

Abstract
Introduction:
Multiple Sclerosis (MS) is one of the most common autoimmune diseases affecting the central nervous system. The prevalence of it is increasing in our country too. The pain from disorders can affect quality of life. Several studies have pointed to the improvement of patients through educational intervention. This study attempted to evaluate the effectiveness of an educational intervention based on raising the awareness and self-efficacy for pain control among patients with multiple sclerosis during 2015 under the coverage of Isfahan MS Society (IMSS).
Materials and methods:
This was a quasi-experimental study involving pre-test, post-test and randomized control group conducted on 100 patients with MS referred to the Isfahan MS Society (IMSS). The educational intervention group learned the pain management self-care lesson during 4 weekly sessions. The data were collected through a self-structured questionnaire with adequate validity and reliability, containing demographic data, awareness and self-efficacy of pain control. The data were assessed through descriptive and analytical tests assisted by SPSS 17. The significant level was considered as P<0.05.
Results:
Concerning the questionnaire, 96% of the items were responded. Most participants were women. The frequency distribution of demographic variables was not significantly different between the two pre-test groups. After the intervention, the mean score of knowledge and efficacy among patients in the intervention group was significantly higher than the control group (P<0.001).
Conclusions:
Educational interventions can improve awareness and self-efficacy for pain control among patients with MS. Therefore, such interventions can be designed to reduce physical and psychological complications following multiple sclerosis.
Keywords: Education, Controlled Before-After Studies, Multiple sclerosis, knowledge, Self-efficacy, pain (chronic pain)
1. INTRODUCTION
Multiple Sclerosis (MS) is one of the most common progressive autoimmune diseases affecting central nervous system (CNS), accompanied by inflammation, loss of the myelin sheath and degradation of the brain tissue and spinal cord. The MS entails various trends and progressive periods (1). Although there is little precise information on the cause of the disease, its prevalence among American women has been demonstrated over the last 40 years (2). Iran was previously known as a low-risk area for MS, but the prevalence of the disease today has dramatically increased especially at a young age and among women (3) According a report by Etemadifar et al. (2011), the prevalence of MS doubled in Isfahan compared to five years ago, falling under the category of regions with great prevalence in Asia Pacific (4, 5)
Studies have shown that the multiple mental and physical disorders due to MS can impair the patients’ quality of life (6). Weakness, fatigue and dizziness are examples of physical complications of this disease. Pain is a contributing factor to the quality of life with an approximate incidence of 63% (7). Nerve damage, nerve fiber membrane disruption pain, weakness, spasms, and paralysis of the muscles are the causes of pain experienced in the form of facial pain, back pain, and chronic pain in other organs (8, 9). Although medicinal treatments, acupuncture, acupressure, massage and relaxation will leave palliative effects on pain among the MS patients (10, 11). Pain management has always been a challenge. Costliness, loss of therapeutic effect and side effects of pain-relievers over time, poor knowledge of pain management techniques are the obstacles to medicinal therapies (12, 13). Pain in patients with multiple sclerosis leads to low levels of health and increasing burden of disease, thus degrading the social functioning of these patients. Celibacy and low education levels are the well-known risk factors for pain in these patients (14).
Additional methods of pain and disability control are rehabilitation and self-management which can be exercised without any massive spending and pharmacological interventions. The key to self-management is knowledge about the disease, and establishing better relations with health care providers (15). Studies have pointed to improvements of health status over face to face educational interventions, demonstrated by MRI (16). Studies have also revealed a significant correlation between education level and self-care knowledge (17). In fact, people with higher awareness can better get along with the disease and tend to report a greater quality of life (18). On the other hand, the effect of psychological factors such as self-efficacy and social support in pain control has been demonstrated in these patients (7, 15, 19). Self-efficacy is the core of social cognitive theory, referring to the individual confidence in a specific aimed at achieving success. Self-efficacy among patients with MS reflects self-confidence and the ability to perform self-care behaviors in order to control MS. Patients with higher self-efficacy are more likely to set out self-care behaviors and tend to be more adhering to that beneficial behavior (7). Furthermore, there has been a significantly reverse relationship reported between perceived self-efficacy, depression and anxiety and intensity of pain felt by patients with multiple sclerosis (13, 20, 21).
In general, studies have shown that the use of self-care education in patients with MS will enhance the quality of life, independence and vitality (22-24) and less fatigue (25).
Due to the growing number of MS cases in Isfahan and physical and emotional difficulties caused by the disease sometimes appearing as chronic pain overshadowing the patient’s quality of life, this study attempted to evaluate the effectiveness of an educational intervention based on raising the awareness and self-efficacy for pain control among patients with multiple sclerosis during 2015 under the coverage of Isfahan MS Society (IMSS).
2. MATERIALS AND METHODS
This was a quasi-experimental prospective study involving pre- and post -test and a randomized control group. Moreover, 88 patients with MS referred to the Isfahan MS Society (IMSS) were selected randomly as sample through the following formula. The subjects were divided into two groups of intervention (44) and control (44), which were increased to 50 in case a few samples were disqualified.
The MS patients were covered by the Isfahan MS Society (IMSS), had expressed their consent to participate in the study, and were excluded if they missed any of the training sessions.
Confidence level were considered as 95% and power factor as 80% based on the estimation of standard deviation for each variable (score of awareness or self-efficacy in both groups).
The minimum difference of each variable between the two groups was, reflecting a significant difference as 0.6s.
Having obtained the approval of the Research Deputy and Ethical Code 293130 on August 24, 2014, coordination was made with the Isfahan MS Society (IMSS) and the required data were collected. For data collection, a self-structured questionnaire was employed, entailing demographic data such as age, gender, duration of disease, job, education, etc. The second section involved a few Yes/No/I do not Know items designed on a scale ranging from 2-0 points. The negative items were scored inversely. In this regard, 10 items concerned perceived pain self-efficacy designed on a 6-point Likert score. The comparison was facilitated by both awareness and self-efficacy items calculated on a basis of 100.
The validity of the data collection tool was content validity. In this way, the awareness questionnaire was handed to five health education and neurology experts whose opinions were applied within the questionnaire. The self-efficacy for pain control questionnaire was designed through a valid questionnaire known as PSEQ translated by Haghighat et al (13).
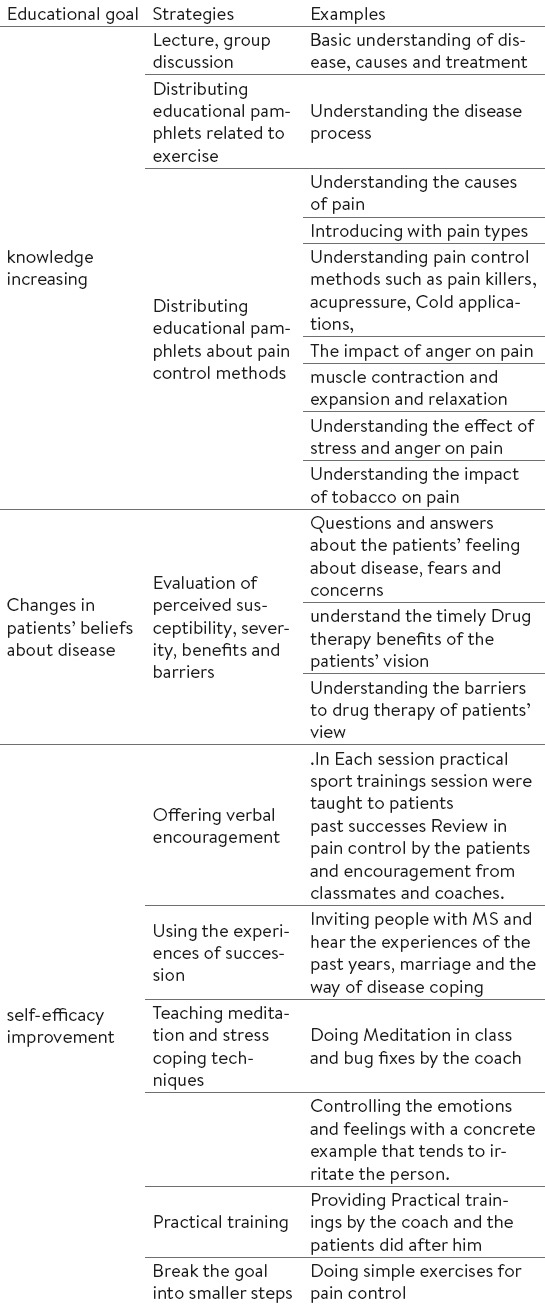
The reliability was evaluated by handing the questionnaire to 15 patients with MS, where the Cronbach’s alpha was calculated to be 0.69. After receiving permission from Isfahan University of Medical Sciences and coordination with the Isfahan MS Society (IMSS), the samples were selected. At first, the questionnaire was completed by 100 patients (intervention and control groups). Then, the subjects in the intervention groups received 4 sessions of 1.5 hour on a weekly basis. During the training sessions, information about the disease, its causes and complications, essential self-care in the lifestyle, stress management, sleep pattern and correct use of medications to prevent and control pain were trained (Table 1). The training involved techniques such as narrowing down the main goal and verbal encouragement to the participants in the classroom. Of these, 47 patients were in the intervention group and 49 patients remained in the control group. The control group did not receive any formal education. After the study, the control group received the necessary training. Before running the training sessions, and then two months later, both groups completed the questionnaires and data were analyzed through SPSS 17. Moreover, the data were analyzed through Mann-Whitney test and descriptive statistics, t-test, ANOVA with repeated observations.
Table 1.
Educational goals, strategies and examples of training sessions for patients with multiple sclerosis
3. RESULTS
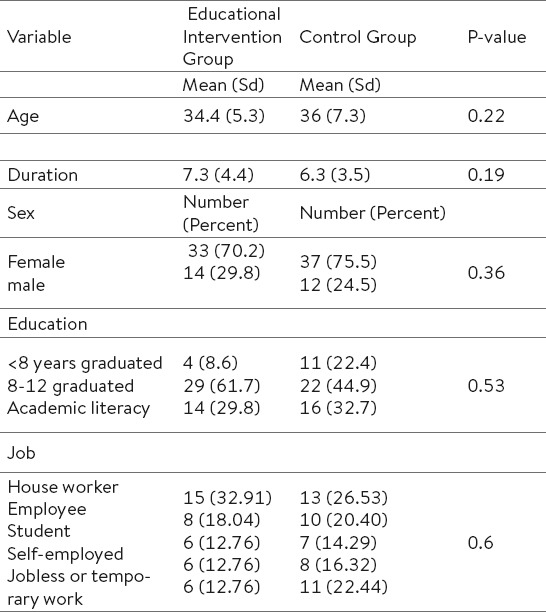
Concerning the questionnaire, 96% of the items were responded. Moreover, 72.9% of participants were women and the rest were men. The mean age of participants was 35.20±6.44 years, where the youngest patient was 18 years old and the oldest was 51. In both groups, the number of women was higher than men (Table 2). The Chi-square test showed that the frequency of gender and occupation of the patients were not significantly different between the two groups (P=0.56). Moreover, the independent T-test showed that the average age and duration of disease were not significantly different between the two groups (Table 2).
Table 2.
The frequency of demographic and contextual characteristic among participants in control and Intervention group
The independent t-test showed that the mean score of knowledge and self-efficacy for pain control were not significantly different between males and females.
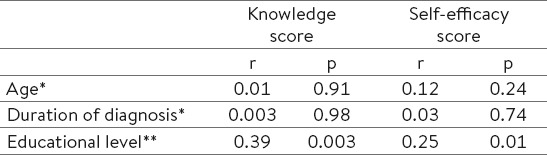
The Mann-Whitney test showed that there was no significant difference between the two groups in terms of education. The Spearman correlation coefficients showed that there was no statistically significant difference between the patients’ education and scores of awareness and self-efficacy (Table 4). In fact, as the education level increases, there will be greater awareness and self-efficacy for pain control. The Pearson’s correlation coefficient showed that age and duration of disease was not significantly correlated with the score of awareness of pain and self-efficacy score (Table 4).
Table 4.
Correlation between age, duration and educational level with pain knowledge and Self-efficacy score. * Pierson correlation, ** Spearman correlation
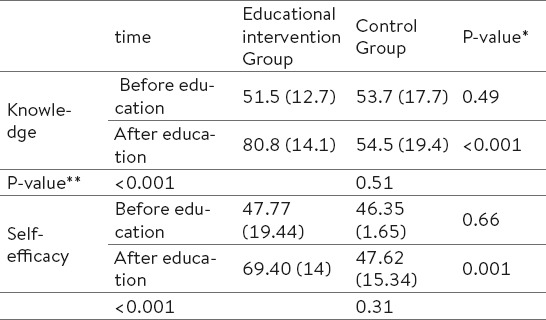
The independent t-test showed that the mean score of knowledge and self-efficacy in patients prior to intervention did not differ significantly between the two groups. After the intervention, however, the mean score of knowledge and self-efficacy was significantly higher in the intervention group than the control group (P<0.001), whereas the mean score of knowledge and self-efficacy in the control group indicated no significant difference before and after the intervention (Table 3).
Table 3.
The mean score of pain knowledge and Self-efficacy between participants in control and Intervention group. *: differences between control and Intervention group **: differences between before and after Intervention
4. DISCUSSION
In this study, since the two groups were not significantly different from each other in terms of demographic characteristics (age, gender, duration of disease, education level), the educational intervention reflected a significant difference between the knowledge and perceived self-efficacy for pain compared to the control group.
The prevalence of pain in MS patients is high. As indicated by Ehde et al. (2015), over 89.6% of patients with MS simultaneously use at least two pharmacological and non-pharmacological methods to relieve their pain. Moreover, 75% of patients refer to at least one health professional for their pain relief during the last 6 months (12). Since other non-pharmacological methods of pain control have been proven fruitful (26, 27). Knowledgeable people about pain control can manage their disease and curtail the physical and psychological consequences. On the other hand, raising knowledge interventions in patients with MS appears to be crucial. As suggested by Solari et al. (2010) in Italy, comprehensive information was delivered to the patients during training in a group by distribution of an interactive CD and booklet and other group through interview by a doctor, so as to assess how knowledge is expanded. Personal information enhanced in two patients. In the current study, the receiving information during a face-to-face interview with a doctor tended to be more knowledgeable until 6 months (28). Another study (2009) suggested that the less frequent use of steroids and fewer doctor visits after participating in 4-hour educational intervention and instructional booklet. These patients reported fewer periods of relapse (29). The study by Heesen et al. (2012) generally demonstrated the impact of educational intervention on improvement of the disease progression in case of MS through the MRI evidence (16). Studies have shown that chronic patients generally tend to have comprehensive information about the disease (28, 30), and since there is no information rising on medical visits, such inadequacy can be resolved through training in times other than appointments. In this study, there was a significant correlation between the education and awareness of disease control methods, where the subjects with university education had the highest awareness about the issue. Other results were consistent with those of the current study (14, 17).
In a study by Stuifbergen et al. (2003) self-efficacy and quality of life improved during an 8-week training course for women to change lifestyle and 2-month telephone follow-up, over three stage of health checkups (31). Educational interventions, even if on the phone based on self-promotion, can bring about physical and emotional improvement among patients with multiple sclerosis (32). Other educational interventions can play a key role in improving self-efficacy and walking ability in these patients. In fact, people with improved self-efficacy can deal with obstacles and challenges more efficiently (32). In a study by Haghighat et al. (2011), it was pointed out there is a link between self-efficacy and pain severity, i.e. people with higher self-efficacy experience less pain (13). Other studies also suggested the usefulness of thoughts control and perceived severity of pain among patients with MS (33).
Although the effects of both biological and psychological factors are not fully known concerning the incidence of MS, various studies have acknowledged the positive effect of educational interventions to improve the adverse effects caused by MS not to mention the improves control skills among patients (16).
5. CONCLUSIONS
Since the studies have shown that higher awareness and self-efficacy can provide are strong predictors of disease control skills in patients with MS, there will be lower subsequent physical and mental complications due to MS. The disease is progressive and sometimes takes a long process. Besides, it is possible to change the disease control skills through training. Hence, it is critical to include self-care programs for MS patients so as to raise knowledge and self-efficacy aimed at better quality of life.
Acknowledgments
The authors find it an obligation to express their gratitude toward the Research Deputy at Isfahan University of Medical Sciences, which funded the project under registration No. 293 130 approved on August 24, 2014. Thanks also go to all the colleagues working in Isfahan MS Society (IMSS) as well as all patients who attended the training sessions, making the implementation of this research possible.
Footnotes
• Limitations: Lack of information about the participants in the study and the perceived severity of the disease were two limitations of the current study.
• Suggestions: It seems essential to design educational interventions for all patients with MS in the Iranian society, so as to curtail the fear and concerns about the disease, and help the patients the less pain and more effectively control their disease.
REFERENCES
- 1.Milo R, Miller A. Revised diagnostic criteria of multiple sclerosis. Autoimmunity Reviews. 2014;13(4–5):518–24. doi: 10.1016/j.autrev.2014.01.012. [DOI] [PubMed] [Google Scholar]
- 2.Noonan CW, Williamson DM, Henry JP, Indian R, Lynch SG, Neuberger JS, et al. The prevalence of multiple sclerosis in 3 US communities. Prev Chronic Dis. 2010;7(1):A12. [PMC free article] [PubMed] [Google Scholar]
- 3.Sahraian MA, Khorramnia S, Ebrahim MM, Moinfar Z, Lotfi J, Pakdaman H. Multiple sclerosis in Iran: a demographic study of 8,000 patients and changes over time. Eur Neurol. 2010;64(6):331–6. doi: 10.1159/000321649. [DOI] [PubMed] [Google Scholar]
- 4.Etemadifar M, Maghzi A-H. Sharp increase in the incidence and prevalence of multiple sclerosis in Isfahan, Iran. Mult Scler J Exp Transl Clin. 2011;17(8):1022–7. doi: 10.1177/1352458511401460. [DOI] [PubMed] [Google Scholar]
- 5.Etemadifar M, Janghorbani M, Shaygannejad V, Ashtari F. Prevalence of multiple sclerosis in Isfahan, Iran. Neuroepidemiology. 2006;27(1):39–44. doi: 10.1159/000094235. [DOI] [PubMed] [Google Scholar]
- 6.Ghaem H, Haghighi AB, Jafari P, Nikseresht A. Validity and reliability of the Persian version of the multiple sclerosis quality of life questionnaire. Neurol India. 2007;55(4):369. doi: 10.4103/0028-3886.33316. [DOI] [PubMed] [Google Scholar]
- 7.Theofilou P, Giannouli V, Kolias S, Tsolaki M. Perception of pain self-efficacy and fatigue in Greek patients with multiple sclerosis: a study protocol. Health Psychol Res. 2015;3(1) doi: 10.4081/hpr.2015.1556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Foley PL, Vesterinen HM, Laird BJ, Sena ES, Colvin LA, Chandran S, et al. Prevalence and natural history of pain in adults with multiple sclerosis: Systematic review and meta-analysis. PAIN®. 2013;154(5):632–42. doi: 10.1016/j.pain.2012.12.002. [DOI] [PubMed] [Google Scholar]
- 9.Nick ST, Roberts C, Billiodeaux S, Davis DE, Zamanifekri B, Sahraian MA, et al. Multiple sclerosis and pain. Neurol Res. 2012;34(9):829–41. doi: 10.1179/1743132812Y.0000000082. [DOI] [PubMed] [Google Scholar]
- 10.Bikmoradi A, Zafari A, Oshvandi K, Mazdeh M, Roshanaei G. Effect of Progressive Muscle Relaxation on Severity of Pain in Patients with Multiple Sclerosis: a Randomized Controlled Trial. Hayat. 2014;20(1):26–37. [Google Scholar]
- 11.Karpatkin H, Napolione D, Siminovich-Blok B. Acupuncture and multiple sclerosis: a review of the evidence. Evid Based Complement Alternat Med. 2014;2014:9. doi: 10.1155/2014/972935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ehde DM, Alschuler KN, Osborne TL, Hanley MA, Jensen MP, Kraft GH. Utilization and patients'perceptions of the effectiveness of pain treatments in multiple sclerosis: A cross-sectional survey. Disabil Health J. 2015;8(3):452–6. doi: 10.1016/j.dhjo.2015.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Haghighat F, Zadhoosh S, Etemadifar M. The relationship between pain self-efficacy and pain intensity in multiple sclerosis patients. International Journal of Behavioral Sciences. 2011;5(1):47–54. [Google Scholar]
- 14.Day MA, Ehde DM, Ward LC, Hartoonian N, Alschuler KN, Turner AP, et al. An Empirical Investigation of a Biopsychosocial Model of Pain in Multiple Sclerosis. Clin J Pain. 2016;32(2):155–63. doi: 10.1097/AJP.0000000000000240. [DOI] [PubMed] [Google Scholar]
- 15.Deibel F, Edwards M, Edwards A. Patients', carers'and providers'experiences and requirements for support in self-management of multiple sclerosis: a qualitative study. Eur J Pers Cent Health. 2013;1(2):457–67. [Google Scholar]
- 16.Heesen C, Köpke S, Kasper J, Poettgen J, Tallner A, Mohr D, et al. Behavioral interventions in multiple sclerosis: a biopsychosocial perspective. Expert Rev Neurother. 2012;12(9):1089–100. doi: 10.1586/ern.12.103. [DOI] [PubMed] [Google Scholar]
- 17.Basak T, Unver V, Demirkaya S. Activities of Daily Living and Self-Care Agency in Patients with Multiple Sclerosis for the First 10 Years. Rehabil Nurs. 2015;40(1):60–5. doi: 10.1002/rnj.153. [DOI] [PubMed] [Google Scholar]
- 18.Patti F, Pozzilli C, Montanari E, Pappalardo A, Piazza L, Levi A, et al. Effects of education level and employment status on HRQoL in early relapsing-remitting multiple sclerosis. Mult Scler. 2007;13(6):783–91. doi: 10.1177/1352458506073511. [DOI] [PubMed] [Google Scholar]
- 19.Osborne TL, Jensen MP, Ehde DM, Hanley MA, Kraft G. Psychosocial factors associated with pain intensity, pain-related interference, and psychological functioning in persons with multiple sclerosis and pain. Pain. 2007;127(1):52–62. doi: 10.1016/j.pain.2006.07.017. [DOI] [PubMed] [Google Scholar]
- 20.Fjeldstad C, Fjeldstad AS, Pardo G. Use of Accelerometers to Measure Real-Life Physical Activity in Ambulatory Individuals with Multiple Sclerosis: A Pilot Study. Int J MS Care. 2015 Sep-Oct;17(5):215–20. doi: 10.7224/1537-2073.2014-037. doi: 10.7224/1537- 2073.2014.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Motl RW, McAuley E, Snook EM, Gliottoni RC. Physical activity and quality of life in multiple sclerosis: Intermediary roles of disability, fatigue, mood, pain, self-efficacy and social support. Psychol Health Med. 2009;14(1):111–24. doi: 10.1080/13548500802241902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rae-Grant AD, Turner AP, Sloan A, Miller D, Hunziker J, Haselkorn JK. Self-management in neurological disorders: systematic review of the literature and potential interventions in multiple sclerosis care. J Rehabil Res Dev. 2011;48(9):1087. doi: 10.1682/jrrd.2010.08.0159. [DOI] [PubMed] [Google Scholar]
- 23.Seyam S, Hidarnia AR, Tavafian SS. Self-care Education through Coping Style for Patients after Heart Surgery. Journal of Isfahan Medical School. 2011;29(135) [Google Scholar]
- 24.O'Hara L, Cadbury H, De Souza L, Ide L. Evaluation of the effectiveness of professionally guided self-care for people with multiple sclerosis living in the community: a randomized controlled trial. Clin Rehabil. 2002;16(2):119–28. doi: 10.1191/0269215502cr478oa. [DOI] [PubMed] [Google Scholar]
- 25.Neill J, Belan I, Ried K. Effectiveness of non-pharmacological interventions for fatigue in adults with multiple sclerosis, rheumatoid arthritis, or systemic lupus erythematosus: a systematic review. J Adv Nurs. 2006;56(6):617–35. doi: 10.1111/j.1365-2648.2006.04054.x. [DOI] [PubMed] [Google Scholar]
- 26.Hartman D. A Comparison of Self-hypnosis versus Progressive Muscle Relaxation in Patients with Multiple Sclerosis and Chronic Pain. Journal of heart-centered therapies. 2010;13(1):104. doi: 10.1080/00207140802665476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Heckman-Stone C, Stone C. Pain management techniques used by patients with multiple sclerosis. J Pain. 2001;2(4):205–8. doi: 10.1054/jpai.2001.23133. [DOI] [PubMed] [Google Scholar]
- 28.Solari A, Martinelli V, Trojano M, Lugaresi A, Granella F, Giordano A, et al. An information aid for newly diagnosed multiple sclerosis patients improves disease knowledge and satisfaction with care. Mult Scler. 2010;16(11):1393–405. doi: 10.1177/1352458510380417. [DOI] [PubMed] [Google Scholar]
- 29.Köpke S, Kasper J, Mühlhauser I, Nübling M, Heesen C. Patient education program to enhance decision autonomy in multiple sclerosis relapse management: a randomized-controlled trial. Mult Scler. 2008;15:96–104. doi: 10.1177/1352458508095921. [DOI] [PubMed] [Google Scholar]
- 30.Tariman JD, Berry D, Cochrane B, Doorenbos A, Schepp K. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Ann Oncol. 2010;21(6):1145–51. doi: 10.1093/annonc/mdp534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Stuifbergen AK, Becker H, Blozis S, Timmerman G, Kullberg V. A randomized clinical trial of a wellness intervention for women with multiple sclerosis. Arch Phys Med Rehabil. 2003;84(4):467–76. doi: 10.1053/apmr.2003.50028. [DOI] [PubMed] [Google Scholar]
- 32.Fraser R, Ehde D, Amtmann D, Verrall A, Johnson KL, Johnson E, et al. Self-management for people with multiple sclerosis: report from the first international consensus conference, November 15 2010. Int J MS Care. 2013;15(2):99–106. doi: 10.7224/1537-2073.2012-044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jensen MP, Ehde DM, Gertz KJ, Stoelb BL, Dillworth TM, Hirsh AT, et al. Effects of self-hypnosis training and cognitive restructuring on daily pain intensity and catastrophizing in individuals with multiple sclerosis and chronic pain. Int J Clin Exp Hypn. 2010;59(1):45–63. doi: 10.1080/00207144.2011.522892. [DOI] [PubMed] [Google Scholar]