may demonstrate a deformed appearance.38,47 Although not specific for OPD, authors have described the trapezoid taking a comma-like shape with an associated transverse-oriented capitate. The scaphoid may also be involved but as with other syndromes, carpal coalitions may be highly variable.38,47
Symphalangism
Symphalangism is an autosomal dominant inherited disorder described as having interphalangeal joint fusions with associated carpal coalitions.9,21,39,57 Symphalangism is often referred to as either proximal or distal, which refers to the distal or proximal interphalangeal joint. The proximal form is more common. Three forms have been described in the literature: Type 1 refers to true symphalangism without additional skeletal abnormalities, type 2 refers to symphalangism associated with symbrachydactyly, and type 3 refers to symphalangism with syndactyly.15 Fingers are often affected from an ulnar to radial pattern with the small finger being the most commonly affected.11,15,39
Other additional upper extremity deformities have been associated with symphalangism and include brachydactyly, camptodactyly, clinodactyly, syndactyly, and radiohumeral fusions. Several carpal coalitions have also been described and include the triquetrum-hamate (most common), capito-hamate, capitate-trapezium, triquetrum-lunate, and scaphoid-trapezium.39,57
Patients often will present with the inability to move their proximal or distal interphalangeal joints with no visible joint creases. Radiographs will often demonstrate the absence of interphalangeal joints (skeletally immature patients may have a pseudo-joint with a cartilaginous bridge that has yet to ossify). Although patients lack interphalangeal joints, hand function is often unimpaired requiring little to no treatment.21,26,47
Turner Syndrome
Turner syndrome is a chromosomal disorder marked by a single X chromosome. The disorder is manifested across multiple systems but also typically affects the carpus. Previously, authors have described the typical anomaly seen in Turner syndrome as having deformed proximal carpal bones with a coarse trabecular pattern.37 Others have described associated Madelung’s deformity with a lunate-triquetrum coalition, but this is not specific to Turner syndrome.
Conclusion
Carpal coalitions and metacarpal synostosis represent rare congenital anomalies seen in both isolation and with associated syndromes. Both disorders represent a spectrum ranging from complete to incomplete coalitions/synostosis. Although most patients with these disorders will likely benefit from conservative measures, surgery should be considered in patients presenting with pain and limitations in wrist and hand function.
Footnotes
Ethical Approval: Permission has been granted to use photos and radiographs of specific patients.
Statement of Human and Animal Rights: This article does not contain any studies with human or animal subjects.
Statement of Informed Consent: All personal and identifying information for radiographs presented in this article have been removed.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Bamshad M, Van Heest AE, Pleasure D. Arthrogryposis: a review and update. J Bone Joint Surg Am. 2009;91(suppl 4):40-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Berkowitz AR, Melone CP, Jr, Belsky MR. Pisiform-hamate coalition with ulnar neuropathy. J Hand Surg. 1992;17(4):657-662. [DOI] [PubMed] [Google Scholar]
- 3. Bevan WP, Hall JG, Bamshad M, Staheli LT, Jaffe KM, Song K. Arthrogryposis multiplex congenita (amyoplasia): an orthopaedic perspective. J Pediatr Orthop. 2007;27(5):594-600. [DOI] [PubMed] [Google Scholar]
- 4. Buck-Gramcko D, Wood VE. The treatment of metacarpal synostosis. J Hand Surg. 1993;18(4):565-581. [DOI] [PubMed] [Google Scholar]
- 5. Burnett SE. Hamate-pisiform coalition: morphology, clinical significance, and a simplified classification scheme for carpal coalition. Clin Anat. 2011;24(2):188-196. [DOI] [PubMed] [Google Scholar]
- 6. Carlson DH. Coalition of the carpal bones. Skeletal Radiol. 1981;7(2):125-127. [DOI] [PubMed] [Google Scholar]
- 7. Cockshott WP. Carpal fusions. Am J Roentgenol Radium Ther Nucl Med. 1963;89:1260-1271. [PubMed] [Google Scholar]
- 8. Cockshott WP. Pisiform hamate fusion. J Bone Joint Surg Am. 1969;51(4):778-780. [PubMed] [Google Scholar]
- 9. Cushing H. Hereditary anchylosis of the proximal phalan-geal joints (symphalangism). Genetics. 1916;1(1):90-106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Delaney TJ, Eswar S. Carpal coalitions. J Hand Surg. 1992;17(1):28-31. [DOI] [PubMed] [Google Scholar]
- 11. Dellon AL, Gaylor R. Bilateral symphalangism of the index finger. A case report. J Bone Joint Surg Am. 1976;58(2):270-271. [PubMed] [Google Scholar]
- 12. Devilliers Minnaar AB. Congenital fusion of the lunate and triquetral bones in the South African Bantu. J Bone Joint Surg Br. 1952;34-B(1):45-48. [DOI] [PubMed] [Google Scholar]
- 13. Ellis RW, van Creveld S. A syndrome characterized by ectodermal dysplasia, polydactyly, chondro-dysplasia and congenital morbus cordis: report of three cases. Arch Dis Child. 1940;15(82):65-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ezaki M, Carter PR. Carpal wedge osteotomy for the arthrogrypotic wrist. Tech Hand Up Extrem Surg. 2004;8(4):224-228. [DOI] [PubMed] [Google Scholar]
- 15. Flatt AE, Wood VE. Rigid digits or symphalangism. The Hand. 1975;7(3):197-214. [DOI] [PubMed] [Google Scholar]
- 16. Foucher G, Navarro R, Medina J, Khouri RK. Metacarpal synostosis: a simple classification and a new treatment technique. Plast Reconstr Surg. 2001;108(5):1225-1231; discussion 1232-1224. [DOI] [PubMed] [Google Scholar]
- 17. Galdzicka M, Patnala S, Hirshman MG, et al. A new gene, EVC2, is mutated in Ellis-van Creveld syndrome. Mol Genet Metab. 2002;77(4):291-295. [DOI] [PubMed] [Google Scholar]
- 18. Ganos DL, Imbriglia JE. Symptomatic congenital coalition of the pisiform and hamate. J Hand Surg. 1991;16(4):646-650. [DOI] [PubMed] [Google Scholar]
- 19. Garn SM, Burdi AR, Babler WJ. Prenatal origins of carpal fusions. Am J Phys Anthropol. 1976;45(2):203-208. [DOI] [PubMed] [Google Scholar]
- 20. Garn SM, Frisancho AR, Poznanski AK, Schweitzer J, McCann MB. Analysis of triquetral-lunate fusion. Am J Phys Anthropol. 1971;34(3):431-433. [DOI] [PubMed] [Google Scholar]
- 21. Geelhoed GW, Neel JV, Davidson RT. Symphalangism and tarsal coalitions: a hereditary syndrome. A report on two families. J Bone Joint Surg Br. 1969;51(2):278-289. [PubMed] [Google Scholar]
- 22. Goodman FR, Bacchelli C, Brady AF, et al. Novel HOXA13 mutations and the phenotypic spectrum of hand-foot-genital syndrome. Am J Hum Genet. 2000;67(1):197-202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Gottschalk HP, Bednar MS, Moor M, Light TR. Metacarpal synostosis: treatment with a longitudinal osteotomy and bone graft substitute interposition. J Hand Surg. 2012;37(10):2074-2081. [DOI] [PubMed] [Google Scholar]
- 24. Gross SC, Watson HK, Strickland JW, Palmer AK, Brenner LH, Fatti J. Triquetral-lunate arthritis secondary to synostosis. J Hand Surg. 1989;14(1):95-102. [DOI] [PubMed] [Google Scholar]
- 25. Halal F. The hand-foot-genital (hand-foot-uterus) syndrome: family report and update. Am J Med Genet. 1988;30(3):793-803. [DOI] [PubMed] [Google Scholar]
- 26. Harle TS, Stevenson JR. Hereditary symphalangism associated with carpal and tarsal fusions. Radiology. 1967;89(1):91-94. [DOI] [PubMed] [Google Scholar]
- 27. Horii E, Miura T, Nakamura R, Nakao E, Kato H. Surgical treatment of congenital metacarpal synostosis of the ring and little fingers. J Hand Surg Br. 1998;23(5):691-694. [DOI] [PubMed] [Google Scholar]
- 28. Hughes PC, Tanner JM. The development of carpal bone fusion as seen in serial radiographs. Br J Radiol. 1966;39(468):943-949. [DOI] [PubMed] [Google Scholar]
- 29. Ingram C, Hall RF, Gonzalez M. Congenital fusion of the scaphoid, trapezium, trapezoid and capitate. J Hand Surg Br. 1997;22(2):167-168. [DOI] [PubMed] [Google Scholar]
- 30. Innis JW. Hand-foot-genital syndrome. In: Pagon RA, Adam MP, Ardinger HH, et al., eds. GeneReviews(R). Seattle, WA; 1993. PMID:20301596[PubMed]. [PubMed] [Google Scholar]
- 31. Jaffer Z, Nelson M, Beighton P. Bone fusion in the foetal alcohol syndrome. J Bone Joint Surg Br. 1981;63B(4):569-571. [DOI] [PubMed] [Google Scholar]
- 32. Jamsheer A, Zemojtel T, Kolanczyk M, et al. Whole exome sequencing identifies FGF16 nonsense mutations as the cause of X-linked recessive metacarpal 4/5 fusion. J Med Genet. 2013;50(9):579-584. [DOI] [PubMed] [Google Scholar]
- 33. Kahane S, Isaac SM, Wildin C. A new type of carpal coalition. J Hand Surg Eur Vol. 2012;37(6):581-582. [DOI] [PubMed] [Google Scholar]
- 34. Kalampokas E, Kalampokas T, Sofoudis C, Deligeoroglou E, Botsis D. Diagnosing arthrogryposis multiplex congenita: a review. ISRN Obstet Gynecol. 2012;2012:264918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Kawamura K, Yajima H, Takakura Y. Pisiform and hamate coalition: case report and review of literature. Hand Surg. 2005;10(1):101-104. [DOI] [PubMed] [Google Scholar]
- 36. Kennedy K, Waller CJ, Hartley RH. Congenital lunotriquetral and capitotrapezoid coalitions. J Hand Surg Eur Vol. 2010;35(1):79-80. [DOI] [PubMed] [Google Scholar]
- 37. Kosowicz J. The roentgen appearance of the hand and wrist in gonadal dysgenesis. Am J Roentgenol Radium Ther Nucl Med. 1965;93:354-361. [PubMed] [Google Scholar]
- 38. Langer LO., Jr. The roentgenographic features of the oto-palato-digital (OPD) syndrome. Am J Roentgenol Radium Ther Nucl Med. 1967;100(1):63-70. [DOI] [PubMed] [Google Scholar]
- 39. Letts M, Davidson D, Beaule P. Symphalangism in children: case report and review of the literature. Clin Orthop Relat Res. 1999(366):178-185. [PubMed] [Google Scholar]
- 40. Miura T. Congenital synostosis between the fourth and fifth metacarpal bones. J Hand Surg. 1988;13(1):83-88. [DOI] [PubMed] [Google Scholar]
- 41. Moreel P, Wilson SM, Descamps S, Roulot E. [Bilateral congenital fusion of the scaphoid and the trapezium. A case report]. Rev Chir Orthop Reparatrice Appar Mot. 2008;94(1):84-86. [DOI] [PubMed] [Google Scholar]
- 42. Muensterer OJ, Berdon W, McManus C, et al. Ellis-van Creveld syndrome: its history. Pediatr Radiol. 2013;43(8):1030-1036. [DOI] [PubMed] [Google Scholar]
- 43. O’Rahilly R. A survey of carpal and tarsal anomalies. J Bone Joint Surg Am. 1953;35-A(3):626-642. [PubMed] [Google Scholar]
- 44. Pearlman HS, Edkin RE, Warren RF. Familial tarsal and carpal synostosis with radial-head subluxation (Nievergelt’s syndrome). J Bone Joint Surg Am. 1964;46:585-592. [PubMed] [Google Scholar]
- 45. Peters S, Colaris JW. Carpal coalition: symptomatic incomplete bony coalition of the capitate and trapezoid—case report. J Hand Surg. 2011;36(8):1313-1315. [DOI] [PubMed] [Google Scholar]
- 46. Polymeropoulos MH, Ide SE, Wright M, et al. The gene for the Ellis-van Creveld syndrome is located on chromosome 4p16. Genomics. 1996;35(1):1-5. [DOI] [PubMed] [Google Scholar]
- 47. Poznanski AK, Holt JF. The carpals in congenital malformation syndromes. Am J Roentgenol Radium Ther Nucl Med. 1971;112(3):443-459. [DOI] [PubMed] [Google Scholar]
- 48. Resnik CS, Grizzard JD, Simmons BP, Yaghmai I. Incomplete carpal coalition. AJR Am J Roentgenol. 1986;147(2):301-304. [DOI] [PubMed] [Google Scholar]
- 49. Richterman IE, Kozin SH. Symptomatic pisiform hamate synchondrosis: a case report and review of the literature. J Hand Surg. 1996;21(2):311-313. [DOI] [PubMed] [Google Scholar]
- 50. Ritt MJ, Maas M, Bos KE. Minnaar type 1 symptomatic lunotriquetral coalition: a report of nine patients. J Hand Surg. 2001;26(2):261-270. [DOI] [PubMed] [Google Scholar]
- 51. Samir N, Al-Mahrezi A. Congenital fusion of the trapezium and trapezoid. Sultan Qaboos Univ Med J. 2010;10(3):405-406. [PMC free article] [PubMed] [Google Scholar]
- 52. Simmons BP, McKenzie WD. Symptomatic carpal coalition. J Hand Surg. 1985;10(2):190-193. [DOI] [PubMed] [Google Scholar]
- 53. Sledge CB. Some morphologic and experimental aspects of limb development. Clin Orthop Relat Res. 1966;44:241-264. [PubMed] [Google Scholar]
- 54. Stern AM, Gall JC Jr, Perry BL, Stimson CW, Weitkamp LR, Poznanski AK. The hand-food-uterus syndrome: a new hereditary disorder characterized by hand and foot dysplasia, dermatoglyphic abnormalities, and partial duplication of the female genital tract. J Pediatr. 1970;77(1):109-116. [DOI] [PubMed] [Google Scholar]
- 55. Szaboky GT, Muller J, Melnick J, Tamburro R. Anomalous fusion between the lunate and triquetrum. J Bone Joint Surg Am. 1969;51(5):1001-1004. [PubMed] [Google Scholar]
- 56. Temtamy SA, McKusick VA. The genetics of hand malformations. Birth Defects Orig Artic Ser. 1978;14(3):i-xviii, 1-619. [PubMed] [Google Scholar]
- 57. Tuncay I, Akpinar F, Tosun N. Congenital true complete symphalangism of all proximal interphalangeal joints of hands with carpal anomalies: a case report. Hand Surg. 2001;6(2):223-226. [DOI] [PubMed] [Google Scholar]
- 58. van Schoonhoven J, Prommersberger KJ, Schmitt R. Traumatic disruption of a fibrocartilage lunate-triquetral coalition—a case report and review of the literature. Hand Surg. 2001;6(1):103-108. [DOI] [PubMed] [Google Scholar]
- 59. Wilson SM, Moreel P, Roulot E. Symptomatic congenital fusion of the scaphoid and the trapezium. J Hand Surg Br. 2006;31(5):581. [DOI] [PubMed] [Google Scholar]
- 60. Weinzweig J, Watson HK, Herbert TJ, Shaer JA. Congenital synchondrosis of the scaphotrapezio-trapezoidal joint. J Hand Surg. 1997;22(1):74-77. [DOI] [PubMed] [Google Scholar]