

Abstract
Introduction:
Genovarum is a common orthopedic problem. Its optimal prompt treatment is an issue of importance.
Aim:
This study was conducted to determine the radiographic changes in patella bone before and after open wedge high tibial osteotomy.
Material and Methods:
In this quasi-experimental study, 43 patients were enrolled and underwent open wedge high tibial osteotomy and the radiographic and CT-scan indices including Q-Angle, Congruence Angle, Insall-Salvati index, and TTTG were measured and compared before and after surgery.
Results:
The result revealed that all indices including Q-Angle, Congruence Angle, Insull-Salvati index, and TTTG were not significantly differed across the study (P > 0.05). There was no difference between DLFA values before and after the operation (P> 0.05), while MPTA values were significantly different before and after operation (p <0.001).
Conclusions:
Totally it may be concluded that imaging indices are not differed after open wedge high tibial osteotomy and monitoring for them is not necessary and they would have no prognostic role.
Keywords: Genovarum, Surgery, Imaging Indices, Orthopedic, Radiology
1. INTRODUCTION
High tibial osteotomy (HTO) with medial opening wedge has gained in popularity over recent years and is used for the treatment of medial compartmental osteoarthritis (OA) and SONK (1, 2, 3). This procedure is appealing because of the high preservation of the knee joint relative to total knee arthroplasty (TKA) or unicompartmental knee arthroplasty UKA (4, 5).
Medial open-wedge high tibial osteotomy (OWHTO) has been recently used as common method because of the simplicity and the possibility of accurate intraoperative adjustments of the desired correction angle. Moreover, this method is useful because of such advantages including, the maintenance of bone stock, and correction of deformities close to their origins in the proximal tibia without the need for a fibular osteotomy (6, 7).
On the other hand, disadvantages of OWHTO are explained that include graft donor site morbidity and theoretical alteration of the posterior tibial slope. Some authors have reported the absence of tibial slope modification in open-wedge high tibial osteotomy (8, 9). Furthermore, altering the tibial slope may affect in situ cruciate ligament forces and consequently influence both knee stability and kinematics (10). However, there is confusion regarding the effect of a high tibial osteotomy on patellar height for closing and opening wedge osteotomies. Elevation and lowering of the patella have been reported for both techniques, often opposite to mechanical expectations (11, 12, 13). Recently, it has been stated that the opening wedge osteotomy may lower the patella (11, 14). The conventional supratubercle horizontal opening wedge technique does reduce patellar height and increase sagittal tibial slope, because correction is primarily designed to correct the varus malalignment of the knee joint in coronal plane (14). This study was aimed to determine the radiographic changes in patella bone before and after open wedge High tibial osteotomy.
2. MATERIAL AND METHODS
From June 2012 to July 2014, 43 patients were enrolled and underwent open wedge High tibial osteotomy, as well as the radiographic and CT-scan indices including Q-Angle, Congruence Angle, Insall-Salvati index, and TTTG were measured and compared before and after surgery.
2.1. Calculation of the sample size
From June 2012 to July 2014, 43 patients (25 males and 18 females, mean age of 32.1 years) with genovarum were enrolled in university hospitals in Tehran, Iran. This study was approved by the institutional review board at our hospital, and all patients provided informed consent. The data were collected using data collection forms. The form contains personal information such as age, gender and radiological indices and also CT- scans include TTTG, insall -Salvati, Congruence Angle etc (Figure 1).
Figure 1.
Gender distribution of patients
2.2. Surgical techniques
A 8-cm incision was made on the anteromedial aspect of the tibia, centered between the tibial tubercle and the posteromedial tibial cortex. mCL was carefully elevated through the osteotomy site just on the proximal to the tibial tubercle, and the medial surface of tibia was completely exposed with periosteum elevator. Initially, a Guide pins Kirschner 10 was placed in lateral ward toward fibular head. Then, it was controlled using imaging and osteotomy was also performed under the Guide Pin. The tibial including anterior and posterior cortex was cut. When cutting is completed, patella tendon is at risk. Therefore, we have to be careful about that. Lateral cortex must also be safe the opening of the osteotomy site on the paper directly indicated the necessary correction angle. Bone bridges with base sizes matching the amount required for planned correction was placed on the anterior and posterior part. Amount of opened site in the posterior part is more important than anterior. To control stability of posterior tibial slope and osteotomy site, locking plate was used (Figure 2, 3, 4).
Figure 2.
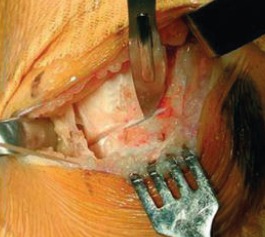
Incision of the superficial medical collateral ligament at the level of the osteotomy
Figure 3.
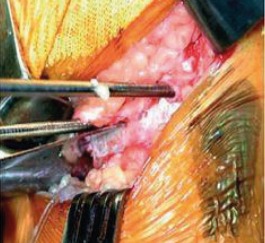
The tibial cut is performed underneath tow guide pins introduced medially
Figure 4.

Control of the correct position of the guide pins with imaging identifier the pins should be introduced from a medial direction and be just superior to the head of the fibula laterally
2.3. Statistical analysis
SPSS software 11.5 (SPSS Inc., Chicago, IL, USA) was applied in current study. Paired sample t-test was used to evaluate difference in ‘before-after’ study. Differences were significant at P<0.05.
3. RESULTS
In the present study, a total of 43 patients were evaluated, based on the results mean age of patents was 32.1 years (SD = 6.11 years). 25 cases were female (58.1%) and 18 were male (41.9 %), (Figure 1). There was no difference between LDFA values before and after the operation (P > 0.05), while MPTA values were significantly different before and after operation (p < 0.001). Our findings indicated that there was no significant difference between the amount of insall–Salvati, Q-Angle and Congruence Angle before and after surgery (P > 0.05). Moreover, no statistically significant difference was found between the values of TT-TG before and after surgery (P > 0.05).
4. DISCUSSION
Several proximal tibial osteotomy techniques are described and traced in their development. Other studies have been indicated that high tibial osteotomy result in confusion regarding whether the patella is raised or lowered, and the effects of these osteotomies on tibial slope and patellar tendon length are not clear (14, 1, 5, 16). Recently, it has been stated that the opening wedge osteotomy may lower the patella (11, 14). The important point in this process is that the mechanical axis of the lower limbs must be corrected, as well as putting extensor mechanism and patella bone in the right position. This produce the greatest possible general benefit for the patient and its side effect falls, reaching its lowest levels, because if these points are not met, contribute to the development of patella femoral pain and also patella lateral movement will be created. This study was conducted to determine the radiographic changes in patella bone before and after open wedge high tibial osteotomy (Figure 5). The osteotomy was performed at the top of the tibia tubercle. Furthermore, we evaluated the amount of displacement of the tibia tubercle along with TT-TG that is relatively accurate criteria. The results indicated that, there was no significant change in the tibial tubercle displacement. In this study, the index of insall – Salvati was also measured that it was not shown significant change; of course the follow-up time was short.
Figure 5.
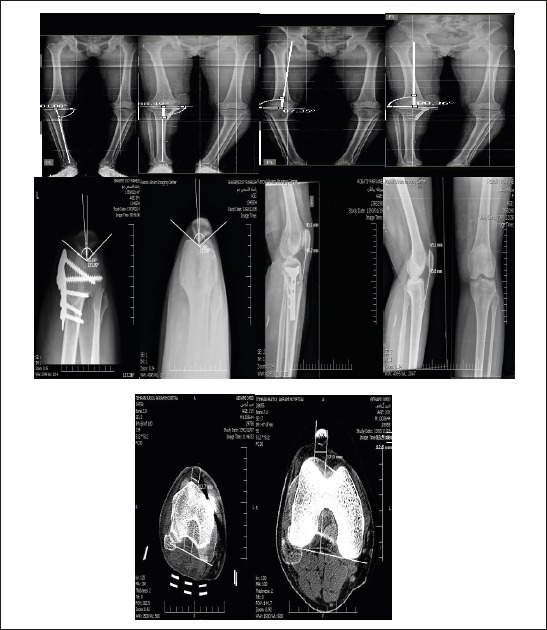
Radiographic findings of patellar dislocation before and after medial opening wedge high tibial osteotomy
Moreover, we measured clinically Q angle changes that no significant difference was found in our study that is in agreement with other studies (8, 9). It was shown that using medial opening wedge HTO does not cause marked changes in other parts of the knee, and displacement of the lateral tubercle is not enough to affect the Q angle. As a matter of fact, the extensor mechanism will be in good condition following surgery, and does not require additional action to correct.
On the other hand, this operation is easier when compared with other osteotomy techniques, as well as, surgical time is shorter, and leading to less soft-tissue damage. However, there are contradictory reports that must be interpreted with caution, because most often these studies have limitations such as small numbers of patients and are very rarely comparative (17, 18, 19).
5. CONCLUSION
It can be inferred that there was no significant difference between radiographic indices of the two phases before and after the opening wedge high tibial osteotomy. Therefore, monitoring of them doesn’t appear necessary to predict the outcomes of the operation. TT-TG clearly showed the lack of this change using the CT- scan imaging techniques. Further studies are required to confirm the findings of this study.
Footnotes
• Conflict of interest: none declared.
REFERENCES
- 1.Hernigou P. Open wedge tibial osteotomy: combined coronal and sagittal correction. Knee. 2002;9:15–20. doi: 10.1016/s0968-0160(01)00111-9. [DOI] [PubMed] [Google Scholar]
- 2.Moghtadaei M, Farahini H, Faiz SH, Mokarami F, Safari S. Pain Management for Total Knee Arthroplasty: Single-Injection Femoral Nerve Block versus Local Infiltration Analgesia. Iran Red Crescent Med J. 2014;16(1):e13247. doi: 10.5812/ircmj.13247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ozalay M, Ozkoc G, Circi E, Akpinar S, Hersekli MA, Uysal M, Cesur N. The correlation of correction magnitude and tibial slope changes following open wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2008;16:948–951. doi: 10.1007/s00167-008-0589-8. [DOI] [PubMed] [Google Scholar]
- 4.Brouwer RW, Bierma-Zeinstra SM, van Raaij TM, Verhaar JA. Osteotomy for medial compartment arthritis of the knee using a closing wedge or an openingwedge controlled by a Puddu plate. A one-year randomised, controlled study. J Bone Joint Surg B. 2006;88:1454–1459. doi: 10.1302/0301-620X.88B11.17743. [DOI] [PubMed] [Google Scholar]
- 5.Coventry MB, Ilstrup DM, Wallrichs SL. Proximal tibial osteotomy. A critical long-term study of eighty-seven cases. J Bone Joint Surg Am. 1993;75:196–201. doi: 10.2106/00004623-199302000-00006. [DOI] [PubMed] [Google Scholar]
- 6.Maquet P. Valgus osteotomy for osteoarthritis of the knee. Clin Orthop. 1976;143:8–120. [PubMed] [Google Scholar]
- 7.Staubli AE, De Simoni C, Babst R, Lobenhoffer P. TomoFix: a new LCP concept for open wedge osteotomy of the medial proximal tibia – early results in 92 cases. Injury. 2003;34:55–62. doi: 10.1016/j.injury.2003.09.025. [DOI] [PubMed] [Google Scholar]
- 8.Sariali E, Catonne Y. Modification of tibial slope after medial openingwedge high tibial osteotomy: clinical study and mathematical modelling. Knee Surg Sports Traumatol Arthrosc. 2009;17:1172–7. doi: 10.1007/s00167-008-0717-5. [DOI] [PubMed] [Google Scholar]
- 9.Chae D, Shetty GM, Lee DB, Choi HW, Han SB, Nha KW. Tibial slope and patellar height after opening-wedge high tibial osteotomy using autologous tricortical iliac bone graft. Knee. 2008;15:128–33. doi: 10.1016/j.knee.2007.11.001. [DOI] [PubMed] [Google Scholar]
- 10.Agneskirchner JD, Hurschler C, Stukenborg-Colsman C, Imhoff AB, Lobenhoffer P. Effect of high tibial flexion osteotomy on cartilage pressure and joint kinematics: a biomechanical study in human cadaveric knees. Winner of the AGADonJoy Award. Arch Orthop Trauma Surg. 2004;124:575–584. doi: 10.1007/s00402-004-0728-8. [DOI] [PubMed] [Google Scholar]
- 11.Schro¨ter S, Lobenhoffer P, Mueller J, Ihle C, Sto ¨ckle U, Albrecht D. [Changes of patella position after closed and open wedge high tibial osteotomy: review of the literature][in German] Orthopade. 2012;41:186, 188–194. doi: 10.1007/s00132-011-1872-9. [DOI] [PubMed] [Google Scholar]
- 12.Farahini H, Moghtadaei M, Bagheri A, Akbarian E. Factors influencing range of motion after total knee arthroplasty. Iran Red Crescent Med J. 2012;14(7):417–21. [PMC free article] [PubMed] [Google Scholar]
- 13.Kesmezacar H, Erginer R, Ogut T, Seyahi A, Babacan M, Tenekecioglu Y. Evaluation of patellar height and measurement methods after valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2005;13:539–544. doi: 10.1007/s00167-004-0572-y. [DOI] [PubMed] [Google Scholar]
- 14.El Amrani MH, Levy B, Scharycki S, Asselineau A. Patellar height relevance in opening-wedge high tibial osteotomy. Orthop Traumatol Surg Res. 2010;96:37–43. doi: 10.1016/j.rcot.2009.11.003. [DOI] [PubMed] [Google Scholar]
- 15.Portner O, Pakzad H. The evaluation of patellar height: a simple method. J Bone Joint Surg Am. 2011;93:73–80. doi: 10.2106/JBJS.I.01689. [DOI] [PubMed] [Google Scholar]
- 16.Gaasbeek R, Welsing R, Barink M, Verdenschot N, van Kampen A. The influence of open and closed high tibial osteotomy on dynamic patellar tracking: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2007;15:978–984. doi: 10.1007/s00167-007-0305-0. [DOI] [PubMed] [Google Scholar]
- 17.El-Azab H, Halawa A, Anetzberger H, Imhoff AB, Hinterwimmer S. The effect of closed- and open-wedge high tibial osteotomy on tibial slope: a retrospective radiological review of 120 cases. J Bone Joint Surg Br. 2008;90:1193–7. doi: 10.1302/0301-620X.90B9.20688. [DOI] [PubMed] [Google Scholar]
- 18.Bito H, Takeuchi R, Kumagai K, Aratake M, Saito I, Hayashi R. Opening-wedge high tibial osteotomy affects both the lateral patellar tilt and patellar height. Knee Surg Sports Traumatol Arthrosc. 2010;18:955–60. doi: 10.1007/s00167-010-1077-5. [DOI] [PubMed] [Google Scholar]
- 19.Coventry MB. Upper tibial osteotomy for gonarthrosis: the evolution of the operationin the last 18 years and long term results. Orthop Clin North Am. 1979;10:191–210. [PubMed] [Google Scholar]