

Abstract
Background
A follow-up study on a cohort of stroke patients through a postal survey questionnaire 3 and 12 months after discharge from hospital was performed. The response rate at 3-months follow-up was lower than desired, and pre-contact by phone as a measure for increasing the response rate at 12 months was studied.
Methods
The study design was a randomized controlled trial on a cohort of 3 months follow-up-non-responders where the intervention group was pre-contacted with an aim to obtain an informal ’consent to receive’ the questionnaire before the 12-months survey was mailed, and the control group was not.
The primary outcome was 45 days response rate; secondary outcome was 365 days response rate. The main analysis followed the intention to treat principle. A secondary, per-protocol analysis (i.e. subjects who were not reached by phone were reassigned to the control group) is included. Also included is a rudimentary cost-utility analysis, where we estimated the cost per additional response.
Results
Of the 235 subjects, 116 were randomized to the intervention group and 119 to the control group. 10 were excluded due to death (7 in the IG and 3 in the CG), 6 due to dementia (3 in the IG and 3 in the CG), and 2 (1 in the IG and 1 in the CG) for other reasons. The primary outcome was a response rate of 42.9 % in the intervention group, and 26.8 % in the control group, giving p =0.014, with estimated OR of 2.04 (95 % CI [1.16,3.64]). The secondary outcome had p =0.009 with OR 2.10 (95 % CI [1.20,3.70]). The as-per-protocol analyses gave stronger results with p =0.001 and p =0.003, respectively. The cost-utility analysis gave a time cost of 1 working hour per additional response.
Conclusions
The results are in line with previous research, and show that pre-contact has a positive effect on response rate also for a population of elderly with reduced health. Given the importance of high response rate in surveys, a cost of 1 working hour per additional response is likely to be worth while.
Trial registration
Registration with ISRCTN initiated on 05/21/2013 and finalised on 06/30/2014 with http://www.isrctn.com/ISRCTN31304930. Following the prospective submission in May 2013, there were no subsequent changes to the protocol. The recruitment started on 01/06/13, after initiation of public registration.
Keywords: Response rates, Postal survey, Questionnaires, Randomized controlled trial, Pre-contact, Stroke patients
Background
Collecting patient data
Certain kind of patient data relevant to health care researchers can only be harvested from the patients themselves, e.g. health related quality of life or treatment satisfaction. While non-subjective patient data, e.g. number of visits with a GP or hours of home care per week received, may be possible to obtain from other sources in theory, postal or electronic survey questionnaires often stand out as the cost-effective alternative ([1], p. 2). Once a survey questionnaire design is chosen, researchers should – subject to their available resources – undertake to maximize the response rate (RR). Low RR’s obviously decrease the statistical power of the final data set, increasing type II errors. Worse yet; if propensity for (non-)responding correlates with any of the collected variables, subsequent analysis will usually be biased, which increases the risk of Type I errors. This problem is particularly acute if an outcome variable is causally linked to response propensity. There is substantial evidence that responders and non-responders differs with respect to a range of characteristics; see e.g. [2] for an introduction and further references.
NORSPOT – the context of the RCT
NORSPOT (Norwegian Stroke – Paths of Treatment) is an established cohort consisting of all patients admitted to the Stroke Unit (SU) of Akerhus University Hospital (Ahus) during the period February 15th 2012 to March 15th 2013. Ahus is situated in the Oslo greater metropolitan area, and is Norway’s largest acute hospital with a catchment area counting circa 500.000 inhabitants (≃10 % of Norway’s population). The project’s charter is to map out stroke patients’ treatment paths through the health services, and to estimate current epidemiological data, with an aim to inform policy makers about future needs within the various parts of the Norwegian health care system. To this end, in addition to data collected during hospitalization, NORSPOT seeks to elicit information about the patients’ levels of, contentment with, and benefit from, consumption of health services over the year following hospitalization. Postal survey questionnaires were therefore sent to the patients’ home address at 3 and 12 months after the time of discharge from the SU. The data set contains 1144 unique patients with a stroke diagnosis. The project recorded data on circa 1900 admissions to the SU. There were several patients with multiple stays, and about two thirds of all patients admitted to the SU received a final stroke diagnosis. Here, the stroke diagnoses are classified into intra-cranial haemorrhages (ICD10 61.X), cerebral infarctions (ICD10 63.X) and transient ischemic attacks (ICD10 45.X excluding 45.4). Patient’s with other diagnoses were not included in the follow-up questionnaire study. During the 3 month survey questionnaire phase, we observed that the response rates were converging towards the lower end of the acceptable range (≃50 %), and we were worried that further loss-to-follow-up during the 12 month questionnaire phase could weaken our study.
We therefore searched the literature on increasing response rates to postal questionnaires to see if there were any easy and efficient steps which could be implemented to maintain – or even improve – the state of affairs.
Review of literature on increasing response rates by pre-contact
A Cochrane review from 2010 [1] identified and analysed 481 papers investigating different strategies to increase response rates to postal questionnaire surveys. We noted that amongst the diverse approaches shown to have a positive effect on response rates, many were already implemented (e.g. handwritten address, university hospital envelope), while other approaches were either considered unethical according to local ethical considerations (pecuniary incentives) or incompatible with our study (short questionnaire, non-sensitive questions).
One intervention singled itself out: pre-contact. Pre-contact here means that the prospective respondents are contacted prior to having the questionnaire mailed to them. The Cochrane report reviewed various studies: pre-contact by mail (e.g. a postcard one week prior to the actual questionnaire) or pre-contact by telephone (i.e. calling the respondents prior to sending them the questionnaire). In addition, some comparisons of these two forms of pre-contact was reported on.
The strategy of pre-contact by telephone was both feasible to implement – at least partially – on NORSPOT’s budget, and ethical approval for the intervention had been obtained already; indeed pre-contact was already implemented for the most frail patients (e.g. above 80 years of age, or discharged to a health care institution) in our cohort. However, resources would not permit pre-contacting all patients. Also, a closer scrutiny of the Cochrane review revealed that despite a highly significant (p<0.001) moderate pooled odds ratio (OR = 1.45) in favour of pre-contact, heterogeneity of study populations, reported odds ratios, and types of questionnaires in the studies included in the meta analysis was substantial.
Of the 45 papers reporting on pre-contact vs. no pre-contact on final response rates, we found very few studies targeting a population similar to our population of elderly patients. The studies were rated from A to C according to Cochrane’s standard quality assessment grading scheme ([1], p. 3). Only 5 studies were A-rated. Furthermore, the review contained information about the various studies’ target groups, and the nature of the surveys. Only 15 of the 45 papers included in [1] had a health perspective; only 8 of these targeted patients. Of the 15 health related studies, there were 6 investigating pre-contact by phone, and 9 investigating pre-contact by mail. Restricting ourselves to A- or B-rated patient-targeted pre-notification by telephone, there were one B-rated study [3] which found found a positive effect (OR = 2.58 [1.50,4.44]) of pre-contact by telephone on response rates, and one A-rated study [4] which found a positive effect (OR = 1.27 [1.00,1.63]). However, the target populations were young and mid-life women; rather dissimilar to our senescent stroke patients.
From our health services researcher’s perspective we concluded that even though the pooled data from [1] yielded a statistically significant and positive effect of pre-contact, we were unsure if it would be efficient with a fairly comprehensive questionnaire eliciting sensitive information in a population like ours. We therefore decided to undertake a randomized controlled trial (RCT), with the aim of establishing whether pre-contact by telephone increases response rates to postal questionnaires in a frail and senescent patient population.
Methods
RCT
The RCT was prospectively registered with Current Controlled Trials [5] on May 25th 2013 with International Standard RCT Number http://www.isrctn.com/ISRCTN31304930. The study was conducted between June 1st 2013 and April 1st 2014. The RCT was designed as an interventional open randomized controlled trial with two study branches – one intervention group (IG) and one control group (CG) – and main outcome was performed with a two-sided test for equality of proportion (significance level of α=0.05), analysed as per intention-to-treat (ITT). Main outcome was response rate after 45 days; secondary outcome was response rate after 365 days.
Inclusion
All patients discharged from the SU with a stroke diagnosis between May 15th 2012 and April 1st 2013, who:
had not previously been pre-contacted;
had not returned the 3-month questionnaire, or, had not received them;
were not pre-selected for care-giver contact, i.e. were either above 80 years of age or were discharged to other than home address with primary care-giver at other address than themselves;
were registered with a phone number for contact.
With regard to items 1. and 3. recall that the RCT was carried out in conjunction with the second round of survey questionnaires mailed to this population. We had already defined a protocol for pre-contacting the primary caregivers of the most frail patients. As these most frail patients were also to be pre-contacted prior to mailing the 12 month questionnaire, they were not eligible for inclusion into the RCT. Item 2. was included in the protocol because we expected that the effect of the intervention would be stronger amongst those patients who were known non-responders at the 3 month follow-up (This inclusion criterion has also been employed in a B-rated study by Ogborn et. al. [6], in which they reported an OR of 1.86 in favour of pre-contact in a non-responder population).
Mailing of questionnaires and intervention
All patients in the study received an envelope with hand-written address in the name of the patient, and, where available, also the name of the spouse. The envelope contained two questionnaires and a cover letter explaining the purpose of the study, ensuring confidentiality, and equipped with contact information for the second author (TBS) in case the recipient had any queries. The cover letter was hand-signed by TBS. The two questionnaires were made out for the patient and for a care giver; such as a spouse, a child, or another close relative or friend. The questionnaires had 16 (patient) and 8 (care giver) pages, and contained questions about history of contacts with various parts of the health care system, self reported general and mental health (modified Rankin scale, EQ-5D, HADS, Barthel ADL), knowledge about stroke, satisfaction with municipal services, and help received from/provided by care-givers. The questionnaires were estimated to take 30–60 minutes to complete. The shipment also contained two stamped and addressed return envelopes; one for the patient’s questionnaire and one for the care giver’s questionnaire. Prior to mailing the questionnaire, the status of the patient was verified with the electronic patient journal system of the hospital; i.e. whether the patient was still alive, had had a change of address or were currently admitted to hospital.
The above describes the standard protocol for the NORSPOT project.
Those who were randomized into the IG were pre-contacted by TBS according to the following protocol:
Three attempts were made at contracting the subjects at their mobile telephone number (or land-line when no mobile telephone number was available).
If contact was established during one of these three attempts, or on a call-back, we aimed at achieving what we refer to as an informal consent to shipping [of the questionnaire]. This means that the caller will aim not at obtaining consent to use the collected data for research (this could be submitted on the back of the questionnaire), nor to persuade or obtain a promise of return, but only to have the participant agreeing to having the questionnaire shipped for their review.
The caller answered questions about the survey, but remained neutral towards anything but the aim: obtain the consent to shipment.
Any house-hold member [in particular when a land-line was used] could act as proxy for the participant, e.g. a spouse or other family member answering the phone.
Whenever a participant/proxy was unwilling to grant the informal consent to shipping the participant would not have a questionnaire mailed to their address. Such participants were logged with REFUSED.
Where a prior written consent to participation (given at the SU) existed, the caller could remind the participant of this fact. However, the caller were required to take all possible measures not to induce guilt for not having responded to the 3-month shipment.
Note that the above protocol for pre-contact was already de facto established, but then aimed primarily at care givers; see item 3. in the Inclusion-section.
Randomization and analyses
Each participant was assigned an internal identification number. A list of the participants identification numbers were sent to a statistician external to the project (see Acknowledgements) who generated the CG and the IG by random allocation. This was performed in two rounds: first in June 2013, and consecutively a second batch of non-responders from the three-month round were included and randomized to the CG and IG in September 2013.
The main analysis of the effect of the pre-contact intervention on response rates is performed according to the principle of intention to treat for both the primary and the outcomes. This means that the response rates calculated for the IG include those who could not be reached by telephone and patients who refused to have a questionnaire sent to them when contacted. This means that also subjects whom we tried, but were not able to, contact are recorded as in the intervention group in the main analysis. However, RCT-participants who were discovered to be either dead, terminal or diagnosed with dementia were excluded at the time of the status check which was routinely performed for all NORSPOT participants.
The primary outcome is defined as response within 45 days from the day when the questionnaire was mailed; the secondary outcome is defined as response within 365 days. Experience from the 3 month questionnaires showed that no participants had responded later than 3 months after receiving the questionnaires. The secondary outcome would therefore very likely be the absolute response rate, and would reveal it if a speed-up effect masqueraded as a true increase in final response rates. Also, for some types of surveys, the timing of the information is paramount, and old information is worthless. Therefore both outcomes can be relevant in different situations.
Return date was defined as the date written by the respondent on the questionnaire. This definition was chosen because the company handling the return of the questionnaires delivered them in batches of 10 or more at a time. This meant that some of the questionnaires would be waiting for some days prior to arriving at the hospital. We therefore decided that the date-of-completion was the most uniform measure of return.
Odds ratios and two-sided significance tests (Fisher’s exact with mid-p correction and χ2-tests) were computed with the oddsratio-function of the epitools-package [7] within the statistical environment R [8]. We report p-values w.r.t. all three tests.
Basic descriptive statistics (age, sex-distribution, type of stroke and the ratio of participants living with a spouse) for the participants were computed for the sample as a whole, and for the IG and the CG separately: The latter values were also tested for significant differences with a standard two-sided t-test. The variable living with a spouse was included because the main protocol for mailing questionnaires involved printing the name of the spouse in addition to the name of the patient wherever a registered spouse existed on the same address. This practise originated in a hope that it would be more likely that the questionnaires were opened and returned when two individuals were named on the envelope.
A binary logistic model was also fitted to the combined data set, with responding as the dependent variable, and with predictors age, sex, type of stroke, a dummy for living with a spouse, and a dummy for being in the pre-contact group (i.e. by ITT).
Finally, a simple Cost Utility Analysis (CUA) reporting the cost per additional reply associated with this strategy for increasing the response rates is also provided.
Ethics
The NOR-SPOT project has been submitted to a regional ethics committee for medical research – Regional Committee for Medical & Health Research Ethics South East Norway, Section B – and exempted from evaluation because the study hypotheses were not directly related to health and illness. Under Norwegian law the project should then be approved by the hospital’s internal Privacy Ombudsman. The RCT was approved prior to initation of recruitment, with Ref.No. 11.076. Any queries should be directed to the Privacy Ombudsman at Akershus University Hospital.
The trial subjects of the prenotification RCT had not given written consent to partake in it. This follows from the nature of the study: trying to obtain answers. More importantly, under the original NORSPOT project, ethical approval for sending out the questionnaires was approved without the necessity of obtaining prior consent.
Results
Main results
A total of 235 patients, out of 652 patients assessed, were found eligible for randomization; 116 (49.4 %) were assigned to the IG and 119 (50.6 %) to the CG. During the intervention period, it was discovered through the ongoing data collection that 6 patients (3 in each arm) suffered from known dementia, and these were excluded from the RCT. 10 patients (7 in the IG and 3 in the CG) died before 12 months had passed from discharge from the SU; these were also excluded. Furthermore, one patient in the IG was discovered to have been misdiagnosed with stroke, and one patient in the control group was discovered to be a very frail nursing home patient, who had been mis-assessed as eligible for inclusion. 105 subjects in the IG and 112 controls remained (see Fig. 1). Basic descriptives of the subjects are given in Table 1; the control- and the intervention groups appear balanced with respect to age, sex, living with a spouse and type of stroke (as classified by Transient Ischemic Attack (TIA), cerebral infarction (INF), and intra-cerebral haemorrhage (ICH)).
Fig. 1.
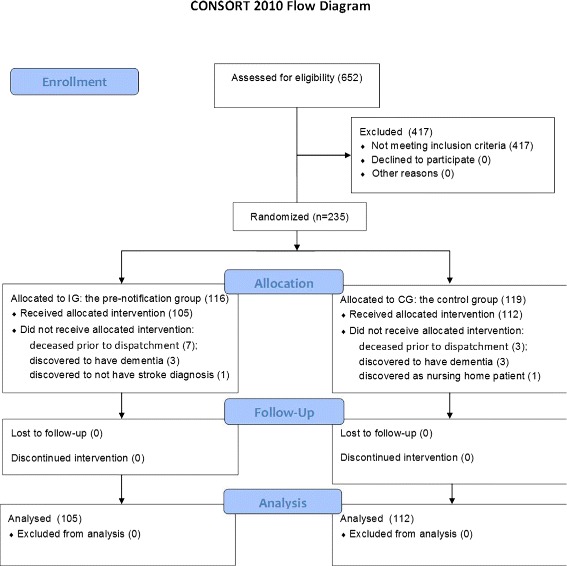
CONSORT 2010 flowchart for the inclusions and distribution of subjects to the IG and CG
Table 1.
Descriptive statistics of RCT participants
| All Participants | IG | CG | |||||
|---|---|---|---|---|---|---|---|
| N | % | N IG | % | N CG | |||
| 217 | 100 % | 105 | 48,4 % | 112 | 51,6 % | ||
| Mean | sd | Mean | sd | Mean | sd | p | |
| Age | 63,1 | 13,0 | 64,1 | 13,1 | 62,1 | 13,1 | 0,274 |
| n | % | n IG | % | n CG | % | p | |
| Male | 143 | 65,9 % | 67 | 63,8 % | 76 | 67,9 % | 0,532 |
| Partner | 139 | 64,1 % | 69 | 65,7 % | 70 | 62,5 % | 0,624 |
| TIA | 81 | 37,3 % | 43 | 41,0 % | 38 | 33,9 % | 0,288 |
| INF | 122 | 56,2 % | 55 | 52,4 % | 67 | 59,8 % | 0,272 |
| ICH | 14 | 6,5 % | 7 | 6,7 % | 7 | 6,2 % | 0,901 |
Simple descriptive statistics for the RCT participants and for the intervention- and control groups. Mean age and standard deviation of samples. The reported p-values are w.r.t. Welch 2-sided t-test for difference of mean/proportion between the IG and the CG computed with the native R t.test-function
The main results of the intention to treat analysis for the primary outcome and secondary outcome first response – defined as response returned within 45 days of the mailing date – are presented in Table 2. A clear positive effect of pre-contact by telephone was measured in both the primary and the secondary outcomes, with ORs of 2.040 (p=0.013) and 2.095 (p=0.009) respectively.
Table 2.
Main result: ITT-analyses of response rates
| 1. Outcome (45 day RR.) | 2. Outcome (365 day RR.) | |||||||
|---|---|---|---|---|---|---|---|---|
| Resp | Non-Resp | Total | RR | Resp | Non-Resp | Total | RR | |
| IG | 45 | 60a | 105 | 42.9 % | 48 | 57 | 105 | 45.7 % |
| CG | 30 | 82 | 112 | 26.8 % | 32 | 80 | 112 | 28.6 % |
| Total | 75 | 142 | 217b | 80 | 137 | 217 | ||
| Test | p | OR [95 % CI]: | ΔRR | p | OR [95 % CI]: | ΔRR | ||
| Mid-p | 0.014 | 2.040 [1.157, 3.639] | 16.1 % | 0.009 | 2.095 [1.197,3.707] | 17.1 % | ||
| Fisher’s | 0.015 | 0.011 | ||||||
| χ 2 | 0.013 | 0.009 | ||||||
The table contains the 2x2-contingency tables w.r.t. 1. and 2. outcomes, with total figures for respondents (Resp) and non-respondents (Non-Resp) in the intervention- and control groups. Response rates (RR) for the two study arms are also provided. Below the contingency tables we report the OR with 95 % CI’s, the absolute difference in response rates (ΔRR), and the p-values from three standard 2-sided tests for effect provided by the oddsratio-function from the epitools-package for R (CI’s are computed w.r.t. the mid-p value)
aIncludes the 5 respondents who were successfully contacted, but refused participation in the questionnaire study
bOriginally 235 patients were included; 10 patients (7 from the IG and 3 from the CG) died before it was time to send them a questionnaire; 6 (3 in the IG and 3 in the CG) were discovered to be demented; 1 IG patient was discovered to have been mis-diagnosed with stroke, and one CG patient was discovered to have been mis-assessed as eligible. These 18 were excluded prior to analysis
Secondary results
Of the 105 participants assigned to the IG we were able to successfully contact 92 (87.6 %) patients (or their care giver); 5 contacted participants (5.4 % of those reached; 4.8 % of the IG) refused to give the sought-after informal consent to shipping (see the Mailing of questionnaires and intervention-section). The 13 (12.4 %) participants whom we were unable to reach on the three attempts specified by the protocol were re-classified as controls (transferred to the CG) for the secondary APP-analysis. The result of this analysis is presented in Table 3, and reinforce the result from the ITT-analysis, demonstrating a positive effect of pre-contact by telephone on both the 1. and the 2. outcome, with ORs of 2.535 (p=0.001) and 2.354 (p=0.003) respectively.
Table 3.
As Per protocol-analysis
| 1. Outcome (45 day RR.) | 2. Outcome (365 day RR.) | |||||||
|---|---|---|---|---|---|---|---|---|
| Resp | Non-Resp | Total | RR | Resp | Non-Resp | Total | RR | |
| IG | 43 | 49a | 92 | 46.7 % | 45 | 47 | 92 | 51.1 % |
| CG | 32a | 93 | 125 | 25.6 % | 36 | 89 | 125 | 28.8 % |
| Total | 75 | 142 | 217b | 81 | 136 | 217 | ||
| Test | p | OR [95 % CI]: | ΔRR | p | OR [95 % CI]: | ΔRR | ||
| Mid-p | 0.001 | 2.535 [1.432, 4.540] | 21.1 % | 0.003 | 2.354 [1.343, 4.167] | 22.3 % | ||
| Fisher’s | 0.001 | 0.003 | ||||||
| χ 2 | 0.001 | 0.002 | ||||||
The table shows the 2x2-contingency tables w.r.t. 1. and 2. outcomes, with total figures for respondents (Resp) and non-respondents (Non-Resp) in the intervention- and control groups as defined in the APP-analysis. Response rates (RR) for the two study arms are also provided. Below the contingency tables we report the OR with 95 % CI’s, the absolute difference in response rates (ΔRR), and the p-values from three standard 2-sided tests for effect provided by the oddsratio-function from the epitools-package for R (CI’s are computed w.r.t. the mid-p value)
aThe IG non-responders includes the 5 respondents who were successfully contacted, but refused participation in the questionnaire study; the CG responders includes 2 responders who were randomized to be pre-contacted, who were not successfully reached, but who nevertheless returned their questionnaires
bOriginally 235 patients were included; 10 patients (7 from the IG and 3 from the CG) died before it was time to send them a questionnaire; 6 (3 in the IG and 3 in the CG) were discovered to be demented; 1 IG patient was discovered to have been mis-diagnosed with stroke, and one CG patient was discovered to have been mis-assessed as eligible. These 18 were excluded prior to analysis
The fitted binary logistic regression model yielded an OR in favour of telephone pre-contact of 2.00 (p=0.02) when adjusted for age, sex, type of stroke and a dummy which coded for living with a spouse. All the control variables – except the spouse-dummy – were insignificant. The independent OR (adjusted for pre-contact, age, sex and type of stroke) from the binary logistic regression model for responding when living with a spouse was 2.34 (p=0.01).
A rudimentary CUA analysis shows that the only significant resource consumed by the intervention is the time spent by the researcher/assistant. The cost of the telephone calls today are negligible (perhaps 10 cents per answered call). We therefore price the intervention in man-hours here. Due to the nature of our survey, it was important to ensure that patients had neither relocated nor were institutionalized, and, that they were still alive. Hence the book-keeping of whom we had tried to call, whom we still needed to call etcetera, and the actual calls themselves were the main driver of additional costs. Conversations could last from a few minutes to half-an-hour with patients who often took the call as an opportunity to talk and ask other questions, but we estimate that the difference in time spent on mailing questionnaires to participants in the IG compared to those in the CG was circa 10 minutes per participant. This figure was not systematically recorded, but TBS estimates that 7–8 minutes are actual time spent, whereas 10 minutes is a liberal guesstimate. An increase of 16.1 percentage points in response rate thus translates into a cost of per extra returned questionnaire. The monetary cost is therefore sensitive to the cost of labour qualified for performing the intervention.
Discussion
The RCT provides evidence supporting the hypothesis that pre-contact by phone increases response rates in postal surveys targeting a patient population with a low baseline response rate. Our population was one of non-responders from the 3-month questionnaire, and the CG response rate was 27 %. The IG had a significantly increased response rate, to 43 %. We expect the result to be fairly generalizable. This is not to say that one can necessarily expect the same OR for all populations, since e.g. a population with a high baseline response rate, might be less, or more, susceptible to stimulus. The fact that our study targeted a population of non-responders – that is, subjects with a low probability of responding as reflected in the CG’s RR of 27 % – could mean that the pre-contact intervention has a higher effect in our population, than on a population of people with higher baseline propensity towards responding.
The finding that living with a spouse was revealed as a strong and independent predictor of response in the secondary analysis is also interesting. The fact that pre-contact remained a strong predictor for response after correcting for a spouse strengthens the main result.
The APP-analysis yielded a higher OR (2.535) in favour of pre-contact than the ITT-analysis (2.040). This might mean that further efforts to reach those participants in the IG whom we did not reach could strengthen the results. However, being a non-responder might be correlated with being hard to reach. We have not attempted to describe the 15 out of the 105 (14.3 %) whom we could not reach, apart from noting that their 45-day and 360-day response rates were 13 % (2) and 20 % (3) respectively, and as such not deviating much from the response rate of the CG.
We end with a few comments with regard to the CUA. Clearly the intervention’s cost depends strongly on the cost of labour; under Norwegian conditions the price is circa 40 Euro for one labour-hour. It is well-known that pecuniary incentives has a very strong and near guaranteed effect on response rates, so that one might obtain the same increase by merely paying for responses. However, adding money to the mix sometimes have unexpected results, and there is no guarantee that paying would help on a population of patients, who might consider the effort not worth the price offered. Prepaid incentives (provide incentives together with the questionnaire) are known to be efficient; see [1] for an array of further references and summarized pooled ORs. However, to beat pre-contact with this latter strategy, the offered prepaid incentive per questionnaire could not exceed the cost of 10 min of labour (under Norwegian conditions about 7 Euro), given that overall reported pooled ORs for monetary incentives are in the same range as the pre-contact OR reported here. The meta-analysis [1] also documents that larger monetary incentives yield better RR than smaller incentives, which might give pre-contact a further advantage due to its relatively low cost.
Regardless of possible local ethical considerations, it would surely be interesting to compare our reported cost-effectiveness with that of pecuniary incentives. Also, response biases could differ between the two approaches, but these questions were outside of the scope of our present study.
The bottom line is perhaps an ethical one: adding money to the equation could be conceived as inappropriate when eliciting sensitive information from a patient population, while contacting them directly to obtain their permission – appealing to a sense of companionship rather than a mercantile one – seems more in the spirit of health services research.
Conclusion
The results are in line with previous research, and show that pre-contact has a positive effect on response rate: the estimated OR in our population was 2.04 (95 % CI [1.16,3.64]). Given the importance of a high response rates in surveys, the stipulated cost of 1 working hour per additional response is likely to be worth while; in particular if pecuniary incentives are off the table.
Protocol available from http://www.isrctn.com/ISRCTN31304930.
Acknowledgements
We thank statistician Dr. Jūratė Šaltytė Benth at the University of Oslo for carrying out the randomization for the study. We also thank our colleagues at the Health Services Research Center at Akershus University Hospital for valuable conversation during the early phases of designing the study.
Funding
The NORSPOT project has been partially financed by NRC grants Simulation Simulating patient flow and health care costs in Norway No. 196454 and Modelling treatment and rehabilitation of stroke patients – Using simulation to evaluate the present and plan for the future No. 237809.
Availability of data and materials
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
Authors’ contributions
MB conceived of and designed the study, drafted the first manuscript, performed the statistical analyses. TBS collected the data, performed the pre-contact, assisted on data analyses and approved and contributed to drafts and final manuscript. FAD designed the study, advised on statistical analyses and approved and contributed to drafts and final manuscript. All authors read and approved the final manuscript.
Authors’ information
Mathias Barra tweets as @Mathbarra.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The NORSPOT project is an in-hospital venture investigating the paths of treatment of the hospital’s patients without any deviation from standard practices and has been classified as a quality-assurance project by the Regional Ethics Committee (REK) of the hospital’s jurisdiction. Therefore, and in accordance with REK’s recommendation, ethical approval was sought with the Privacy Ombudsman at Ahus (Approval number 11-076).
Abbreviations
- ABB
Abbreviation
- APP
As-per-protocol
- CG
Control group
- CUA
Cost-utility analysis
- GP
General practitioner
- ICH
Intra cerebral haemorrhage
- INF
Cerebral Infarction
- IG
Intervention group
- ITT
Intention-to-treat
- OR
Odds ratio
- RCT
Randomized controlled trial
- RR
Response rate
- SU
Stroke unit
- TIA
Transient Ischemic attack
Contributor Information
Mathias Barra, Email: mathias.barra@ahus.no.
Tone Breines Simonsen, Email: tone.breines.simonsen@ahus.no.
Fredrik Andreas Dahl, Email: fredrik.a.dahl@ahus.no.
References
- 1.Edwards PJ, Clarke MJ, DiGuiseppi C, Wentz R, Kwan I, Cooper R, Felix LM, Pratap S. Methods to increase response to postal and electronic questionnaires (review). Cochrane Database Syst Rev.2009; 3. doi:10.1002/14651858.MR000008.pub4. [DOI] [PMC free article] [PubMed]
- 2.Harrison RA, Cock D. Increasing response to a postal survey of sedentray patients – a randomised controlled trial [isrctn45665423]. BMC Health Serv Res.2004; 4(31). doi:10.1186/1472-6963-4-31. [DOI] [PMC free article] [PubMed]
- 3.Wiseman F. Factor interaction effects in mail survey response rates. J Market Res. 1973;10(3):330–3. doi: 10.2307/3149705. [DOI] [Google Scholar]
- 4.Whiteman MK, Langenberg P, Kjerulff K, McCarter R, Flaws JA. A randomized trial of incentives to improve response rates to a mailed women’s health questionnaire. J Women’s Health. 2003;12(8):821–8. doi: 10.1089/154099903322447783. [DOI] [PubMed] [Google Scholar]
- 5.ISRCTN registry. http://www.isrctn.com/ISRCTN31304930.
- 6.Ogborne AC, Rush B, Fondacaro R. Dealing with nonrespondents in a mail survey of professionals the cost-effectiveness of two alternatives. Eval Health Prof. 1986;9(1):128–8. doi: 10.1177/016327878600900109. [DOI] [Google Scholar]
- 7.Aragon TJ. epitools: Epidemiology tools. 2012. R package version 0.5–7. https://cran.r-project.org/web/packages/epitools/index.html.
- 8.Team RC. R: A language and environment for statistical computing. r foundation for statistical computing. 2013. http://www.R-project.org/.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.