

Abstract
In this note, we describe an arthroscopic repair of a degenerative tear of the triceps using a suture weave and an anatomic footprint anchor. We are able to assess, debride, and anatomically repair the distal triceps to its insertion. Compared with open procedures, this arthroscopic repair offers lower morbidity, faster recovery, and improved cosmesis. Our goal was to improve the function and strength of the elbow through this arthroscopic surgical fixation.
The triceps serves as the primary extensor of the elbow joint, and injury to this muscle and tendon can cause significant disability. The triceps tendon is a single unit with contributions from the medial, lateral, and long heads of the triceps muscle.1 The triceps tendon inserts into the olecranon, forming a footprint of approximately 21 mm in width and 13 mm in length.2
Traumatic rupture of the triceps tendon can occur, which often requires operative repair to restore the extension strength of the elbow.2 Avulsion from the olecranon process commonly occurs with traumatic ruptures, and the distal triceps tendon incurs much of the damage during such an injury. In the case of chronic injuries, distal triceps tears can be masked by a concomitant olecranon bursitis.3, 4, 5, 6
The most frequent approach to repair the triceps is an open posterior approach to the elbow. Splitting or reflecting the triceps insertion is usually completed for deep exposure. Surgical repair of the triceps tendon to the olecranon process may include heavy nonabsorbable sutures passed through bone tunnels placed in the olecranon process, suture anchors or anatomic footprint repair.2, 3, 7, 8 Distal triceps tears can be managed arthroscopically. Advantages include avoidance of wound healing problems, less morbidity, shortened postoperative recovery, and improved cosmesis. Also, concomitant pathologies and injuries can be addressed from the diagnostic elbow arthroscopic examination, such as olecranon bursitis and traction spurs. Arthroscopic olecranon bursectomy has also been shown to have a faster recovery and significantly lower morbidity compared with open bursectomy.4, 5, 6 The purpose of this technical note and Video 1 is to describe our technique of arthroscopic distal triceps repair.
Surgical Technique
Preoperative Planning
A thorough history and physical examination is paramount in accurate diagnosis. Radiographs and MRI can aid in the identification of traction spurs, calcifications, bursitis, and triceps tear patterns (Fig 1).
Fig 1.

Lateral radiograph of the left elbow showing triceps enthesopathy, scattered distal triceps tendon mineralization, and soft-tissue swelling within the olecranon bursal region.
Positioning
Under general anesthesia, the patient is placed in the prone position. A tourniquet is placed on the upper arm and the elbow positioned with a bump propped under the upper arm. An arm board is used for support. The ulnar nerve site is then carefully marked.
Portals
An anteromedial portal, a proximal anterolateral portal, and a posterior central portal are established to perform a complete diagnostic elbow arthroscopy.
The anterior structures are well visualized with the anteromedial and proximal anterolateral portals, whereas the posterior central portal aids in visualization of the olecranon fossa, the olecranon tip, and the medial and lateral gutters. A proximal posterior portal and a distal posterior portal are then placed to perform arthroscopic olecranon bursectomy.
Olecranon Bursa Excision
The arthroscope (560 H Camera System; Smith & Nephew, Andover, MA) is placed in the more distal posterior portal. An extensive bursitis is commonly encountered, and this is resected away with an oscillating 4.5-mm full-radius shaver (Smith & Nephew) placed through the proximal posterior portal (Figs 2 and 3).
Fig 2.
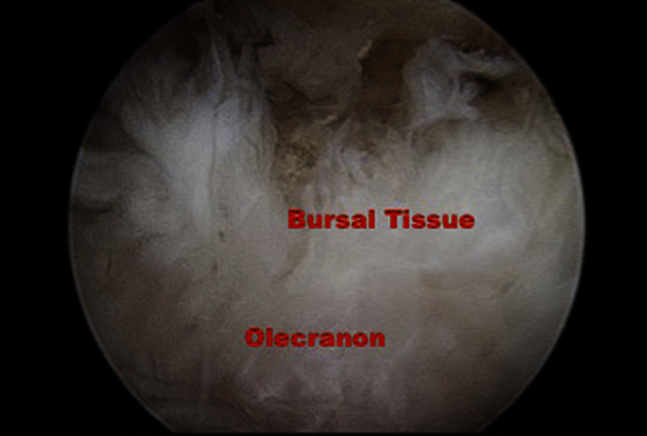
Arthroscopic view of the olecranon bursa from a posterior central viewing portal. Removal of the inflamed bursa assists in improving visualization for the triceps repair.
Fig 3.
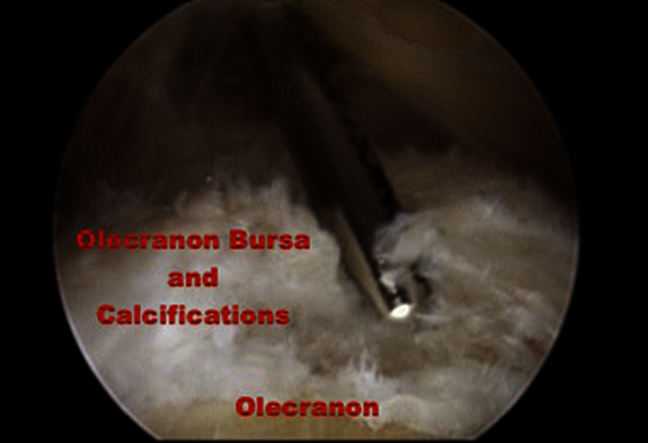
Arthroscopic view from the posterior central viewing portal showing an arthroscopic shaver debriding the edges of the triceps tendon. This helps to define the margins of the tear for later suture fixation.
Triceps Repair
Step I: Diagnosis
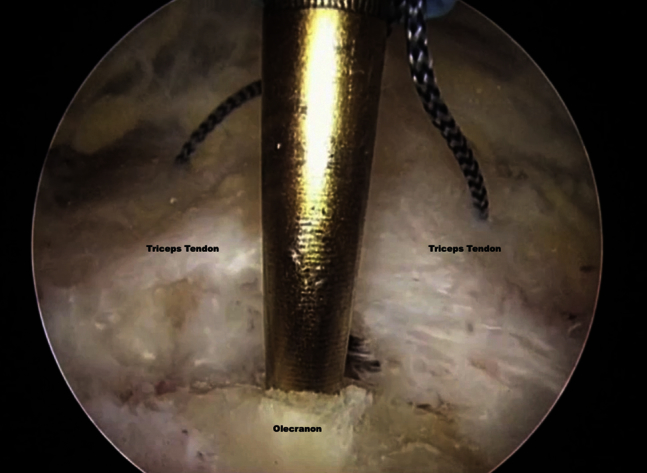
The triceps is clearly visualized once the bursectomy is complete. The edges of the triceps tear are debrided, and the olecranon tip is abraded with a 4.5-mm Helicut burr (Smith & Nephew). Calcifications can be removed to aid in visualization (Fig 4).
Fig 4.
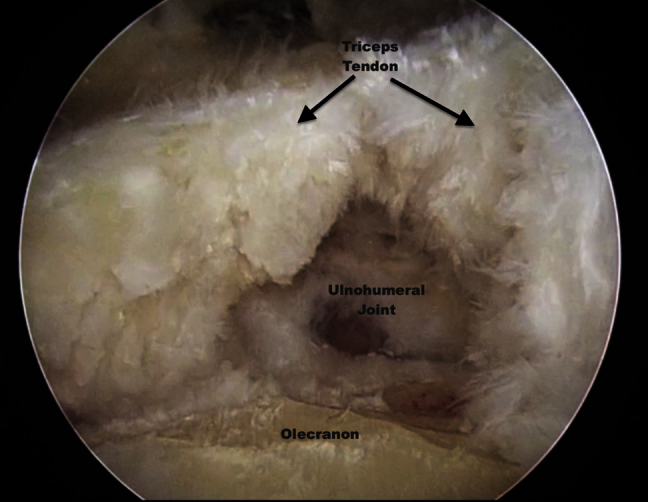
Arthroscopic view from the posterior central viewing portal showing the debrided edges of the triceps tendon and the triceps insertion on the olecranon.
Step II: Suture Passage and Retrieval
The next step is to create a Bunnell suture configuration in the triceps tendon.
A retrograde 60° suture retriever (DePuy Mitek, Raynham, MA) is placed through the proximal posterior portal, and the triceps tendon is pierced just lateral to the apex of the tear (Fig 5). A mid-central posterior portal, approximately 3 cm proximal to the viewing portal, is then established and a plastic cannula is placed. A suture grasper is used to pass a No. 2 Orthocord suture (DePuy Mitek)to the retrograde receiver (Fig 6). With the nonabsorbable suture grasped by the retrograde retriever, the retriever is backed up past the edge of the tear, and the retrograde retriever is brought through the medial apex of the triceps tendon. The suture is handed off to a suture grasper through the mid-central posterior portal.
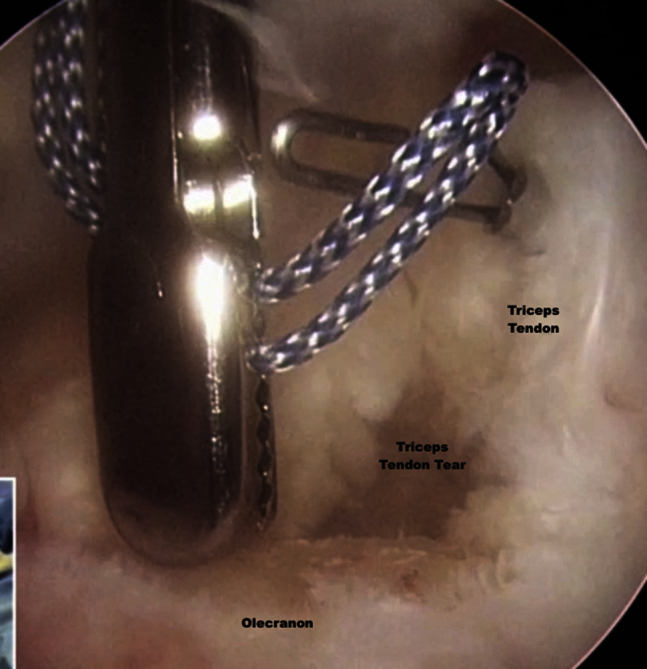
Fig 5.
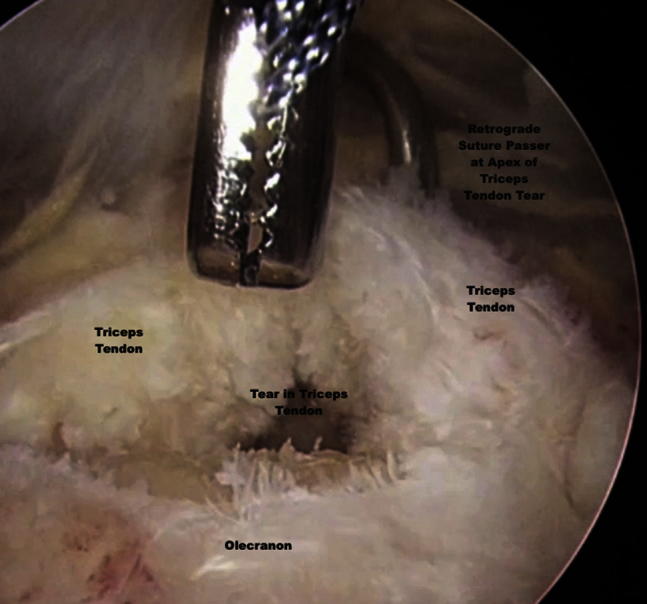
Arthroscopic view from the distal posterior portal. A retrograde retriever is brought in through the proximal posterior portal, and a grasper holding a No. 2 Orthocord is placed through the posterior central portal. The retrograde retriever pierces the triceps tendon just lateral to the apex of the tear.
Fig 6.
Arthroscopic view from the distal posterior portal showing the retrograde retriever capturing the nonabsorbable suture.
The retriever is backed up and reinserted to a more peripheral portion of the tendon. One strand of the nonabsorbable suture is grasped, and then the strand is pulled out of the proximal posterior portal. This step is repeated on the lateral margin. The sutures are then retrieved through the blue cannula in the mid-central posterior portal.
Step III: Anchor Placement
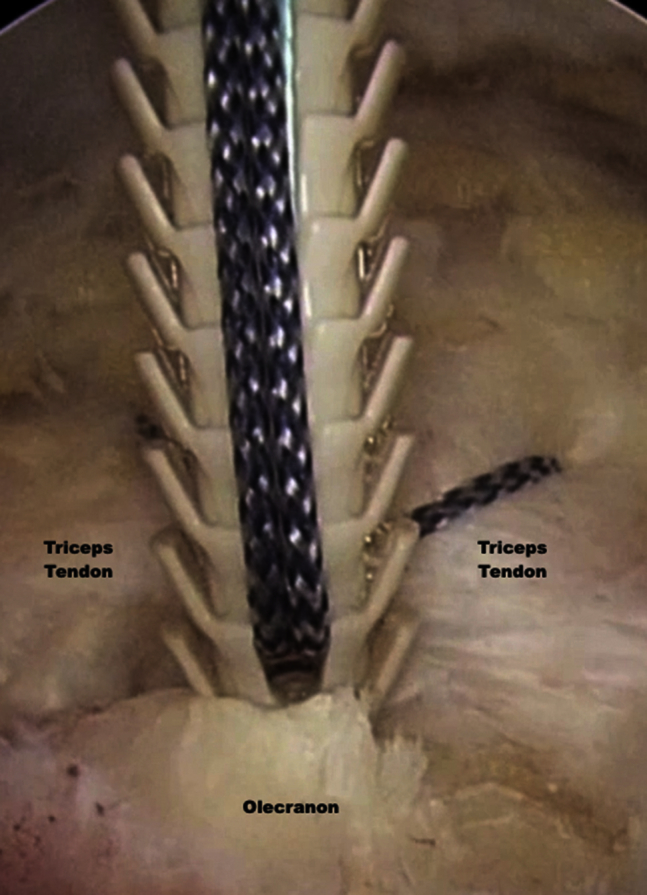
An awl is then used to tap a hole in the olecranon, and a 5.5-mm Footprint PK anchor (Smith & Nephew) is tapped into the olecranon to facilitate closure of the avulsed triceps (Fig 7, Fig 8, Fig 9). The elbow is ranged through flexion and extension and a stable repair is completed.
Fig 7.
Arthroscopic view from the distal posterior portal as an awl is used to tap into the dense bone of the triceps insertion at the olecranon.
Fig 8.
Arthroscopic view from the distal posterior portal during anchor placement within the olecranon.
Fig 9.
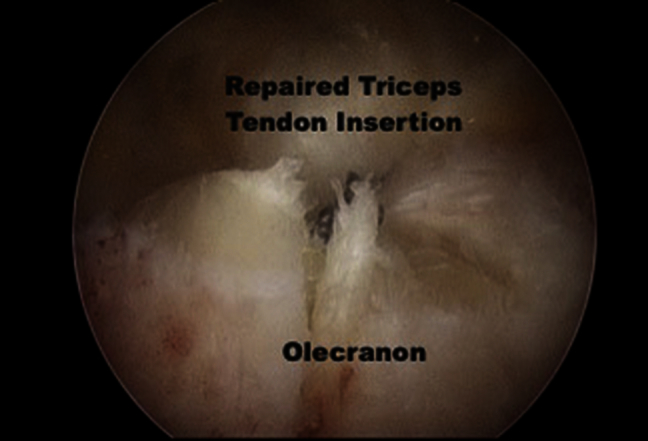
A view from the distal posterior portal after final repair, showing adequate seating of the anchor and an appropriately tensioned repair of the triceps tendon insertion.
All the fluid is then extravasated out of the bursa and 3-0 Nylon sutures are used to close the bursal holes. A compressive wrap is applied and the patient is placed in a plaster splint in full extension.
Discussion
Rupture of the distal triceps tendon is a rare phenomenon, accounting for less than 1% of tendon injuries in the upper extremity.9 As such, there is little evidence and literature to guide orthopaedic surgeons in treating this rare but debilitating injury. The most frequent approach to repair the triceps is an open posterior approach to the elbow. However, advances in the arthroscopic technique have allowed for the repair of distal triceps tears through less invasive measures.
Advantages to an arthroscopic approach include decreased postoperative recovery, smaller incisions with improved cosmesis, and decreased wound complications. Perhaps the greatest advantage of an arthroscopic technique is the added ability to address concomitant elbow pathology, such as olecranon bursitis or olecranon traction spurs.
This technique is not without its disadvantages. Visualization of the triceps tendon is often difficult owing to the thick bursal layer that overlies the triceps insertion. Calcifications often are found with the bursal layer and can make visualization even more challenging. Proper portal placement is paramount to a successful surgery. Also, this technique is not suitable for midsubstance tears, and a careful review of preoperative MRI or ultrasound imaging can help guide the treatment plan.
We prefer the use of suture anchors to secure the distal triceps fixation within the olecranon. Suture anchors allow for an anatomic restoration of the tendinous insertional footprint with a minimal surgical incision. Also, suture anchors have been shown to have comparable biomechanical properties to other methods of distal triceps tendon fixations. Yeh et al.'s7 biomechanical study of 27 cadaveric elbows analyzed 3 different distal triceps repair groups. Elbows were randomly assigned to either a transosseous cruciate repair group, a suture anchor group (2 metal 4.5-mm suture anchors), or an anatomic repair group (a transosseous equivalent footprint repair). Biomechanical measurement of load at yield and peak load was made and cyclic loading was performed for a total of 1,500 cycles. The amount of displacement was measured in each group. The anatomic repair group produced the least amount of displacement, and loading characteristics at yield and peak load were similar in all 3 repair groups. The anatomic repair group was found to provide the greatest coverage of the native triceps insertion, encompassing 86% of the footprint.
There are few published reports regarding the use of suture anchors in distal triceps repairs. The only case series to date is that of Bava et al.,10 who evaluated the clinical outcomes of open distal triceps tendon repair utilizing 2 double-loaded 3.5-mm suture anchors. Five patients were retrospectively reviewed with an average follow-up of 32 months. Results showed the patients to have excellent elbow function on validated clinical outcome measures.
Anchor placement may be complicated by the presence of dense bone within the olecranon. Maintaining good visualization and proper trajectory when placing the anchors can avoid anchor breakage and olecranon fracture. It is often necessary to overtap the anchor to ensure that it is seated to the appropriate depth. See Tables 1 and 2 for summaries of pearls/pitfalls and advantages/disadvantages of arthroscopic distal triceps repair.
Table 1.
Pearls and Pitfalls
| 1. Anchor placement in the olecranon is difficult because of the presence of dense bone. Maintaining a proper trajectory when placing anchors in this region is important to avoid anchor breakage. Overtapping the anchor can ensure proper depth of the anchor. |
| 2. Iatrogenic olecranon fracture can occur with tapping and anchor placement. Ensure that the awl or drill guide is centered over the olecranon before tapping or drilling to avoid this error. |
| 3. Always be mindful of the location of the ulnar nerve during the use of the retrograde suture passer. |
Table 2.
Advantages and Disadvantages of Arthroscopic Triceps Repair
| Advantages: |
| 1. Decreased wound complications associated with bursa excision |
| 2. Quicker recovery, less morbidity than open techniques |
| Disadvantages: |
| 1. Difficult visualization |
| 2. Not suitable for midsubstance tears and more proximal triceps tears |
In our approach, the anterior and posterior aspect of the elbow is visualized from the diagnostic arthroscopy and can address and treat other concomitant pathologies. The direct visualization of the triceps insertional footprint is achieved and anatomic surgical repair is facilitated with the use of nonabsorbable suture and suture anchors. Compared with open procedures, this arthroscopic repair offers lower morbidity, faster recovery, musculature preservation, and improved cosmesis.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Arthroscopy of the left elbow with the patient in the prone position. Viewing is from the posterior central viewing portal and the posterior distal viewing portal with a 30° arthroscope. Treatment of a distal triceps tendon tear with an all-arthroscopic repair is performed.
References
- 1.Madsen M., Marx R.G., Millett P.J., Rodeo A.S., Sperling J.W., Warren R.F. Surgical anatomy of the triceps brachii tendon. Am J Sports Med. 2006;34:1839–1843. doi: 10.1177/0363546506288752. [DOI] [PubMed] [Google Scholar]
- 2.Keener J.D., Chafik D., Kim H.M., Galatz L.M., Yamaguchi K. Insertional anatomy of the triceps brachii tendon. J Shoulder Elbow Surg. 2010;19:399–405. doi: 10.1016/j.jse.2009.10.008. [DOI] [PubMed] [Google Scholar]
- 3.Heikenfeld R., Listringhaus R., Godolias G. Endoscopic repair of tears of the superficial layer of the distal triceps tendon. Arthroscopy. 2014;30:785–789. doi: 10.1016/j.arthro.2014.03.005. [DOI] [PubMed] [Google Scholar]
- 4.Baumbach S.F., Lobo C.M., Badyine I., Wolf M., Kanz K.G. Prepatellar and olecranon bursitis: Literature review and development of a treatment algorithm. Arch Orthop Trauma Surg. 2014;134:359–370. doi: 10.1007/s00402-013-1882-7. [DOI] [PubMed] [Google Scholar]
- 5.Kerr D.R., Carpenter C.W. Arthroscopic resection of olecranon and prepatellar bursae. Arthroscopy. 1990;6:86–88. doi: 10.1016/0749-8063(90)90003-v. [DOI] [PubMed] [Google Scholar]
- 6.Ogilvie-Harris D.J., Gilbart M. Endoscopic bursal resection: The olecranon bursa and prepatellar bursa. Arthroscopy. 2000;16:249–253. doi: 10.1016/s0749-8063(00)90048-3. [DOI] [PubMed] [Google Scholar]
- 7.Yeh P.C., Stephens K.T., Solovyova O. The distal triceps tendon footprint and a biomechanical analysis of 3 repair techniques. Am J Sports Med. 2010;38:1025–1033. doi: 10.1177/0363546509358319. [DOI] [PubMed] [Google Scholar]
- 8.Athwal G.S., McGill R.J., Rispoli D.M. Isolated avulsion of the medial head of the triceps tendon: An anatomic study and arthroscopic repair in 2 cases. Arthroscopy. 2009;25:983–988. doi: 10.1016/j.arthro.2009.02.020. [DOI] [PubMed] [Google Scholar]
- 9.Van Riet R.P., Morrey B.F., Ho E., O'Driscoll S.W. Surgical treatment of distal triceps ruptures. J Bone Joint Surg Am. 2003;85:1961–1967. doi: 10.2106/00004623-200310000-00015. [DOI] [PubMed] [Google Scholar]
- 10.Bava E.D., Barber F.A., Lund E.R. Clinical outcome after suture anchor repair for complete traumatic rupture of the distal triceps tendon. Arthroscopy. 2012;28:1058–1063. doi: 10.1016/j.arthro.2011.12.016. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Arthroscopy of the left elbow with the patient in the prone position. Viewing is from the posterior central viewing portal and the posterior distal viewing portal with a 30° arthroscope. Treatment of a distal triceps tendon tear with an all-arthroscopic repair is performed.