

Abstract
Background
To discuss the management of impacted canines and the various approaches used for the same.
Materials and methods
The data of 33 cases, with 43 impacted canine teeth, seen and operated over a period of 3-year in Santosh Dental College and Hospital has been compiled. The diagnostic methods and treatment modalities undertaken are described and discussed.
Results
Canine impactions were more common in the maxilla as compared with mandible in our study, which was statistically significant. Impacted canine position was mostly palatal in maxilla and labial in mandible. Chi-square test yielded a p-value of 0.002 which shows that there is an association between arch and position. The treatment options used were surgical exposure and orthodontic repositioning, cyst enucleation with extraction of impacted canine and surgical removal of impacted canine.
Conclusion
Surgical exposure and orthodontic repositioning was successfully applied as first-line treatment for correcting ectopic positioned canine. In cases where exposure and subsequent orthodontic treatment was not indicated, the impacted canine was surgically removed to prevent future problems and surgical procedure was designed according to position of impacted canine.
Keywords: Impacted maxillary canine, Impacted mandibular canine, Surgical exposure, Orthodontic repositioning.
INTRODUCTION
Impacted canine is not an uncommon clinical problem in dental patients. The permanent canines are developed deep within the jaws, complete their development late, and emerge into oral cavity after the neighboring teeth. Due to these circumstances, eruption disturbances are more common with canines than with other teeth, except for third molar.1 Studies have reported that the incidence of tooth impaction varies from 5.6 to 18.8% of the population.2-6 It is of concern that the method of diagnosis and the choice of treatment planning of this problem poses as a dilemma to the dental clinician. Maximum success with least complications and failures requires a systematic approach to each case.
We have reviewed 34 patients diagnosed with impacted canines. Each of these case had a detailed history followed by meticulous clinical and radiological examination to determine the exact site and position of the impacted tooth and to detect if any associated pathology was present in relation to the impacted tooth. This paper describes our approach for management and highlights the tips for successful management which can be applied as a protocol to each patient presenting with impacted canine.
MATERIALS AND METHODS
A total of 33 cases (13 males and 20 females) within the age group of 12 to 18 years, who were referred from the department of pedodontics, were included in this review. The criterion for a diagnosis of impacted canine included both clinical and radiological findings. The clinical elements which were suggestive of occurrence and location of impacted canine include:
Overretained deciduous canine.
Absent deciduous canine and resulting in loss of the available space for permanent tooth.
Tipping of lateral incisor in a vestibular or palatal position (Due to the pressure of the canine at its root).
Presence of a bump which can be felt by palpating the vestibular or palatal mucosa depending on the position of the retained canine. Clinically palpation of the buccal and palatal surface of the alveolar process distal to the lateral incisor may reveal the position of the maxillary canine about 1 to 1.5 years before emergence, and this has been suggested as a diagnostic tool.1
This was followed by radiologic examinations (IOPA/ orthopantomogram/occlusal view/paranasal sinus view/ dentascan) which were indispensable in diagnosing and locating the position of impacted canines (Figs 1 to 4). The etiologic factors observed in our study were arch length, tooth size discrepancy, accounting for 41% of cases, followed by overretained deciduous teeth, early loss of deciduous canine, cyst, trauma, cleft palate and cleidocranial dysostosis.
Fig. 1.
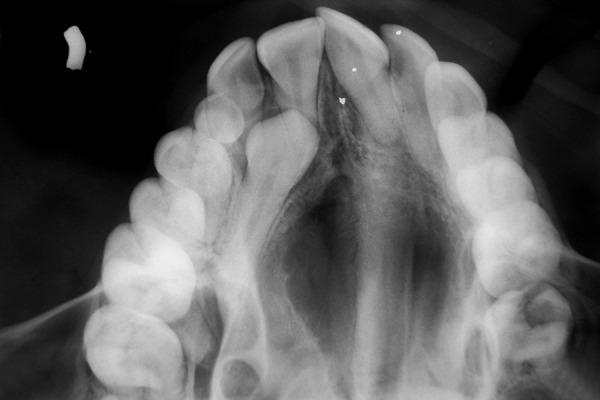
Occlusal view of maxilla showing impacted right maxillary canine
Fig. 4.

Dentascan showing bilateral impacted mandibular canines labially
The available treatment options were surgical removal of impacted canine (along with its associated pathology), or surgical exposure and orthodontic repositioning. Surgical removal of impacted canine was indicated if there was evidence of pathology around the tooth; if there was interference with planned orthodontic treatment; and if there was impingement on adjacent teeth. Exposure and orthodontic repositioning was carried out if space analysis revealed that tooth can be brought into occlusion and deviation of tooth axis was not too excessive (Table 1).
Table 1: Treatment modalities
|
No. of cases (total 33) |
Percentage |
No. of teeth (total 43) |
Percentage | ||||||
| Surgical removal of impacted canine | 10 | 30.30 | 16 | 37.2 | |||||
| Surgical exposure and orthodontic treatment | 15 | 45.45 | 18 | 41.8 | |||||
| Cyst enucleation with extraction of impacted canine | 7 | 21.21 | 7 | 16.2 | |||||
| Surgical removal with fracture fixation | 1 | 3.03 | 2 | 4.6 |
Fig. 2.

IOPA showing impacted maxillary canine
Fig. 3.

OPG showing bilateral impacted mandibular canines and left maxillary impacted canine
RESULTS
Statistical tests were applied to the descriptive data to detect any predilection for either arch and any preponderance of placement within the arch. Z test for comparing proportions yielded p-value of 0.000123 which is significant. Impacted canines are most commonly found in maxilla as compared with mandible (Table 2). Chi-square test yielded a p-value of 0.002 which shows that there is an association between arch and position. In maxilla, the impacted canine is in palatal position whereas in mandible, it is commonly located in labial position (Tables 3, 4 and Graph 1).
Table 2: Position of impacted teeth
| Arch | No. of teeth (total 43) | Percentage | |||
| Maxilla | 30 | 69.76 | |||
| Mandible | 13 | 30.23 |
Table 3: Arch vs position crosstabulation
| Arch |
Buccal/ vestibular |
Palatal/ lingual |
Intermediate |
Unusual position |
Total | ||||||||
| Maxilla | 7 | 19 | 2 | 2 | 30 | ||||||||
| 23.3% | 63.3% | 6.7% | 6.7% | 100.0% | |||||||||
| Mandible | Count | 8 | 0 | 3 | 2 | 13 | |||||||
| Percent within | 61.5% | 0.0% | 23.1% | 15.4% | 100.0% | ||||||||
| according to arch | |||||||||||||
| Total | 15 | 19 | 5 | 4 | 43 | ||||||||
| 34.9% | 44.2% | 11.6% | 9.3% | 100.0% |
Table 4: Statistical inference
| Value | df |
Asymp. sig. (two-sided) |
|||||
| Pearson Chi-square | 14.870 | 3 | 0.002 | ||||
| Likelihood ratio | 19.700 | 3 | 0.000 | ||||
| Linear-by-linear | 0.020 | 1 | 0.887 | ||||
| association | |||||||
| No. of valid cases | 43 |
Graph 1.
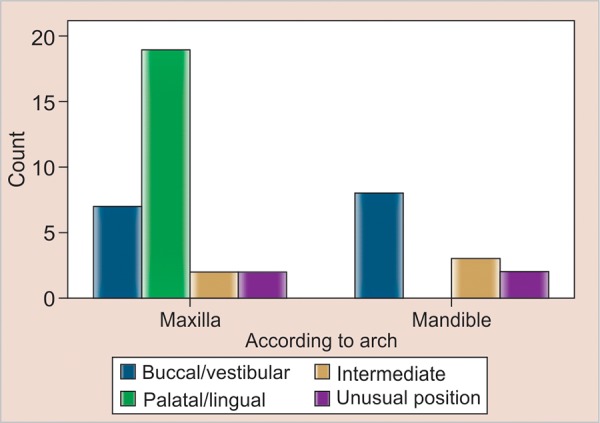
Arch vs position
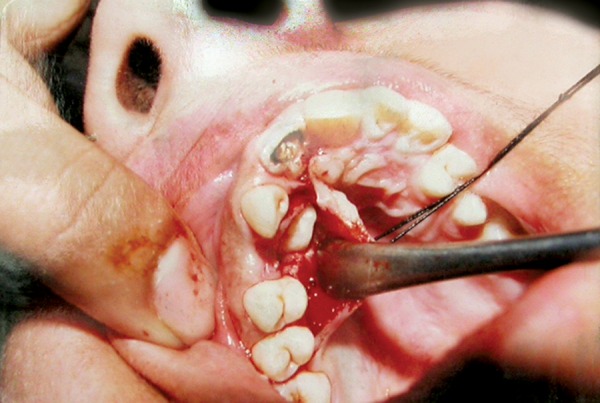
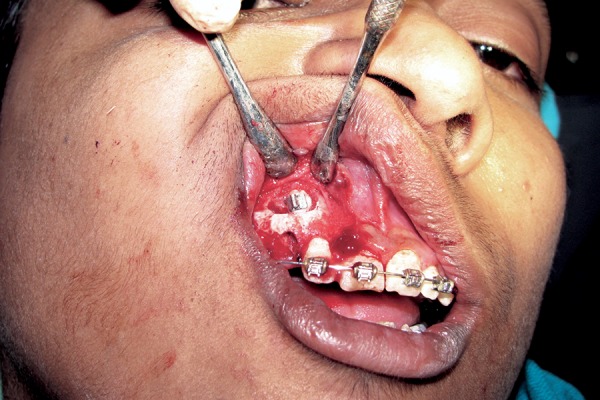
The frequency of surgical approach was determined to show that the ease of access to the impacted canine is the main decisive factor (Figs 5 and 6). The operator should not be hesitant to use the combined approach wherever indicated (Tables 5 to 7).
Fig. 5.
Clinical photograph showing palatal approach
Fig. 6.
Clinical photograph showing buccal approach
Table 5: Surgical approaches
| Approach | No. of teeth | Percentage | |||
| Labial/vestibular | 19 | 44.19 | |||
| Palatal | 19 | 44.19 | |||
| Combined (labial and palatal) | 5 | 11.63 | |||
| Total | 43 | 100 |
Table 7: Statistical inference
| Value | df |
Asymp. sig. (two-sided) |
|||||
| Pearson Chi-square | 86.000 | 6 | 0.000 | ||||
| Likelihood ratio | 83.591 | 6 | 0.000 | ||||
| Linear-by-linear | 7.749 | 1 | 0.005 | ||||
| association | |||||||
| No. of valid cases | 43 |
DISCUSSION
Canine impactions are more commonly associated with the maxilla than with the mandible; the same has been reported in our study which was statistically significant. One interesting finding seen in our study was the position of impacted canine in the two jaws that the impacted canine was mostly palatal in maxilla, whereas in the mandible it was more frequently seen in labial position. Chi-square test yielded a p-value of 0.002 which shows that there is a strong association between arch and position. According to Andreason,1 85% impactions are palatally located in the maxilla. Unusual positions seen in our study was the location of canine in symphysis, maxillary sinus and infraorbital regions. Bilateral representation of impacted canines was also observed.
To establish a diagnosis, several diagnostic methods have been adopted which include a variety of radiographs. IOPA radiographs with or without shift cone technique was the primary diagnostic modality in all our cases. As per requirement other radiographs, such as orthopantomogram, occlusal and PNS views, were advised. Recently in few cases, computed tomography was utilized to evaluate the impacted canines. Dentascan provided detailed information about exact position of canine, degree of crowding, incisor resorption and width of dental follicle.7-10
To treat a case of impacted canine, there can be various options ranging from keeping the patient under observation; surgical exposure and orthodontic repositioning; reimplantation and surgical relocation of impacted canine in the socket of the deciduous canine; to surgical removal of the impacted canine (Figs 7 to 11).
Fig. 7.

OPG showing horizontally impacted right maxillary canine
Fig. 11.

Primary wound closure
The factors that need to be evaluated before the mode of treatment of impacted tooth is decided, include the patient’s age, dental status of adjacent teeth (including periodontal, endodontic and operative status, shape and resorption), dental status of the impacted tooth, occlusal relationship, presence of any other associated condition (e.g. trauma/cyst/ odontoma) and arch length.11-14
Surgical exposure and orthodontic repositioning was considered the treatment of choice in all those cases wherever it was clinically feasible and a predictable and successful outcome could be obtained. The prognosis for orthodontically assisted eruption and repositioning of an impacted tooth within the alveolar process depends on the position and angulation of the impacted tooth, the length of treatment time, the patient’s age, degree of patient cooperation, the available space in the arch and the presence of keratinized gingival tissue.15-17
Fig. 8.

Flap raised and marking done
Fig. 9.

Impacted canine exposed and sectioned
Fig. 10.

Removal of the tooth after sectioning
In cases, where exposure and subsequent orthodontic treatment was not indicated, the impacted canine was surgically removed to prevent future problems and surgical procedure was designed according to position of impacted canine.
After tooth impaction is diagnosed and if a decision to not undertake any immediate intervention is made, it is recommended that periodic observation is done to rule out possible pathological sequelae. During this observation period, clinicians must perform clinical and radiologic examinations after every 18 to 24 months. The following pathological sequelae associated with tooth impaction have been noted: Dentigerous cyst, odontogenic keratocyst, adenomatoid odontogenic tumor, calcifying epithelial odontogenic (Pindborg) tumor, odontogenic myxoma, ameloblastoma, external/internal resorption of the impacted tooth, external root resorption of adjacent teeth, transmigration, referred pain and periodontitis.11,18-27
Therefore, when decision is to retain an impacted tooth clinician must be vigilant for the potential development of a dentigerous cyst or ameloblastoma. The excised cyst/tissue should always be submitted to pathologist for microscopic examination for diagnosis.
Table 6: Surgical approach vs position crosstabulation
| Position | |||||||||||||
| Approach |
Buccal/ vestibular |
Palatal/ lingual |
Intermediate |
Unusual position |
Total | ||||||||
| Labial/ | 15 | 0 | 0 | 4 | 19 | ||||||||
| vestibular | 78.9% | 0.0% | 0.0% | 21.1% | 100.0% | ||||||||
| Palatal | Count | 0 | 19 | 0 | 0 | 19 | |||||||
| Percent within | 0.0% | 100.0% | 0.0% | 0.0% | 100.0% | ||||||||
| surgical approach | |||||||||||||
| Combined | 0 | 0 | 5 | 0 | 5 | ||||||||
| (labial | 0.0% | 0.0% | 100.0% | 0.0% | 100.0% | ||||||||
| and palatal) | |||||||||||||
| Total | 15 | 19 | 5 | 4 | 43 | ||||||||
| 34.9% | 44.2% | 11.6% | 9.3% | 100.0% | |||||||||
CONCLUSION
In our study, canine impactions were more common in the maxilla as compared with the mandible which is statistically significant. Our study also shows that impacted canine position is mostly palatal in maxilla and labial in mandible. The crosstabulation shows that there is a strong association between arch and position. As the sample size was less, we need to study more number of cases to establish that such a correlation exists. Radiographs play a major role in diagnosing and determining the position of impacted canine. This further helps in deciding the approach to be used, i.e. labial, palatal or combined surgical approach. Various options can be used to manage a case of impacted canine. Surgical exposure and orthodontic repositioning was considered the treatment of choice. In cases where exposure and subsequent orthodontic treatment was not indicated, the impacted canine was surgically removed to prevent future problems and surgical procedure was designed according to position of impacted canine. We did not find any difference in complication rate between the palatal or buccal or combined approach.
REFERENCES
- 1.Andreason JO, Peterson JK., Laskin DM. Textbook and color atlas of tooth impactions. Copenhagen: Munksgaard Publishers; 1997. p. 544. [Google Scholar]
- 2.Kramer RM, Williams AC. The incidence of impacted teeth: A survey at Harlem Hospital. Oral Surg Oral Med Oral Pathol. 1970 Feb;29(2):237–241. doi: 10.1016/0030-4220(70)90091-5. [DOI] [PubMed] [Google Scholar]
- 3.Grover PS, Lorton L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol. 1985 Apr;59(4):420–425. doi: 10.1016/0030-4220(85)90070-2. [DOI] [PubMed] [Google Scholar]
- 4.Dachi SF, Howell FV. A survey of 3,874 routine full-mouth radiographs, II: A study of impacted teeth. Oral Surg Oral Med Oral Pathol. 1961 Oct;14:1165–1169. doi: 10.1016/0030-4220(61)90204-3. [DOI] [PubMed] [Google Scholar]
- 5.Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res. 1973;81(1):12–20. doi: 10.1111/j.1600-0722.1973.tb01489.x. [DOI] [PubMed] [Google Scholar]
- 6.Shah RM, Boyd MA, Vakil TF. Studies of permanent tooth anomalies in 7,886 Canadian individuals, I: impacted teeth. Dent J. 1978 Jun;44(6):262–264. [PubMed] [Google Scholar]
- 7.Ericson S, Kurol J. Incisor resorption caused by maxillary cuspids. A radiographic study. Angle Orthod. 1987 Oct;57(4):332–346. doi: 10.1043/0003-3219(1987)057<0332:IRCBMC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987 Jun;91(6):483–492. doi: 10.1016/0889-5406(87)90005-9. [DOI] [PubMed] [Google Scholar]
- 9.Ericson S, Kurol J. CT diagnosis of ectopically erupting maxillary canines: A case report. Eur J Orthod. 1988 May;10(2):115–120. doi: 10.1093/ejo/10.2.115. [DOI] [PubMed] [Google Scholar]
- 10.Schmuth GP, Freisfeld M, Koster O, Schuller H. The application of computerized tomography in cases of impacted maxillary canines. Eur J Orthod. 1992 Aug;14(4):296–301. doi: 10.1093/ejo/14.4.296. [DOI] [PubMed] [Google Scholar]
- 11.Kokich VG, Mathews DP. Surgical and orthodontic management of impacted teeth. Dent Clin North Am. 1993 Apr;37(2):181–204. [PubMed] [Google Scholar]
- 12.Di Salvo NA. Evaluation of unerupted teeth: Orthodontic viewpoint. J Am Dent Assoc. 1971 Apr;82(4):829–835. doi: 10.14219/jada.archive.1971.0137. [DOI] [PubMed] [Google Scholar]
- 13.Wise RJ. Periodontal diagnosis and management of the impacted maxillary cuspid. Int J Periodontics Restorative Dent. 1981;1(2):56–73. [PubMed] [Google Scholar]
- 14.Peterson LJ., Ellis E., Hupp JR . Contemporary oral and maxillofacial surgery. St Louis: CV Mosby; 1988. pp. 232–246. [Google Scholar]
- 15.Proffit WR. Contemporary orthodontics. St Louis: CV Mosby; 1993. pp. 217–219, 403-410. [Google Scholar]
- 16.Fournier A, Turcotte JY, Bernard C. Orthodontic considerations in the treatment of maxillary impacted canines. Am J Orthod. 1982 Mar;81(3):236–239. doi: 10.1016/0002-9416(82)90056-2. [DOI] [PubMed] [Google Scholar]
- 17.Lorenz T. Orthodontic considerations of the impacted canine. J Gen Orthod. 1990 Mar;1(1):12–21. [PubMed] [Google Scholar]
- 18.Bishara SE. Impacted maxillary canines: A review. Am J Orthod Dentofacial Orthop. 1992 Feb;101(2):159–171. doi: 10.1016/0889-5406(92)70008-X. [DOI] [PubMed] [Google Scholar]
- 19.Bishara SE. Clinical management ofimpacted maxillary canines. Semin Orthod. 1998 Jun;4(2):87–98. doi: 10.1016/s1073-8746(98)80006-6. [DOI] [PubMed] [Google Scholar]
- 20.Kuftinec MM, Shapira Y, Nahlieli O. A case report: Bilateral transmigration of impacted mandibular canines. J Am Dent Assoc. 1995 Jul;126(7):1022–1024. doi: 10.14219/jada.archive.1995.0279. [DOI] [PubMed] [Google Scholar]
- 21.Bishara SE, Kommer DD, McNeil MH, Montagano LN, Oesterle LJ, Youngquist HW. Management of impacted canines. Am J Orthod. 1976 Apr;69(4):371–387. doi: 10.1016/0002-9416(76)90207-4. [DOI] [PubMed] [Google Scholar]
- 22.Wertz RA. Treatment of transmigrated mandibular canines. Am J Orthod Dentofacial Orthop. 1994 Oct;106(4):419–427. doi: 10.1016/S0889-5406(94)70064-8. [DOI] [PubMed] [Google Scholar]
- 23.Bhaskar SN. Synopsis of oral pathology. St Louis: Mosby; 1981. pp. 217–225. [Google Scholar]
- 24.Waldron CA. Odontogenic cysts and tumors. In: Neville BW, Damm DD, Allen CM, Bouquot JE, editors. Oral and maxil-lofacial pathology. Philadelphia: Saunders; 1995. pp. 493–540. [Google Scholar]
- 25.Nordenram A. Impacted maxillary canines: A study of surgically treated patients over 20 years of age. Swed Dent J. 1987;11(4):153–58. [PubMed] [Google Scholar]
- 26.Stafne EC, Austin LT. Resorption of embedded teeth. J Am Dent Assoc. 1945 Aug;32(15):1003–1009. [Google Scholar]
- 27.Pogrel MB. Evaluation of over 400 autogenous tooth transplants. J Oral Maxillofac Surg. 1987 Mar;45(3):205–211. doi: 10.1016/0278-2391(87)90116-9. [DOI] [PubMed] [Google Scholar]