

Abstract
The open anatomic repair of the anterior talofibular and calcaneofibular ligaments (modified Brostrom procedure) is widely accepted as the standard surgical stabilization procedure for lateral ankle instability that does not respond to conservative measures. Arthroscopic Brostrom procedures with a suture anchor have been reported to achieve both anatomic repair of the lateral ankle ligaments and management of the associated intra-articular lesions. However, the complication rates are higher than open Brostom procedures. Many of these complications are associated with the use of a suture anchor. We report a modified arthroscopic Brostrom procedure in which the anterolateral ankle capsule is anchored to the lateral malleolus through small bone tunnels instead of suture anchors.
Chronic lateral ankle instability can sometimes occur as a result of ankle sprain. In general, the first line of treatment is nonoperative therapy including functional rehabilitation. Surgery is indicated if nonoperative measures cannot control the symptoms. The surgical options can be divided into 2 groups: anatomic repair and nonanatomic reconstruction of the lateral ligament complex. The open modified Brostrom anatomic repair technique is the reference standard stabilization procedure for lateral ankle instability.1 However, there is high incidence of intra-articular pathologies associated with chronic lateral ankle instability1, 2, 3, 4, 5 that can result in poor clinical outcome if they are not addressed during the open repair.6, 7, 8 Preoperative magnetic resonance imaging is useful for detection of the associated intra-articular pathologies, but some of the lesions can still be missed.6, 9, 10 Some authors advocated ankle arthroscopy to assess and treat the intra-articular pathologies followed by the open Brostrom procedure.2, 3, 4, 6, 8, 11 Techniques of arthroscopic stabilization procedure are developed to address both the lateral ankle instability and the associated intra-articular lesions through the same arthroscopic approach. Arthroscopic or arthroscopically assisted lateral ankle ligament reconstruction, such as plication, staples, suture anchor, and thermal shrinkage, has also been reported.1, 12, 13, 14, 15 The arthroscopic Brostrom procedure with a suture anchor has been described for anatomic repair of chronic lateral ankle instability and management of intra-articular lesions. Treatment outcomes associated with this procedure have been positive.1, 13, 14, 15 However, the complication rates seemed to be higher than the open Brostrom procedure and many of them are related to the use of a suture anchor.16 We report a modified arthroscopic Brostrom procedure17 in which the anterolateral ankle capsule is anchored to the lateral malleolus through small bone tunnels instead of suture anchors. Because of the use of this alternative, complications previously reported as a result of suture anchors can now be prevented.
Technique
Step 1: Preoperative Planning
Careful history taking and clinical examination is usually sufficient to establish the diagnosis of chronic lateral ankle instability. Preoperative magnetic resonance imaging can be useful for detection of associated intra-articular lesions, for example, osteochondral lesion.
Step 2: Patient Positioning and Setup
The patient is put in supine position. The ankle varus stress test under fluoroscopy is performed before arthroscopy. A thigh tourniquet is applied to provide a bloodless surgical field. No ankle distractor is used. The knee is flexed and supported by a triangular frame.
Step 3: Portal Placement of Ankle Arthroscopy
Ankle arthroscopy is performed using the anteromedial and anterolateral portals. The anteromedial portal locates medial to the tibialis anterior tendon and the anterolateral portal locates lateral to the peroneus tertius tendon. Five-millimeter (mm) incisions are made at the portal site. The subcutaneous tissue is spread with a hemostat and the capsule is pierced by the tip of the hemostat. A 2.7-mm 30° arthroscope (Henke Sass Wolf GmbH, Germany) is used. The ankle joint is examined for any concomitant pathology, for example, osteochondral lesion and treated accordingly. During the modified arthroscopic Brostrom procedure, the anteromedial portal is the viewing portal and the anterolateral portal is the working portal. The arthroscopic varus stress test is performed (Fig 1).
Fig 1.
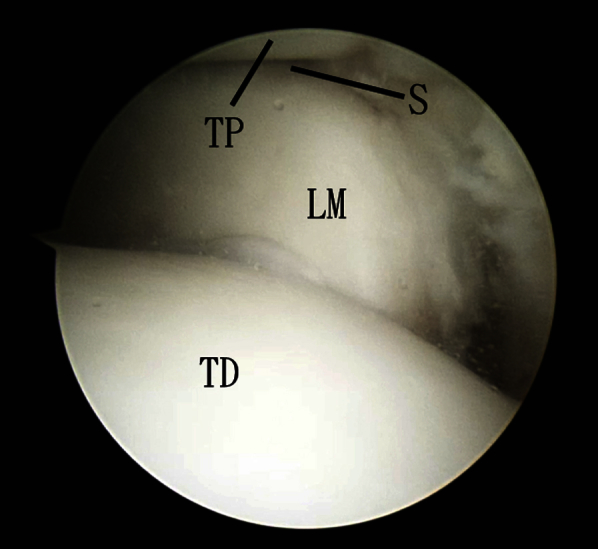
Modified arthroscopic Brostrom procedure of the left ankle. The anteromedial portal is the viewing portal. The arthroscopic view shows that the lateral joint space is opened up on the varus stress test. (LM, lateral malleolus; S, distal tibiofibular syndesmosis; TD, talar dome; TP, tibial plafond.)
Step 4: Debridement of Anterior Surface of the Lateral Malleolus
Any hypertrophic synovium is debrided and the scar tissue covering the surface of the lateral malleolus is resected by an arthroscopic shaver (Dyonics Powermini, Smith and Nephew, Andover, MA) and an arthroscopic curette (Acufex, Smith and Nephew). The debridement should be completed from the level of syndesmosis to the lateral malleolar tip (Fig 2). The fibular insertion of the distal anterior tibiofibular ligament should be preserved. The fibrous tissue of the anterolateral capsule is left untouched for subsequent anchorage of sutures. The anterior cortex of the lateral malleolus is ablated to prepare for subsequent capsular and ligamentous adhesion.
Fig 2.

Modified arthroscopic Brostrom procedure of the left ankle. The arthroscopic view shows that the fibular insertion of the anterolateral capsule (ALC) is debrided and detached from the lateral malleolus. (a, the subcutaneous tissue seen through the gap between the lateral malleolus and ALC; LM, lateral malleolus; TD, talar dome.)
Step 5: Suturing of the Anterolateral Capsule Including the Anterior Talofibular Ligament
Two No. 0 FiberWire suture loops are passed through the anterolateral capsule by means of a Viper suture passer (CPR, Arthrex, Naples, FL). The Viper suture passer preloaded with No. 0 FiberWire suture is inserted through the anterolateral portal to the debrided proximal end of the anterolateral capsule. The head of the passer is slipped into the superficial surface of the capsule and the capsule together with the anterior talofibular ligament is bitten (Fig 3). The suture loop is passed through the stump and retrieved to the anterolateral portal. The limbs of the suture are passed through the suture loop and the suture is tightened to create a stable bite of the capsule. The step is repeated to make another suture loop 1 cm plantar to the first loop.
Fig 3.

Modified arthroscopic Brostrom procedure of the left ankle. (A) The anteromedial portal is the viewing portal. A viper suture passer is inserted through the anterolateral portal. (B) The anterolateral capsule (ALC) is grasped by the passer (V) to pass a suture loop through the capsule. (LM, lateral malleolus.)
Step 6: Making 2 Bone Tunnels
Two 2.5-mm bone tunnels are made at the lateral malleolus and are approximately 1 cm apart at the anterior surface of the malleolus and convergent toward the posterior surface. The drilling is guided by arthroscopy and fluoroscopy. After completing the drilling, the guide sleeve is held in position and 2.4-mm femoral eye-loop guidewires of the anterior cruciate ligament reconstruction instrument set (Acufex, Smith and Nephew) are inserted into the bone tunnels (Fig 4). The guidewires pierce the skin just lateral to the Achilles tendon. A small incision is made at the posterior border of the lateral malleolus at the exit points of the guidewires.
Fig 4.

Modified arthroscopic Brostrom procedure of the left ankle. (A) The anteromedial portal is the viewing portal. The lateral malleolus is drilled by a 2.5-mm drill bit through the anterolateral portal. (B) The arthroscopic view shows that two 2.4-mm guidewires are passed through the bone tunnels of the lateral malleolus. (ALC, anterolateral capsule; LM, lateral malleolus.)
Step 7: Passing the Sutures Through the Bone Tunnels
The limbs of dorsal and plantar suture loops are passed through the eye-loops of the upper and lower guidewires respectively. When the wires are removed from the posterior heel, the limbs of the dorsal and plantar suture loops are brought through the superior and inferior bone tunnels, respectively (Fig 5). They are retrieved to the posterior incision.
Fig 5.

Modified arthroscopic Brostrom procedure of the left ankle. (A) The limbs of dorsal and plantar suture loops are passed through the eye-loops of the upper and lower guidewires, respectively. (B) When the wires are removed from the posterior heel, the limbs of the dorsal and plantar suture loops are brought through the superior and inferior bone tunnels, respectively. (C) The sutures are passed through the skin of the posterior heel just lateral to the Achilles tendon. (ALC, anterolateral capsule; LM, lateral malleolus; S, sutures; TD, talar dome.)
Step 8: Repair of the Anterolateral Capsule Including the Anterior Talofibular Ligament
The foot is held in an everted position, whereas the ankle is held in a neutral to slightly dorsiflexed position. Each limb of the dorsal sutures is paired up with one of the plantar sutures. Each pair of sutures is tightened and tied. The repair of the anterolateral capsule including the anterior talofibular ligament is then completed and can be confirmed arthroscopically (Fig 6, Video 1).
Fig 6.

Modified arthroscopic Brostrom procedure of the left ankle. (A) The sutures are retrieved to the incision just posterior to the lateral malleolus. Each limb of the dorsal sutures is paired up with one of the plantar sutures. Each pair of sutures is tightened and tied with the foot in an everted and ankle in a neutral to slightly dorsiflexed position. The repair of the anterolateral capsule including the anterior talofibular ligament is then completed. (B) The repair is confirmed arthroscopically. (ALC, anterolateral capsule; LM, lateral malleolus; TD, talar dome.)
Discussion
The arthroscopic Brostrom procedure is a viable alternative of the open procedure (Table 1). The cadaveric study showed that there is no statistical difference in strength or stiffness of a traditional open repair as compared with an arthroscopic anatomic repair of the lateral ligaments of the ankle.18 It is indicated in symptomatic lateral ankle instability that does not respond to conservative therapy. The arthroscopic approach allows the surgeon to address both the lateral ligament instability and associated intra-articular pathologies without extensive dissection. Moreover, it has the advantages of minimally invasive surgery, for example, small incisions, less soft tissue trauma, and better cosmetic result. Most of the reported arthroscopic techniques use a suture anchor to reattach the anterior talofibular ligament to the lateral malleolus. Potential complications of using a suture anchor in the lateral malleolus include dislodgement of the implant, iatrogenic fracture of the lateral malleolus, and malpositioning of the implant causing impingement of the syndesmosis or the peroneal tendons.19 The transosseous tunnel fixation technique instead of a suture anchor technique is used in this technique. This has been a popular choice for open lateral ligament reconstruction for ankle instability. The strength of pullout is at least comparable with a suture anchor.20 The risk of iatrogenic fracture of the lateral malleolus is reduced as the size of bone tunnels needed for the transosseous tunnel fixation technique is smaller than that of the suture anchor fixation technique. Because of the “all-inside” technique of suturing of the anterolateral capsule, the risk of injury to the peroneus tertius tendon, extensor tendons, and intermediate dorsal cutaneous branch of the superficial peroneal nerve is reduced.6, 21 However, the risk of sural nerve injury is higher because of the need of passing the guidewire and sutures to the posterolateral heel. This risk can be reduced by piercing the skin just lateral to the Achilles tendon. Moreover, the knots behind the lateral malleolus may irritate the peroneal tendons (Table 2).
Table 1.
Pearls and Pitfalls of the Modified Arthroscopic Brostrom Procedure With Bone Tunnels
| Pearls | Pitfalls |
|---|---|
|
|
Table 2.
Advantages and Risks of the Modified Arthroscopic Brostrom Procedure With Bone Tunnels
| Advantages | Risks |
|---|---|
|
|
This technique only addresses the anterior talofibular ligament and not the calcaneofibular ligament. Lee et al.22 have reported the long-term results of a modified Brostrom procedure without calcaneofibular ligament repair and concluded that the results were good to excellent, considering the subjective, functional, and radiographic findings. However, this technique may not adequately stabilize the lateral ankle if concomitant subtalar instability exists. Similar, it is not suitable if the quality of the anterolateral capsule is suboptimal for repair. Ligament reconstruction is indicated in this situation.
Finally, any varus inclination of the ankle and hindfoot should be corrected together with the repair to reduce the chance of recurred instability and severe chondral damage of the ankle in patients with a prolonged history of lateral ankle instability.23
Footnotes
The author reports that he has no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Modified arthroscopic Brostrom procedure of the left ankle. The anteromedial portal is the viewing portal and the anterolateral portal is the working portal. First, lateral ankle instability is confirmed by the varus stress test. Second, the anterior surface of the lateral malleolus is debrided. Third, the anterolateral capsule including the anterior talofibular ligament is sutured by a CPR Viper suture passer. Fourth, 2 bone tunnels are made at the lateral malleolus. Fifth, sutures limbs are passed through the bone tunnels by means of guidewires with an eye-loop. Sixth, the sutures are retrieved to the incision just posterior to the lateral malleolus. Each limb of the dorsal sutures is paired up with one of the plantar sutures. Each pair of sutures is tightened and tied with the foot in an everted and ankle in a neutral to slightly dorsiflexed position.
References
- 1.Cottom J.M., Rigby R.B. The “all inside” arthroscopic Brostrom procedure: A prospective study of 40 consecutive patients. J Foot Ankle Surg. 2013;52:568–574. doi: 10.1053/j.jfas.2013.02.022. [DOI] [PubMed] [Google Scholar]
- 2.Cannon L.B., Hackney R.G. Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg. 2000;39:383–386. doi: 10.1016/s1067-2516(00)80074-5. [DOI] [PubMed] [Google Scholar]
- 3.Choi W.J., Lee J.W., Han S.H., Kim B.S., Lee S.K. Chronic lateral ankle instability: The effect of intra-articular lesions on clinical outcome. Am J Sports Med. 2008;36:2167–2172. doi: 10.1177/0363546508319050. [DOI] [PubMed] [Google Scholar]
- 4.Ferkel R.D., Chams R.N. Chronic lateral instability: Arthroscopic findings and long-term results. Foot Ankle Int. 2007;28:24–31. doi: 10.3113/FAI.2007.0005. [DOI] [PubMed] [Google Scholar]
- 5.Lee J., Hamilton G., Ford L. Associated intra-articular ankle pathologies in patients with chronic lateral ankle instability: Arthroscopic findings at the time of lateral ankle reconstruction. Foot Ankle Spec. 2011;4:284–289. doi: 10.1177/1938640011416355. [DOI] [PubMed] [Google Scholar]
- 6.Cha S.D., Kim H.S., Chung S.T. Intra-articular lesions in chronic lateral ankle instability: Comparison of arthroscopy with magnetic resonance imaging findings. Clin Orthop Surg. 2012;4:293–299. doi: 10.4055/cios.2012.4.4.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Guillo S., Bauer T., Lee J.W. Consensus in chronic ankle instability: Aetiology, assessment, surgical indications and place for arthroscopy. Orthop Traumatol Surg Res. 2013;99S:S411–S419. doi: 10.1016/j.otsr.2013.10.009. [DOI] [PubMed] [Google Scholar]
- 8.Hua Y., Chen S., Li Y., Chen J., Li H. Combination of modified Broström procedure with ankle arthroscopy for chronic ankle instability accompanied by intra-articular symptoms. Arthroscopy. 2010;26:524–528. doi: 10.1016/j.arthro.2010.02.002. [DOI] [PubMed] [Google Scholar]
- 9.Hunt K.J., Githens M., Riley G.M., Kim M., Gold G.E. Foot and ankle injuries in sport imaging correlation with arthroscopic and surgical findings. Clin Sports Med. 2013;32:525–557. doi: 10.1016/j.csm.2013.03.007. [DOI] [PubMed] [Google Scholar]
- 10.Joshy S., Abdulkadir U., Chaganti S., Sullivan B., Hariharan K. Accuracy of MRI scan in the diagnosis of ligamentous and chondral pathology in the ankle. Foot Ankle Surg. 2010;16:78–80. doi: 10.1016/j.fas.2009.05.012. [DOI] [PubMed] [Google Scholar]
- 11.Maffulli N., Del Buono A., Maffulli G.D. Isolated anterior talofibular ligament Brostrom repair for chronic lateral ankle instability: 9-year follow-up. Am J Sports Med. 2013;41:858–864. doi: 10.1177/0363546512474967. [DOI] [PubMed] [Google Scholar]
- 12.Acevedo J., Mangone P. Arthroscopic lateral ankle ligament reconstruction. Tech Foot Ankle Surg. 2011;10:111–116. [Google Scholar]
- 13.Corte-Real N.M., Moreira R.M. Arthroscopic repair of chronic lateral ankle instability. Foot Ankle Int. 2009;30:213–217. doi: 10.3113/FAI.2009.0213. [DOI] [PubMed] [Google Scholar]
- 14.Nery C., Raduan F., Del Buono A., Asaumi I.D., Cohen M., Maffulli N. Arthroscopic-assisted Brostrom-Gould for chronic ankle instability: A long-term follow-up. Am J Sports Med. 2011;39:2381–2388. doi: 10.1177/0363546511416069. [DOI] [PubMed] [Google Scholar]
- 15.Kim E.S., Lee K.T., Park J.S., Lee Y.K. Arthroscopic anterior talofibular ligament repair for chronic ankle instability with a suture anchor technique. Orthopedics. 2011;34 doi: 10.3928/01477447-20110228-03. [DOI] [PubMed] [Google Scholar]
- 16.Wang J., Hua Y., Chen S., Li H., Zhang J., Li Y. Arthroscopic repair of lateral ankle ligament complex by suture anchor. Arthroscopy. 2014;30:766–773. doi: 10.1016/j.arthro.2014.02.023. [DOI] [PubMed] [Google Scholar]
- 17.Lui T.H. Modified arthroscopic Brostrom procedure. Foot Ankle Surg. 2015;21:216–219. doi: 10.1016/j.fas.2015.01.008. [DOI] [PubMed] [Google Scholar]
- 18.Giza E., Shin E.C., Wong S.E. Arthroscopic suture anchor repair of the lateral ligament ankle complex: A cadaveric study. Am J Sports Med. 2013;41:2567–2572. doi: 10.1177/0363546513500639. [DOI] [PubMed] [Google Scholar]
- 19.Lui T.H. Eckert and Davis grade 3 superior peroneal retinaculum injury: Treated by endoscopic peroneal retinaculum reconstruction and complicated by malposition of the suture anchors. J Orthop Case Rep. 2015;5:73–76. doi: 10.13107/jocr.2250-0685.352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Li H.Y., Hua Y.H., Wu Z.Y., Chen B., Chen S.Y. Strength of suture anchor versus transosseous tunnel in anatomic reconstruction of the ankle lateral ligaments: A biomechanical study. Arthroscopy. 2013;29:1817–1825. doi: 10.1016/j.arthro.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 21.Drakos M., Behrens S.B., Mulcahey M.K., Paller D., Hoffman E., DiGiovanni C.W. Proximity of arthroscopic ankle stabilization procedures to surrounding structures: An anatomic study. Arthroscopy. 2013;29:1089–1094. doi: 10.1016/j.arthro.2013.02.011. [DOI] [PubMed] [Google Scholar]
- 22.Lee K., Park Y., Kim J., Kim J., Kim K., Kang S. Long-term results after modified Brostrőm procedure without calcaneofibular ligament reconstruction. Foot Ankle Int. 2011;32:153–157. doi: 10.3113/FAI.2011.0153. [DOI] [PubMed] [Google Scholar]
- 23.Sugimoto K., Takakura Y., Okahashi K., Samoto N., Kawate K., Iwai M. Chondral injuries of the ankle with recurrent lateral instability: An arthroscopic study. J Bone Joint Surg Am. 2009;91:99–106. doi: 10.2106/JBJS.G.00087. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Modified arthroscopic Brostrom procedure of the left ankle. The anteromedial portal is the viewing portal and the anterolateral portal is the working portal. First, lateral ankle instability is confirmed by the varus stress test. Second, the anterior surface of the lateral malleolus is debrided. Third, the anterolateral capsule including the anterior talofibular ligament is sutured by a CPR Viper suture passer. Fourth, 2 bone tunnels are made at the lateral malleolus. Fifth, sutures limbs are passed through the bone tunnels by means of guidewires with an eye-loop. Sixth, the sutures are retrieved to the incision just posterior to the lateral malleolus. Each limb of the dorsal sutures is paired up with one of the plantar sutures. Each pair of sutures is tightened and tied with the foot in an everted and ankle in a neutral to slightly dorsiflexed position.