

Abstract
Introduction
Although bilateral facial nerve palsy is a rare condition, its etiology is more detectable than the unilateral type. A temporal bone fracture is one cause of bilateral facial nerve palsy, contributing in 3% of the cases.
Case Presentation
Here, we report the case of a 35-year-old man complaining of bilateral incomplete eye closure, two weeks after a closed head injury caused by a motor vehicle accident.
Conclusions
The high resolution computed tomography findings revealed a bilateral temporal bone fracture line, which extended to the fallopian canal. With regard to treatment, near complete recovery was obvious after two weeks of treatment with oral corticosteroids. Overall, bilateral facial palsy is hard to diagnose; therefore, clinical suspicion and the early detection of facial nerve injuries is necessary for good nerve recovery in temporal bone fractures.
Keywords: Bilateral Facial Paralysis, Fracture, Temporal Bone
1. Introduction
Facial palsy is a common medical condition, with an incidence of 20 - 25 cases per 100,000 individuals per year (1). Idiopathic facial palsy, also known as Bell’s palsy, is the most common cause, while simultaneous bilateral facial palsy, defined as the involvement of both hemifacies in less than a 4-week period, is a rare condition and occurs one in 5 million cases per year (2, 3). The separate diagnoses are difficult to make due to the lack of facial asymmetry (4); however, the etiologies of the bilateral cases include systemic diseases, neuromuscular problems, and vascular, infectious, toxic, and traumatic problems, while some cases remain idiopathic (5). A temporal bone fracture is one cause of bilateral facial nerve palsy, contributing in 3% of the cases (6, 7).
2. Case Presentation
A 35-year-old man presented to the ear, nose, and throat (ENT) clinic complaining of an inability to close his eyes, even with effort. He had no previous significant medical history, with the exception of a 10 days previous car accident, which resulted in an intracranial hemorrhage and a 2-day coma. He was discharged 2 days previously with no other remarkable side effects. Upon physical examination, an expressionless and masked face was obvious, and the patient exhibited no forehead movement or mouth motion (House-Brackmann 4). The otoscopic examination showed no clot, active bleeding, canal fractures, or cerebral spinal fluid otorrhea. Hemotympanums, with no perforations, were seen bilaterally.
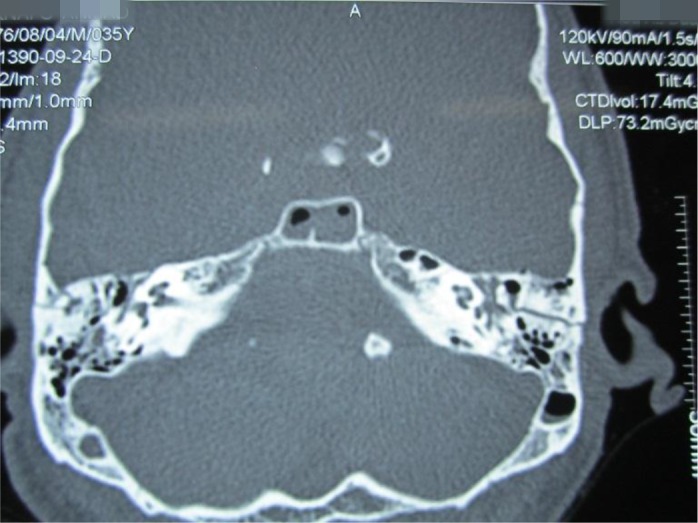
The electromyography and nerve conduction velocity (EMG-NCV) testing revealed decreased amplitudes, with prolongation latencies in maximal stimulation. Denervation potentials were present in the EMG of the tested muscles, compatible with moderate to severe acute bilateral central type facial nerve lesions, and the pure tone audiometry showed bilateral conductive hearing loss with Type B tympanometry. The high resolution computed tomography (HRCT) showed fractures of the squamous parts of both temporal bones, with extensions of the fracture lines to both petrous, the skull base and sphenoidal sinus, the tympanic part of the fallopian canal on the left side, and to the temporomandibular joint (TMJ) on the right side. No ossicular mass dislocations were seen, while mastoid air cell opacification and normal inner ears were present.
With the diagnosis of bilateral facial palsy due to temporal bone fracture, the patient underwent oral prednisolone therapy (1 mg/kg/day) for 2 weeks. Artificial tears were added for eye protection. At the 2nd week follow up visit, he had complete eye closure with minimal effort, good function in his forehead movement, and only slight asymmetry in his mouth motion (House-Brackmann 2) (Figures 1 - 4).
Figure 1. Patient Before Treatment.

Figure 4. Patient Movement After Treatment.

Figure 2. Audiometry Report.
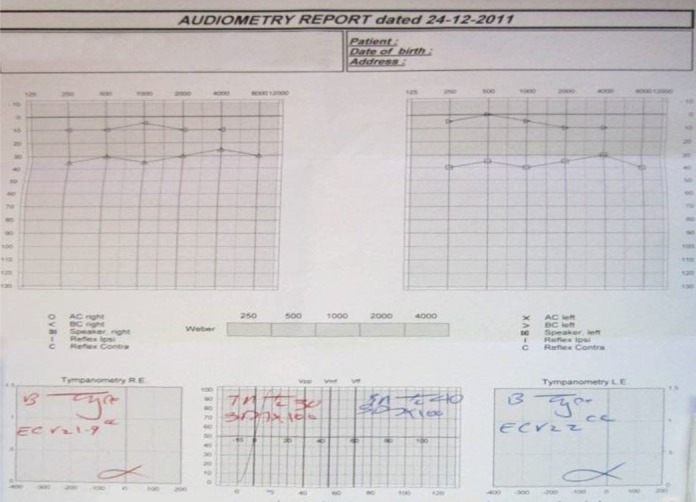
Figure 3. Radiographic Images.
3. Discussion
Bilateral facial nerve palsy is a rare condition, and its etiology is more detectable than the unilateral type. Although the idiopathic bilateral involvement of the nerve (Bell’s palsy) is a diagnosis of exclusion, which occurs in 20% - 23% of the cases, serious life threatening conditions (metabolic, immunologic, toxic, infectious, vascular, etc.) should be ruled out prior to the establishment of the diagnosis (8). According to the article by Elicora et al. bilateral facial paralysis caused by bitemporal bone fractures is very rare, with eight cases reported to date (9).
Temporal bone trauma is common in closed head injuries caused by traffic, falling, assaults, or gunshot accidents. The symptoms and signs include facial nerve involvement, hearing loss, cerebrospinal fluid leakage, and vertigo (10). Traumatic facial nerve injury can be classified into two categories, immediate and delayed onset facial paralysis (8), with delayed onset being more common than immediate onset (11, 12). The laceration, contusion, entrapment, crushing, or traction of the facial nerve at the site of fracture may cause the immediate onset of facial paralysis. Facial paralysis which begins 2 - 21 days (an average of 4 - 5 days) after head trauma is delayed onset (8). A delay in the onset of facial paralysis can be the result of edema, arterial or venous thromboses, or bleeding into the facial nerve bony canal that leads to external compression of the nerve. Each of these causes may lead to the loss of the blood supply and ischemic damage to the nerve with a compressive effect. The geniculate ganglion is the most frequent site of injury (8).
The diagnosis of facial paralysis is made by using the patient’s history, clinical data, and the findings of the radiologic, audiologic, vestibular function, and electrodiagnostic tests. The EMG-NCV elicits demyelinating neuropathy and is used for the determination of the prognosis. The HRCT is used for fracture line assessment, and its probable fallopian canal involvement (4, 7).
Medical and surgical treatment options are available. The indications for medical or conservative treatment include delayed paralysis, incomplete paralysis, or complete paralysis with less than 95% degeneration in the EMG findings over a 2-week duration. However, complete paralysis with more than 95% degeneration is managed by facial nerve exploration (13, 14). For example, in the Elicora et al. study, patients with complete facial paralysis were treated via the surgical method (nerve decompression) with good results (9). In the Hwang study, the patient was placed on corticosteroids, while in the Hwang et al. and Ramamoorthy and Kumaran study they used methylprednisolone and oral steroids for treatment, and achieved good results (4, 10).
Steroid therapy is used for traumatic and infectious facial nerve palsy cases. In addition, artificial tears and lubricants should be administered as prophylaxis for exposure keratitis (4).
3.1. Conclusions
In temporal bone fractures, clinical suspicion and the early detection of facial nerve injuries are necessary for good nerve recovery. However, the lack of asymmetry in the associated facial movements cannot rule out bilateral facial nerve paralysis. The Bell’s phenomenon and incomplete eye closure could highlight bilateral nerve involvement (7, 8).
Acknowledgments
The authors wish to express their gratitude and special thanks for the insights of Miss. Farzaneh Javdani from the Urmia University, department of English language during the preparation of this manuscript.
References
- 1.Kim YH, Choi IJ, Kim HM, Ban JH, Cho CH, Ahn JH. Bilateral simultaneous facial nerve palsy: clinical analysis in seven cases. Otol Neurotol. 2008;29(3):397–400. doi: 10.1097/mao.0b013e3181656998. [DOI] [PubMed] [Google Scholar]
- 2.Wormald PJ, Sellars SL, de Villiers JC. Bilateral facial nerve palsies: Groote Schuur Hospital experience. J Laryngol Otol. 1991;105(8):625–7. doi: 10.1017/s0022215100116858. [DOI] [PubMed] [Google Scholar]
- 3.George MK, Pahor AL. Sarcoidosis: a cause for bilateral facial palsy. Ear Nose Throat J. 1991;70(8):492–3. [PubMed] [Google Scholar]
- 4.Hwang JY, Jwa CS, Kim KH, Kang JK. Post-traumatic Bilateral Facial Paralysis. J Kor Neurotraumatol . 2006;2:136–9. [Google Scholar]
- 5.Keane JR. Bilateral seventh nerve palsy: analysis of 43 cases and review of the literature. Neurology. 1994;44(7):1198–202. doi: 10.1212/wnl.44.7.1198. [DOI] [PubMed] [Google Scholar]
- 6.Glasscock M3, Wiet RJ, Jackson CG, Dickins JR. Rehabilitation of the face following traumatic injury to the facial nerve. Laryngoscope. 1979;89(9 Pt 1):1389–404. doi: 10.1002/lary.5540890904. [DOI] [PubMed] [Google Scholar]
- 7.Li J, Goldberg G, Munin MC, Wagner A, Zafonte R. Post-traumatic bilateral facial palsy: a case report and literature review. Brain Inj. 2004;18(3):315–20. doi: 10.1080/0269905031000149489. [DOI] [PubMed] [Google Scholar]
- 8.Undabeitia J, Liu B, Pendleton C, Nogues P, Noboa R, Undabeitia JI. Bilateral traumatic facial paralysis. Case report. Neurocirugia (Astur). 2013;24(5):225–8. doi: 10.1016/j.neucir.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 9.Elicora SS, Dinc AE, Biskin S, Damar M, Bilgin E. Bilateral Facial Paralysis Caused by Bilateral Temporal Bone Fracture: A Case Report and a Literature Review. Case Rep Otolaryngol. 2015;2015:306950. doi: 10.1155/2015/306950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ramamoorthy M, Kumaran R. Post Traumatic Delayed Bilateral simultaneous symmetrical facial palsy-A rare presentation. Otolaryngology Online J. 2012;2(1) [Google Scholar]
- 11.Holla SP, Smith RR, Sanford RA. Bilateral traumatic facial paralysis. Neurosurgery. 1980;6(3):290–2. [PubMed] [Google Scholar]
- 12.Roth J, Toaff JS, Margalit N, Salame K. Traumatic Facial Diplegia and Horner Syndrome: Case Report. Eur J Trauma Emerg Surg. 2007;33(4):425–9. doi: 10.1007/s00068-007-6913-z. [DOI] [PubMed] [Google Scholar]
- 13.Darrouzet V, Duclos JY, Liguoro D, Truilhe Y, De Bonfils C, Bebear JP. Management of facial paralysis resulting from temporal bone fractures: Our experience in 115 cases. Otolaryngol Head Neck Surg. 2001;125(1):77–84. doi: 10.1067/mhn.2001.116182. [DOI] [PubMed] [Google Scholar]
- 14.Coello AF, Canals AG, Gonzalez JM, Martin JJ. Cranial nerve injury after minor head trauma. J Neurosurg. 2010;113(3):547–55. doi: 10.3171/2010.6.JNS091620. [DOI] [PubMed] [Google Scholar]