

Dynamic hyperinflation (DH) is a consequence of severe airflow obstruction in patients with asthma and chronic obstructive pulmonary disease (COPD). Incorrect setting of positive end-expiratory pressure (PEEP) can lead either to unopposed intrinsic PEEP (iPEEP) (when set too low) or to an increase in lung volume if PEEP is set above iPEEP. DH and iPEEP can lead to haemodynamic compromise [1], increased work of breathing and asynchrony [2]. PEEP setting is challenging because iPEEP is clinically difficult to quantify. Electrical impedance tomography (EIT) provides information on the temporal and spatial heterogeneity of ventilation [3]. EIT may prove useful in optimizing PEEP to overcome gas trapping and DH [4]. We present a method in which the use of EIT allowed selection of PEEP to provide the least DH and inhomogeneity of lung mechanics.
A patient with severe acute COPD exacerbation was on pressure control ventilation: FiO2 0.25, PEEP 10 cmH2O, peak pressure 28 cmH2O, tidal volume 515 ml, I:E 1:4.4 and set frequency 14/min using an Evita XL ventilator (Draeger–Luebek, Germany). After a short period, the patient developed worsening hypercapnia and clinical evidence of DH. Subsequently a PEEP titration using EIT (Pulmovista®; Draeger–Luebek) was performed to optimize ventilator settings with the aim of minimizing DH.
The patient remained sedated, paralysed and in a supine position throughout the PEEP titration. We measured static iPEEP and compliance using end-inspiratory and end-expiratory hold manoeuvres. iPEEP was measured in a range of set external PEEP, and the iPEEP was calculated as total PEEP minus set PEEP. EIT, tidal volumes, trapped gas volumes and ventilator pressures were then measured at PEEP set to 0 %, 50 %, 80 %, 100 % and 150 % of iPEEP.
EIT waveforms were analysed offline to determine ventilation heterogeneity at different levels of applied PEEP corresponding to 50 %, 80 %, 100 % and 150 % of the static iPEEP. We measured the regional delay of ventilation as a marker of homogeneity of ventilation [5]. We compared this index with oesophageal pressure, with static and dynamic compliance and with arterial blood gases.
EIT allowed determination of the level of PEEP able to achieve greatest lung homogeneity. This level of PEEP was 80 % of iPEEP (Fig. 1). This value also achieved the highest expired tidal volume and the lowest airway resistance. Lung mechanics suggest that PEEP between 80 and 100 % of iPEEP achieves the best compromise between total PEEP and trapped volume (Table 1).
Fig. 1.
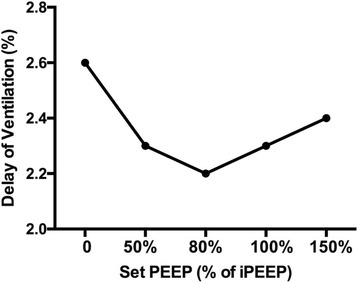
Delays in ventilation as an index of ventilation heterogeneity calculated by EIT using different levels of positive end-expiratory pressure (PEEP) as a percentage of the calculated intrinsic PEEP (iPEEP). Setting PEEP at 80 % of iPEEP achieves the greatest homogeneity of ventilation
Table 1.
Measurements of lung mechanics at different PEEP levels
| ZEEP | 50 % iPEEP | 80 % iPEEP | 100 % iPEEP | 150 % iPEEP | |
|---|---|---|---|---|---|
| Set PEEP (cmH2O) | 0 | 5 | 8 | 10 | 15 |
| PEEP tot measured (cmH2O) | 10 | 10 | 11 | 11 | 15 |
| Plateau pressure (cmH2O) | 18 | 21 | 20 | 19 | 21 |
| Expired tidal volume (ml) | 505 | 515 | 515 | 500 | 372 |
| Static compliance (ml/cmH2O) | 63 | 47 | 57 | 62.5 | 62 |
| Trapped volume (ml) | 390 | 350 | 150 | 80 | 0 |
ZEEP zero end-expiratory pressure, iPEEP intrinsic positive end-expiratory pressure, PEEP positive end-expiratory pressure
This case illustrates how EIT may be useful in assessing regional ventilation and suggesting optimal PEEP. Through optimizing conventional ventilation, bedside EIT may guide ventilatory strategy to reduce hyperinflation, reduce dead space and hence reduce asynchrony and work of breathing without the need for more invasive procedures.
Acknowledgments
Authors’contributions
EK, NB and LC designed and participated in drafting the manuscript. EK and LC approved the final version. All authors read and approved the final manuscript.
Competing interests
LC received speaking honoraria from Draeger. NB receives research and educational funding from Draeger, ALung, Maquet, Corpak, Fisher & Paykel and Mitsubishi-Tanabe Pharmaceuticals. EK declares that they have no competing interests.
Declaration of interests
EK is in a clinical research fellowship funded by ALung Technologies Incorporated. LC and NB have no personal financial interests to disclose.
Abbreviations
- COPD
Chronic obstructive pulmonary disease
- DH
Dynamic hyperinflation
- EIT
Electrical impedance tomography
- iPEEP
Intrinsic positive end-expiratory pressure
- PEEP
Positive end-expiratory pressure
- ZEEP
Zero end-expiratory pressure
Contributor Information
Eirini Kostakou, Phone: +44 (0) 20 7188 3038, Email: ekostakou@yahoo.com.
Nicholas Barrett, Email: Nicholas.Barrett@gstt.nhs.uk.
Luigi Camporota, Email: Luigi.Camporota@gstt.nhs.uk.
References
- 1.Brandolese R, Broseghini C, Polese G, Bernasconi M, Brandi G, Milic-Emili J, Rossi A. Effects of intrinsic PEEP on pulmonary gas exchange in mechanically-ventilated patients. Eur Respir J. 1993;6(3):358–63. [PubMed] [Google Scholar]
- 2.Laghi F, Goyal A. Auto-PEEP in respiratory failure. Minerva Anestesiol. 2012;78(2):201–21. [PubMed] [Google Scholar]
- 3.Vogt B, Pulletz S, Elke G, Zhao Z, Zabel P, Weiler N, Frerichs I. Spatial and temporal heterogeneity of regional lung ventilation determined by electrical impedance tomography during pulmonary function testing. J Appl Physiol. 2012;113:1154–61. doi: 10.1152/japplphysiol.01630.2011. [DOI] [PubMed] [Google Scholar]
- 4.Mauri T, Bellani G, Salerno D, Mantegazza F, Pesenti A. Regional distribution of air trapping in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;188:1466–7. doi: 10.1164/rccm.201303-0463IM. [DOI] [PubMed] [Google Scholar]
- 5.Muders T, Luepschen H, Zinserling J, Susanne Greschus S, Fimmers R, Guenther U, Buchwald M, Grigutsch D, Leonhardt S, Putensen C, Wrigge H. Tidal recruitment assessed by electrical impedance tomography and computed tomography in a porcine model of lung injury. Crit Care Med. 2012;40(3):903–11. doi: 10.1097/CCM.0b013e318236f452. [DOI] [PubMed] [Google Scholar]