

Abstract
Patients with rotator cuff tears may present with or subsequently develop concomitant shoulder stiffness. The treatment of rotator cuff tears in the face of passive glenohumeral motion loss is controversial. Preoperative shoulder stiffness has been considered by some a contraindication to rotator cuff repair. Some surgeons recommend staging surgical procedures and delaying rotator cuff repair until shoulder stiffness has resolved. However, this can lead to prolonged recovery times and patient dissatisfaction. We describe a surgical technique that allows for the single-stage arthroscopic management of rotator cuff tears with associated adhesive capsulitis. Arthroscopic capsular release and shoulder manipulation are performed in the same operative setting as arthroscopic rotator cuff repair. We have found that this combined, single-stage arthroscopic approach can effectively treat patients with rotator cuff tears and concomitant shoulder stiffness.
Arthroscopic rotator cuff repair has proven reliable and reproducible. Some patients with rotator cuff tears present with or subsequently develop significant preoperative shoulder stiffness. Prior research has shown that stiffness is common after rotator cuff repair, that preoperative stiffness predisposes one to this complication, and that postoperative stiffness leads to suboptimal surgical outcomes.1 Therefore, some authors consider preoperative stiffness a contraindication to rotator cuff repair, and recommend staging surgical procedures and delaying rotator cuff repair until shoulder stiffness has resolved.
Although resolution of adhesive capsulitis before rotator cuff repair is desirable, some patients remain stiff despite extensive nonoperative intervention. Refractory shoulder stiffness in the absence of rotator cuff pathology has been successfully managed with arthroscopic capsular release with or without manipulation. Although arthroscopy is a proven method of addressing adhesive capsulitis and rotator cuff tears separately, few articles have discussed the technique of single-stage arthroscopic capsular release and rotator cuff repair for patients with rotator cuff tears and recalcitrant shoulder stiffness.
Surgical Technique
Indications
It should be noted that conservative management of shoulder pain and stiffness is initially attempted. Nonoperative management usually consists of nonsteroidal anti-inflammatory drugs and a comprehensive physical therapy program focusing on shoulder range of motion. In addition, patients are typically offered subacromial and glenohumeral corticosteroid injections.
The most patients will show improvement in passive shoulder range of motion with these nonoperative techniques and can undergo isolated arthroscopic rotator cuff repair (Table 1). However, a subset of patients will show recalcitrant shoulder stiffness, and it is for these patients whom single-stage arthroscopic capsular release and rotator cuff repair is recommended.
Table 1.
Indications and Contraindications
| Indications | Contraindications |
|---|---|
| Persistent pain, stiffness, and weakness despite attempted nonoperative management. Surgical delay does not improve patient outcomes, and failure to improve with conservative treatment is an indication for surgical intervention. | Inadequate trial of conservative management for shoulder stiffness. Most patients will improve and can undergo isolated rotator cuff repair. |
Operative Technique
Before patient positioning, the operative shoulder is examined under anesthesia. The patient is placed in the supine position and the scapula is stabilized. Passive forward elevation and passive external rotation with the arm at the side are evaluated. Arthroscopic capsular release is indicated for patients with passive forward elevation less than or equal to 120° and/or passive external rotation less than or equal to 30°.
Closed Manipulation
Closed manipulation is then performed at the discretion of the treating surgeon (some prefer to perform arthroscopic capsular release before shoulder manipulation). The patient's scapula is stabilized with one hand, whereas the other hand controls the operative extremity. The operative extremity is gently manipulated into full abduction and full forward elevation, releasing the inferior capsule. The operative extremity is then placed at the patient's side, and gentle external rotation is used to release the anterior capsule and rotator interval. The arm is placed in 90° of abduction, and gentle external rotation force is applied until passive range of motion is restored. With the patient's arm still in an abducted position, gentle internal rotational force is applied to release the posterior capsule. The patient's arm is then adducted across the body to complete posterior capsular release.
Diagnostic Arthroscopy
Standard diagnostic shoulder arthroscopy is then conducted via posterior and anterior portals. Figure 1 shows the combined rotator cuff tear and capsulitis pathology typically encountered by the surgeon. If closed manipulation is performed before arthroscopy, the capsular rent created by closed manipulation is identified arthroscopically. An angled arthroscopic upbiter (Acufex 1/4 curve upbiter, Smith & Nephew, Andover, MA) and/or arthroscopic hooked cautery instrument (RF Hook 30° probe, Smith & Nephew Dyonics, Andover, MA) are then used to carry out complete capsular release of the anterior, inferior, and posterior capsule under direct visualization. Capsular release surgical technique is shown in Video 1.
Fig 1.
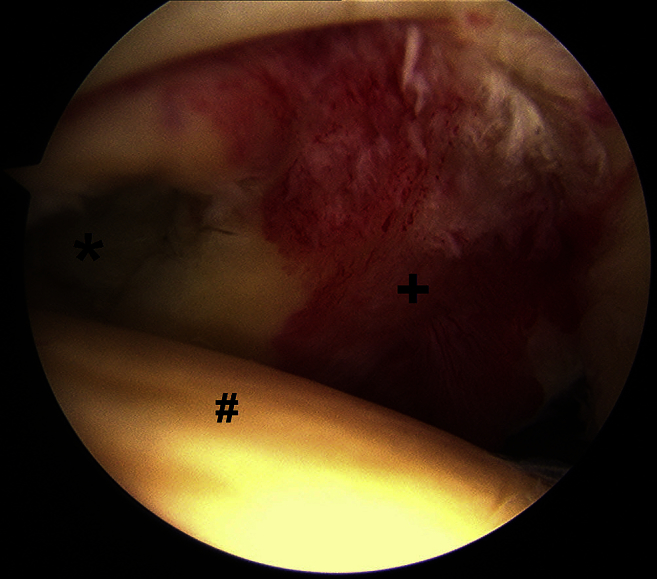
Right shoulder as viewed from the anterior portal in beach chair position, showing full-thickness rotator cuff tear with associated adhesive capsulitis. (Asterisk, rotator cuff tear; pound sign, humeral head; plus sign, inflamed and thickened capsule.)
Anterior Capsular Release
For anterior capsular release, the 30° arthroscope (Smith & Nephew Dyonics) is placed in the posterior portal. An arthroscopic biter or hooked cautery device is then placed within the anterior cannula (Clear-Trac 5.5 mm × 72 mm threaded plastic cannula, Smith & Nephew), and the cannula is withdrawn until it is just superficial to the capsule. This allows the arthroscopic instruments access to the capsule in the area of the portal, where capsular release can be initiated if a capsular rent was not already created by manipulation.
The biter and/or cautery are then used to incise the thickened capsule while staying deep to the rotator cuff musculature, creating a vertically oriented linear capsular defect. The biter can then be used to bluntly separate the medial and lateral capsular limbs so as to create space between them and to encourage healing in an elongated position. In addition, an arthroscopic shaver (4.5-mm Incisor, Smith & Nephew) can be used to shave away small amounts of capsule at the margins of the release, thus widening the capsular defect so that the capsular limbs are no longer opposed.
Inferior Capsular Release
Inferior capsular release is performed with the scope in the posterior portal and electrocautery instrument in the anterior cannula. A surgical assistant applies slight traction and lateral translational force to the humerus so that the inferior labrum and capsule can be visualized. Inferior capsular release is then performed with cautery under direct visualization, with care to stay adjacent to the glenoid labrum and to avoid plunging through the capsule to minimize risk of iatrogenic axillary nerve injury. Cautery is preferred instead of an arthroscopic biter for inferior capsular release, as short cautery pulses can be used to incise the capsule in controlled fashion and deltoid contraction warns the surgeon of proximity to the axillary nerve.
Posterior Capsular Release
Typically, the posterior capsule is less severely involved with adhesive capsulitis. However, posterior capsular release is performed as necessary with the arthroscope in the anterior portal, and the arthroscopic biter or cautery in the posterior portal. Similar to the technique used for anterior capsular release, the posterior cannula is slightly withdrawn just superficial to the capsule to give instruments access to the capsule in the area of the portal. A capsular defect is created and widened in the same fashion used for anterior capsular release. Figure 2 shows posterior capsular release obtained after manipulation and use of an arthroscopic biter.
Fig 2.
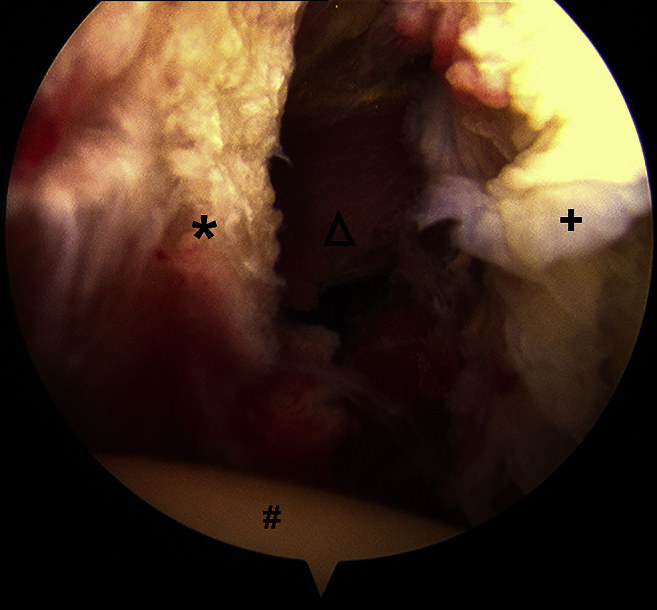
Right shoulder in beach chair position viewed from the anterior portal, showing completed posterior capsular release. (Asterisk, lateral capsular limb; triangle, infraspinatus muscle seen through completed capsulotomy; plus sign, medial capsular limb adjacent to glenoid; pound sign, humeral head.)
Complete release of the capsule is confirmed when the arthroscopist can visualize rotator cuff muscle fibers through the capsular defects from approximately 2 o'clock to 10 o'clock. Note that superior capsular release is not performed, as this is not pathologically thickened and is confluent with the overlying rotator cuff tendons. The shoulder is then placed through full range of motion to confirm adequate capsular release. Table 2 highlights salient surgical technique steps for shoulder manipulation and capsular release.
Table 2.
Key Intraoperative Steps
|
|
|
|
|
|
|
Rotator Cuff Repair
Attention is then turned to arthroscopic rotator cuff repair, which is performed in standard fashion. The arthroscopic rotator cuff technique is well described elsewhere, and detailed discussion is unnecessary. The arthroscope is redirected into the subacromial space via the posterior portal, and a metal inflow cannula (5.5 mm, Smith & Nephew) is placed in the subacromial space via the anterior portal. Reactive tissue and/or scarring is frequently encountered, and thorough subacromial bursectomy is performed with the shaver in the lateral subacromial portal. The authors routinely perform acromioplasty in cutting block fashion, with the camera in the lateral subacromial portal and a burr (4.5-mm Helicut, Smith & Nephew) in the posterior portal.
The rotator cuff tear is identified and soft tissue releases are carried out as necessary for tissue mobilization. The coracohumeral ligament and any contractures of the rotator interval are released. The greater tuberosity footprint is then debrided and the rotator cuff is reapproximated to its anatomic footprint utilizing suture anchors and standard locking arthroscopic knots. Figures 3 and 4 depict the full-thickness rotator cuff tear before and after repair in this patient with concomitant stiffness.
Fig 3.
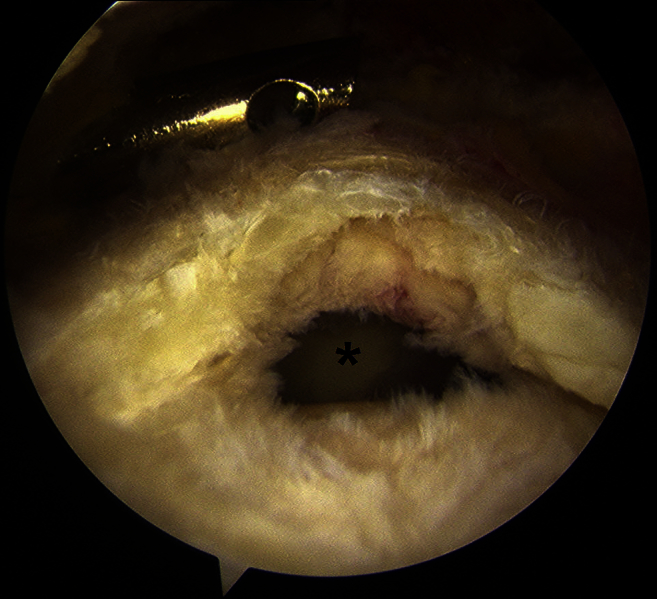
Full-thickness rotator cuff tear in the same patient, as viewed from the subacromial space. (Asterisk, rotator cuff tear.)
Fig 4.
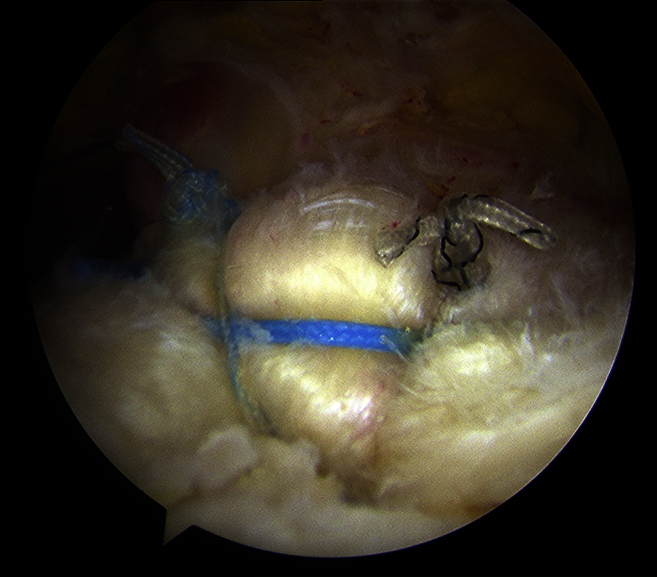
Repaired rotator cuff tear, as viewed from the subacromial space.
Postoperative Care
Patients are placed into a pillow abduction orthosis (Donjoy, Vista, CA) that is worn for 2 to 3 weeks when not doing therapy exercises. Early range of motion is emphasized, and organized physical therapy focusing on passive shoulder range of motion is started on postoperative day 1. Regional nerve blocks are often used to assist with postoperative pain management and facilitate early mobilization with physical therapy. Active-assisted and active shoulder range of motion exercises are typically initiated 6 weeks after surgery unless the patient has a large rotator cuff tear, in which case active exercises are delayed until 8 weeks postoperatively. Rotator cuff strengthening exercises are typically added 12 weeks after surgery.
Discussion
Patients with rotator cuff tears and concomitant shoulder stiffness may not do well with isolated arthroscopic rotator cuff repair.1 Although earlier studies have reported good results after arthroscopic capsular release for isolated shoulder stiffness,2, 3 only recently have authors reported on single-stage arthroscopic management of rotator cuff tears with associated adhesive capsulitis.
Oh et al.4 evaluated 30 patients who underwent capsular release and manipulation for moderate shoulder stiffness at the time of rotator cuff repair. They concluded that adding manipulation and capsular release to rotator cuff repair provides acceptable outcomes and minimizes surgical delay.
Cho and Rhee5 reported similar findings in patients with stiff shoulders who underwent rotator cuff repair with concomitant manipulation. However, they noted that shoulder range of motion took longer to improve and did not completely return to normal. Cho et al.6 found that patients with stiff shoulders in the setting of rotator cuff tears, who underwent combined arthroscopic capsular release and manipulation, had similar outcomes as a comparison group without shoulder stiffness. However, as noted by other authors, it took approximately 6 months for range of motion to normalize in the stiff group.
Ho et al.7 recently reported on 41 patients who underwent 1-stage arthroscopic capsular release and rotator cuff repair. Functional outcomes were similar to a comparison group of patients without shoulder stiffness who underwent isolated arthroscopic rotator cuff repair.
Kim et al.8 examined the effect of surgical timing on patients with rotator cuff tears and shoulder stiffness. They found that delaying surgery to complete 6 months of preoperative physical therapy did not lead to improved outcomes over early surgical intervention.
Chuang et al.9 evaluated the benefit of capsular release for patients with rotator cuff tears and concomitant stiff shoulders. They found that capsular release in addition to manipulation provided earlier and more complete restoration of shoulder range of motion than manipulation alone. Capsular release has also been shown to be particularly beneficial in diabetic patients.10 Although the increasing literature supports single-stage arthroscopic management of rotator cuff tears with concomitant shoulder stiffness, this technique is not without risk (Table 3). Humeral fractures, shoulder dislocations, and iatrogenic rotator cuff and labral tears have been reported after shoulder manipulation. Furthermore, the axillary nerve is at risk during inferior capsular release. The surgeon must take care to use gentle, controlled force during manipulation, and to stay adjacent to the glenoid during inferior capsular release.
Table 3.
Pearls and Pitfalls
| Pearls | Potential Pitfalls |
|---|---|
|
|
|
|
We retrospectively reviewed 36 patients who underwent arthroscopic rotator cuff repair of full-thickness rotator cuff tears with concurrent arthroscopic capsular release for moderate to severe passive glenohumeral motion loss by the senior authors (L.D.F., F.H.S.). At average follow-up of 2.2 years, average passive shoulder forward flexion improved from 106° preoperatively to 159° postoperatively. External rotation at the side improved from 4° to 65°. Mean University of California at Los Angeles (UCLA) shoulder scores improved from 14.8 to 32.2. These improvements were statistically significant (P < .01). No patient in our cohort suffered iatrogenic fracture or glenohumeral instability after closed manipulation and capsular release. The authors feel that this single-stage, combined approach can effectively treat patients with rotator cuff tears and recalcitrant shoulder stiffness.
Footnotes
The authors report the following potential conflict of interest or source of funding: L.D.F. receives support from AANA. F.H.S. receives support from DePuy Mitek and Smith & Nephew.
Supplementary Data
Anterior and posterior capsular release techniques are first shown in a right shoulder in beach chair position. Then inferior capsular release is shown in a right shoulder in lateral decubitus position. Finally, rotator cuff repair of a right shoulder in beach chair position is shown.
References
- 1.Tauro J.C. Stiffness and rotator cuff tears: Incidence, arthroscopic findings, and treatment results. Arthroscopy. 2006;22:581–586. doi: 10.1016/j.arthro.2006.03.004. [DOI] [PubMed] [Google Scholar]
- 2.Pearsall A.W., Osbahr D.C., Speer K.P. An arthroscopic technique for treating patients with frozen shoulder. Arthroscopy. 1999;15:2–11. doi: 10.1053/ar.1999.v15.0150002. [DOI] [PubMed] [Google Scholar]
- 3.Ide J., Takagi K. Early and long-term results of arthroscopic treatment for shoulder stiffness. J Shoulder Elbow Surg. 2004;13:174–179. doi: 10.1016/j.jse.2003.11.001. [DOI] [PubMed] [Google Scholar]
- 4.Oh J.H., Kim S.H., Lee H.K., Jo K.H., Bin S.W., Gong H.S. Moderate preoperative shoulder stiffness does not alter the clinical outcome of rotator cuff repair with arthroscopic release and manipulation. Arthroscopy. 2008;24:983–991. doi: 10.1016/j.arthro.2008.06.007. [DOI] [PubMed] [Google Scholar]
- 5.Cho N.S., Rhee Y.G. Functional outcome of arthroscopic repair with concomitant manipulation in rotator cuff tears with stiff shoulder. Am J Sports Med. 2008;36:1323–1329. doi: 10.1177/0363546508314402. [DOI] [PubMed] [Google Scholar]
- 6.Cho C.H., Jang H.K., Bae K.C. Clinical outcomes of rotator cuff repair with arthroscopic capsular release and manipulation for rotator cuff tear with stiffness: A matched-pair comparative study between patients with and without stiffness. Arthroscopy. 2015;31:482–487. doi: 10.1016/j.arthro.2014.09.002. [DOI] [PubMed] [Google Scholar]
- 7.Ho W.P., Huang C.H., Chiu C.C. One-stage arthroscopic repair of rotator cuff tears with shoulder stiffness. Arthroscopy. 2013;29:1283–1291. doi: 10.1016/j.arthro.2013.05.024. [DOI] [PubMed] [Google Scholar]
- 8.Kim Y.S., Lee H.J., Park I., Im J.H., Park K.S., Lee S.B. Are delayed operations effective for patients with rotator cuff tears and concomitant stiffness? An analysis of immediate versus delayed surgery on outcomes. Arthroscopy. 2015;31:197–204. doi: 10.1016/j.arthro.2014.08.014. [DOI] [PubMed] [Google Scholar]
- 9.Chuang T.Y., Ho W.P., Chen C.H., Lee C.H., Liau J.J., Huang C.H. Arthroscopic treatment of rotator cuff tears with shoulder stiffness: A comparison of functional outcomes with and without capsular release. Am J Sports Med. 2012;40:2121–2127. doi: 10.1177/0363546512453296. [DOI] [PubMed] [Google Scholar]
- 10.Park J.Y., Chung S.W., Hassan Z., Bang J.Y., Oh K.S. Effect of capsular release in the treatment of shoulder stiffness concomitant with rotator cuff repair: Diabetes as a predisposing factor associated with treatment outcome. Am J Sports Med. 2014;42:840–850. doi: 10.1177/0363546513519326. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Anterior and posterior capsular release techniques are first shown in a right shoulder in beach chair position. Then inferior capsular release is shown in a right shoulder in lateral decubitus position. Finally, rotator cuff repair of a right shoulder in beach chair position is shown.