

Abstract
Previous research reported positive associations between alcohol mixed with energy drink (AMED) consumption and overall alcohol consumption. However, results were largely based on between-subjects comparisons comparing AMED consumers with alcohol-only (AO) consumers, and therefore cannot sufficiently control for differences in personal characteristics between these groups. In order to determine whether AMED consumers drink more alcohol on occasions they consume AMED compared to those when they drink AO additional within-subjects comparisons are required.
Therefore, this UK student survey assessed both alcohol consumption and alcohol-related negative consequences when consumed alone and when mixed with energy drinks, using a within-subject design.
A total of 1873 students completed the survey, including 732 who consumed AMED. It was found that AMED consumers drank significantly less alcohol when they consumed AMED compared to when they drank AO (p < 0.001). In line with reduced alcohol consumption significantly fewer negative alcohol-related consequences were reported on AMED occasions compared to AO occasions (p < 0.001).
These findings suggest that mixing alcohol with energy drinks does not increase total alcohol consumption or alcohol-related negative consequences.
Abbreviations: AMED, Alcohol Mixed with Energy Drink; AO, Alcohol-Only; BYAACQ, Brief Young Adult Alcohol Consequences Questionnaire
Keywords: Alcohol mixed with energy drinks, Student alcohol consumption, Consequences
Highlights
-
•
First UK student survey to examine effects of mixing alcohol with energy drinks
-
•
AMED consumers drink more alcohol than AO consumers.
-
•
AMED consumers drink less alcohol on AMED occasions compared to AO occasions.
-
•
Mixing alcohol with energy drinks does not increase total alcohol consumption.
-
•
Excessive alcohol consumption remains a persistent concern among UK students.
1. Introduction
Excessive alcohol consumption is a persistent global issue, ranked the third leading cause of death and disability worldwide (SS et al., 2012). In England in 2013/14 there were 6592 alcohol-related deaths, a 10% increase from 2003, and over 1 million hospital admissions related to alcohol consumption (Health and Social Care Information Centre, 2015). These alarming statistics are underlined by the findings that 24% of people in the UK consume alcohol in a way that is harmful or potentially harmful to their health and well-being (National Health Service, n.d.-a).
In the past decade there has been increased concern regarding heavy episodic or binge drinking. In the UK binge drinking is defined as consuming > 8 units of alcohol for men, and more than six units of alcohol for women (National Health Service, n.d.-b). Recent research by the World Health Organization (2014) found that Britain is one of the worst countries in the world for binge drinking, ranked 13th out of 196 countries, with 28% of Britons classed as having had an episode of heavy drinking in the previous month- twice the global average. Binge drinking is particularly prevalent among young people, with 27% of 16–24 year olds found to have drunk very heavily at least once in the past week (Office for National Statistics, n.d.). These findings indicate a serious public health problem and social issue that requires attention. Therefore, it is important to study the factors that may be contributing to high rates of alcohol consumption among young people in the UK.
Recently there has been much public health interest and British media attention on the rise in popularity of mixing alcohol with energy drinks and its possible effect on overall alcohol consumption and negative alcohol-related consequences. Indeed, despite energy drinks comprising only 1% of the total non-alcoholic beverage market (UNESDA, 2012), 15–24% of students aged 18–30 years old report consuming alcohol mixed with energy drinks (AMED) at least once in the past month (O'Brien et al., 2008, Velazquez et al., 2012). Research attention has primarily focused on whether consuming AMED poses a public health concern above and beyond consuming alcohol by itself, and therefore a behaviour worth targeting to reduce excessive alcohol consumption.
Several studies have compared alcohol consumption among those who mix alcohol with energy drinks and those who consume alcohol only, using a between-subjects design. The majority of these studies (Brache and Stockwell, 2011, Eckschmidt et al., 2013, Flotta et al., 2014, O'Brien et al., 2013) have consistently found that those who consume AMED drink significantly more alcohol on an average drinking occasion compared to those who consume alcohol only (AO). In line with increased alcohol consumption those who consumed AMED also reported significantly more alcohol-related consequences than those who consumed AO, including driving whilst intoxicated (Brache and Stockwell, 2011, Eckschmidt et al., 2013, Flotta et al., 2014, O'Brien et al., 2013) and having unplanned unprotected sex (O'Brien et al., 2008, O'Brien et al., 2013). Early explanations for these findings purported that AMED consumption leads to a reduced perception of alcohol intoxication (Marczinski, 2011), increasing the amount of alcohol consumed and susceptibility to negative alcohol-related consequences (O'Brien et al., 2008, Arria et al., 2010, Arria et al., 2011, Miller, 2008, Thombs et al., 2010, Berger et al., 2010). The foundations of these claims were based on the hypothesis that the stimulant effects of caffeine counteract the sedative effects of alcohol, resulting in AMED consumers feeling less impaired and less intoxicated than they actually are, and therefore more likely to consume further quantities of alcohol and more likely to take risks. However, as evidenced in a recent meta-analysis (Benson et al., 2014) experimental research has consistently failed to support the notion that mixing alcohol with caffeinated beverages reduces the perceived level of intoxication. Other between-subjects research has also disputed the relationship between AMED consumption and increased alcohol consumption. A survey by Penning et al. found no significant difference in alcohol consumption or next day hangover severity between those that consumed AMED and those that consumed AO Penning et al., 2011. Similarly, Rossheim and Thombs (2011) reported no significant relationship between AMED consumption and the chances of being intoxicated, and intoxication levels for AMED consumers were comparable to those consuming non-caffeinated mixed drinks.
Moreover, some researchers (Skeen and Glenn, 2011, Verster et al., 2012) have questioned the methodological shortcomings of using between-subjects designs to reach causal conclusions on the effects of mixing alcohol with energy drinks on overall alcohol consumption. The main reason for criticism is that this approach does not reveal relevant information about the possible role that energy drinks play in affecting overall alcohol consumption or its related consequences. Even when, as the research outlined shows, AMED individuals consume more alcohol than those who consume AO, this does not imply that mixing alcohol with energy drinks caused increased alcohol consumption. The presented correlations in the surveys between energy drink and alcohol consumption do not imply that one causes the other. In fact, between-subjects comparisons introduce the influence of potential confounders that are not controlled for and may explain the observed differences in the frequency and quantity of alcohol consumption. Therefore, between-subjects comparison surveys are unsuitable and may lead to inappropriate conclusions regarding the need for policy changes to reduce the consumption of AMED.
In order to verify whether mixing alcohol with energy drinks increases overall alcohol consumption and negative alcohol-related consequences some researchers have adopted a within-subjects design. This approach compares the drinking behaviour on AMED occasions with other occasions on which the same people consume AO, therefore controlling for potential between-subject variables. Thus, when using a within-subjects design the only difference between the drinking occasions is the co-consumption of energy drinks allowing causal inferences to be made. Whilst some studies have found small but statistically significant increases in alcohol consumption and negative alcohol-related consequences on AMED occasions compared to AO occasions (Brache and Stockwell, 2011, Peacock et al., 2012, Price et al., 2010), the majority of research has found no difference (Verster et al., 2015) or statistically significant decreases in alcohol consumption and negative alcohol-related consequences (Woolsey et al., 2010, De Haan et al., 2012a, Lubman et al., 2013). For example, in the first large scale survey (Total N = 6002, AMED consumers N = 1239) applying a within-subjects design, De Haan et al., 2012a, De Haan et al., 2012b found that compared with consuming AO, when consuming AMED, students drank significantly fewer alcoholic drinks, reported significantly fewer drinking days and days being drunk, and significantly fewer occasions of consuming more than five alcoholic drinks. In addition, when consuming AMED, significantly fewer negative alcohol-related consequences were reported. In a recent meta-analysis of all within-subject comparisons AMED research Verster et al. (2016) found no significant difference in overall alcohol consumption between AMED and AO occasions. This finding is reflected in recent authoritative evaluation (UK COT, 2012; EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2015) concluding that the mixing of energy drinks with alcohol does not pose any additional risks compared with drinking alcohol on its own.
In summary, research to date suggests that AMED consumers drink significantly more alcohol than AO consumers. However, there does not appear to be any difference in the amount of alcohol consumed by AMED consumers on AMED occasions compared to AO occasions. Some researchers have explained this observed pattern of alcohol consumption as being caused by underlying personality differences between the two groups, such as levels of risk-taking behaviours (Verster et al., 2012). Indeed, much of the previous between-subjects research has found that AMED consumers had higher scores on sensation-seeking, childhood conduct problems, masculine norms and drug use compared to alcohol only consumers (Arria et al., 2010, Arria et al., 2011, Miller, 2008, Berger et al., 2010, Snipes and Benotsch, 2013). Thus a personality with higher levels of risk taking behaviour may be the primary reason for increased alcohol and drug abuse, with the co-consumption of energy drinks being just one of the many expressions of such a lifestyle.
Despite the concerns raised regarding the effects of mixing energy drinks with alcohol there is currently a lack of available data from the UK. Indeed, despite the UK having one of the highest rates of binge drinking in the World (World Health Organization, 2014), in a review of the available research no studies were identified from the UK (Verster et al., 2012). In order to throw light on current energy drink and alcohol use in the UK, a partial replication of the Utrecht survey by De Haan et al., 2012a, De Haan et al., 2012b was conducted, but with students at Universities throughout the UK. The primary aim of this survey was to examine alcohol consumption and its consequences when consumed alone or when mixed with energy drinks using the appropriate within-subjects design. Differences in demographics, alcohol, smoking and drug use between alcohol only and AMED consumers were also explored using between-subjects analysis.
2. Materials and methods
2.1. Sample
All student unions at Universities throughout the UK (N = 139) were contacted via email to ask if they would be willing to act as a gatekeeper and distribute the link to the AMED student survey via their social media platforms (Facebook and Twitter). This link was posted at three stages during the five week data collection period; on the opening day, half way through the data collection period and one week before the survey was due to close. In total 30% of student unions, including institutions from each country (England, Wales, Scotland, Northern Ireland) responded and agreed to take part. Given the nature of using social media as a recruitment method it was not possible to determine the response rate.
The study protocol was reviewed and approved by the University of the West of England Ethics committee. Participation was anonymous and voluntary. In order to reduce the likelihood of non-response bias, those who wished to take part were entered into a monetary prize draw of 1 × £500 and 10 × £50.
A total of 2371 respondents opened the link to the survey. Responses were included if they provided informed consent, were students, 18–30 years old and answered the questions necessary to classify them as one of the drinking groups. After cleaning the data 498 participants were excluded, giving a complete dataset of 1873 student responses. For the analysis in this paper, data were used for the AO group (i.e. those who consumed alcohol and did not mix alcohol with energy drinks, N = 865) and AMED group (those who consumed both AO and AMED, N = 732). Data concerning those who consume both alcohol alone and energy drinks alone but do not mix these on the same drinking occasion, as well as those who do not consume alcohol but consume energy drinks alone will be discussed elsewhere.
2.2. Survey outline
After obtaining informed consent, the first part of the survey assessed demographic data and participants' medication, smoking and drug use, as well as membership to university society/sports group.
Following this, participants were asked a number of questions regarding their consumption of alcohol alone and when mixed with energy drinks. Participants who responded “yes” to whether or not they consumed the particular beverage in question (i.e. do you consume alcohol? or do you consume energy drinks?) were considered current consumers. Alcohol-only consumption was explicitly stated as consuming alcohol (beer, larger, wine, spirits etc) not mixed with energy drinks or other soft drinks. Mixing was defined as consuming energy drinks within a time period of 2 h before through to 2 h after drinking alcohol. This operationalization allowed for both the consumption of alcohol mixed with energy drinks, i.e. Jägerbombs, and the consumption of energy drinks between alcoholic drinks. Alcohol consumption was defined using standardised UK alcohol units (1 standard unit = 10 ml of pure alcohol) (National Health Service, n.d.-c) and one energy drink standardised to 250 ml (containing 80 mg of caffeine). The consumption questions (Table 1) were standard questions adapted from the Quick Drinking Screen (QDS) that investigated participant's consumption habits (frequency and quantity) across differing timescales (one occasion, 30 days, 12 months) considering the particular drink in question. This method has been previously used (Woolsey et al., 2010, De Haan et al., 2012a) with four of the questions having been shown to be highly reliable and consistent when compared to the Timeline Followback method (Roy et al., 2008).
Table 1.
Consumption questions.
| Alcohol only (AO) | Alcohol mixed with energy drinks (AMED) |
|---|---|
| 1. How many standard alcoholic drinks do you usually have on one occasion? 2. In the past 30 days, how many days did you drink alcohol? 3. In the past 30 days, how many days did you get drunk? 4. In the past 30 days, how many times did you have > 5 (males)/4 (females) alcoholic drinks on one occasion? 5. In the past 30 days, what is the greatest number of alcoholic drinks you had on one occasion? 6. On that occasion (previous question), how many hours did you consume alcohol? 7. In the past 12 months, what was the greatest number of alcoholic drinks you consumed on one occasion? |
1a. When you combine, how many standard alcoholic drinks do you usually have on one occasion? 1b. When you combine, how many standard energy drinks do you usually have on one occasion? 2. In the past 30 days, how many days did you combine energy drinks and alcohol? 3. In the past 30 days, while combining, how many days did you get drunk? 4. While combining in the past 30 days, how many times did you have > 5 (males)/4 (females) alcoholic drinks on one occasion? 5a. While combining in the past 30 days, what was the greatest number of alcoholic drinks you consumed on one occasion? 5b. While combining in the past 30 days, what was the greatest number of energy drinks you consumed on one occasion? 6. On that occasion (previous question), how many hours did you consume alcohol? 7. While combining in the past 12 months, what was the greatest number of alcoholic drinks and energy drinks you consumed on one occasion? |
To investigate alcohol-related negative consequences, the Brief Young Adult Alcohol Consequences Questionnaire (BYAACQ) was used (Kahler et al., 2005). The BYAACQ contains 24 possible consequences of alcohol consumption, such as “I have often found it difficult to limit how much I drink” and “My drinking has got me into sexual situations I later regretted”, with participants indicating whether the statement was applicable to them in the past year by answering “yes” or “no”. The total BYAACQ scores range from 0 to 24. In addition to the standard BYAACQ, following De Haan et al., 2012a, De Haan et al., 2012b two additional items were included to determine whether participants were injured or got into a fight after alcohol consumption. Depending on the participant's specific drinking behaviour, the BYAACQ and additional items were completed for AO and AMED drinking occasions.
2.3. Data collection and statistical analysis
Data were collected online via SurveyMonkey® (Palo Alto, CA), cleaned in Microsoft Excel and analysed using the Statistical Package for the Social Sciences version 20 (SPSS Inc., Chicago, IL). The mean, standard deviation and frequency distribution were computed for alcohol consumption and BYAACQ scores for occasions on which participants consumed AO and AMED. Variables with a normal distribution were tested with the Student t-test (Paired t-test for within-subjects, independent t-test for between-subjects). For nominal variables, a Chi Square test was used. For the BYAACQ data, a McNemar test was performed on single items and a paired t-test on the total scores. All tests were two-tailed, and differences were regarded as significant at p < 0.05.
3. Results
3.1. Between-subjects comparisons
The age and gender distribution of the sample obtained was similar to that of students throughout UK Universities (2013). The AO group comprised of 865 participants and the AMED group comprised 732 participants. Between-subjects analysis (Table 2) revealed significant differences in sex and age, with a higher percentage of females in both the AO and AMED group, and relatively more males and younger participants in the AMED group. The groups differed significantly from each other on illicit drug use and smoking, with AMED consumers more likely to take illicit drugs and smoke than AO consumers. In addition AMED consumers were significantly more likely to consume alcohol regularly at an earlier age than the AO group, but there was no significant difference in the age at which each group first consumed alcohol.
Table 2.
Between-subjects demographics of study participants.
| AO group (N = 865) | AMED group (N = 732) | Cohen's d | P value | |
|---|---|---|---|---|
| Male/Female ratio M %/F % (CI%) | 33.1%/66.9% (± 3.1%) | 45.9%/54.1% (± 3.6%) | 0.26 | < 0.001⁎ |
| Age (years), (SD) | 21.0 (2.3) | 20.6 (2.0) | 0.19 | < 0.001⁎ |
| Member of student union % (CI%) | 57.3% (± 3.3%) | 59.6% (± 3.6%) | 0.10 | 0.114 |
| Member of sports/society group % (CI%) | 51.9% (± 3.3%) | 53.8% (± 3.6%) | 0.04 | 0.448 |
| Medication use (past year) % (CI%) | 18.2% (+ 2.6%) | 19.5% (± 2.9%) | 0.04 | 0.480 |
| Illicit Drug use (past year) % (CI%) | 17.8% (± 2.6%) | 24.9% (± 3.1%) | 0.17 | 0.001⁎ |
| Current Smoker % (CI%) | 18.2% (± 2.6%) | 25.8% (± 3.2%) | 0.19 | < 0.001⁎ |
| Age first consumed alcohol (SD) | 14.1 (3.0) | 13.9 (3.0) | 0.07 | 0.089 |
| Age consumed alcohol regularly (SD) | 17.2 (1.9) | 17.0 (1.6) | 0.11 | 0.009⁎ |
Notes: % = yes. 95% CI.
Abbreviations: N, number, , mean, SD, standard deviation, CI, confidence interval, AO, alcohol-only, AMED, alcohol mixed with energy drinks.
Significant differences (p < 0.05) between AO group and AMED group.
In addition, the between-subjects analysis also revealed a consistent pattern of significant differences across all AO consumption questions (all comparisons significantly different at p < 0.001), in that those who consumed AMED drank more alcohol during AO occasions compared to AO consumers. For example, compared with the AO group, the AMED group consumed significantly more alcoholic drinks (8.9 ± 6.0 versus 6.4 ± 4.1, d = 0.48) during an average drinking session, reported significantly more drinking days (7.1 ± 5.3 versus 6.1 ± 4.7, d = 0.20) and days drunk (4.0 ± 3.8 versus 2.8 ± 3.0, d = 0.35) in the past month, and significantly more occasions of consuming more than four (female)/five (male) alcoholic drinks (4.7 ± 4.4 versus 3.3 ± 3.4, d = 0.35). Furthermore, when compared to the AO group, the AMED group consumed significantly more maximum number of drinks on a single occasion in the previous month (12.8 ± 8.5 versus 9.4 ± 6.4, d = 0.45) and the duration of alcohol consumption on this occasion was significantly longer for AMED group compared to AO group (5.8 ± 3.0 versus 5.2 ± 2.8 h, d = 0.21). Finally, the maximum number of alcoholic drinks consumed on one occasion in the past 12 months was higher among the AMED group than the AO group (18.0 ± 9.3 versus 13.7 ± 7.8, d = 0.50).
There were also significant differences (p < 0.001) in alcohol-related negative consequences (BYAACQ), with AMED consumers experiencing significantly more overall negative alcohol-related consequences compared to AO consumers, on AO occasions (9.0 ± 5.4 versus 6.6 ± 4.7, d = 0.47).
3.2. Within-subjects analysis for AMED group
To establish whether mixing energy drinks with alcohol had an impact on total alcohol consumption, within-subjects comparisons were performed for members of the AMED group (N = 732), comparing occasions on which they consumed AMED with occasions on which they consumed AO. As can be seen in Fig. 1. the analysis revealed statistically significant differences across all consumption questions (p < 0.001) indicating generally lower frequency and quantity of alcohol consumption when combining with energy drinks compared to consuming alcohol alone. For example, compared to consuming AO, when consuming AMED, participants consumed significantly fewer alcoholic drinks during an average drinking session (6.0 ± 4.9 versus 9.0 ± 6.1, d = 0.54), reported significantly fewer drinking days (2.3 ± 2.8 versus 7.0 ± 5.3, d = 1.11) and days drunk (2.1 ± 2.7 versus 4.0 ± 3.8, d = 0.58) in the past month, and significantly fewer occasions consuming more than four (female)/five (male) alcoholic drinks (2.1 ± 2.9 versus 4.7 ± 4.4, d = 0.70). They also consumed fewer maximum number of alcoholic drinks (7.0 ± 7.9 versus 12.9 ± 8.6, d = 0.72) on a single occasion in the previous month, and the duration of alcohol consumption on this occasion was significantly shorter (4.5 ± 3.2 versus 5.8 ± 2.9 h, d = 0.43) when consuming AMED than when consuming AO. Finally, when consuming AMED they consumed fewer alcoholic drinks on a single occasion in the previous years than when consuming AO (7.0 ± 6.8 versus 17.9 ± 9.4, d = 1.33).
Fig. 1.
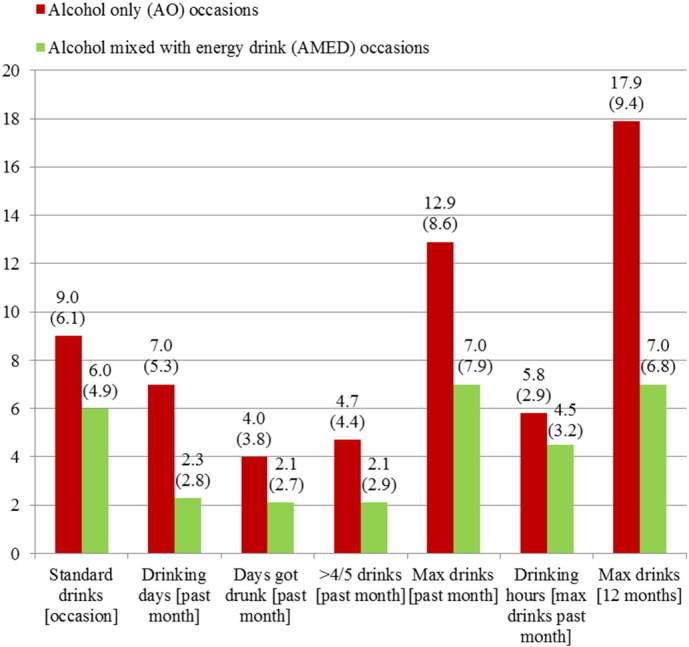
UK Student Survey: Means (standard deviations) for within-subjects comparisons of AMED group (N = 732) on consumption questions for AO occasions and AMED occasions.
Notes: Questions are specifically asked for both conditions (consuming solely alcohol/consuming alcohol mixed with energy drinks). All differences are significant at the p < 0.001 level.
Confirmation of alcohol-related consequences when consuming AMED or AO are summarised in Table 3. The within-subjects comparisons show that across all items when consuming AMED alcohol-related negative consequences were experienced significantly less when compared with consuming AO. There was a 21% reduction in the total BYAACQ score, from 9.0 ± 5.4 for drinking AO to 7.1 ± 5.1 for AMED (p ≤ 0.001, d = 0.36). None of the individual items showed an increased chance of experiencing an alcohol-related negative consequence on AMED occasions compared with drinking AO.
Table 3.
Within-subjects comparison in the AMED group (N = 732) on BYAACQ items for occasions on which they consumed alcohol-only compared with the occasions on which they mixed alcohol with energy drinks.
| Within-subjects comparison |
|||||
|---|---|---|---|---|---|
| BYAACQ | AO occasions | AMED occasions | Cohen's d | P value | |
| I have had a hangover (headache, sick stomach) the morning after I had been drinking % (CI%) | 86.2% (± 2.8%) | 77.1% (± 3.4%) | 0.43 | < 0.001 | |
| I have had less energy or felt tired because of my drinking % (CI%) | 69.6% (± 3.7%) | 50.3% (± 4.0%) | 0.74 | < 0.001 | |
| I have had felt very sick to my stomach or thrown up after drinking % (CI%) | 60.8% (± 3.9%) | 49.2% (± 4.0%) | 0.45 | < 0.001 | |
| I've not been able to remember large stretches of time while drinking heavily % (CI%) | 60.6% (± 4.0%) | 50.3% (+ 4.0%) | 0.40 | < 0.001 | |
| While drinking, I have said or done embarrassing things % (CI%) | 73.5% (± 3.6%) | 61.6% (± 3.9%) | 0.55 | < 0.001 | |
| I often have ended up drinking on nights when I had planned not to drink % (CI%) | 52.8% (± 4.0%) | 32.4% (± 3.8%) | 0.76 | < 0.001 | |
| I have taken foolish risks when I have been drinking % (CI%) | 51.1% (± 4.0%) | 45% (± 4.0%) | 0.27 | 0.001 | |
| I have not gone to work or missed classes at school because of drinking, a hangover or illness caused by drinking % (CI%) | 47.7% (± 4.0%) | 41.4% (± 4.0%) | 0.30 | < 0.001 | |
| The quality of my work or school work has suffered because of my drinking % (CI%) | 28.9% (± 3.7%) | 19% (± 3.2%) | 0.50 | < 0.001 | |
| When drinking, I have done impulsive things I regretted later % (CI%) | 38.9% (± 3.9%) | 33.3% (± 3.8%) | 0.29 | 0.001 | |
| I have found that I needed larger amounts of alcohol to feel any effect, or that I could no longer get high or drunk on the amount that used to get me high or drunk % (CI%) | 34.8% (± 3.9%) | 26.7% (± 3.6%) | 0.47 | < 0.001 | |
| I have felt badly about myself because of my drinking % (CI%) | 25.8% (± 3.5%) | 20.9% (± 3.3%) | 0.29 | < 0.001 | |
| My drinking has got me into sexual situations I later regretted % (CI%) | 33.8% (± 3.8%) | 26.5% (± 3.6%) | 0.38 | < 0.001 | |
| I have been overweight because of drinking % (CI%) | 19.4% (± 3.2%) | 15.4% (± 2.9%) | 0.26 | 0.002 | |
| I have spent too much time drinking % (CI%) | 31.1% (± 3.7%) | 21.9% (± 3.3%) | 0.51 | < 0.001 | |
| I have often found it difficult to limit how much I drink % (CI%) | 31.4% (± 3.8%) | 26.5% (± 3.6%) | 0.27 | 0.001 | |
| I have neglected my obligations to family, work, or school because of drinking % (CI%) | 19.5% (± 3.2%) | 14.3% (± 2.8%) | 0.37 | < 0.001 | |
| My drinking has created problems between myself and my boyfriend/girlfriend/spouse, parents, or other near relatives % (CI%) | 17.7% (± 3.1%) | 11.5% (± 2.6%) | 0.42 | < 0.001 | |
| I have woken up in an unexpected place after heavy drinking % (CI%) | 22.9% (± 3.4%) | 16.3% (± 3.0%) | 0.43 | < 0.001 | |
| My physical appearance has been harmed by my drinking % (CI%) | 22.6% (± 3.4%) | 16.5% (+ 3.0%) | 0.36 | < 0.001 | |
| I have become very rude, obnoxious, or insulting after drinking % (CI%) | 26% (± 3.5%) | 21.7% (± 3.3%) | 0.24 | 0.003 | |
| I have driven a car when I knew I had too much to drink to drive safely % (CI%) | 9.5% (± 2.4%) | 7.5% (± 2.1%) | 0.16 | 0.043 | |
| I have felt like I needed a drink after I′d gotten up (that is, before breakfast) % (CI%) | 7.6% (± 2.1%) | 4.1% (± 1.6%) | 0.29 | < 0.001 | |
| I have passed out from drinking % (CI%) | 26.5% (± 3.6%) | 19.4% (± 3.2%) | 0.43 | < 0.001 | |
| Total BYAACQ score mean (SD) | 9.0 (5.4) | 7.1 (5.1) | 0.36 | < 0.001 | |
| #I have physically injured myself or others after drinking –separate to being in a fight % (CI%) | 25.5% (± 3.5%) | 20% (± 3.2%) | 0.33 | < 0.001 | |
| #I have got into a fight after drinking % (CI%) | 12.7% (± 2.7%) | 9.7% (± 2.4%) | 0.24 | 0.003 | |
Notes: % = yes. 95% CI. #Additional question added by the authors. All differences between AO group and AMED group are significant at p < 0.05.
Abbreviations:, mean, SD, standard deviation, CI, confidence interval, AO, alcohol-only, AMED, alcohol mixed with energy drinks, BYAACQ-Brief Young Adult Alcohol Consequences Questionnaire.
4. Discussion
The results of this survey show that people who mix alcohol with energy drinks consumed significantly fewer alcoholic drinks when they combine alcohol with energy drinks compared to when they consume alcohol alone. In addition, there was a reduction in the number of reported alcohol-related consequences when consuming AMED compared to consuming AO. These results are comparable with previous within-subjects comparisons (Woolsey et al., 2010, De Haan et al., 2012a, Lubman et al., 2013) and provides further support that mixing alcohol with energy drinks does not increase overall alcohol consumption or the likelihood of experiencing negative alcohol-related consequences such as driving whilst intoxicated. These findings are of importance given that some authors (Arria et al., 2011, Howland and Rohsenow, 2013) have made premature calls for policy changes to reduce the consumption of AMED based on inappropriate between-subjects comparisons.
Despite the findings that AMED does not increase the relative negative impact on overall alcohol consumption or negative consequences in comparison to AO consumption, the data indicates that regardless of consumption occasion the majority of students (87% alcohol-only occasions, 69% AMED occasions) still consumed alcohol above the levels generally accepted as safe in the UK. Thus, the majority of students engaged in binge drinking, and this increased on days when they did not consume AMED. In addition, the number of reported alcohol-related negative consequences across both drinking occasions were alarming. Therefore, it is clear that alcohol abuse is an ongoing problem among UK students and further work is needed, including the promotion of protective behavioural strategies, to reduce excessive alcohol consumption and its knock on effects of negative consequences. However, the findings from this survey suggest that the pre-occupation with AMED consumption is only diverting attention away from the more pressing issue of excessive alcohol consumption per se.
The significance of these findings lies in the fact that this is a large scale survey, using a within-subjects design, to collect data on students from across the UK. The demographics of the current sample reflect those of the general student population in the UK Universities (2013) supporting the generalization of the results to all UK students. However, this must be done with caution given that convenience sampling via social media was used, meaning it was not possible to determine the response rate and marginalized sections of the student population may have been excluded. In addition, as with all retrospective AMED surveys, the ability of students to reliably recall the number and type of drinks consumed in the past is likely to be affected by the high volume of alcohol reportedly consumed on these occasions. This is especially the case for recalling drinking occasions within the last 12 months, which may make it difficult to differentiate whether an alcohol related consequence occurred on an AMED or AO occasion. However, an advantage of using a within-subjects design is that any between-subject differences in recall bias are controlled for. To completely rule out the possibility of recall bias, prospective studies are required. However, this approach is expensive and time consuming.
A further limitation is that the sample obtained focused on university students, therefore the results cannot be generalized beyond this population. Given the unique drinking practices of university students, future research could usefully investigate alcohol and AMED consumption among different sub-populations.
5. Conclusions
This UK student survey found that although AMED consumers drink more alcohol and engage in more harmful behaviours than AO consumers, on AMED occasions they drank less alcohol and engaged in fewer harmful behaviours compared to alcohol only occasions. These findings provide support to the growing body of evidence that mixing alcohol with energy drinks does not increase total alcohol consumption or alcohol-related negative consequences. However, excessive alcohol consumption and associated alcohol related harms remain a persistent concern among the UK student population.
Author contributions
SJ led the study presented in this paper; collected, analysed, interpreted the data and drafted the manuscript. CA, JV and KS participated in the design and coordination of the study and helped to draft and review the manuscript. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content. All authors read and approved the final manuscript.
Conflicts of interest
Red Bull GmbH had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
Sean J Johnson has been involved in sponsored research for Pfizer, AstraZeneca, Merck, Gilead, Novartis, Roche and Red Bull GmbH. Chris Alford has undertaken sponsored research, or provided consultancy, for a number of companies and organisations including Astra, British Aerospace/BAeSystems, Civil Aviation Authority, Duphar, FarmItalia Carlo Erba, Ford Motor Company, ICI, Innovate UK, Janssen, LERS Synthélabo, Lilly, Lorex/Searle, Ministry of Defense, Quest International, Red Bull GmbH, Rhone-Poulenc Rorer, Sanofi Aventis. Joris C Verster has received grants/research support from The Dutch Ministry of Infrastructure and the Environment, Janssen, Nutricia, Takeda, Red Bull, and has acted as a consultant for Canadian Beverage Association, Centraal Bureau Drogisterijbedrijven, Coleman Frost, Danone, Deenox, Eisai, Janssen, Purdue Pharma, Red Bull, Sanofi-Aventis, Sepracor, Takeda, Transcept, Trimbos Institute, and Vital Beverages. Karina Stewart has no competing interests.
Acknowledgments
This survey was financially supported by Red Bull GmbH as part of a PhD studentship.
The authors are grateful to the UK university students unions who advertised the survey and the students who took the time to participate.
References
- Arria A.M., Caldeira K.M., Kasperski S.J. Increased alcohol consumption, nonmedical prescription drug use, and illicit drug use are associated with energy drink consumption among college students. J. Addict. Med. 2010;4(2):74–80. doi: 10.1097/ADM.0b013e3181aa8dd4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria A.M., Caldeira K.M., Kasperski S.J., Vincent K.B., Griffiths R.R., O'Grady K.E. Energy drink consumption and increased risk for alcohol dependence. Alcohol. Clin. Exp. Res. 2011;35:365–375. doi: 10.1111/j.1530-0277.2010.01352.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berger L.K., Fendrich M., Chen H.Y., Arria A.M., Cisler R.A. Sociodemographic correlates of energy drink consumption with and without alcohol: results of a community survey. Addict. Behav. 2010;36:516–519. doi: 10.1016/j.addbeh.2010.12.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benson S., Verster J.C., Alford C., Scholey A. Effects of mixing alcohol with caffeinated beverages on subjective intoxication: a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2014;47:16–21. doi: 10.1016/j.neubiorev.2014.07.008. [DOI] [PubMed] [Google Scholar]
- Brache K., Stockwell T. Drinking patterns and risk behaviors associated with combined alcohol and energy drink consumption in college drinkers. Addict. Behav. 2011;36(12):1133–1140. doi: 10.1016/j.addbeh.2011.07.003. [DOI] [PubMed] [Google Scholar]
- De Haan L., de Haan H.A., van der Palen J., Olivier B., Verster J.C. Effects of consuming alcohol mixed with energy drinks versus consuming alcohol only on overall alcohol consumption and negative alcohol-related consequences. Int. J. Gen. Med. 2012;5:953–960. doi: 10.2147/IJGM.S38020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Haan L., de Haan H., Olivier B., Verster J.C. Alcohol mixed with energy drinks: methodology and design of the Utrecht Student Survey. Int. J. Gen. Med. 2012;5:889–898. doi: 10.2147/IJGM.S37401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eckschmidt F., Guerra de Andrade A., dos Santos B., Garcia de Oliveira L.C. The effects of alcohol mixed with energy drinks (AmED) on traffic behaviours among Brazilian college students: a national survey. Traffic Inj. Prev. 2013;14:671–679. doi: 10.1080/15389588.2012.755261. [DOI] [PubMed] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies) Scientific opinion on the safety of caffeine. EFSA J. 2015;13(5):4102. 120 pp. [Google Scholar]
- Flotta D., Micò R., Nobile C.G.A., Pileggi C., Bianco A., Pavia M. Consumption of energy drinks, alcohol, and alcohol-mixed energy drinks among Italian adolescents. Alcohol. Clin. Exp. Res. 2014;38:1654–1661. doi: 10.1111/acer.12394. [DOI] [PubMed] [Google Scholar]
- Health and Social Care Information Centre Statistics on alcohol-England. 2015. http://www.hscic.gov.uk/catalogue/PUB17712/alc-eng-2015-rep.pdf
- Howland J., Rohsenow D.J. Risks of energy drinks mixed with alcohol. JAMA. 2013;309(3):245–246. doi: 10.1001/jama.2012.187978. [DOI] [PubMed] [Google Scholar]
- Kahler C.W., Strong D.R., Read J.P. Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: the brief young adult alcohol consequences questionnaire. Alcohol. Clin. Exp. Res. 2005;29(7):1180–1189. doi: 10.1097/01.alc.0000171940.95813.a5. [DOI] [PubMed] [Google Scholar]
- Lubman D.L., Peacock A., Droste N. Alcohol and energy drinks in NSW. (a,b) 2013. www.health.nsw.gov.au Available at.
- Marczinski C.A. Alcohol mixed with energy drinks: consumption patterns and motivations for use in US college students. Int. J. Environ. Res. Public Health. 2011;8(8):3232–3245. doi: 10.3390/ijerph8083232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller K.E. Energy drinks, race, and problem behaviors among college students. J. Adolesc. Health. 2008;43:490–497. doi: 10.1016/j.jadohealth.2008.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Health Service Alcohol misuse. http://www.nhs.uk/conditions/Alcohol-misuse/Pages/Introduction.aspx
- National Health Service Binge drinking. http://www.nhs.uk/Livewell/alcohol/Pages/
- National Health Service Alcohol units. http://www.nhs.uk/Livewell/alcohol/Pages/alcohol-units.aspx
- O'Brien M.C., McCoy T.P., Egan K.L., Goldin S., Rhodes S.D., Wolfson M. Caffeinated alcohol, sensation seeking, and injury risk. J. Caffeine Res. 2013;3:59–66. doi: 10.1089/jcr.2013.0004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Brien M.C., McCoy T.P., Rhodes S.D., Wagoner A., Wolfson M. Caffeinated cocktails: energy drink consumption, high-risk drinking, and alcohol-related consequences among college students. Acad. Emerg. Med. 2008;15(5):453–460. doi: 10.1111/j.1553-2712.2008.00085.x. [DOI] [PubMed] [Google Scholar]
- Office for National Statistics Opinions and lifestyle survey, drinking habits amongst adults. http://www.ons.gov.uk/ons/rel/ghs/opinions-and-lifestyle-survey/drinking-habits-amongst-adults--2012/sty-alcohol-consumption.html
- Peacock A., Bruno R., Martin F.H. The subjective physiological, psychological, and behavioral risk-taking consequences of alcohol and energy drink co-ingestion. Alcohol. Clin. Exp. Res. 2012;36(11):2008–2015. doi: 10.1111/j.1530-0277.2012.01820.x. [DOI] [PubMed] [Google Scholar]
- Price S.R., Hilchey C.A., Darredeau C., Fulton H.G., Barrett S.P. Energy drink co-administration is associated with increased reported alcohol ingestion. Drug Alcohol Rev. 2010;29:331–333. doi: 10.1111/j.1465-3362.2009.00163.x. [DOI] [PubMed] [Google Scholar]
- Penning R., de Haan L., Verster J.C. Caffeinated drinks, alcohol consumption, and hangover severity. Open Neuropsychopharmacol. J. 2011;4:36–39. [Google Scholar]
- Rossheim M.E., Thombs D.L. Artificial sweeteners, caffeine, and alcohol intoxication in bar patrons. Alcohol. Clin. Exp. Res. 2011;35:1891–1896. doi: 10.1111/j.1530-0277.2011.01534.x. [DOI] [PubMed] [Google Scholar]
- Roy M., Dum M., Sobell L.C. Comparison of the quick drinking screen and the alcohol timeline followback with outpatient alcohol abusers. Subst. Use Misuse. 2008;43:2116–2123. doi: 10.1080/10826080802347586. [DOI] [PubMed] [Google Scholar]
- Skeen M.P., Glenn L.L. Imaginary link between alcoholism and energy drinks. Alcohol. Clin. Exp. Res. 2011;35:1375–1376. doi: 10.1111/j.1530-0277.2011.01585.x. [DOI] [PubMed] [Google Scholar]
- SS L., Vos T., Flaxman A.D. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snipes D.J., Benotsch E.G. High-risk cocktails and high-risk sex: examining the relation between alcohol mixed with energy drink consumption, sexual behavior, and drug use in college students. Addict. Behav. 2013;38(1):1418–1423. doi: 10.1016/j.addbeh.2012.07.011. [DOI] [PubMed] [Google Scholar]
- Thombs D.L., O'Mara R.J., Tsukamoto M. Event-level analyses of energy drink consumption and alcohol intoxication in bar patrons. Addict. Behav. 2010;35:325–330. doi: 10.1016/j.addbeh.2009.11.004. [DOI] [PubMed] [Google Scholar]
- UK COT . December 2012. Statement on the Interaction of Caffeine and Alcohol and Their Combined Effects on Health and Behaviour. [Google Scholar]
- UNESDA UNESDA code for the labelling and marketing of energy drinks. 2012. www.unesda.org Available at.
- UK Universities Patterns and Trends in UK Higher Education. 2013. http://www.universitiesuk.ac.uk/highereducation/Documents/2013/PatternsAndTrendsinUKHigherEducation2013.pdf
- Velazquez C.E., Poulos N.S., Latimer L.A., Pasch K.E. Associations between energy drink consumption and alcohol use behaviors among college students. Drug Alcohol Depend. 2012;123(1):167–172. doi: 10.1016/j.drugalcdep.2011.11.006. [DOI] [PubMed] [Google Scholar]
- Verster J.C., Aufricht C., Alford C. Energy drinks mixed with alcohol: misconceptions, myths, and facts. Int. J. Gen. Med. 2012;5:187–198. doi: 10.2147/IJGM.S29313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster J.C., Benjaminsen J.M.E., van Lanen J.H.M., van Stavel N.M.D., Olivier B. Effects of mixing alcohol with energy drink on objective and subjective intoxication: results from a Dutch on-premise study. Psychopharmacology. 2015;232:835–842. doi: 10.1007/s00213-014-3715-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster J.C., Benson S., Johnson S.J., Scholey A., Alford C. Mixing alcohol with energy drink (AMED) and total alcohol consumption: a systematic review and meta-analysis. Human Psychopharmacol. 2016;31(1):2–10. doi: 10.1002/hup.2513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolsey C., Waigandt A., Beck N.C. Athletes and energy drinks: reported risk-taking and consequences from the combined use of alcohol and energy drinks. J. Appl. Sport Psychol. 2010;22:65–71. [Google Scholar]
- World Health Organization . 2014. Global Status Report on Alcohol and Health. Geneva. [Google Scholar]