

Abstract
Objectives:
To investigate whether healthy foods in Saudi Arabia cost more compared with less healthy options.
Method:
This is a cross-sectional study conducted in Riyadh, Saudi Arabia during June and July 2015. The study targeted well-known market chains in the city of Riyadh. The selection of food items was purposive to include healthy and less healthy food items in each category. Price, caloric value, salt, fat, sugar, and fiber contents for each food item were collected. To test for the correlation between nutritional contents and average price, Spearman’s correlation coefficients were calculated. The Mann-Whitney U test was used to test for the presence of average price difference between healthy and less healthy food items.
Results:
A total of 162 food items were collected. Sixty-six food items were classified as healthy compared with 96 less healthier options. The calculated correlation coefficients indicate an association between increased cost of food with increased caloric values (0.649 p=0.0000001), increased fat content (0.610 p=0.0000003), and increased salt contents (0.273 p=0.001). Prices of food items with higher fiber contents showed a weaker association (0.191 p=0.015). The overall average cost of healthy food was approximately 10 Saudi riyals cheaper than less healthy food (p=0.000001).
Conclusion:
The findings of the study suggest that the cost of healthy food is lower than that of less healthy items in the Saudi market.
The consumption of unhealthy food and decreased physical activity are important risk factors for chronic non-communicable diseases (NCD). The World Health Organization (WHO) reported that unhealthy eating behavior is an important contributor for cardiovascular diseases and certain cancers. Approximately 1.7 million deaths occurring globally could be attributed to the low consumption of vegetables and fruits.1 Several investigations conducted in Saudi Arabia have indicated a progressive increase of obesity among the Saudi population.2-7 The Saudi Health Interview Survey (SHIS) published in 2013 revealed that the prevalence of obesity among Saudis is 28.7%.8 Additionally, the prevalence of metabolic syndrome among Saudis aged between 30 and 70 has been reported to reach 39.3%.9 Prevalence of obesity and its complications in the Saudi population has been partially attributed to unhealthy dietary habits, where elevated consumption of food items high in sugar and, fat and lower intake of fruits and vegetables were witnessed.2,8,10,11 Adherence to a healthy lifestyle can result in reduction of NCD despite the presence of augmenting factors, such as familial history of diseases. A systematic review studied published randomized controlled trials, which investigated the effect of exercise and a healthier diet with regard to increased risk of type 2 diabetes development. It revealed that combined physical activity and balanced diet reduced the risk of the disease (relative risk: 0.63, 95% confidence interval: 0.49 to 0.79).12 Additionally, a longitudinal study indicated that lifestyle intervention reduced the incidence of obesity and type 2 diabetes, even among subjects with a family history of diabetes.13 Given the importance of balanced diet in reducing the burden of NCD, several local and global initiatives were conducted to encourage higher consumption of vegetables and fruits. The WHO and the Food and Agricultural Organization (FAO) launched an initiative in 2003 to promote higher consumption of fruits and vegetables worldwide.1 Locally, the Saudi Ministry of Health produced the Dietary Guidelines for Saudis, which encouraged the higher consumption of wholegrain food items, higher consumption of fruits and vegetables, and lower consumption of food items rich in carbohydrates, salt, and fat.14 It has been postulated that lower consumption of healthy food items could be due to the elevated cost of healthy food compared with non-healthy food items. A systematic review was performed to assess the cost of healthy food in comparison with less healthy food. This review included 27, studies where most of the studies were from European and North American countries except for 5 studies which were conducted in Brazil, Japan, South Africa, and New Zealand. This review reveales that healthy food options were relatively more expensive compared with non-healthy options.15 The difference was mostly observed with the meats group. The cost of healthy food options in Saudi Arabia compared with other non healthier options is currently unknown. Although the current best evidence indicates that healthy food costs more internationally, none of the studies included in this systematic review was conducted in Arabian countries. A difference in the price variation between healthy and non-healthy food options is expected in Saudi Arabia, given the different economic status of Saudi Arabia compared with other countries. This study aims to investigate whether healthy food items in Saudi Arabia cost more compared with other less healthy options. The importance of this study relies on identifying whether adherence to the Dietary Guidelines for Saudis is more expensive or not.
Methods
Study context
This investigation is a cross-sectional study conducted in Riyadh, Saudi Arabia during June and July 2015. The study targeted well-known market chains in the city of Riyadh which have nationwide branches. Three different chains were targeted where prices of food items were recorded. Targeting more than one chain was carried out to measure any possible variation of prices of the same food items. Ethical approval to conduct the study was provided by the ethical committee of the College of Medicine at King Saud University, Riyadh, Saudi Arabia.
Data collection
Data were collected using a Microsoft Excel 2007 spreadsheet. The spreadsheet was designed to facilitate the collection of information related to name, caloric value, salt, fat, sugar, and fibers contents, and price of food items in each store. Food items were categorized into 2 market baskets including healthier versus less healthy baskets within several food groups including meats, dairy products, grain products, fruits, vegetables, snacks, drinks, and oils. The selection of food items was purposive to include healthy and less healthy food items in each category. In-store surveys were conducted by 2 trained investigators. The surveys were conducted by inspecting price labels of the selected food items and inspection of the nutritional profile label of each food item. Prices of food items were validated by recording the price of the same brand of each food item in each supermarket where 3 different supermarkets were involved in this survey. The price of each food item was the average of the prices recorded in each supermarket. Nutritional information of each food item was collected by recording the nutritional label provided on each item. However, if no nutritional information was provided by the producer, nutritional databases, such as the National Nutrient Database for Standard Reference in the United States of America (USDA)16 and the Canadian Nutrient File (CNF)17 were consulted. Standardized units of 100 g (for solid food) and 100 ml (for liquid food) were used to measure the nutritional content of each food item. The units of the nutritional profile were presumed as kcal for calories, mg of sodium for salt content, and g for fibers, fat, and carbohydrates. To standardize prices of food items in Saudi riyals, a unit of one kg or one liter was used as a unified price indicator for all food items.
Statistical analysis
Data analysis was performed using the Statistical Package for Social Sciences version 22 (IBM Corp., Armonk, NY, USA). To assess the association between the prices index and nutritional information, data analysis was performed through 2 steps. First, correlations between caloric value, salt, fibers, fat, and carbohydrate contents with the average price were calculated; Second, food items were divided into 2 groups within each food category, where one group was presumed healthy and the other was presumed less healthy in comparison. Healthfulness assumption was based on each food item having lower caloric value, salt, fat, carbohydrate, and higher fibers contents compared with other food items within the same group. For example, grain-based items were presumed healthy if they were wholegrain products in comparison with the less healthy options of non-wholegrain products. Non-parametric tests were used in this study as the collected variables did not follow normal distribution. To test for the correlation between nutritional contents and average price, Spearman’s correlation coefficients were calculated. The Mann-Whitney U test was used to test for the presence of average price difference between healthy and less healthy food items within each food category. A p-value of 0.05 or less was designated as statistically significant for applied statistical tests.
Results
A total of 162 food items were collected. Sixty-six food items were classified as healthy compared with 96 less healthier options. A summary of healthy and less healthy food items are described in Table 1. The correlation of average food price with caloric value, salt, fibers, fat, and carbohydrates contentsare illustrated in Table 2. The calculated correlation coefficients indicate a moderate association between increased cost of food with increased caloric values and fat content of food items in the Saudi markets (Spearman’s coefficient of 0.649 for correlation with caloric value and 0.61 for correlation with fat content). Additionally, a smaller association was detected between average price and salt content (Spearman’s coefficient of 0.273). Carbohydrates content was not significantly associated with average cost of food. The increased cost of food with higher caloric value, fat, and salt indicates that healthier options are relatively cheaper than less healthier options. On the other hand, a weak association between fibers content and cost was detected (Spearman’s coefficient of 0.191). This association suggests that food items with higher fiber contents costs more compared with other items with lower fiber contents in the Saudi market. Table 3 and Figure 1 compare the cost of healthy food items with the less healthy options. By the overall difference of cost of the total sample, it is noticeable that healthier options are cheaper. Most food products revealed no significant difference in the cost of healthy food compared with less healthy options. Only dairy products and vegetable prices indicated a statistically significant difference where healthier options were cheaper in the Saudi market. The significantly increased price of less healthy food items within the dairy products category was mostly driven by cheese and cream products. These products are rich in fat contents and cost more compared with other healthier options, such as labnah and yoghurt. It was similarly observed within the vegetable category that healthier vegetables options were cheaper. This difference was mostly affected by the availability of more expensive canned vegetables products, where higher levels of salt were detected when compared with the cheaper fresh vegetables. Additionally, certain fruits were classified as less healthier options when having higher levels of carbohydrates (such as, dates, banana, and canned fruits) in comparison with other fruits. Nonetheless, no statistically significant difference was detected, indicating that healthier options are not more expensive in comparison with the less healthy products. Within the meats category, the study was not able to detect a statistically significant difference of prices when comparing healthy meat products with less healthy ones. However, it was noted that processed meat products, such as kebabs and burgers, which are rich in added salt and fat contents are relatively cheaper than fresh meat products. However, only chicken-based processed products were more expensive than fresh chicken meat. Nonetheless, we cannot neglect the effect of value-added components to the chicken-based processed products on increasing the price. It was also observed that lamb meat is more expensive than veal or camel meat in the Saudi market, where lamb meat has a higher fat content compared with veal or camel meat. Out of the 16 grain products collected in this study, only 3 were wholegrain products. The healthier wholegrain products are noticeably more expensive compared with the non-wholegrain ones. However, the abundance of non-wholegrain products compared with wholegrain ones might affect consumers’ selection of healthy grain products in the Saudi markets. Twenty-five different types of sweets and snacks were collected in this study; most of them were rich in caloric value and salt content. Additionally, snacks which were produced using wholegrain products had relatively lower levels of caloric values and were cheaper in comparison with the less healthy options. Five different oil brands related to 3 different types of oil products were identified. The caloric value and fat contents of corn, sunflower, and olive oils were almost identical. Therefore, it was difficult to assume healthy oil products in comparison. However, olive and corn oils were relatively high in saturated fat contents and more expensive compared with sunflower oil. Eight different types of drinks were collected. The average cost of soft drinks, juices, and fruit-based drinks was similar. Additionally, the caloric values which are mostly driven by carbohydrates were similar. However, diet drinks which can be labeled as healthy compared with sugary soft drinks contain higher levels of salt than non-diet products. Therefore, it was difficult to assume, which drinks are relatively healthy compared with other drinks. Twenty-two food items included in this study were either processed meats products, or canned vegetables and fruits. It is speculated that these products which have value-added components are likely to cost more compared with similar fresh and unprocessed products. Including these food items to the comparison list might affect the overall comparison between healthy and less healthy options. To investigate this issue, a smaller food baskets were formed where the healthy basket would contain food items with low sugar, fat, and salt content and compared with a less healthy basket, which would contain food items with high sugar, fat, and salt content where both baskets contained food items with the same level of processing. Selection of food items within these smaller baskets was based on comparing each food items with its similar less healthier option, such as comparing low fat milk and whole milk, low-sugar fresh fruits and high-sugar fresh fruit, and skinless chicken compared with regular chicken. This smaller basket only contained 24 healthy food items compared with 24 similar less healthier versions excluding processed meats products and canned fruits and vegetables. The healthy basket was only 1.11 SR more expensive than the less healthy basket, where this difference was not statistically significant (p=0.665). The low difference in the cost of healthy basket compared with the less healthy basket is mostly driven by the similarity of prices of low fat milk, laban, cream, labnah, and yogurt compared with full fat ones, which are almost identical in the Saudi market.
Table 1.
Summary of healthy and less healthy food items in the Saudi market.
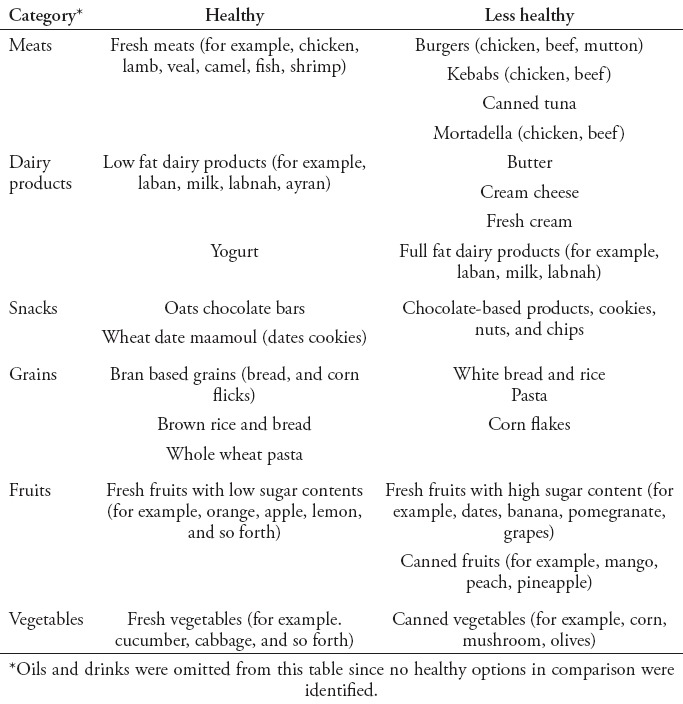
Table 2.
Association of food price in Saudi Riyal with nutritional profile in the Saudi market.
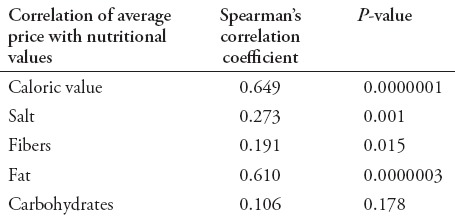
Table 3.
Comparison of cost in Saudi Riyal of healthy and less healthy food items found in the Saudi market.
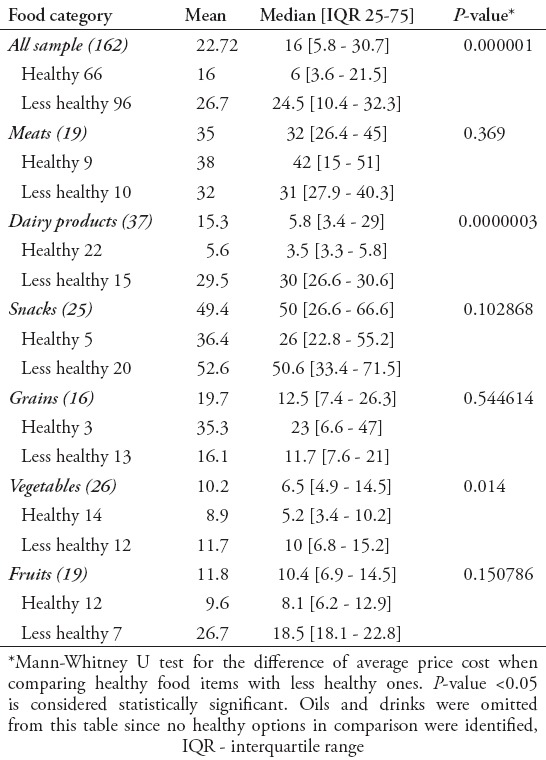
Figure 1.
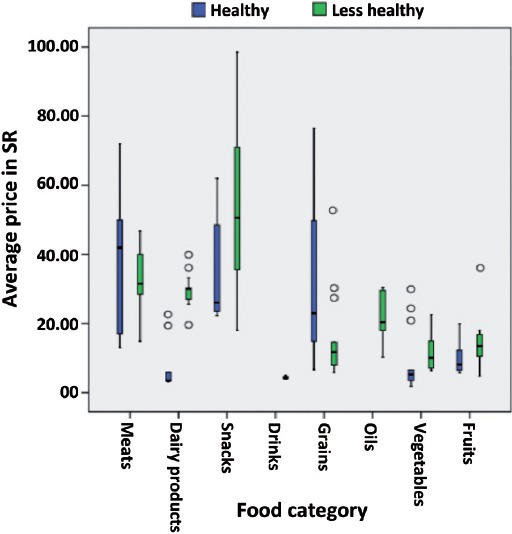
Boxplot of comparison between average cost of healthy compared with less healthy food items in the Saudi market. SR - Saudi Riyal
Discussion
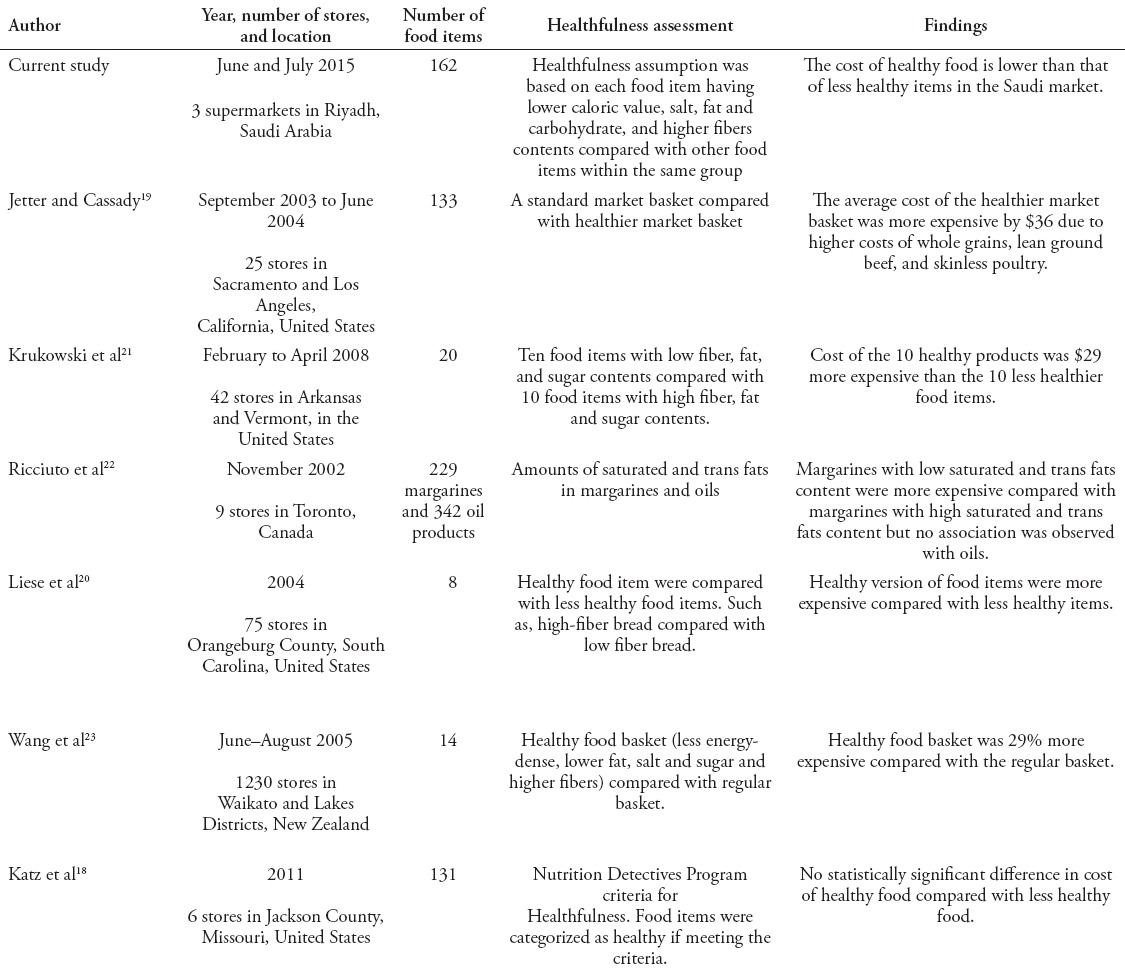
This study aimed to investigate whether healthy food options cost more compared with less healthy items in the Saudi market. The findings of this study suggest that healthy food options are relatively cheaper. This suggestion is mostly influenced by the lower average cost of food items, which are lower in caloric value, fat, and salt contents. The findings were consistent when categorizing the sample according to food types, as the cost of healthy food was not significantly more expensive than the less healthy options. Table 4 summarizes similarities and differences of the current study compared with similar previous studies conducted in other areas. Major methodological variations are witnessed including number of food items and assessment of healthfulness. However, the study by Katz et al18 is the most similar one to the current study. Katz et al18 compared the cost of consuming healthy food with less healthy food in the US market and revealed no significant difference between the prices of the 2 groups. However, the remaining studies indicated higher cost of healthy food compared with less healthy options. The systematic review by Rao et al15 investigating the cost of healthy food in 10 different countries, indicated that only healthy meat products were significantly more expensive than less healthy meats. Additionally, a study19 revealed that the cost of a healthier market basket in the US was $36 more expensive than the average non-healthy basket. The cost of the healthy basket was higher owing to the elevated cost of wholegrain and healthy meat products.19 This notion is similar to what was observed in our study, where wholegrain products were more expensive than non-wholegrain products. However, the availability of wholegrain products was limited in our study. Although this study surveyed 3 large scale nationwide supermarket chains, the availability or even pricing of healthy food could differ if this research was conducted in rural areas with limited access to large stores. A US study20 revealed variability of prices of the same healthy food items in rural areas. It suggested that healthier options were relatively less expensive in supermarkets compared with convenience stores.20 Similarly, another study21 indicated more favorable prices for healthy food offered in large stores compared with smaller ones. The current study suggests that the cost of consuming healthy food is not largely more expensive than less healthy items. However, the findings of this study can only be generalized to urban areas in Saudi Arabia. The availability of healthy food items in rural areas or locations with limited access to large stores should be investigated. Similarly, the availability and pricing of healthy food options in smaller stores can provide different findings from those detected in our investigation. This investigation targeted only basic raw foods or ingredients available in supermarkets. Further investigation could assess the cost of consuming prepared healthy food provided by restaurants. Similarly, the availability and pricing of healthy food items provided by restaurants in Saudi Arabia might have an impact on the consumers’ choices.
Table 4.
A summary of similarities and differences of the current investigation of cost of healthy food in Saudi Arabiato similar previous studies.
In conclusion, this study suggests that healthy food is not more expensive than less healthy items in Saudi Arabia. Prices of healthy options within dairy and vegetables were significantly lower than non-healthy options. This suggests that access to healthy food in the Saudi market in urban areas is not largely affected by cost, and other factors might influence the consumers’ choice of selecting healthy foods.
Footnotes
References
- 1.Organization WH. Global Strategy on Diet, Physical Activity and Health. 2003. [Cited 2015 November 3]. Available from: http://www.who.int/dietphysicalactivity/fruit/en/
- 2.Washi SA, Ageib MB. Poor diet quality and food habits are related to impaired nutritional status in 13- to 18-year-old adolescents in Jeddah. Nutr Res. 2010;30:527–534. doi: 10.1016/j.nutres.2010.07.002. [DOI] [PubMed] [Google Scholar]
- 3.Al-Rukban MO. Obesity among Saudi male adolescents in Riyadh, Saudi Arabia. Saudi Med J. 2003;24:27–33. [PubMed] [Google Scholar]
- 4.Al-Othaimeen AI, Al-Nozha M, Osman AK. Obesity: an emerging problem in Saudi Arabia. Analysis of data from the National Nutrition Survey. East Mediterr Health J. 2007;13:441–448. [PubMed] [Google Scholar]
- 5.Alam AA. Obesity among female school children in North West Riyadh in relation to affluent lifestyle. Saudi Med J. 2008;29:1139–1144. [PubMed] [Google Scholar]
- 6.Al-Dossary SS, Sarkis PE, Hassan A, Ezz El Regal M, Fouda AE. Obesity in Saudi children: a dangerous reality. East Mediterr Health J. 2010;16:1003–1008. [PubMed] [Google Scholar]
- 7.Mahfouz AA, Shatoor AS, Khan MY, Daffalla AA, Mostafa OA, Hassanein MA. Nutrition, Physical Activity, and Gender Risks for Adolescent Obesity in Southwestern Saudi Arabia. Saudi J Gastroenterol. 2011;17:318–322. doi: 10.4103/1319-3767.84486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Saudi Ministry of Health. Survey of Health Information. 2013. Available from: http://www.moh.gov.sa/en/ministry/statistics/pages/healthinformatics.aspx .
- 9.Al-Nozha M, Al-Khadra A, Arafah MR, Al-Maatouq MA, Khalil MZ, Khan NB, et al. Metabolic syndrome in Saudi Arabia. Saudi Med J. 2005;26:1918–1925. [PubMed] [Google Scholar]
- 10.Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int J Behav Nutr Phys Act. 2011;8:140. doi: 10.1186/1479-5868-8-140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bin Horaib G, Al-Khashan HI, Mishriky AM, Selim MA, Alnowaiser N, Binsaeed AA, et al. Prevalence of obesity among military personnel in Saudi Arabia and associated risk factors. Saudi Med J. 2013;34:401–417. [PubMed] [Google Scholar]
- 12.Orozco LJ, Buchleitner AM, Gimenez-Perez G, Roque IFM, Richter B, Mauricio D. Exercise or exercise and diet for preventing type 2 diabetes mellitus. Cochrane Database Syst Rev. 2008:CD003054. doi: 10.1002/14651858.CD003054.pub3. [DOI] [PubMed] [Google Scholar]
- 13.Uusitupa MI, Stancakova A, Peltonen M, Eriksson JG, Lindstrom J, Aunola S, et al. Impact of positive family history and genetic risk variants on the incidence of diabetes: the Finnish Diabetes Prevention Study. Diabetes care. 2011;34:418–423. doi: 10.2337/dc10-1013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dkheel MH. Dietary Guidelines for Saudis. 2012. Available from: http://www.moh.gov.sa/en/HealthAwareness/Pages/SaudihealthFoodGuide.aspx .
- 15.Rao M, Afshin A, Singh G, Mozaffarian D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ open. 2013;3:e004277. doi: 10.1136/bmjopen-2013-004277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.United states department of agriculture. National Nutrient Database for Standard Reference Release 28. 2015. Available from: http://ndb.nal.usda.gov/ndb/search .
- 17.Canada H. Canadian Nutrient File. 2012. Available from: http://webprod3.hc-sc.gc.ca/cnf-fce/index-eng.jsp .
- 18.Katz DL, Doughty K, Njike V, Treu JA, Reynolds J, Walker J, et al. A cost comparison of more and less nutritious food choices in US supermarkets. Public health nutrition. 2011;14:1693–1699. doi: 10.1017/S1368980011000048. [DOI] [PubMed] [Google Scholar]
- 19.Jetter KM, Cassady DL. The availability and cost of healthier food alternatives. American journal of preventive medicine. 2006;30:38–44. doi: 10.1016/j.amepre.2005.08.039. [DOI] [PubMed] [Google Scholar]
- 20.Liese AD, Weis KE, Pluto D, Smith E, Lawson A. Food store types, availability, and cost of foods in a rural environment. J Am Diet Assoc. 2007;107:1916–1923. doi: 10.1016/j.jada.2007.08.012. [DOI] [PubMed] [Google Scholar]
- 21.Krukowski RA, West DS, Harvey-Berino J, Elaine Prewitt T. Neighborhood impact on healthy food availability and pricing in food stores. J Community Health. 2010;35:315–320. doi: 10.1007/s10900-010-9224-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ricciuto L, Ip H, Tarasuk V. The relationship between price, amounts of saturated and trans fats, and nutrient content claims on margarines and oils. Can J Diet Pract Res. 2005;66:252–255. doi: 10.3148/66.4.2005.252. [DOI] [PubMed] [Google Scholar]
- 23.Wang J, Williams M, Rush E, Crook N, Forouhi NG, Simmons D. Mapping the availability and accessibility of healthy food in rural and urban New Zealand--Te Wai o Rona: Diabetes Prevention Strategy. Public Health Nutr. 2010;13:1049–1055. doi: 10.1017/S1368980009991595. [DOI] [PubMed] [Google Scholar]