

Abstract
Purpose:
Despite the importance of patients believes as one of the most important predictors of treatment adherence behavior, it is rarely considered in numerous studies. Then the current survey was aimed to develop and study the beliefs about medicines questionnaire (BMQ) in patients with hypertension.
Materials and Methods:
The BMQ developed by Horn and et al. was used in the current study. This questionnaire included 18 questions in both public and private beliefs regarding drug. Face and content validity of the tool was investigated using expert’s panel. In final, aforementioned tool was tested in 612 participants. To explore structure validity and internal consistency, exploratory and confirmatory factor analysis and alpha coefficient was conducted. To evaluate the final validity of instrument, the mean score of the beliefs about medicines of patients with appropriate medication adherence were compared to patients without medication adherence.
Results:
The mean age of patients was 44.08 ± 10.38 years. Women were 314 of participants. Calculated face validity by the impact score for each item indicated that all the items of the questionnaire had the impact score of more than 1.5. In total, all items had scored higher than 0.79 by considering 18 items for content validity. The average of content validity index for the questionnaire was 0.93. Load of factors were in the range of 0.51 to 0.79. Four items explained % 57 of the total variance. Comparison of all instrument items in the two groups showed that patients with good adherence had higher score in 15 items (% 83 of all items).
Conclusion:
The findings suggested that the BMQ in patients with hypertension as a valid and reliable instrument can be used to evaluate the patients’ medication adherence.
Keywords: Belief, BMQ, Medication adherence, Hypertension
1. INTRODUCTION
Advances in diagnosis and treatment of high blood pressure play an important role in reducing deaths caused by coronary heart disease and stroke in industrialized countries (1, 2). Modern approach in the management of hypertension is medication approach, and blood pressure medicines are the most commonly drugs prescribed by doctors. Evidence showed that drug treatment of blood pressure can diminish diastolic blood pressure by 5 to 6 mmHg, and then it can likely increase the quality of life, and also decrease the risk of coronary heart disease by 20 to 25 percent and stroke by 35 to 40 per cent (3). Studies conducted in Iran show 48.1% patients with high blood pressure are treated and 21.3% only is controlled (4). It is estimated that only 57 percent of patients with high blood pressure have controlled blood pressure across the world (5). In the recent years, Iran statistics report provides a worse situation in the way that the prevalence of hypertension in Tehran suggested that only 36% of patients with hypertension used blood pressure drugs (23% of men and 43% of women) that only 40% had normal blood pressure (45% of men and 39% of women) (6). It is supposed that about 50% of patients, who have received blood pressure drugs, do not continue treatment within a year (7). The researcher’s attention focused on adherence to drug consumption in patients with hypertension due to the low number of patients consuming blood pressure medications as well as lack of control of significant amounts of blood pressure. Poor adherence to drug therapy is a major obstacle to achieve afore mentioned health outcomes; moreover, non-adherence that is one of the main factors of failures to achieve normal blood pressure, refractory blood pressure and sudden loss of control is emphasized (8). There are many reasons for non-adherence to drug therapy of blood pressure. Evidence emphasized on the possible influence of patient, service providers and providing services in non- adherence. Numerous theories and cognitive models have been applied to explain the behavior of adherence to treatment that suggested that patient’s beliefs have been regarded as one of the most important predictors of adherence behavior (9, 10). Beliefs about medicines can be categorized by general and special beliefs that are associated with different diseases and cultural groups. Despite the importance of this belief in adherence to the treatment of blood pressure, the current study showed that the role of beliefs has been rarely considered in Iranian society patients that might be caused by the lack of appropriate instrument in relevance with demographic and cultural characteristics of Iran society. Thus the current survey was aimed to develop and study the beliefs about medicines questionnaire (BMQ) in patients with hypertension.
2. MATERIALS AND METHODS
2.1. Participants
In a cross-sectional survey, 612 patients with hypertension attended to health center of Isfahan city were studied. There are 11 health centers in Isfahan city. A multi-stage sampling method was conducted in the way that 4 health centers were randomly selected and a list of patients with hypertension was provided those had a file in the centers and were eligible to be included in the study, then, samples with equal volume were selected using systematic random sampling method from each center. Inclusion criteria were as follow: 1) diagnosis of hypertension, 2) periodical follow-up of treatment for 1 year at least, 3) aged >18 and 60> years, 4) being literate and 5) consumption of a reducing hypertension drug at least. Exclusion criteria were considered as: 1) having a special mental disease or 2) unmotivated to participate in the study.
2.2. Instrument
Demographic characteristics including marital status, education, family history of hypertension, duration and type of treatment.
BMQ includes 18 questions in the two parts of general and specific beliefs about drug. The specific part explores patients’ beliefs about the medications prescribed for a specific condition (Beliefs about hypertension). The aforementioned part consists of two sub scales in terms of personal beliefs about need for medication to control blood pressure (specific- necessity) and concerns about the adverse consequences (specific- concerns) of drug (5 states). The questions of general part investigate total patient’s beliefs toward drugs. The general consists of two sub scales includes total belief that assess individuals belief regarding doctors procedure to use drugs (General- Overuse) and damage scale that test the beliefs of patients about drugs harmfulness (General- Harm).
Each question was scored based on 5 point Likert scale (1-strongly disagree, 2-disagree, 3- no comments, 4-agree, 5- completely agree). Scale of specific beliefs (necessity & concern) had 5 questions and ranged 5 to 25. Higher scores of specific beliefs sub scale of need indicated the stronger perception to use drug to maintain health compared to personal need. Higher scores of specific beliefs sub scale of specific- concerns indicated more concern about adverse effect of drug consumption. In general beliefs, sub scales of general-overuse and general- Harm had 5 questions and scored 4 to 20. Higher scores of general beliefs sub scale of general- Harm demonstrated more negative perspective to all drugs, and considering drugs as an addictive and toxic substance, moreover, higher scores in general-overuse sub scales indicated more negative opinions in terms of drug prescription methods. Morisky Medication Adherence Scale (MMAS) was used to study adherence to treatment in the current survey. This scale is one of the most common structured self-report instruments to study medication adherence in chronic diseases (11-14). MMAS is a reliable instrument (alpha = 0.83) in the evaluation of adherence to treatment that is significantly associated with blood pressure control (13). Sensitivity and specificity of MMAS are 93% and 53%, respectively. It has 8 questions with a range of 0 to 8. MMAS scored as follow: 2 < low adherence, 1 or 2 average adherences and 0 high adherences (15).
2.3. Translation of BMQ
In this study, BMQ2 was used. This questionnaire was developed by Hornet and et al. by using of collecting and reviewing all available tools in the related field. Standard method was considered in translation and back translation process for the cultural adaptation of questionnaires (19). At first, questionnaire translation process was implemented by the two bilingual translators from English to Persian, independently. There was little difference in the translation that researcher reconciled them. Then, back- translation process was conducted. In the next phase, a bilingual translator (different from the first translators) translated questionnaires into English. This process was continued until all the differences between the items were matched.
2.4. Face validity
Face validity was evaluated in both quantitative and qualitative phases. In the qualitative stage, face validity measurement, relevancy, ambiguous and difficulty were studied by 13 specialists. Researcher used specialist’s view of points to correct items. In the second phase (quantitative stage), impact score was calculated. At this stage, the experts were asked to categorize items of questionnaire based on a 5 point Likert scale ranged from very important (score 5) to never important (score 1). Questions with impact score higher than 1.5 were suitable for further analysis and were also retained.
2.5. Content validity
To evaluate content validity, qualitative and quantitative methods were used (16). In the qualitative method some of specialists were interviewed and asked to present their comments in terms of compliance with grammar, use of appropriate and understandable words, proper scoring for the completion of tool, proportionality of selected scales and items placement in their proper place. After collecting expert’s comments, researcher provided final version of instrument with regards to the collected data. To determine content validity, content validity rate (CVR (and content validity index (CVI) were investigated for 18 items. To do this, comments of 13 experts and scholars in the related fields were taken. To assess the content validity rate, experts were asked to comment on items related to structures in the form essential, useful but non-essential and non-essential. In final, CVR was estimated with regards to the experts numbers and the formula of CVR= ne–(n/2) /(n/2) for each items. In this formula “n” means the total number of professionals who was participated in this stage to assess the validity and “ne” means number of specialists who voted the necessary options.
2.6. Construct validity
In the current survey, exploratory factor analysis with principal components analysis and varimax rotation was used to assess construct validity. To assess the adequacy of sample size and the correlation between the variables, Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity was used. In this study, turning point of 0.4 was considered as the minimum of required load factor to maintain each item extracted from factor analysis.
Maximum likelihood analysis was used to measure the structure validity and items conformity of original version of questionnaire with Persian version. Structure validity measurement was aimed to response to this question that to what extent the structure of the questionnaire has compliance with the primary goal of questionnaire. This model is evaluated by Chi-squared test, the comparative fit index (CFI), the normed fit index (NFI), and the root mean square error of approximation (RMSEA).
2.7. Reliability
Internal consistency was conducted to test reliability of the questionnaire. Internal consistency means a degree that questions summarized by an index and correlated with each other that Cronbach’s alpha coefficient is the most common method for its calculation. According to this method, a reliable instrument has Cronbach’s alpha coefficient greater than or equal to 0.7 (17). To determine the internal consistency, Item-total Correlation method was used that measures the correlation of each question with instrument, and also decide to eliminate some of questions.
2.8. The validity of final scale
To test final scale validity, the mean score of the beliefs about medicines of patients with good medication adherence was compared with patients with poor medication adherence with assumption of higher score of beliefs in patients with good medication adherence, therefore, the mean score of medication adherence was applied based on MMAS questionnaire.
2.9. Procedure
Prior to the survey, the current study was confirmed by the ethical committee of Isfahan University of Medical Science (project no 393777), moreover, informed consent form and data confidentiality as well as being voluntary to exclude from the study were considered by the project researcher. Self-administered questionnaire was completed by the patients. To prevent data missing, all parts of the questionnaire was controlled by the researcher and returned to the patients if they were incomplete. All questionnaires were completed in 2 months.
2.10. Analysis
Data were analyzed using SPSS software (ver.21) through descriptive methods, Cronbach’s alpha, Pearson correlation, KMO, Bartlett’s test of sphericity and Varimax rotation. To investigate structure validity, AMOS software and Chi-squared test, CFI, NFI, and RMSEA were executed.
3. RESULTS
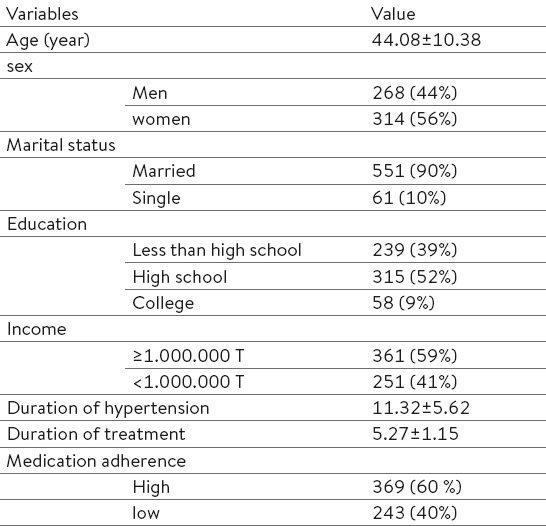
All 612 participants were studied. The mean age of patients was 44.08 ± 10.38 years and 314 of patients were women, 10% was single, 52% had high school degree, and, in brief, 40% of patients had good medication adherence (Table 1). Face validity tested for all items using impact score showed that all items had impact score higher than 1.5. According to 18 explored items by the specialist’s comments about content validity, all questionnaire items were scored higher than 0.79. The average index of content validity of questionnaire was 0.93.
Table 1.
Demographic characteristics of included patients
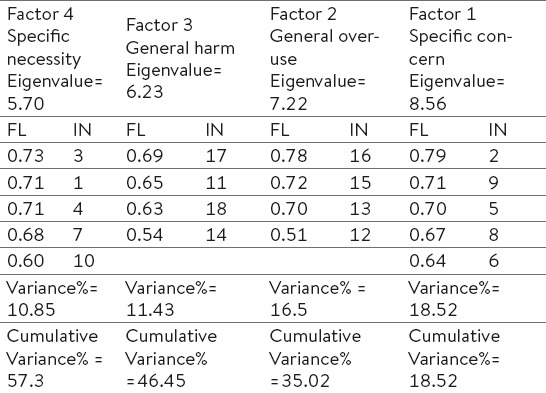
KMO test was used to investigate adequate sample size before implementing exploratory factor analysis. KMO was 0.89 that suggested adequate sample size to conduct factor analysis. Bartlett’s test of sphericity was also significant (P< 0.001, 8453.45) that reported appropriate correlation to analyze variables. Exploratory factor analysis was conducted on 18 items and it found that items were collected in 6 factors with special value greater than one. According to the four factor structure of the original questionnaire with varimax rotation, structure validity was studied by limiting to 4 factors. Results of the factor analysis for the developed scale in the form of four factors with 18 items showed in Table 1. One item only had a load factor greater than 0.4 in more than two different factors. Load factors were in the range of 0.51- 0.79. In general, four factors explained 57% of the total variance (Table 1).
Exploring indicator variables that formed BMQ was done using confirmatory factor analysis and by considering four indexes of fitness that all of indexes confirmed the proposed model. Chi-square was 6.425 and p= 0.45 that reported an appropriate fitness between the proposed model and collected data. CFI and NFI are the relative fitness that compare model with theoretical model associated with null model with acceptable value of 0.95. CFI and NFI were 0.958 and 0.962, respectively that indicated the ideal fitness of the model. RMSEA measures the difference between the sample coefficients and society coefficients that suggest closer value to zero indicates the better fitness of the model. RMSEA was 0.073 that showed moderate fitness.
Reliability was tested after conducting factor analysis using Cronbach’s alpha for the questionnaire and for each factor. Total reliability of instrument was 0.91 and 0.85 – 0.93 for four factors (Table 3). The correlation of each question with total correlation was reported in Table 4.
Table 3.
Cronbach’s Alpha Reliability Coefficients and Item-total Correlations of the Components, A: Alpha values, r: Item-total correlation
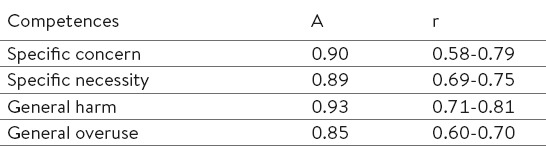
Table 4.
Item’s Total Statistics of BMQ
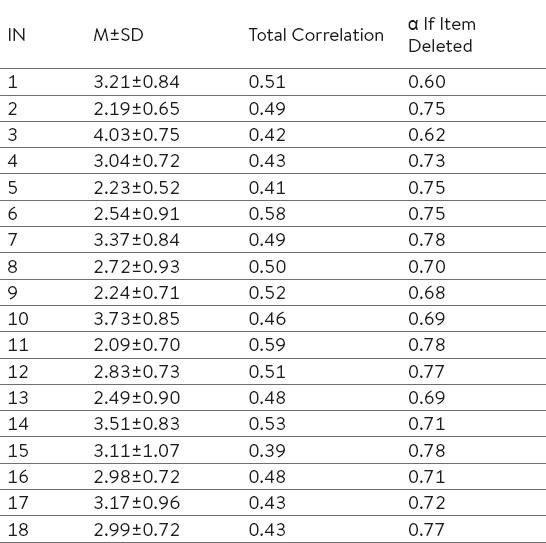
Table 2.
Factor Loadings of CIPP Scale. IN: Item Number, FL: Factor loading
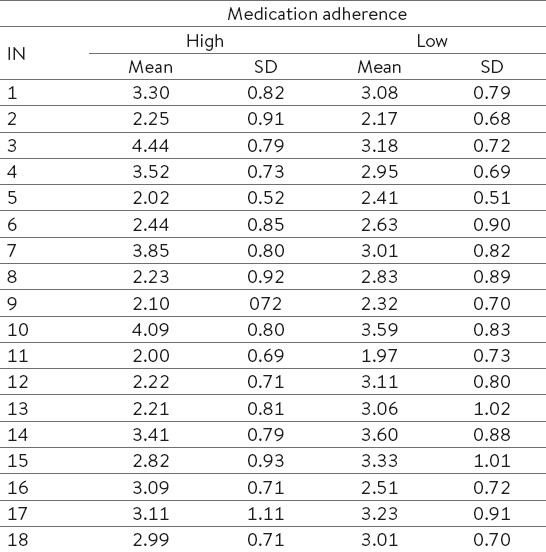
In the current study, the score of patients’ beliefs about medicines was compared in good adherence to poor adherence group. The average score of adherence in all patients was 3.05 ± 0.29. The results reported that patients with good adherence had higher score in BMQ compared with patients with low adherence. Comparison of all items between the two groups showed that patients with good adherence had higher score in 15 items (83% of items) (Table 5).
Table 5.
Mean scores ± SD on the BMQ, comparing non-adherent with adherent patients
4. DISCUSSION
Validity and reliability of BMQ was tested in patients with hypertension because of the poor adherence of patients to prescribed drugs; moreover, with regard to the chronic and serious nature of this disease, lack of cooperation and adherence might be risky and it is so necessary to follow and scrutiny. While, many studies have been introduced their patient’s believes about medication as one of the most important predictors of drug treatment and ultimate success in controlling of disease. In this study, exploratory factor analysis showed four-factor structure of the BMQ in the two categorization including specific beliefs about prescribed medicines in hypertensive patients and public opinion about all drugs. Confirmatory factor analysis was also approved the above mentioned structure. Meanwhile, the internal consistency and correlation of each question with the measurement tool showed that mentioned instrument achieved the consistent scores over time which points to the reliability of the tool for exploring beliefs about medicines in patients with hypertension in Iranian society. Special beliefs in the current questionnaire were about drug requirements to keep health (special beliefs–necessity) and concerns about the drug (special beliefs- concerns).
The construct of special beliefs- necessity indicates the perceived rule toward protection against deterioration of the patient’s current and future health. The construct of special beliefs- concerns investigates patient concerns regarding the use of blood pressure drugs in both the emotional aspect (need to blood pressure medication worry me) and cognitive (medications are a mystery to me).
As many studies suggested, although patients believed in effective role of drugs in treating of a variety of diseases, however, when several studies have investigated the beliefs about medicines in patients, it was found that strong beliefs about the potential harms of drugs hid beliefs about benefits. It seems likely persuade researchers to make a questionnaire for exploring negative beliefs in general beliefs. In general beliefs construct, two sub scales explores the nature of drugs in general–harms and general- Overuse of drugs by doctors.
Given the nature of hypertension in various studies, poor adherence to prescribed medicines is a major cause of treatment failure (18). Criterion validity of the final questionnaire showed that this tool had a good ability to separate Iranian patients adheres to drug therapy.
The current study had some limitations as the same as other survey. Despite the patients attending in health centers, it is not possible to generalize these samples to the entire community. Researcher was not able to test predictive validity because of inaccessibility of reliable tool in terms of beliefs about medicines. Due to the cross-sectional study, we were not capable to investigate causal relationship between the medication adherence and beliefs about medicines in patients with hypertension, then the current correlation indicate only to the existed relationship and prospective studies are needed to study this relationship. To increase the discriminant validity (a limitation of current survey), it suggests to use classified sampling with more samples.
5. CONCLUSIONS
Despite of these limitations, results of face, content, construct, criterion validity and reliability of BMQ was confirmed to use in patients with hypertension. The current results finally approved the usability of BMQ in Iranian patients with hypertension for prescribed drugs and, in general, for all drugs. This questionnaire is a flexible tool to study beliefs about medicines in various diseases as belied by the developers of the questionnaire. The researchers recommend to asses validity and reliability and to use the questionnaire for investigating other diseases as well.
Footnotes
• Conflict of interest: none declared.
REFERENCES
- 1.Malekzadeh MM, Etemadi A, Kamangar F, Khademi H, Golozar A, Islami F, et al. Prevalence, awareness and risk factors of hypertension in a large cohort of Iranian adult population. Journal of hypertension. 2013;31(7):1364–71. doi: 10.1097/HJH.0b013e3283613053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Namayandeh S, Sadr S, Rafiei M, Modares-Mosadegh M, Rajaefard M. Hypertension in Iranian urban population, epidemiology, awareness, treatment and control. Iranian journal of public health. 2011;40(3):63–70. [PMC free article] [PubMed] [Google Scholar]
- 3.Whiteley JA. Exploring predictors of medication adherence in hypertensive African Americans: What is the role of psychosocial predictors?[Ed.D.] Ann Arbor: Teachers College, Columbia University. 2006 [Google Scholar]
- 4.Barikani Ameneh Sf. Prevalence of hypertension among women aged +30 in Minoodar region of Qazvin in 2009. The Journal of Qazvin University of Medical Sciences. 2009;14(1):41–8. [In Persian] [Google Scholar]
- 5.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560–72. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- 6.Azizi F, Ghanbarian A, Madjid M, Rahmani M. Distribution of blood pressure and prevalence of hypertension in Tehran adult population: Tehran Lipid and Glucose Study (TLGS) 1999-2000. Journal of human hypertension. 2002;16(5):305–12. doi: 10.1038/sj.jhh.1001399. [DOI] [PubMed] [Google Scholar]
- 7.Shermock KM. Impact of continuity of care and provider factors on medication adherence in patients with hypertension [Ph.D.] Ann Arbor: The Johns Hopkins University; 2009. [Google Scholar]
- 8.Phillips LS, Branch WT, Cook CB, Doyle JP, El-Kebbi IM, Gallina DL, et al. Clinical inertia. Annals of internal medicine. 2001;135(9):825–34. doi: 10.7326/0003-4819-135-9-200111060-00012. [DOI] [PubMed] [Google Scholar]
- 9.Mann DM, Ponieman D, Leventhal H, Halm EA. Predictors of adherence to diabetes medications: the role of disease and medication beliefs. Journal of behavioral medicine. 2009;32(3):278–84. doi: 10.1007/s10865-009-9202-y. [DOI] [PubMed] [Google Scholar]
- 10.Maguire LK, Hughes CM, McElnay JC. Exploring the impact of depressive symptoms and medication beliefs on medication adherence in hypertension - a primary care study. Patient education and counseling. 2008;73(2):371–6. doi: 10.1016/j.pec.2008.06.016. [DOI] [PubMed] [Google Scholar]
- 11.Al-Qazaz H, Hassali MA, Shafie AA, Sulaiman SA, Sundram S, Morisky DE. The eight-item Morisky Medication Adherence Scale MMAS: translation and validation of the Malaysian version. Diabetes research and clinical practice. 2010;90(2):216–21. doi: 10.1016/j.diabres.2010.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Oliveira-Filho AD, Barreto-Filho JA, Neves SJ, Lyra Junior DP. Association between the 8-item Morisky Medication Adherence Scale (MMAS-8) and blood pressure control. Arquivos brasileiros de cardiologia. 2012;99(1):649–58. doi: 10.1590/s0066-782x2012005000053. [DOI] [PubMed] [Google Scholar]
- 13.Lee GK, Wang HH, Liu KQ, Cheung Y, Morisky DE, Wong MC. Determinants of medication adherence to antihypertensive medications among a Chinese population using Morisky Medication Adherence Scale. PloS one. 2013;8(4):e62775. doi: 10.1371/journal.pone.0062775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wang Y, Kong MC, Ko Y. Psychometric properties of the 8-item Morisky Medication Adherence Scale in patients taking warfarin. Thrombosis and haemostasis. 2012;108(4):789–95. doi: 10.1160/TH12-05-0368. [DOI] [PubMed] [Google Scholar]
- 15.Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. Journal of clinical hypertension (Greenwich, Conn) 2008;10(5):348–54. doi: 10.1111/j.1751-7176.2008.07572.x. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 16.Polit DF, Beck CT. The content validity index: are you sure you know what's being reported? Critique and recommendations. Research in nursing & health. 2006;29(5):489–97. doi: 10.1002/nur.20147. [DOI] [PubMed] [Google Scholar]
- 17.Santos JRA. Cronbach's alpha: A tool for assessing the reliability of scales. Journal of extension. 1999;37(2):1–5. [Google Scholar]
- 18.Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient preference and adherence. 2012;6:613–22. doi: 10.2147/PPA.S34704. [DOI] [PMC free article] [PubMed] [Google Scholar]