

Abstract
Objective
This brief report summarizes a replication and extension of a developmental outcome modeling study, by examining whether delayed substance initiation during adolescence, resulting from universal middle school preventive interventions, reduces problematic use in young adults ages 25–27, up to 14.5 years after baseline.
Method
Participants were middle school students from 36 Iowa schools randomly assigned to the Strengthening Families Program plus Life Skills Training (SFP 10–14 + LST), LST-only, or a control condition. Self-report questionnaires originally were collected at 11 time points, through age 22. An NIH competing continuation grant funded additional assessments at ages 25 and 27, including measures of drunkenness, alcohol-related problems, cigarette use, illicit drug use (lifetime and frequency), marijuana use and prescription drug misuse. These outcomes were modeled as variables influenced by growth factors describing substance initiation during adolescence. Models included the effects of baseline risk, intervention condition assignment, and their interaction; risk-related moderation effects were examined and relative reduction rates were calculated for dichotomous variables.
Results
Model fits were good. Analyses showed significant or marginally significant indirect intervention effects on all outcomes, through effects on adolescent substance initiation growth factors. Intervention X Risk interaction effects favored the higher-risk subsample, replicating earlier findings. Additional direct effects on young adult use were observed only for cigarette frequency. Relative reduction rates were larger for the higher-risk subsamples, ranging from 3.9% to 36.2%.
Conclusions
Universal preventive interventions implemented during early adolescence have the potential to decrease the rates of substance misuse and associated problems, into young adulthood.
Keywords: Universal prevention, young adult substance misuse outcomes, risk-related moderation
This brief report summarizes long-term outcomes of combined universal family- and school-based interventions designed to prevent adolescent substance misuse in general populations. It is based on post high school follow-up assessments in a prevention trial called the Capable Families and Youth Study. Previous reports examined outcomes through 12th grade (Spoth, Randall, Trudeau, Shin, & Redmond, 2008) and early emerging adulthood (ages 19–22, see Spoth, Trudeau, Redmond, & Shin, 2014). This study, funded by a competing continuation grant from the National Institutes of Health, extends earlier reports with follow-up assessments through the subsequent phase of young adulthood, ages 25 and 27.
Epidemiological data concerning patterns of substance misuse from adolescence through young adulthood (Johnston, O’Malley, Bachman, & Schulenberg, 2012; Ohannessian, Finan, Schultz, & Hesselbrock, 2015) guided specification of our developmental mediation model, with adolescent substance initiation as a key intervention effect mechanism (see Guo, Hawkins, Hill, & Abbott, 2001). The study summarized for this report basically replicates the previously-tested developmental outcome mediation model, with additional outcomes in a later phase of young adulthood. The previous testing of the model revealed positive intervention effects on young adult substance misuse frequency measures, mediated through effects on adolescent substance initiation growth factors (intercept and slope). In addition, Intervention X Risk interaction effects were found, favoring the higher risk subsample.
Spoth et al. (2014) examined effects across the 19–22 age range, when young adults were likely obtaining their post-secondary education and/or beginning their adult careers, as well as establishing more stable romantic attachments. This study followed these young adults into a later phase, when responsibilities in both career and family increase, and risk factors for substance misuse continue to emerge (Johnston et al., 2012; Ohannessian et al., 2015). Substance misuse at this young adult stage may be associated with less competent functioning, lower occupational attainment, risky sexual practices, mental health problems, adult crime, and increased mortality (Boden, Fergusson, & Horwood, 2013; Kertesz et al., 2012; Parks, Collins, & Derrick, 2012), supporting attention to long-term effects of universal preventive interventions.
The interventions consisted of two programs with designs based on replicated etiological findings (Jackson, Henderson, Frank, & Haw, 2012): (1) the Strengthening Families Program: For Parents and Youth 10–14 (SFP 10–14–Molgaard, Spoth, & Redmond, 2000); and (2) Life Skills Training (LST–Botvin, 2000). Together they target a wide range of empirically- and theoretically-supported risk and protective factors (e.g., family-, school-, peer-, and individual-related) for adolescent substance misuse. Although some universal interventions have been shown to be effective in delaying substance initiation through adolescence (National Institute on Drug Abuse, 2003), and some studies have demonstrated positive effects into young adulthood (e.g., Haggerty, Skinner, Catalano, Abbott, & Crutchfield, 2015; Wolchik et al., 2013), no longitudinal studies of combined family and school universal interventions, other than our own, could be found.
To summarize, the pattern of earlier results (Spoth et al., 2014) sets the stage for this replication and extension study with two more waves of data at ages 25 and 27. We applied a similar analytic model, assessing results up to 14.5 years after baseline assessment (see Figure 1) and extended to additional outcomes. We hypothesized a replication of the positive substance misuse outcomes found earlier, along with effects on the additional outcomes.
Figure 1.
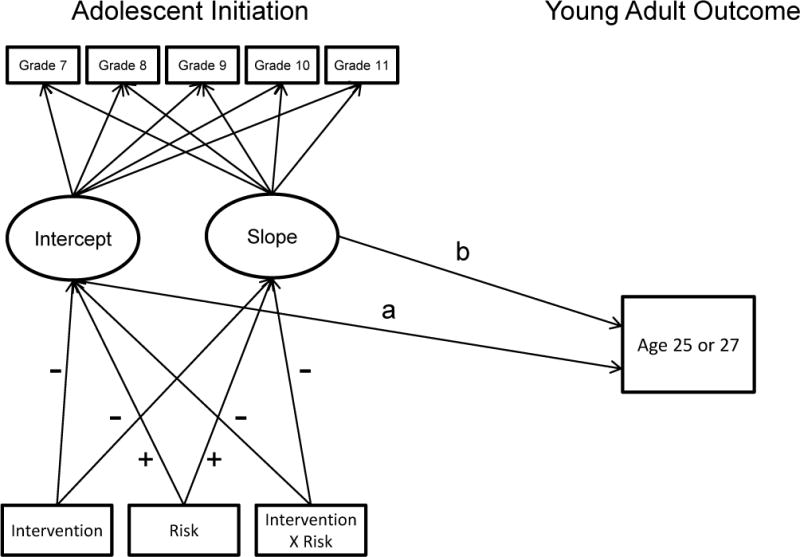
Indirect Effects Model Illustration with Paths Identified
Methods
Sample, Design, Procedures
The university IRB approved the project, APA ethical standards were followed and safety was monitored. At the time the study began, participants were 7th graders and their families enrolled in 36 rural NE Iowa schools in 1997. School selection criteria were: ≥20% of district families eligible for the school lunch program; district enrollment (≤1200); and middle school grades in one location. A randomized block design guided the assignment of 12 schools to each of the three conditions: those schools offered (1) both SFP 10–14 and LST, or (2) LST alone, or (3) a control condition. Students completed in-school assessments (randomly-selected students and their parents in each school district also were recruited to complete more extensive in-home assessments). Participation data are presented in Figure 2; the in-school participation rate at baseline was approximately 90% of the eligible sample. Baseline equivalence was established; more detailed information regarding the sample is provided in earlier reports (e.g. Spoth, Randall, Shin, & Redmond, 2005; Spoth et al., 2008). Analyses were conducted to assess differential attrition on a range of sociodemographic factors and the examined outcomes. Results indicated a higher prevalence of dual biological parent families in the control group than in the intervention groups at baseline, and a lower rate of attrition among control group participants from dual biological parent families at the 19 and 22 year-old assessment point; across conditions, those who remained in the study demonstrated a lower level of substance use at baseline than those who dropped out.
Figure 2.
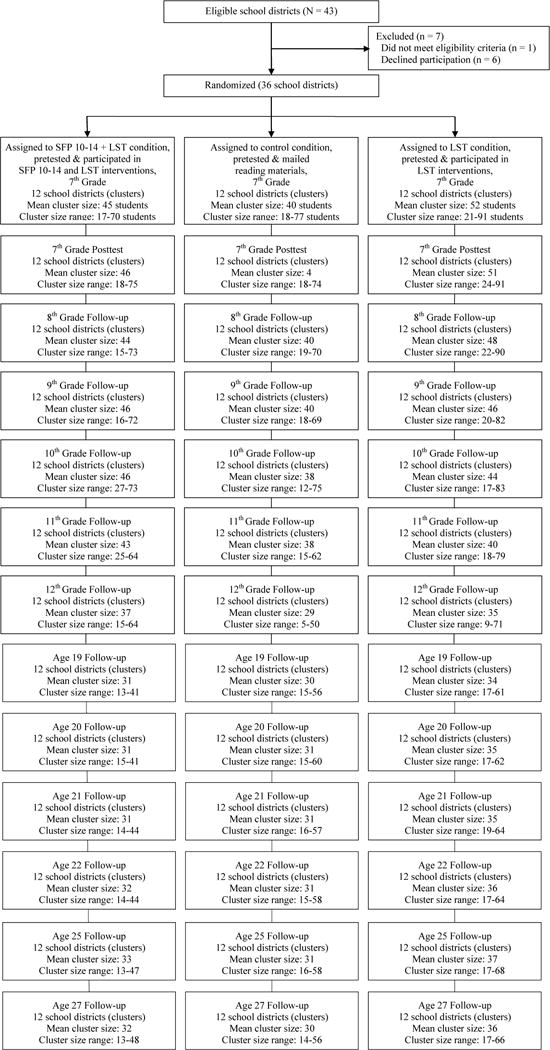
Capable Families and Youth Project Participation Through Age 27: In-School Assessments.
Notes: LST = Life Skills Training. SFP 10–14 + LST = Strengthening Families Program: For Parents and Youth 10–14 + Life Skills Training. Participation in the SFP 10–14 or SFP 10–14 + LST condition was 25%. Participation in a given wave of data collection was not contingent on participation in a prior wave (all enrolled students in the targeted grade were recruited for participation at each wave). The enrolled samples showed considerable stability from year to year; however, we eliminated from the sample those students who changed conditions (i.e., moved from a school district in one condition into one in a different condition) to preserve randomization (n = 18). Following high school, a selected sample was assessed, based on their participation in previous waves (i.e., those present at the pretest and the 11th and/or 12th grade data collection, plus any others who participated in in-home family assessments during adolescence; total eligible n = 1410.
University-trained data collectors conduced assessments in the fall (baseline) and spring (posttest) of 7th grade, and in the spring of grades 8–12; following 12th grade, telephone interviews and mailed questionnaires were utilized. Assessments of intervention group students were not contingent on participation in the interventions. Schools received monetary compensation for their cooperation in classroom-based assessments; following high school, the participants themselves were compensated for their time in completing study assessments.
Intervention Implementation
After the baseline assessment, all students in the intervention conditions were offered the LST program, provided as part of the school curriculum. In addition, intervention group families in the SFP 10–14+LST schools who participated in the in-home baseline assessments were recruited for the SFP 10–14 program; other families in the SFP 10–14+LST condition were allowed to enroll as well. Interventions were delivered via university partnerships with local implementers, as detailed in earlier reports (Spoth, 2007). The interventions are summarized in Table 1 and the measures are described in Table 2.
Table 1.
Capable Families and Youth Project Interventions
| Intervention Theory | Goals | Training process | Delivery | Adherence to content/tasks/activities |
|---|---|---|---|---|
|
| ||||
|
Life Skills Training (LST)
| ||||
| Social learning theory (Bandura, 1977); problem behavior theory (Jessor & Jessor, 1977) | Skill development (social resistance, self-management, general social skills) and knowledge regarding avoidance of substance misuse | Interactive teaching techniques, homework, behavioral rehearsal | (a) University-trained teachers conducted the 15 session program | (a) 85% |
| (b) Five booster sessions one year later | (b) 82% | |||
| (c) Four 11th grade booster sessions for a randomly-selected half of the schools | (c) 77% | |||
|
| ||||
|
Strengthening Families Program: For Parents and Youth 10–14 (SFP 10–14)
| ||||
| Biopsychosocial Model Empirically-based risk/protective factors originating in the family (Molgaard et al., 2000) | Reduce youth substance misuse and other problem behaviors; enhance parenting skills (nurturing, limit-setting, and communication); enhance youth skills (prosocial, peer resistance) | Interactive with videotaped modeling of positive behavior; each session required one parent and two youth facilitators | (a) University-trained facilitators conducted seven 1-hour concurrent youth and parent sessions, plus 1-hour conjoint sessions for 137 families | (a) 98% families, 92% parents, 94% youth |
| (b) Four booster sessions offered one year later (69% of families attended ≥1 session) | (b) 97% families, 94% parents, 96% youth | |||
| (c) Booster sessions for a randomly-selected half of the schools included: videotape and handout on effective parenting with self-assessment questionnaire; family-school resource fair and resource directory; student goal-setting seminar | (c) 68% return on self-assessment, 40% attendance for resource fair, 65% of students attended goal-setting seminar | |||
Table 2.
Measures for the Capable Families and Youth Project: Indirect Effects Model of Young Adult Outcomes
| Measure | Description | Coding |
|---|---|---|
| Drunkenness frequency | This and other substance misuse frequency measures were adapted from item sets in the Monitoring the Future study (see Johnston et al., 2012). Drunkenness frequency was assessed with one question, “How often do you usually get drunk?” | Scaled from 1 = “Not at all” to 7 = “About every day.” |
| Alcohol-related problems | Alcohol-related problem behaviors during the past year were measured with a short, modified form of the Rutgers Alcohol Problems Index (White & Labouvie, 1989); included ten questions with the stem, “How often have the following things happened during the past 12 months?” An example item was “You had trouble remembering what you had done when you were drinking.” | Scaled from 0 = “Never” to 4 = “Four or more times”; averaged (α = .70). |
| Cigarette frequency | Past year cigarette frequency was measured with the item: “During the past 12 months how often did you smoke cigarettes?” | Scaled from 1 = “Not at all” to 7 = “About 2 packs/day.” |
| Illicit substance use frequency | Past year illicit substance use frequency was measured with nine open-ended items (e.g., “How many times in the past 12 months did you use [specific substance]?”). Items assessed past year use of marijuana, cocaine, ecstasy (MDMA), methamphetamine, and LSD (hallucinogens), as well as misuse of narcotics (Vicodin, Oxycontin, Percocet), amphetamines, barbiturates (sedatives), and tranquilizers—not under a doctor’s order. | In order to address item skew and to obtain an appropriate weighting of items in the measure, each item was natural-log transformed and summed. |
| Additional Measures not included in Spoth et al. (2014) | ||
| Marijuana index | Lifetime, past year, and past month marijuana use were combined in this index to assesses more serious use and address the problem associated with a small number of very frequent users that can skew results. | Each item was coded dichotomously, so that 0 = “No” and 1 = “Yes” and the items were summed, for an index where 0 = “Never used,” 1= “Used at least once,” 2 = “Used within the last year,” and 3 = “Used within the past month.” |
| Lifetime illicit drug use | This scale combined five lifetime illicit drug use items: methamphetamine, ecstasy, cocaine, GHB or Rohypnol, and LSD or other hallucinogens. | Each item was dichotomously scored (0 = “No”; 1 = “Yes”) and summed. |
| Lifetime prescription drug misuse | This scale combined four lifetime misuse items addressing commonly-misused prescription drugs – narcotics, barbiturates, tranquilizers, and amphetamines. The questions inquired about the use of these drugs “not under a doctor’s order.” | Each item was scored 0 = “No” or 1 = “Yes” and summed. |
Note: In order to further explore and differentiate the illicit substances analyzed in the past year illicit substance use frequency measure above, the number of users and the frequency of use for each substance were examined. As expected, marijuana had both the largest number of current users and the highest frequency of use, so it was analyzed separately. Of the additional items, prescription drug misuse is separately addressed in the literature; as applied in an earlier report (Spoth et al., 2013), an “overall” measure of such use was employed here. The additional illicit drugs assessed had low frequencies, so they were combined into an index, based on dichotomous lifetime use (to avoid issues of skewing resulting from elevated use of any given substance).
SFP 10–14 = Strengthening Families Program: For Parents and Youth 10–14; LST = Life Skills Training. The latent growth factor loadings on the observed measures of ASI set the growth model intercept to the midpoint of the post-intervention period so that the intercept value corresponded to the average level of initiation across that time period, as estimated by the model. Growth was modeled as linear (polynomial contrasts fixed at −2, −1, 0, 1 and 2). The growth factor indicators were modeled with an autoregressive error structure and the latent intercept and slope factors were allowed to correlate. The model controlled for pre-intervention ASI, dual biological parent families, and gender on the adolescent growth factors.
Analyses
As noted, the current analyses represent a replication and extension of the earlier age 19–22 report that evaluated the indirect effect of the interventions on growth factors of young adult substance use outcomes from ages 19–22 via effects on adolescent substance initiation (ASI) intercept and slope. We extended the analysis to evaluate indirect intervention effects, via the intercept and slope of ASI, on point-in-time outcomes at ages 25 and 27 (see Figure 1). SFP 10–14+LST versus Control and LST-only versus Control models were analyzed separately.
To test for risk-related moderation of intervention effects, participants were classified as either higher- or lower-risk, based on their baseline levels of gateway substance initiation. Higher risk was indicated by initiation of two or more gateway substances—alcohol, cigarettes, marijuana; approximately 20% were classified as higher-risk. We also considered whether participants who had reported lifetime use of only one substance (thereby classified as lower-risk) should be classified higher-risk, due to high-frequency use of that one substance. To address this issue we examined the frequency of use among those that used any one of the three gateway substances at baseline. This examination verified that nearly all (over 99%) of those who used any one of the three substances at rates of monthly use or more were included in the higher-risk group. Analyses examined risk moderation with two-way interactions (Intervention X Risk). Contrast coding (1 and −1) for the risk and the intervention variables was used to create orthogonal terms to facilitate interpretation of main and interaction effects.
Analyses were performed with Mplus 7.1 (Muthén & Muthén, 1998–2010). School ID was included as a higher-level cluster variable to adjust standard errors to account for intra-unit dependency. Robust maximum likelihood estimation addressed effects of non-normality and non-independence of observations. Mplus computes full-information maximum likelihood (FIML) estimates with incomplete data. Analyses were restricted to those who had data on intervention condition, baseline risk level, and cluster [school]); for SFP 10–14+LST versus Control, N = 983 and for LST-only versus control, N = 1060. Missing data averaged around 16%. Model fit was evaluated using the root mean square error of approximation (RMSEA: Steiger & Lind, 1980), the comparative fit index (CFI: Bentler, 1988), and the chi-square; a RMSEA ≤ .06 and a CFI ≥ .95 indicate good model fit (Hu & Bentler, 1999).
As in the earlier report, following estimation of the indirect effects of interventions and risk, subsequent models were tested in which direct effects were added to the models. The significance of the direct and indirect effects was evaluated, and the difference in the fit of the models was compared to determine whether adding direct effects produced a better-fitting model. The addition of direct effects can help determine whether intervention, risk, and the interaction effects were primarily mediated by adolescent substance initiation or whether additional mechanisms also were influential. Finally, to estimate the practical significance of the intervention effects, dichotomous variables were constructed by establishing cut-points for the young adult outcome variables to represent caseness, indicating the potential for public health consequences. Cut-points based on health-related consequences of use were identical to the earlier report for the drunkenness, alcohol-related problems, cigarettes, and illicit substance use measures (see Spoth et al., 2014); the additional measures in this report—the marijuana index, lifetime illicit drug use, and lifetime prescription drug misuse measures—were considered to have health-related consequences at any level of use. Effects on the dichotomous outcomes were modeled in the same manner as the earlier modeling, with or without direct effects, based on overall model fit. Relative reduction rates (RRR) were computed from the estimated percentages of those above the cutoff in the intervention and control condition, for both the overall sample and the higher-risk subsample.
Results
Regarding model fits, although the chi-square was significant in all models, the CFIs (> .960) and RMSEAs (< .06) indicated good fits; detail on the results concerning effects of the Interventions, Risk, and Intervention X Risk on the ASI intercept and slope is provided online (http://www.online). As found in the earlier analyses, all the Intervention, Risk, and Intervention X Risk paths to the adolescent intercept and slope were either significant or marginally significant for both intervention conditions vs. control, for all outcomes, and at both ages.
Table 3 summarizes the paths from the ASI intercept and slope to the Age 25 and 27 young adult outcomes, along with the indirect effects from Intervention and Intervention X Risk. As Table 3 indicates, the ASI intercept – that is, the average level across time – was generally stronger in predicting to the young adult outcomes than was the slope. However, there were instances in which the slope was a significant predictor (i.e., LST effects on cigarette frequency and both interventions’ effects on the marijuana index), and was a stronger predictor, than was the intercept (i.e., SFP 10–14+LST effects on drunkenness frequency). The indirect effects of the interventions were significant for most outcomes; exceptions were the indirect effects on illicit substance use frequency for both interventions at age 25 and for SFP 10–14+LST at age 27, and for lifetime prescription drug misuse for SFP 10–14+LST at both ages. The Intervention X Risk interaction indirect effects also were significant, with three exceptions—the LST X Risk indirect effect on illicit substance use frequency at age 25 was nonsignificant, and the LST X Risk indirect effects on alcohol-related problems at age 25, along with illicit substance use frequency at age 27, were marginally significant. Figures 3 and 4 illustrate the comparative levels of outcomes in the intervention and control groups by risk level for age 27 drunkenness frequency (Figure 3) and age 27 lifetime prescription drug misuse (Figure 4).
Table 3.
Indirect Effects Model: Effects paths from the adolescent substance initiation intercept and slope, and indirect intervention effects
| Outcome | Model Effect Paths | ||||
|---|---|---|---|---|---|
|
|
|||||
| Age | Intercept effect on Outcome | Slope effect on Outcome | Intervention Indirect Effects | Int. X Risk Indirect Effects | |
|
|
|||||
| Drunkenness Frequency | |||||
| SFP 10–14+LST vs Control | 25 | .045 | .212*** | −.039*** | −.033** |
| 27 | .023 | .215*** | −.039** | −.033** | |
| LST vs Control | 25 | .163** | .077 | −.030* | −.021* |
| 27 | .143+ | .122 | −.038* | −.027* | |
| Alcohol-Related Problems | |||||
| SFP 10–14+LST vs Control | 25 | .094+ | .094+ | −.023* | −.021* |
| 27 | .074 | .100+ | −.023* | −.021** | |
| LST vs Control | 25 | .166** | .019 | −.019+ | −.014+ |
| 27 | .193* | .082 | −.034* | −.025** | |
| Cigarette Frequency | |||||
| SFP 10–14+LST vs Control | 25 | .432*** | .064 | −.041* | −.046** |
| 27 | .436*** | .067 | −.042* | −.047** | |
| LST vs Control | 25 | .349*** | .208** | −.073*** | −.054* |
| 27 | .359*** | .161* | −.066*** | −.049** | |
| Illicit Substance Use Frequency | |||||
| SFP 10–14+LST vs Control | 25 | .334** | −.059 | −.013 | −.020* |
| 27 | .231+ | .035 | −.022 | −.025** | |
| LST vs Control | 25 | .415*** | −.073 | −.025 | −.019 |
| 27 | .357** | −.010 | −.032* | −.024+ | |
| Marijuana Index | |||||
| SFP 10–14+LST vs Control | 25 | .376*** | .176*** | −.058** | −.057** |
| 27 | .353*** | .224*** | −.066** | −.063*** | |
| LST vs Control | 25 | .467*** | .102* | −.063** | −.046** |
| 27 | .443*** | .153** | −.73** | −.053** | |
| Lifetime Illicit Drug Use | |||||
| SFP 10–14+LST vs Control | 25 | .418*** | .089 | −.045** | −.048** |
| 27 | .395*** | .110 | −.049** | −.050*** | |
| LST vs Control | 25 | .460*** | .024 | −.047** | −.034* |
| 27 | .454*** | .064 | −.057** | −.040** | |
| Lifetime Prescription Drug Misuse | |||||
| SFP 10–14+LST vs Control | 25 | .470*** | −.052 | −.026 | −.035** |
| 27 | .426*** | .005 | −.032+ | −.038** | |
| LST vs Control | 25 | .391*** | .036 | −.045** | −.033** |
| 27 | .385*** | .060 | −.049** | −.036** | |
Note: SFP 10–14 = Strengthening Families Program: For Parents and Youth 10–14; LST = Life Skills Training. Contrast coding was used so that the effect of the intervention can be interpreted as the overall effect of assignment to the intervention condition, controlling for risk status, and the effect of risk can be interpreted as the overall effect of risk, controlling for intervention status. The interaction can be interpreted as the difference in intervention effect by level of risk—a significant negative Intervention X Risk effect would suggest that the intervention was more effective in lowering levels of substance misuse for the higher-risk group.
Figure 3.
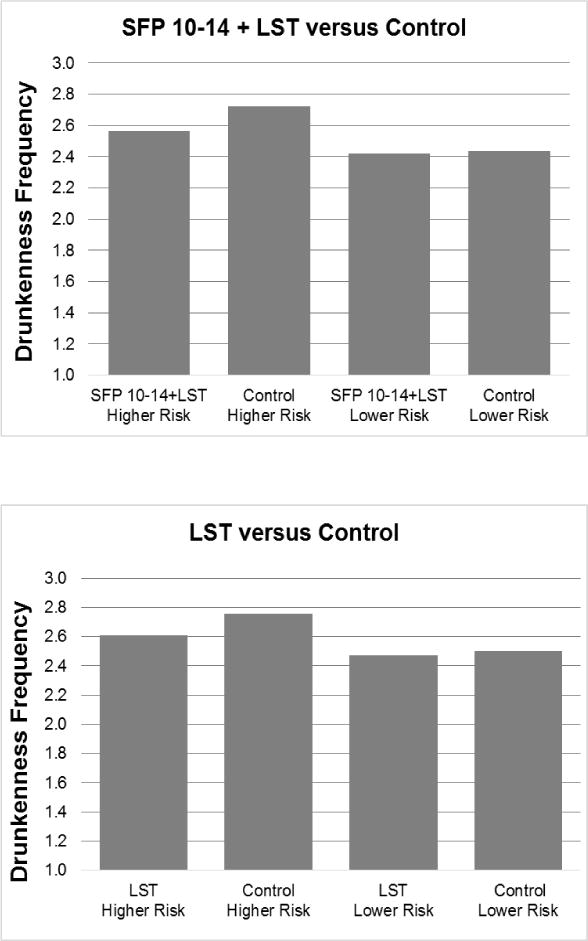
Model-based Drunkenness Frequency Outcome by Intervention Condition and Risk Level
Figure 4.
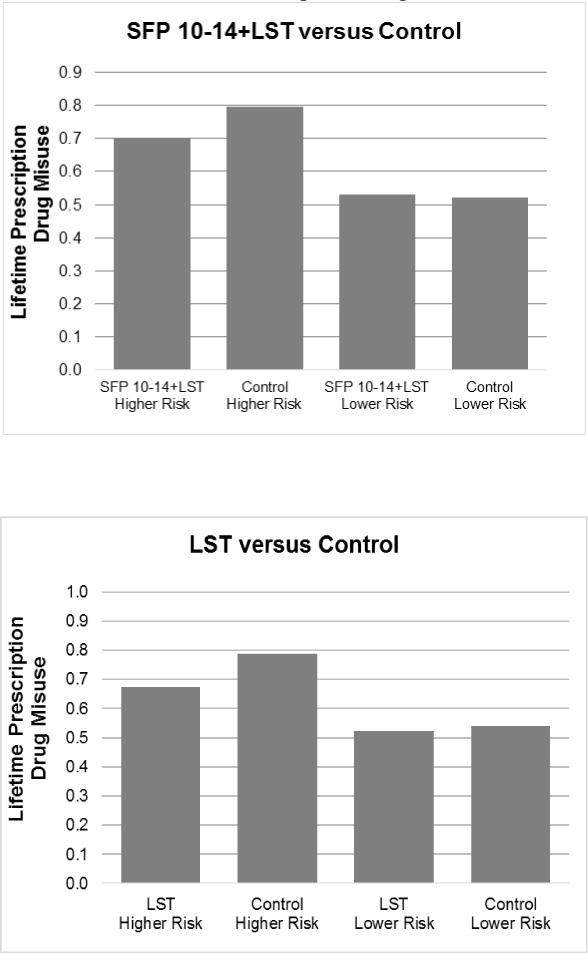
Model-based Lifetime Prescription Drug Misuse Outcome by Intervention Condition and Risk Level
To further explore the mechanisms of long-term effects, direct effects of Intervention, Risk, and Intervention X Risk were added to the indirect effects models. Consistent with earlier findings, adding direct effects improved model fit for cigarette frequency for both intervention conditions at both time points; indirect effects remained significant.
Finally, to evaluate the practical significance of the findings, the dichotomous outcomes were modeled to provide estimates of the RRRs for each of the variables (see Table 4). The RRRs range from 2.5% to 36.2%. In general, The SFP 10–14+LST intervention produced somewhat larger RRRs across outcomes, with the most notable exceptions of cigarette frequency and lifetime prescription drug misuse, where the LST-only condition demonstrated larger RRRs, consistent with earlier analyses. It also is important to note that RRRs were stronger for the higher risk subsample.
Table 4.
Relative reduction rates (RRR) for age 25 and 27 dichotomous variables by intervention condition: Full sample and higher risk subsample
| SFP 10–14 + LST
|
LST
|
|||
|---|---|---|---|---|
| Variable | RRR (%)
|
RRR (%)
|
||
| Age 25 | Age 27 | Age 25 | Age 27 | |
| Drunkenness | ||||
| Full Sample | 9.4 | 13.8 | 9.6 | 9.2 |
| Higher Risk | 18.8 | 17.4 | 12.6 | 12.2 |
| Alcohol Problems | ||||
| Full Sample | 9.2 | 6.1 | 2.5 | 5.9 |
| Higher Risk | 12.2 | 8.8 | 3.9 | 8.3 |
| Cigarette Usea | ||||
| Full Sample | 22.0 | 14.9 | 28.3 | 25.3 |
| Higher Risk | 25.8 | 16.7 | 36.2 | 29.5 |
| Illicit Drug Use | ||||
| Full Sample | 7.6 | 12.7 | 6.3 | 9.8 |
| Higher Risk | 11.5 | 16.3 | 9.1 | 12.9 |
| Marijuana Use | ||||
| Full Sample | 10.6 | 12.0 | 11.1 | 11.7 |
| Higher Risk | 14.1 | 15.9 | 14.2 | 14.9 |
| Lifetime Illicit Drug Use | ||||
| Full Sample | 10.7 | 12.5 | 11.5 | 9.8 |
| Higher Risk | 14.2 | 16.2 | 14.6 | 12.9 |
| Lifetime Prescription Drug Misuse | ||||
| Full Sample | 8.8 | 9.8 | 13.1 | 13.6 |
| Higher Risk | 13.0 | 13.9 | 16.3 | 16.8 |
Note. SFP 10–14 = Strengthening Families Program: For Parents and Youth 10–14; LST = Life Skills Training; RRR = relative reduction rate calculated from the model-based estimates (RRR = control rate – intervention rate/control rate). Variables were dichotomized (0 and 1) so that a score of 1 indicated: drunkenness at greater than once per month; alcohol-related problems at one or more out of 10; cigarette use at greater than no use during the past year; illicit substance use (past year) at greater than no use; marijuana index (a sum of dichotomous measures of lifetime use, past year use, and past month use) at greater than no use; lifetime other illicit (a sum of dichotomous measures of five substances – cocaine, methamphetamine, ecstasy, GHB, and LSD or other hallucinogens) at greater than no use; lifetime prescription drug misuse (a sum of dichotomous measures of misuse of narcotics, amphetamines, barbiturates, and tranquilizers) at greater than no misuse. The lifetime use variables were corrected for consistency, so that once an individual indicated initiation of a substance, that initiation was also indicated at all later waves.
The best fitting models included direct effects from the intervention condition, risk, and the Intervention Condition X Risk interaction.
Discussion
The potential of universal preventive intervention during young adolescence is further supported by this extension of our earlier study, addressing a gap in the relevant outcome literature concerning possible benefits of developmentally well-timed universal interventions on substance-related problems in young adulthood. This gap was underscored in the National Research Council and Institute of Medicine report on the prevention of behavioral health-related disorders (NRC-IOM, 2009). The key mechanism of intervention effects we examined was a delay in substance initiation for students in school districts that offered the family-focused and school-based universal interventions.
We previously tested a longitudinal developmental model grounded in developmental epidemiology concerning age-related patterns of substance misuse and positing adolescent initiation as a mediator of later misuse (Spoth et al., 2014); findings supported the model. The present replication and extension of this model retained important features, including: (1) a parsimonious model for examining the complex interplay of developmental pathways toward substance misuse; and (2) a model that addresses salient methodology and measurement issues in the literature (e.g., differing assessment instruments across time; compounding of errors across measures, complexity of modeling chains of effects). The findings clearly support the model, providing evidence for the hypothesized indirect effects for both interventions, through 12.5 and 14.5 years past baseline. As was the case in the earlier young adult outcomes model tested, the strongest effects were observed via the adolescent growth intercept, although a strong slope effect for the marijuana index also was observed, along with slope effects for SFP 10–14+LST on drunkenness frequency and for LST on cigarette frequency.
It is noteworthy that a similarity in effects for both interventions was observed; indirect effects were generally significant for both, as in our earlier longitudinal model findings; it also was consistent with the longitudinal pattern of findings subsequent to the assessment conducted 1.5 years past baseline. This pattern of findings entailed an emerging, increasing similarity in levels of effects, likely due, at least in part, to the limited participation in the family intervention, as explained in the earlier longitudinal model testing paper.
Interestingly, adding direct effects only improved model fit in the case of cigarette frequency for both interventions at both time points, although indirect effects remained significant. This same pattern of influences was found in the earlier report on cigarette frequency at age 22, and suggests that, in addition to intervention effects transmitted into young adulthood via adolescent substance initiation, there were additional intervention factors that remained directly relevant to cigarette use in young adulthood. As noted in the earlier report, interventions could have influenced choices via lessons on assertiveness, decision-making, refusal skills, general social skills, and specific substance knowledge (e.g., negative health effects of cigarette use) that remain salient during young adulthood.
As this study and earlier intervention outcome articles demonstrate, universal preventive interventions have the potential to decrease the rates of substance misuse and associated problems into young adulthood; results are consistent with the hypothesized mechanism of effects through which intervention-driven delays in substance initiation during young adolescence lead to diminished young adult substance misuse. Also worthy of note, Intervention X Risk effects suggested that participants at higher levels of risk generally benefited more from the interventions, a fairly consistent finding from examination of earlier follow-up studies. Results for the RRRs underscore relatively stronger effects for those at higher risk. That is, for both intervention conditions and every variable at each time point, the RRRs were larger for the higher risk subsample than for the overall sample. However, taken as a whole, the RRRs suggest that over a range of substance misuse problems in young adulthood, individuals who attended brief, universal substance misuse preventive interventions during middle school and high school were less likely to misuse substances during young adulthood, and for those at higher risk, the interventions were especially effective.
Supplementary Material
What is the public health significance of this article?
The findings from this study suggests that brief interventions for general populations implemented in middle school can have meaningful long-term effects on substance misuse up to 14.5 years after pretest assessments, particularly for higher-risk participants. Positive effects were observed on a range of substances and associated problems, including those concerning prescription drug misuse; relative reduction rates suggested the practical significance of those results. These long-term effects and related economic benefits confirmed in earlier reports suggest further efforts to disseminate, in order to achieve public health impact.
Acknowledgments
Work on this paper was supported by research grant DA 10815 from the National Institute on Drug Abuse.
Footnotes
Conflict of interest: None
References
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977;84(2):191–215. doi: 10.1037//0033-295x.84.2.191. [DOI] [PubMed] [Google Scholar]
- Bentler PM. Comparative fit indices in structural models. Psychological Bulletin. 1988;107:238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Boden JM, Fergusson DN, Horwood LJ. Alcohol misuse and criminal offending: Findings from a 30-year longitudinal study. Drug and Alcohol Dependence. 2013;128(1–2):30–36. doi: 10.1016/j.drugalcdep.2012.07.014. [DOI] [PubMed] [Google Scholar]
- Botvin GJ. Life Skills Training: Promoting health and personal development. Princeton NJ: Princeton Health Press; 2000. [Google Scholar]
- Guo J, Hawkins JD, Hill KG, Abbott RD. Childhood and adolescent predictors of alcohol abuse and dependence in young adulthood. Journal of Studies on Alcohol. 2001;62(6):754–762. doi: 10.15288/jsa.2001.62.754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haggerty KP, Skinner ML, Catalano RF, Abbott RD, Crutchfield RD. Long-term effects of Staying Connected with your Teen on drug use frequency at age 20. Prevention Science. 2015;16(4):538–549. doi: 10.1007/s11121-014-0525-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu LT, Bentler PM. Cutoff criteria for fit indices in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Jackson CA, Henderson M, Frank JW, Haw SJ. An overview of prevention of multiple risk behaviour in adolescence and young adulthood. Journal of Public Health. 2012;34(1):i31–i40. doi: 10.1093/pubmed/fdr113. [DOI] [PubMed] [Google Scholar]
- Jessor R, Jessor SL. Problem behavior and psychosocial development: A longitudinal study of youth. New York: Academic Press; 1977. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975–2011: Volume II, College students and adults ages 19–50. Ann Arbor: Institute for Social Research, The University of Michigan; 2012. [Google Scholar]
- Kertesz SG, Khodneva Y, Richman J, Tucker JA, Safford MM, Jones B, Pletcher MJ. Trajectories of drug use and mortality outcomes among adults followed over 18 years. Journal of General Internal Medicine. 2012;27:808–16. doi: 10.1007/s11606-011-1975-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molgaard VM, Spoth RL, Redmond C. OJJDP Juvenile Justice Bulletin (NCJ 182208) Washington, DC: U.S. Department of Justice, Office of Juvenile Justice and Delinquency Prevention; 2000. Competency training: The Strengthening Families Program for Parents and Youth 10–14. [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. Sixth. Los Angeles, CA: Muthén & Muthén; 1998–2010. [Google Scholar]
- National Institute on Drug Abuse. Preventing drug use among children and adolescents: A research-based guide for parents, educators, and community leaders. 2nd. Bethesda, MD: National Institute on Drug Abuse; 2003. (NIH Publication 04–4212[A]). [Google Scholar]
- National Research Council and Institute of Medicine. Preventing mental, emotional, and behavioral disorders among young people: progress and possibilities. In: O’Connell ME, Boat T, Warner KE, editors. Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. Washington DC: National Academies Press; 2009. [PubMed] [Google Scholar]
- Ohannessian CM, Finan LJ, Schultz J, Hesselbrock V. A long-term longitudinal examination of the effect of early onset of alcohol and drug use on later alcohol abuse. Substance Abuse. 2015;11:1–5. doi: 10.1080/08897077.2014.989353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parks KA, Collins L, Derrick JL. The influence of marijuana and alcohol use on condom use behaviors: Findings from a sample of young adult female bar drinkers. Psychology of Addictive Behaviors. 2012;26(4):888–894. doi: 10.1037/a0028166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R. Opportunities to meet challenges in rural prevention research: Findings from an evolving community-university partnership model. Journal of Rural Health. 2007;23(S):42–54. doi: 10.1111/j.1748-0361.2007.00123.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R, Randall GK, Shin C, Redmond C. Randomized study of combined universal family and school preventive interventions: Patterns of long-term effects on initiation, regular use, and weekly drunkenness. Psychology of Addictive Behaviors. 2005;19(4):372–381. doi: 10.1037/0893-164X.19.4.372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R, Randall GK, Trudeau L, Shin C, Redmond C. Substance-related outcomes of universal family-and school-based interventions 5½ years past baseline. Drug and Alcohol Dependence. 2008;96:57–68. doi: 10.1016/j.drugalcdep.2008.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R, Trudeau L, Redmond C, Shin C. Replication RCT of early universal prevention effects on young adult substance misuse. Journal of Consulting and Clinical Psychology. 2014;82:949–963. doi: 10.1037/a0036840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R, Trudeau L, Shin C, Ralston E, Redmond C, Greenberg M, Feinberg M. Longitudinal effects of universal preventive intervention on prescription drug misuse: Three RCTs with late adolescents and young adults. American Journal of Public Health. 2013;103(4):665–672. doi: 10.2105/AJPH.2012.301209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steiger JH, Lind J. Statistically based tests for the number of common factors. Paper presented at the Annual Meeting of the Psychometric Society; Iowa City, Iowa. 1980. [Google Scholar]
- White HR, Labouvie EW. Toward the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- Wolchik SA, Sandler IN, Tein JY, Mahrer NE, Millsap RE, Winslow E, Reed A. Fifteen-year follow-up of a randomized trial of a preventive intervention for divorced families: Effects on mental health and substance use outcomes in young adulthood. Journal of Consulting and Clinical Psychology. 2013;81(4):660–673. doi: 10.1037/a0033235. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.