

Abstract
Objectives:
67-Gallium-citrate three-phase bone scan (Ga-TPBS), a new approach for the diagnosis of bone infection is evaluated. The interpretation of TPBS is based on the normal physiological vascular endothelial-related response noted in infection.
Materials and Methods:
Three cases of suspected bone infection as determined by clinical, laboratory, and radiological examinations were further subjected to conventional technetium-99m-TPBS (Tc-99m-TPBS) and Ga-TPBS. Nuclear scan diagnosis of bone infection was made by the presence of generalized vasodilatation with increased capillary permeability noted on the flow and the pool phase of the TPBS and the comparative evaluation of the 4 h delayed Tc-TPBS and 24–48 h delayed Ga-TPBS. Diagnosis of bone infection was confirmed in all three cases on histopathologcal examination of the surgically excised tissues.
Results:
The data clearly indicated that all three cases of bone infection (osteomyelitis) had generalized massive flow and pool pattern. Infection could be diagnosed only on the Ga-TPBS by noting generalized vasodilatation with increased capillary permeability on the flow and the pool phase with focal retention of the radiotracer on the delayed scan.
Conclusions:
By incorporating the concept of vascular endothelial-related response causing massive vasodilatation in infection, the interpretation of the Ga-TPBS can be more précised as it is based on the normal physiology. In comparison to two Tc-99m scans (white blood cell scan + bone marrow scan), a single Ga-TPBS is also cost-effective and compliance friendly. Larger, comparative, and statistically unbiased studies are needed.
Keywords: 67-Gallium-citrate, bone infection, interpretation, massive hyperemia, osteomyelitis, three-phase bone scan, vascular endothelium-related response
INTRODUCTION
67-Gallium (67-Ga)-citrate has been a well-known radionuclide for imaging infection and tumor. Advent of radiolabeled leukocyte (white blood cell [WBC]) imaging, with much higher sensitivity and specificity, rendered the use of 67-Ga-citrate for bone infection obsolete. Second, interpretation of 67-Ga-citrate bone scan required comparison with the technetium-99m (Tc-99m) bone scan. The comparison being subjective in nature, suffered with significant interobserver variability. However, because of the various logistical reasons, radiolabeled WBCs imaging is not done at many centers, even in developed countries like the USA. In such situations, one has to resort to the conventional 67-Ga-citrate bone imaging. Therefore, it is imperative to revisit the 67-Ga-citrate bone imaging in light of the normal physiological response of generalized or massive vasodilatation with increased capillary permeability noted following infection as described for the interpretation of the conventional three-phase bone scan [TPBS, Figure 1].[1] Addition of this component is expected to improve the sensitivity and specificity of the conventional 67-Ga-citrate bone imaging interpretation for bone infection and may even eliminate the necessity of performing Tc-99m bone scan before the 67-Ga-citrate bone scan.
Figure 1.
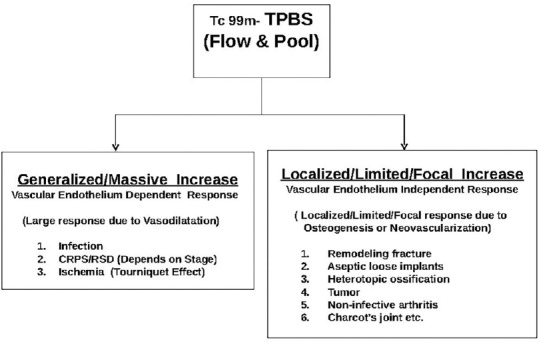
New classification for the interpretation of the technetium-99m three-phase bone scan
MATERIALS AND METHODS
Three cases of foot ulcers of various durations, sizes, and depths with suspicion of osteomyelitis of the underlying bone as determined by clinical, laboratory, and radiological parameters were further evaluated by the three phase Tc-99m-methylene diphosphonate (MDP) bone scan (Tc-TPBS) followed by the three phase 67-Gallium-citrate bone scan (Ga-TPBS). General Electric Co., GE-Infinia Multipeak Gamma Camera, (Milwaukee, WI, USA) was used for scanning, interpretation, and generating the time-activity curves (TACs). For two patients with body mass index (BMI) <30, the usual administered activity was 150–220 MBq (4–6 mCi) intravenously, and 330 MBq (9 mCi) was used in one patient with BMI >30. Imaging of first two phases (flow and pool) of the Ga-TPBS were comparable to the Tc-TPBS, but the third phase (delayed) images for Ga-TPBS were obtained after 24–48 h to permit better tissue clearance and adequate incorporation of the radiotracer to the bone, instead of 3–4 h as done to obtain Tc-TPBS delayed images. For delayed 67-Ga-citrate images, 250,000–1,000,000 total counts (5–20 min) were obtained. The large range in counts obtained (and the maximum time per image) was necessary because quality depended up on the (a) time after the injection that the images are obtained and (b) the ability of the patient to cooperate.[2] Tape was used for immobilization while imaging. During the processing of the images, 2–3 images of the first flow phases were fused to generate better dynamic flow images of the Ga-TPBS because the quality of the imaged obtained are not very good as evident in various illustrations.
The 67-Ga-citrate bone scan interpretation for osteomyelitis is a comparative study with Tc-99m-MDP bone scan. In general, following criteria were used: (1) The combined bone/gallium study was negative for infection in untreated patients when (a) gallium scintigraphy was negative, regardless of the bone scintigraphy results or (b) the distribution activity on both studies was spatially congruent and the relative intensity of gallium activity was less than that of bone activity. (2) The combined bone/gallium study was positive for infection when (a) the distribution of activity on both studies was spatially congruent and the relative intensity of gallium activity was greater than that of bone activity or (b) the distribution of activity on both studies was spatially incongruent, with gallium activity exceeding bone activity in at least one area.(3) The combined bone/gallium study was equivocal for infection when the distribution of activity on both studies was spatially congruent, and the relative intensity of the gallium activity was equal to the bone activity. This result could occur in patients who are taking antibiotics and were partially treated. However, in the presence of generalized increased intensity of skeletal activity, focal inflammatory or neoplastic lesions of the skeleton may not be apparent on images.[2] Visual or quantitative segmental evaluation of the TPBS by drawing a region of interest (ROI) and developing TAC is a helpful tool in diagnosing generalized or massive vasodilatation and increased tissue permeability in much wider area. No quantitative analysis as described by Sorsdahl et al.[3] was performed. Diagnosis of osteomyelitis was confirmed in all three cases on subsequent histopathological examinations of the surgically excised tissues.
Case 1
A 79-year-old male patient presented with diabetes mellitus and chronic nonhealing left heel ulcer with unhealthy granulation in the base. Plane radiograph and computed tomography (CT) scan of the calcaneus revealed: “soft tissue ulcer with swelling and bone destruction appear similar to previous, again consistent with osteomyelitis” [Figure 2a]. Tc-TPBS was performed which revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the left calcaneus [Figure 2b and c]. Ga-TPBS also revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the left calcaneus [Figure 2d and e]. Surgical debridement with curettage of the ulcer was performed. Histopathology confirmed the diagnosis of bone infection.
Figure 2.

(a) Plane radiograph and computed tomography scan, reported as “Soft tissue ulcer with swelling and bone destruction appear similar to previous, again consistent with osteomyelitis.” (b) Time-activity curve after drawing region of interest in different segments of a technetium-99m-methylene diphosphonate flow image for comparison and to confirm generalized increased flow. (c) Technetium-99m-methylene diphosphonate pool and delayed images indicating generalized increased retention of radiotracer in the pool images (upper row) and focal retention of radiotracer in the region of the left calcaneus bone on delayed images (lower row). (d) Time-activity curve after drawing region of interest in different segments of a gallium-67 flow image for comparison and to confirm generalized increased flow. (e) Gallium-67 pool and 48 h delayed images indicating generalized increased retention of radiotracer in the pool images (upper row) and focal retention of radiotracer in the region of the left calcaneus bone on delayed images (lower row)
Case 2
A 65-year-old male patient having chronic ulcer left 5th metatarsal base with low-grade cellulitis. Prior history of the left 5th metatarsal head resection with postgunshot left sciatic nerve injury. A plane radiograph was reported as, “Mild soft tissue swelling and small skin ulceration at the base of the 5th metatarsal, lateral foot. No evidence of osteomyelitis” [Figure 3a]. Tc-TPBS was performed which revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the left 5th metatarsal base, consistent with osteomyelitis [Figure 3b and c]. Ga-TPBS also revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the left 5th metatarsal base, consistent with osteomyelitis [Figure 3d–f]. Surgical debridement with curettage of the ulcer was performed. Histopathology confirmed the diagnosis of bone infection.
Figure 3.

(a) Plane radiograph of the left foot, reported as “Mild soft tissue swelling and small skin ulceration at the base of the 5th metatarsal, lateral foot. No evidence of osteomyelitis.” (b) Time-activity curve after drawing region of interest in different segments of a technetium-99m-methylene diphosphonate flow image for comparison and to confirm generalized increased flow. (c) Technetium-99m-methylene diphosphonate pool and delayed images indicating generalized increased retention of radiotracer in the pool images (upper row) and focal retention of radiotracer in the region of the left 5th metatarsal base on delayed images (lower row). (d) Time-activity curve after drawing region of interest in different segments of a gallium-67 flow image for comparison and to confirm generalized increased flow. (e) Gallium-67 pool and 24 h delayed images indicating generalized increased retention of radiotracer in the pool images (upper row) and focal retention of radiotracer in the region of the left 5th metatarsal base on delayed images (lower row). (f) Gallium-67 pool and 48 h delayed images indicating focal retention of radiotracer in the region of the left 5th metatarsal base
Case 3
A 59-year-old male patient with chronic ulcer over the left ankle was referred to rule out osteomyelitis of lateral malleolus. A plane radiograph was reported as “No evidence of osteomyelitis of the underlying bone” [Figure 4a]. Tc-TPBS was performed which revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the left lateral malleolus, consistent with osteomyelitis [Figure 4b and c]. Ga-TPBS also revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the left lateral malleolus, consistent with osteomyelitis [Figure 4d and e].
Figure 4.

(a) Plane radiograph of the left ankle with enlarged inserts showing the ulceration in the soft tissue over the lateral malleolus. No of osteomyelitis of the lateral malleolus was reported. (b) Time-activity curve after drawing region of interest in different segments of a technetium-99m-methylene diphosphonate flow image for comparison and to confirm generalized increased flow. (c) Technetium-99m-methylene diphosphonate pool and delayed images indicating generalized increased retention of radiotracer in the pool images (upper row) and focal retention of radiotracer in the region of the left lateral malleolus on delayed images (lower row). (d) Time-activity curve after drawing region of interest in different segments of a gallium-67 flow image for comparison and to confirm generalized increased flow. (e) Gallium-67 pool and 48 h delayed images indicating focal retention of radiotracer in the region of the left lateral malleolus
RESULTS
In all three cases, Tc-TPBS was performed which revealed generalized vasodilatation (massive hyperemia) on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the suspected site of the bone infection, underlying the base of the ulcer and reported as consistent with bone infection. Similarly, Ga-TPBS also revealed generalized vasodilatation on the flow and pool phase with focal retention of the radiotracer in the region corresponding to the suspected site of the bone infection, underlying the base of the ulcer. Comparison of the delayed images of the Tc-TPBS and Ga-TPBS was done to support infection. In all the three cases, the 67-Ga-citrate bone scan was found positive for infection. Surgical debridement with curettage of the ulcer was performed in all three cases. Histopathology confirmed the diagnosis of bone infection in all three cases.
DISCUSSION
Early, accurate, and dependable diagnosis of osteomyelitis is crucial in preventing serious morbidity. Radionuclide bone scanning is extremely sensitive in the detection of bone infection in adults[3] and shows bone abnormalities earlier than plane radiography or CT scan.[4,5] Conventionally, 67-Ga-citrate has been used in the diagnosis of bone infection and determining the clinical course of the disease.[6,7] 67-Ga-citrate has been shown to localize in a variety of tumors[8] as well as in the inflammatory lesions.[9] Many mechanisms involved in this uptake have been suggested from time to time. These have ranged from increased capillary permeability to the association of 67-Ga with various proteins,[10] polymorphonuclear leukocytic infiltration,[11] siderophores uptake,[12] and uptake by the infectious microorganisms.[13] It has also been reported that the main 67-Ga-binding substance in inflammatory tissue is keratan polysulfate or oversulfated acid mucopolysaccharide.[14]
The 67-Ga-citrate bone scan interpretation for osteomyelitis is a comparative study with Tc-99m-MDP bone scan. The comparison is visual and subjective with significant interobserver variability. To improve the sensitivity of the 67-Ga-citrate evaluation and reduce the interobserver variability, quantitative bone-gallium scintigraphy in osteomyelitis was described with claim that it “offers excellent specificity and accuracy comparable to the best claims for In-111 WBC imaging. The addition of quantitative ratio analysis adds objectivity to the subjective assessment of spatial in congruency because relative amounts of tracer uptake may be artifactually influenced by altered photographic intensity or other technical factors”.[3] Single photon emission computed tomography (SPECT) 67-Ga-citrate and SPECT Tc-99m bone scans are more sensitive than planar 67-Ga-citrate and planar Tc-99m bone scans specifically for vertebral osteomyelitis.[15,16]
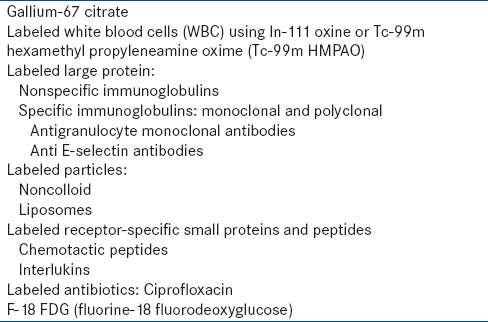
Advent of In-111 oxine and Tc-99m-HMPAO (hexamethylpropylene amine oxime) labeled WBCs imaging has almost replaced 67-Ga-citrate for the diagnosis of osteomyelitis in the appendicular skeletal system. Overall, sensitivity of 88% and specificity of 91% has been reported for WBCs imaging in the diagnosis of osteomyelitis.[17] However, 67-Ga-citrate is much more convenient to use and is less expensive than the cumbersome, time-consuming task of withdrawing whole blood and separating, washing repeatedly, labeling, and reinjecting radiolabeled WBCs.[18,19] Besides requiring appropriate laboratory facilities and expertise, cell radiolabeling involves handling of whole blood with its inherent risks to laboratory personnel(s) and multiple opportunities for mistakes.[20] It has also been reported that WBC bone scanning may be more accurate than bone-gallium scanning for acute osseous infection[4,21,22,23] but gallium is of equivalent or superior accuracy, especially in subacute or chronic infections.[18,24,25,26,27] In-111 WBCs have shown decreased sensitivity for demonstrating infection of central lesions of the axial skeleton compared to the peripheral lesions[28] and “cold” defects in the presence of confirmed osteomyelitis are more common than originally anticipated.[20,24] Causes of false-positive uptake of In-111 WBCs are the same as with 67-Ga-citrate.[29] Confirmation for the diagnosis of chronic osteomyelitis is often the cause of referral for nuclear bone scan. Several radiopharmaceuticals have been described for infection [Table 1] but WBC scan for acute infection and 67-Ga-citrate scan for chronic infection are commonly used.
Table 1.
Various radiopharmaceuticals used for infection
Interpretation of Tc-TPBS based on the vascular endothelium response helps in differentiation between infection and other noninfection pathologies more precisely.[1] The first part or flow-phase of the TPBS is also known as nuclear angiography suggests increased flow of the blood to the limb or the region. Further characterization of the flow-phase is not done; hence, the specificity decreases. Etiology of increased flow varies in different conditions and therefore, the type or pattern of increased flow also varies in different conditions. In conditions where increased flow is as a result of generalized vasodilatation with increased capillary permeability, the increased flow is generalized, and massive involving much larger segment of the extremity is commonly noted in infection. This is normal physiological response for cellular and noncellular defense mechanism to reach at the site of infection in adequate quantity for the containment of infection. Vasodilatation in infection is the direct result of the positive endothelial response. Vascular endothelium is the largest organ in the human body, though not officially designated the status of an organ. It is present all over, from head to toe, and therefore, the vascular endothelium derived response is also quite extensive, dilating the main vessel(s) and opening the collateral circulations, producing massive hyperemia. Quantitative interpretation of the first two parts of the three-phase bone scan in segments of the limb (proximal/middle/distal), either by pixel counts or by drawing ROI and developing the TAC certainly improves the quality of the interpretation.[1]
Patients with high probability of bone infection as determined by clinical, laboratory, and radiological parameters were chosen for this preliminary study, and the Tc-TPBS study results were further reevaluated by Ga-TPBS. Preliminary evaluation of 3–4 h delayed Tc-TPBS with 24–48 h delayed Ga-TPBS in 3 cases has been encouraging. Diagnosis of osteomyelitis was confirmed in all three cases on subsequent histopathological examinations of the surgically excised tissues. In retrospective analysis, interpretation of only Ga-TPBS is interesting. Generalized or massive vasodilatation (hyperemia) on the flow and pool phase with focal retention of the radiotracer (67-Ga-citrate) in the region corresponding to the suspected site of the bone infection may be enough to establish the diagnosis of bone infection on Ga-TPBS, even without the need to get a prior Tc-99 m bone scan for comparative analysis or to be used in conjunction with the Tc-TPBS to further strengthen the diagnosis of bone infection. In comparison to two Tc-99m scans (WBC scan + bone marrow scan), a single Ga-TPBS is also cost-effective and compliance friendly. SPECT-CT of delayed images will further help in localization of the infection. Radiation effectiveness has not been worked out. This is a very small, selective, and statistically biased report of three cases only but certainly an interesting way and concept of interpretation of Ga-TPBS for firmer diagnosis of bone infection than what was achieved so far by conventional method of interpretation.
Variations are not uncommon in medicine. Our rainbow has black and brown colors also. Sometimes, it may be difficult to exclude infection. In situations of poor vascularity with compromised delivery of the radiotracer, low-grade chronic infection, very early phase of infection, in bilateral limb infections as often noted in bilateral diabetic/neuropathic feet or in persons with endothelial dysfunction, which often presents clinically by associated erectile dysfunction, the classical extensive flow, and tissue phase response involving large and massive hyperemia may not be present and clear distinction between infection or no infection may be difficult. The matter compounds and becomes yet more difficult when two or more pathologies exist together. This is the first study of its kind where TPBS has been performed with 67-Ga-citrate. Larger and statistically unbiased studies are needed for proper evaluation of this new concept.
CONCLUSION
Ga-TPBS is a novel concept in determining the bone infection. This method may be of great use in centers where radiolabeled leukocyte imaging facility is not available for various logistical reasons. This is the first study of its kind. Larger, comparative, and statistically unbiased studies are needed for proper evaluation of this new concept.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kumar K. Three phase bone scan interpretation based upon vascular endothelial response. Indian J Nucl Med. 2015;30:104–10. doi: 10.4103/0972-3919.152949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.SNM-Protocol. Society of Nuclear Medicine Procedure Guideline for Gallium Scintigraphy in Inflammation. Version 3.0. Approved. 2004 Jun 2; [Google Scholar]
- 3.Sorsdahl OA, Goodhart GL, Williams HT, Hanna LJ, Rodriquez J. Quantitative bone gallium scintigraphy in osteomyelitis. Skeletal Radiol. 1993;22:239–42. doi: 10.1007/BF00197666. [DOI] [PubMed] [Google Scholar]
- 4.Gupta NC, Prezio JA. Radionuclide imaging in osteomyelitis. Semin Nucl Med. 1988;18:287–99. doi: 10.1016/s0001-2998(88)80038-2. [DOI] [PubMed] [Google Scholar]
- 5.David R, Barron BJ, Madewell JE. Osteomyelitis, acute and chronic. Radiol Clin North Am. 1987;25:1171–201. [PubMed] [Google Scholar]
- 6.Handmaker H, Leonards R. The bone scan in inflammatory osseous disease. Semin Nucl Med. 1976;6:95–105. doi: 10.1016/s0001-2998(76)80039-6. [DOI] [PubMed] [Google Scholar]
- 7.Scoles PV, Hilty MD, Sfakianakis GN. Bone scan patterns in acute osteomyelitis. Clin Orthop Relat Res. 1980;153:210–7. [PubMed] [Google Scholar]
- 8.Higasi T, Nakayama Y, Murata A, Sugiyama M, Nakamura K. Clinical evaluation of 67 Ga-citrate scanning. J Nucl Med. 1972;13:196–201. [PubMed] [Google Scholar]
- 9.Lavender JP, Lowe J, Barker JR, Burn JI, Chaudhri MA. Gallium 67 citrate scanning in neoplastic and inflammatory lesions. Br J Radiol. 1971;44:361–6. doi: 10.1259/0007-1285-44-521-361. [DOI] [PubMed] [Google Scholar]
- 10.Tzen KY, Oster ZH, Wagner HN, Jr, Tsan MF. Role of iron-binding proteins and enhanced capillary permeability on the accumulation of gallium-67. J Nucl Med. 1980;21:31–5. [PubMed] [Google Scholar]
- 11.Tsan MF, Chen WY, Scheffel U, Wagner HN., Jr Studies on gallium accumulation in inflammatory lesions: I. Gallium uptake by human polymorphonuclear leukocytes. J Nucl Med. 1978;19:36–43. [PubMed] [Google Scholar]
- 12.Emery T, Hoffer PB. Siderophore-mediated mechanism of gallium uptake demonstrated in the microorganism Ustilago sphaerogena. J Nucl Med. 1980;21:935–9. [PubMed] [Google Scholar]
- 13.Menon S, Wagner HN, Jr, Tsan MF. Studies on gallium accumulation in inflammatory lesions: II. Uptake by Staphylococcus aureus: Concise communication. J Nucl Med. 1978;19:44–7. [PubMed] [Google Scholar]
- 14.Ando A, Nitta K, Ando I, Katsuda S, Tonami N, Hiraki T, et al. 67Ga accumulation in inflammatory lesion and its mechanism: Comparison with malignant tumor. Eur J Nucl Med. 1987;12:560–6. doi: 10.1007/BF00296098. [DOI] [PubMed] [Google Scholar]
- 15.Knight D, Gray HW, McKillop JH, Bessent RG. Imaging for infection: Caution required with the Charcot joint. Eur J Nucl Med. 1988;13:523–6. doi: 10.1007/BF00256628. [DOI] [PubMed] [Google Scholar]
- 16.Love C, Patel M, Lonner BS, Tomas MB, Palestro CJ. Diagnosing spinal osteomyelitis: A comparison of bone and Ga-67 scintigraphy and magnetic resonance imaging. Clin Nucl Med. 2000;25:963–77. doi: 10.1097/00003072-200012000-00002. [DOI] [PubMed] [Google Scholar]
- 17.Kolindou A, Liu Y, Ozker K, Krasnow AZ, Isitman AT, Hellman RS, et al. In-111 WBC imaging of osteomyelitis in patients with underlying bone scan abnormalities. Clin Nucl Med. 1996;21:183–91. doi: 10.1097/00003072-199603000-00001. [DOI] [PubMed] [Google Scholar]
- 18.Al-Sheikh W, Sfakianakis GN, Mnaymneh W, Hourani M, Heal A, Duncan RC, et al. Subacute and chronic bone infections: Diagnosis using In-111, Ga-67 and Tc-99m MDP bone scintigraphy, and radiography. Radiology. 1985;155:501–6. doi: 10.1148/radiology.155.2.3157204. [DOI] [PubMed] [Google Scholar]
- 19.Hoffer PB, Neumann RD. Gallium and infection. In: Gottschalk A, Hoffer PB, Potchen EJ, editors. Diagnostic Nuclear Medicine. 2nd ed. Baltimore: Williams and Wilkins; 1988. p. 1122. [Google Scholar]
- 20.Mok YP, Carney WH, Fernandez-Ulloa M. Skeletal photopenic lesions in In-111 WBC imaging. J Nucl Med. 1984;25:1322–6. [PubMed] [Google Scholar]
- 21.Dutcher JP, Schiffer CA, Johnston GS. Rapid migration of 111indium-labeled granulocytes to sites of infection. N Engl J Med. 1981;304:586–9. doi: 10.1056/NEJM198103053041007. [DOI] [PubMed] [Google Scholar]
- 22.Maurer AH, Millmond SH, Knight LC, Mesgarzadeh M, Siegel JA, Shuman CR, et al. Infection in diabetic osteoarthropathy: Use of indium-labeled leukocytes for diagnosis. Radiology. 1986;161:221–5. doi: 10.1148/radiology.161.1.3763871. [DOI] [PubMed] [Google Scholar]
- 23.Propst-Proctor SL, Dillingham MF, McDougall IR, Goodwin D. The white blood cell scan in orthopedics. Clin Orthop Relat Res. 1982;168:157–65. [PubMed] [Google Scholar]
- 24.Datz FL, Thorne DA. Effect of chronicity of infection on the sensitivity of the In-111-labeled leukocyte scan. AJR Am J Roentgenol. 1986;147:809–12. doi: 10.2214/ajr.147.4.809. [DOI] [PubMed] [Google Scholar]
- 25.Merkel KD, Brown ML, Dewanjee MK, Fitzgerald RH., Jr Comparison of indium-labeled-leukocyte imaging with sequential technetium-gallium scanning in the diagnosis of low-grade musculoskeletal sepsis. A prospective study. J Bone Joint Surg Am. 1985;67:465–76. [PubMed] [Google Scholar]
- 26.Schauwecker DS, Park HM, Mock BH, Burt RW, Kernick CB, Ruoff AC, 3rd, et al. Evaluation of complicating osteomyelitis with Tc-99m MDP, In-111 granulocytes, and Ga-67 citrate. J Nucl Med. 1984;25:849–53. [PubMed] [Google Scholar]
- 27.Sfakianakis GN, Al-Sheikh W, Heal A, Rodman G, Zeppa R, Serafini A. Comparisons of scintigraphy with In-111 leukocytes and Ga-67 in the diagnosis of occult sepsis. J Nucl Med. 1982;23:618–26. [PubMed] [Google Scholar]
- 28.Schauwecker DS. Osteomyelitis: Diagnosis with In-111-labeled leukocytes. Radiology. 1989;171:141–6. doi: 10.1148/radiology.171.1.2928518. [DOI] [PubMed] [Google Scholar]
- 29.Abreu SH. Skeletal uptake of indium 111-labeled white blood cells. Semin Nucl Med. 1989;19:152–5. doi: 10.1016/s0001-2998(89)80009-1. [DOI] [PubMed] [Google Scholar]