

Abstract
Background:
A woman carrying her first pregnancy is starting a new life, and this is a crucial time in her obstetric career. This study was aimed to compare the obstetric performance of primigravidae to that of the multigravidae with a view to suggesting ways of preventing the associated complications.
Patients and Methods:
The study was a cross-sectional case-control study carried out among women who delivered in the study center over a year period. Relevant data of primigravid parturients who delivered in the hospital were retrieved from the labor ward register, and an equal number of multigravidae who delivered during the same study were selected by simple random sampling as the control group.
Results:
Primigravidae constituted 15.3% of the total number of parturients seen during the study period. The age range of the primigravidae was 20–48 years and with a mean age of 28.24 ± 4.28 years. The obstetric complications seen in statistically significant proportion among the primigravidae case group include hypertensive disorder (P = 0.048), prolonged pregnancy (P = 0.039), prolonged labor (P = 0.006), oxytocin augmentation (P = 0.022), cephalopelvic disproportion (P = 0.001), obstructed labor (P = 0.008), instrumental delivery (P = 0.035), cesarean delivery rates (P = 0.011), and increased neonatal unit admission rate (P = 0.002).
Conclusion:
Primigravidity is a high-risk pregnancy with several associated obstetric complications. Primigravidae should, therefore, be managed by specialists in well-equipped hospitals that will provide comprehensive antenatal and intrapartum care which will eventually result in a satisfactory obstetric outcome.
Key words: Multigravidae, obstetric, performance, primigravidae
INTRODUCTION
A primigravida is a woman carrying her first pregnancy.1 A woman carrying her first pregnancy is starting a new life and it is a crucial time in her obstetric career as subsequent obstetric performance will depend on how well the first pregnancy was managed.2 Pregnancy in a primigravida is often viewed with anxiety not only by the patient who is going through the experience for the first time but also her relatives and her caregiver. The obstetric performance of primigravidae is associated with many complications; therefore, they are considered high risk because of both maternal and fetal concerns.2 Numerous studies have shown that primigravidae are at increased risk of complications during pregnancy, labor, and delivery and if not properly managed, these complications can result in increased morbidity and mortality for both the mother and baby.3 Reported complications include hypertensive disorders of pregnancy, preterm delivery and associated low birth weight, abnormal labor patterns, increased risk of operative deliveries, increased rate of admissions into neonatal intensive care unit and increased perinatal deaths.4,5,6,7 These risks are further increased among primigravidae in our environment due to poverty, poor utilization of antenatal care, lack of optimal labor monitoring facilities, lack of hospital infrastructures and staffing, adverse sociocultural practices. This study will, therefore, compare the obstetric performance of this group of women to that of their multiparous counterparts with a view to suggesting ways of anticipating and preventing the associated complications.
PATIENTS AND METHODS
The study was a cross-sectional case-control study carried out among women who delivered in a teaching hospital in Lagos between May 2012 and April 2013. The relevant data of primigravid parturients who delivered in the hospital were retrieved from the labor ward register, and subsequently their case notes were retrieved from the medical records department of the hospital. An equal number of multigravidae who delivered during the same study period were selected by simple random sampling as the control group.
A study pro forma was used to retrieve information such as the sociodemographic characteristics of the women (parity, age, booking status), pregnancy and labor complications, and perinatal outcome from the case records of these women and data was analyzed using SPSS version 20.0 statistical package for windows manufactured by IBM Corp., Armonk, NY, United States. Associations were tested using Chi-square and all statistical significances were reported at P < 0.05.
Ethical approval was obtained for the study from the hospital's Health Research and Ethics Committee before the commencement of the study.
RESULTS
There was a total of 253 primigravidae among the 1659 parturients that delivered during the study constituting 15.3% of the total number of parturients [Figure 1]. However, only 242 case notes were successfully retrieved with the age range of the primigravidae being 20–48 years. As shown in Table 1, the mean age of the primigravidae was 28.24 ± 4.28 years whereas that of the multigravidae was 32.79 ± 4.07 years (P = 0.025). There were fewer booked parturients among the primigravidae compared to the control multigravidae, although this was not statistically significant (76.9% vs. 83.5%; P = 0.097).
Figure 1.
Distribution of parturients seen during the study period
Table 1.
Sociodemographic factors of women
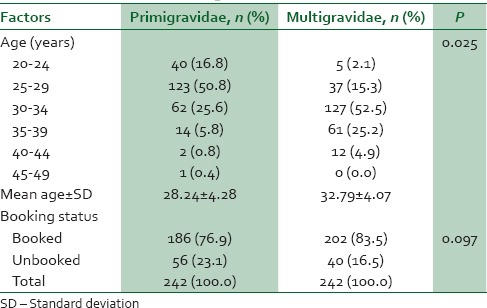
Table 2 shows that only two (hypertensive disorder; P = 0.048 and prolonged pregnancy; P = 0.039) out of the seven antenatal complications reviewed occurred more significantly among the primigravidae group compared to the multigravidae control group. There were, however, more intrapartum complications among the primigravidae [Table 3]. These include prolonged labor (P = 0.006), cephalopelvic disproportion (CPD) (P = 0.001), obstructed labor (P = 0.008), instrumental delivery (P = 0.035), and cesarean delivery rates (P = 0.011). Precipitate labor, genital tract laceration, and uterine atony, however, occurred more in the control multigravidae group.
Table 2.
Antenatal complications
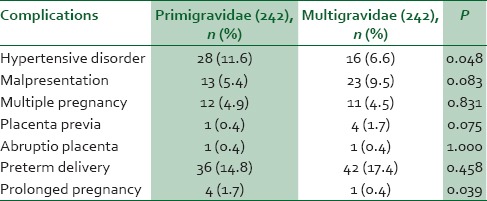
Table 3.
Intrapartum complications
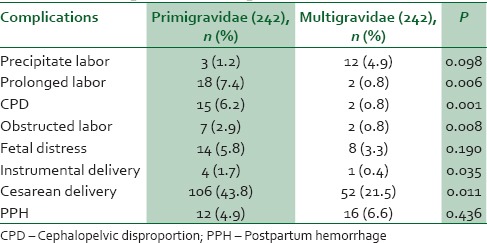
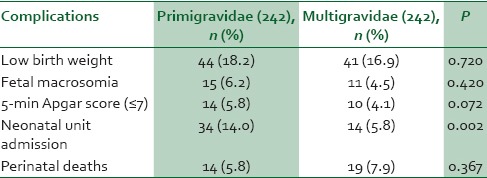
Table 4 shows that among the five perinatal complications assessed, only one (neonatal unit) admission rate occurred in a significantly higher proportion among the primigravidae compared to the multigravidae group (P = 0.002).
Table 4.
Perinatal complications
DISCUSSION
The proportion of primigravidae among the parturients reviewed in the study was 15.3%. This was far lower than the figure reported from centers in Benin (27.3%),2 Imo (33.7%),3 and Ibadan (37.0%).8 The statistically lower mean and modal ages for the primigravidae in this study compared to that of the multigravidae women was not unexpected as women carrying their first pregnancies are usually of the younger age group.
A higher proportion (76.7%) of the primigravidae in this study was booked compared to the 66.8% from the Imo study;3 this can be attributed to the location of the center in this study where expectedly most of the clients are more educated and enlightened. However, more of the control multigravidae group (83.5%) were booked just as in other similar studies.3,4,5,6,7,8 This slight difference in the booking status could have contributed to the various complications observed in the primigravidae as several studies have associated unbooked status with higher incidence of complications in pregnancy, labor, and delivery.2,9,10,11
The occurrence of hypertensive disorder in pregnancy was higher in the primigravidae group from this study, a finding that is consistent with that from other previous studies.5,6,7 This was however at variance to that from the studies by Danish et al.2 and Orji and Ndububa.4 The higher rate of malpresentation among the multigravidae compared to the primigravidae in this study, although not statistically significant (9.5% vs. 5.4%, P = 0.083), was in conformity to that of previous studies that associated high parity with fetal malpresentation.4,12 There were no statistically significant differences in the causes of antepartum hemorrhage (placenta previa and abruptio placentae) in the two groups; a finding that suggests that risk factors other than parity may play far more significant role in the occurrence of these complications. Prolonged pregnancy was observed in a significantly higher proportion among the primigravidae in this study (P = 0.045); an association that has consistently been confirmed by other previous studies.4,8 However, preterm delivery was shown to be commoner in the multigravid control group (17.4% vs. 14.8%) as highlighted by studies done by Fawole in Nigeria 8 and Naheed in Pakistan.13
Most labor complications occurred in the primigravidae compared to the multigravidae as shown by this study. These findings were consistent with that of other similar studies carried out within and outside Nigeria.3,4,7,8,14,15 Although low birth weight and low Apgar score have been demonstrated by previous studies to be more common in primigravidae,5,11 these findings were not demonstrated in statistically significant proportions in this study. The need for neonatal intensive care which was significantly noted among the primigravid case group could be attributed to the associated higher intrapartum complication rates such as prolonged labor, CPD, obstructed labor and instrumental delivery which occurred more among the primigravidae in this study. Perinatal deaths, however, occurred more in the multigravidae women as also shown in a previous study by Orji and Ndububa.4
This study is limited by the poor medical record keeping system in the hospital which affected the data collection as some data could not be retrieved.
CONCLUSION
The study showed primigravidity is a high-risk pregnancy with several associated obstetric complications. Primigravidae should, therefore, be managed by specialists in well-equipped hospitals that will provide comprehensive antenatal and intrapartum care which will eventually result in satisfactory pregnancy, labor, and perinatal outcome.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Okpere E, editor. Clinical Obstetrics. Revised Edition. Benin City: UNIBEN Press; 2004. Protocol for antenatal care; pp. 1–7. [Google Scholar]
- 2.Danish N, Fawad A, Abbasi N. Assessment of pregnancy outcome in primigravida: Comparison between booked and un-booked patients. J Ayub Med Coll Abbottabad. 2010;22:23–5. [PubMed] [Google Scholar]
- 3.Ojiyi EE, Anozie UM, Dike EI, Okeudo C, Anolue F, Uzoma OI, et al. Pregnancy Outcome in primigravidae in a tertiary hospital: A three year review. Int J Gynaecol Obstet. 2012;16:1–5. [Google Scholar]
- 4.Orji EO, Ndububa VI. Obstetric performance of women aged over forty years. East Afr Med J. 2004;81:139–41. doi: 10.4314/eamj.v81i3.9143. [DOI] [PubMed] [Google Scholar]
- 5.Ziadeh S, Yahaya A. Pregnancy outcome at age 40 and older. Arch Gynecol Obstet. 2001;265:30–3. doi: 10.1007/s004040000122. [DOI] [PubMed] [Google Scholar]
- 6.Ogedengbe OK, Odeneye TO. Outcome of Instrumental deliveries in Lagos Nigeria. Implications for its use at the second tier healthcare level. Nig Med Pract. 2006;45:106–10. [Google Scholar]
- 7.Hashim N, Naqvi S, Khanam M, Jafry HF. Primiparity as an intrapartum obstetric risk factor. J Pak Med Assoc. 2012;62:694–8. [PubMed] [Google Scholar]
- 8.Fawole AO, Fadare O. Influence of parity on the partographic management of labour in a Nigerian tertiary hospital. Niger Postgrad Med J. 2008;15:234–7. [PubMed] [Google Scholar]
- 9.Owolabi AT, Fatusi AO, Kuti O, Adeyemi A, Faturoti SO, Obiajuwa PO. Maternal complications and perinatal outcomes in booked and unbooked Nigerian mothers. Singapore Med J. 2008;49:526–31. [PubMed] [Google Scholar]
- 10.Chigbu B, Onwere S, Kamanu CI, Aluka C, Okoro O, Adibe E. Pregnancy outcome in booked and unbooked mothers in South Eastern Nigeria. East Afr Med J. 2009;86:267–71. doi: 10.4314/eamj.v86i6.54136. [DOI] [PubMed] [Google Scholar]
- 11.Mutihir JT, Nyiputen YA. The unbooked patient: A lingering obstetric pathology in Jos, Nigeria. J Obstet Gynaecol. 2007;27:695–8. doi: 10.1080/01443610701612110. [DOI] [PubMed] [Google Scholar]
- 12.Omole-Ohonsi A, Ashimi AO. Grand multiparity: Obstetric performance in Aminu Kano Teaching Hospital, Kano, Nigeria. Niger J Clin Pract. 2011;14:6–9. doi: 10.4103/1119-3077.79231. [DOI] [PubMed] [Google Scholar]
- 13.Naheed F, Tufail A, Kammeruddin K, Madiha S. Obstetrical risks with increased maternal age greater than 35 years. Pak J Surg. 2009;25:240–3. [Google Scholar]
- 14.Baloch S, Khaskeli M, Khushk IA, Sheeba A. Frequency of second stage interventions and its outcome in relation with instrumental vaginal delivery versus caesarean section. J Ayub Med Coll Aboottabad. 2008;20:87–90. [PubMed] [Google Scholar]
- 15.Kramer MS, Dahhou M, Vallerand D, Liston R, Joseph KS. Risk factors for postpartum hemorrhage: Can we explain the recent temporal increase? J Obstet Gynaecol Can. 2011;33:810–9. doi: 10.1016/S1701-2163(16)34984-2. [DOI] [PubMed] [Google Scholar]