

Abstract
Aims
To examine associations between cannabis use in adolescence (at age 18) and unemployment and social welfare assistance in adulthood (at age 40) among Swedish men.
Design
Longitudinal cohort study.
Setting and Participants
A total of 49 321 Swedish men born in 1949–51, who were conscripted to compulsory military service at 18–20 years of age.
Measurements
All men answered two detailed questionnaires at conscription and were subject to examinations of physical aptitude psychological functioning and medical status. By follow‐up in national databases, information on unemployment and social welfare assistance was obtained.
Findings
Individuals who used cannabis at high levels in adolescence had increased risk of future unemployment and of receiving social welfare assistance. Adjusted for all confounders (social background, psychological functioning, health behaviours, educational level, psychiatric diagnoses), an increased relative risk (RR) of unemployment remained in the group reporting cannabis use > 50 times [RR = 1.26, 95% confidence interval (CI) = 1.04–1.53] only. For social welfare assistance, RR in the group reporting cannabis use 1–10 times was 1.15 (95% CI = 1.06–1.26), RR for 11–50 times was 1.21 (95% CI = 1.04–1.42) and RR for > 50 times was 1.38 (95% CI = 1.19–1.62).
Conclusions
Heavy cannabis use among Swedish men in late adolescence appears to be associated with unemployment and being in need of social welfare assistance in adulthood. These associations are not explained fully by other health‐related, social or behavioural problems.
Keywords: Cannabis, cohort study, education, longitudinal, social welfare assistance, unemployment
Introduction
Cannabis use, and especially heavy use, in adolescence has been associated with social and socio‐economic consequences, such as impaired cognitive functioning 1, low educational attainment 2, 3 and educational problems 4. Cannabis use in late adolescence and early adulthood has also been associated with lower income and lower work commitment in early adulthood, i.e. before 30 years of age 5, 6, 7. Cannabis users have been found less likely to work 8, 9, and in a recent study we found adolescent heavy cannabis users to be at an increased risk of later receiving disability pension 10. Moreover, cannabis users have been found to be at an increased risk for receiving social welfare assistance and to be less likely to leave the assistance system 11.
However, previous research on possible associations between cannabis use and later social outcomes is inconsistent, and above all fails to elucidate the causal direction and possible mechanisms behind these associations. For one thing, a recent Australian study combining three long‐running longitudinal studies showed that adolescent cannabis users had an increased risk of dropping out of high school, but not of later welfare dependence 12. In a recent American study, the importance of unobserved confounding in the relationship between cannabis use and labour market outcomes was examined, and the authors concluded that cannabis use may be less harmful with regard to employment and income than previous studies have reported 13.
Given that cognitive impairment may possibly result from heavy cannabis use 1, 14, one would expect cannabis users to be less likely to achieve high education and, as a consequence, more likely to be unemployed and in need of societal support. However, it has not been clarified whether cannabis use causes disengagement from education and subsequent work opportunities with increased dependence on societal aid as a result, or if the observed associations are instead results of overlapping risk factors, which increases the risk for both cannabis use and adverse social consequences. For example, several studies have reported that conduct problems in childhood precede illicit drug use, and may consequently also affect later outcomes in life 15. Furthermore, the reported causal link between persistent cannabis use and neuropsychological (in terms of IQ) decline 14 has been questioned, and possible confounding from socio‐economic status has been highlighted 16. In view of the policy debate on the availability of cannabis, knowledge on the long‐term effects of its use is important, and more solid evidence is needed.
By using a population‐based cohort with data on cannabis use in adolescence as well as an extensive number of covariates in childhood, adolescence and adulthood, we aimed to determine whether there is an association between adolescent cannabis use (age 18) and adverse life‐course outcomes in adulthood. Specifically, we wanted to assess the associations between adolescent cannabis use and unemployment and receiving social welfare assistance 20 years later, and to what extent any association is explained by a wide range of potential confounders, such as social background, mental function (e.g. IQ), conduct problems, health behaviours, achieved educational level and later psychiatric and/or drug‐related diagnoses.
Methods
Study population
Our study cohort, which has been described in detail elsewhere 17, 18, is based on 49 321 Swedish men born from 1949 to 1951 and conscripted to compulsory military service in 1969–70 (at age 18–20 years).
In brief, the study cohort comprises 97–98% of the approximately 18‐year‐old Swedish male population at that time; 2–3% were exempted due to severe handicaps or congenital disorders. All men answered two questionnaires, one concerned with family and social background, school performance, behaviour and adjustment, psychological factors and self‐rated health, and the other focused on alcohol, tobacco and illicit drug use. They were subject to examinations of physical aptitude and psychological functioning, including cognitive ability as measured by IQ tests. All men underwent medical examination by a physician, and any diagnosis was recorded according to the Swedish version of the International Classification of Disease (ICD) 8th revision (ICD‐8). Those with indications of a psychiatric disorder were examined by a psychiatrist.
Study exposure
The study exposure is life‐time cannabis use as reported during conscription. The conscripts completed questions on ever having used drugs (including cannabis), which drugs had ever been used and frequency of use from a list of alternatives. For the purpose of this study we used the question on frequency of cannabis use, which had fixed responding alternatives, i.e. never, one time, two to four times, five to 10 times (the three later groups were combined into one to 10 times), 11–50 times and > 50 times.
Study outcome—follow‐up
Study outcomes are unemployment and social welfare assistance, and data were collected from the Longitudinal Register of Education and Labor Market Statistics (LISA) 19 between the years 1990 and 1995, i.e. when the men were aged 39–46 years. The LISA register started in 1990, such that it contains data from 1990 and onwards only. The conscript cohort was linked to LISA by unique personal identification numbers.
Unemployment
Unemployment is defined according to Statistics Sweden as any person who is (1) lacking work, (2) currently available for work and (3) seeking work. In Sweden, a person is eligible for unemployment insurance compensation given that they have been in work for a specified time‐period before being unemployed. In this study, we defined unemployment as having received any income from an unemployment insurance fund during 1990–95 (yes/no). Eligible participants (i.e. at risk for unemployment) were those individuals who reported an occupation in the National Population and Housing Censuses 1990.
Social welfare assistance
Social welfare assistance is provided to people who, due to illness, unemployment (and not entitled to insurance) or other special circumstances, are in need of economic support. Often people have other types of income, either from work, sickness insurance or similar, but in cases where the income does not attain a defined level of subsistence, social welfare assistance is granted. Social welfare assistance was categorized as having received it at least once during 1990–95 (yes/no).
Confounders
In this study, we adjusted for a number of potential confounders that have been found to influence the associations between cannabis use, unemployment and social welfare assistance.
Childhood/adolescence
Social background was measured by (1) childhood socio‐economic position (SEP) based on the father's occupational position in 1960: non‐manual workers, manual workers and no occupation. The data were from the National Population and Housing Census, (2) having divorced parents (yes/no) and (3) having been in contact with the police and/or childcare authorities (yes/no).
Mental function was measured on a stanine scale of general intelligence (based on scores from multiple tests 20 and social maturity (high versus low levels of extraversion, initiative, independence and responsibility on a five‐level scale) 20. Low scores on these measures aimed to identify individuals with potential adjustment problems. We also included having been diagnosed with a psychiatric disease (according to ICD‐8) at conscription in our analyses.
Health behaviours were measured by: tobacco smoking, divided into three categories (none, one to 10 and > 10 cigarettes/day); alcohol consumption defined as ‘risky use’ including one of the following (ever been apprehended by the police for drunkenness, ever consumed alcohol during a hangover, been drunk often/quite often, drinking ≥ 250 g of alcohol per week); and having used other illicit drugs, such as amphetamine, morphine, lysergic acid diethylamide (LSD) and opium, which was divided into three categories (none, yes and yes, injected).
Adulthood
Educational level
Educational level was categorized according to the highest obtained educational level (primary ≥ 9 years, secondary ≥ 12 years and tertiary education > 12 years). Data were collected from 1990 in the LISA register.
Psychiatric and drug‐related disorders
We assessed whether having been diagnosed and hospitalized due to a psychiatric (neurotic disorders or personality disorders being the most common ones) and/or drug‐related disorder during 1973–89 (yes/no) affected the associations between cannabis use and the outcomes. Data for diagnoses were collected from the Swedish National Patient register. See Fig. 1 for a detailed time‐line.
Figure 1.
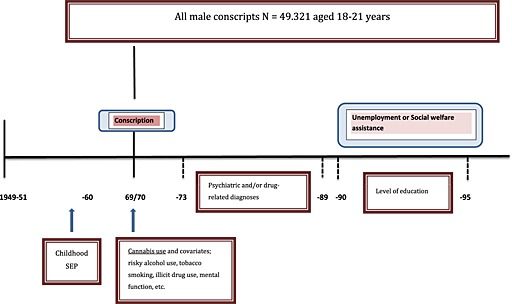
Time‐line showing conscript cohort, record linkages and timing of surveys. The cohort consisted of all 49 321 Swedish males presenting for mandatory conscription at ages 18–20 years. SEP: socio‐economic position
Statistical analysis
Modified Poisson regression was used for direct and accurate estimations of relative risks (i.e. risk ratios: RR) of unemployment and social welfare assistance across levels of cannabis use compared to non‐use. This is the preferred method for RR estimation in cohort studies with common outcomes 21. RRs and 95% confidence intervals were computed by means of the GENMOD procedure in SAS, version 9.3 (SAS Institute, Inc., Cary, NC, USA)
First, crude associations were examined, and thereafter blocks of potential confounders were included stepwise in multivariable models: social background factors (childhood SEP, divorced parents and contact with police and/or childcare authorities), mental functions (social maturity, cognitive ability and having a psychiatric diagnosis) and health behaviours (tobacco smoking, risky use of alcohol and having tried other illicit drugs). Finally, all potential confounders were included simultaneously, also adding attained level of education, and psychiatric and/or drug‐related disorders.
In the cohort, 42 240 men had full information on all variables and were included in the follow‐up of social welfare assistance. In the follow‐up of unemployment, only those 37 606 men who reported having an occupation in 1990 were included, as only those individuals with an occupation were regarded as being at risk of unemployment.
Results
In total, 3734 (8.8%) of 42 240 individuals reported having used cannabis at 18 years of age. Approximately 616 individuals (1.5%) reported use more than 50 times. In almost all cases, the proportions of the examined confounders increased with increased use of cannabis (Table 1). For example, 75% among the frequent cannabis users reported having been in contact with the police and/or childcare authorities, 93% being daily smokers and 80% also having used other illicit drugs, compared to 25, 55 and 0.7%, respectively, among those reporting never having used cannabis.
Table 1.
Distribution of covariate frequencies (%) across levels of adolescent cannabis use measured at ~18 years of age in a cohort of Swedish men.
| Adolescent cannabis use | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | Never | 1–10 times | 11–50 times | >50 times | ||||||
| n | % | n | % | n | % | n | % | n | % | |
| 42 240 | 100 | 38 506 | 91.16 | 2515 | 5.95 | 603 | 1.43 | 616 | 1.46 | |
| Childhood/adolescence | ||||||||||
| Parental SEP | ||||||||||
| Non‐manual occupation | 18 142 | 42.95 | 16 417 | 42.63 | 1170 | 46.52 | 291 | 48.26 | 264 | 42.86 |
| Manual occupation | 23 210 | 54.95 | 21 286 | 55.28 | 1294 | 51.45 | 297 | 49.25 | 333 | 54.06 |
| No occupation | 888 | 2.10 | 803 | 2.09 | 51 | 2.03 | 15 | 2.49 | 19 | 3.08 |
| Divorced parents | 4285 | 10.14 | 3556 | 9.23 | 443 | 17.61 | 129 | 21.39 | 157 | 25.49 |
| Contact with police or childcare authorities | 11 727 | 27.76 | 9683 | 25.15 | 1207 | 47.99 | 377 | 62.52 | 460 | 74.68 |
| IQ (1–9) | 5.40a | 2.05b | 5.36a | 2.06b | 5.84a | 1.84b | 5.62a | 1.84b | 5.48a | 1.84b |
| Social maturity (1–5) | 3.10a | 0.87b | 3.13a | 0.86b | 3.01a | 0.92b | 2.67a | 1.00b | 2.20a | 0.93b |
| Psychiatric diagnosis | 4855 | 11.49 | 3864 | 10.03 | 451 | 17.93 | 202 | 33.50 | 338 | 54.87 |
| Cigarette smoking | ||||||||||
| None | 17 859 | 42.28 | 17 367 | 45.10 | 373 | 14.83 | 73 | 12.11 | 46 | 7.47 |
| 1–10 cigarettes/day | 13 501 | 31.96 | 12 211 | 31.71 | 929 | 36.94 | 179 | 29.68 | 182 | 29.55 |
| >10 cigarettes/day | 10 880 | 25.76 | 8928 | 23.19 | 1213 | 48.23 | 351 | 58.21 | 388 | 62.99 |
| Risky alcohol use | 5334 | 12.63 | 4148 | 10.77 | 669 | 26.60 | 230 | 38.14 | 287 | 46.59 |
| Illicit drug use | ||||||||||
| None | 40 956 | 96.96 | 38 380 | 99.67 | 2147 | 85.37 | 303 | 50.25 | 126 | 20.45 |
| Yes | 1049 | 2.48 | 124 | 0.32 | 330 | 13.12 | 244 | 40.46 | 351 | 56.98 |
| Yes, injected | 235 | 0.56 | 2 | 0.01 | 38 | 1.51 | 56 | 9.29 | 139 | 22.56 |
| Adulthood | ||||||||||
| Level of education | ||||||||||
| Tertiary education | 11 691 | 27.68 | 10 637 | 27.62 | 777 | 30.89 | 153 | 25.37 | 124 | 20.13 |
| Secondary education | 19 487 | 46.13 | 17 616 | 45.75 | 1239 | 49.26 | 308 | 51.08 | 324 | 52.60 |
| Primary education | 11 062 | 26.19 | 10 253 | 26.63 | 499 | 19.84 | 142 | 23.55 | 168 | 27.27 |
| Psychiatric disorder | 1806 | 4.28 | 1529 | 3.97 | 145 | 5.77 | 55 | 9.12 | 77 | 12.50 |
| Drug‐related disorder | 167 | 0.40 | 89 | 0.23 | 34 | 1.35 | 16 | 2.65 | 28 | 4.55 |
Mean;
standard deviation; SEP = socio‐economic position.
Unadjusted cannabis use in adolescence was associated with increased RR of being unemployed and receiving social welfare assistance at follow‐up in cannabis users at all levels (Tables 2 and 3), with RR = 1.72 for being unemployed and RR = 3.13 for receiving social welfare assistance in the group using cannabis > 50 times. The RRs increased in a graded manner, i.e. the more frequent cannabis use in adolescence, the higher the RR of future unemployment and receiving social welfare assistance. Furthermore, when unadjusted, hospitalizations due to psychiatric and or drug‐related disorders after age 20 years were associated with increased risks of later social welfare assistance, with RR = 3.97 and 5.67, respectively.
Table 2.
Relative risk of unemployment as adult across levels of adolescent cannabis use (and across confounders) in a cohort of Swedish men.
| Crude model | Multivariable model | Multivariable model | Multivariable model | Multivariable model | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Adolescent cannabis use | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI |
| Never | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – |
| 1–10 times | 1.11 | 1.01–1.21 | 1.02 | 0.94–1.11 | 1.10 | 1.00–1.20 | 1.03 | 0.94–1.13 | 1.05 | 0.96–1.15 |
| 11–50 times | 1.27 | 1.08–1.51 | 1.14 | 0.96–1.34 | 1.15 | 0.98–1.36 | 1.07 | 0.89– 1.29 | 1.07 | 0.89–1.29 |
| > 50 times | 1.72 | 1.49–1.98 | 1.43 | 1.24–1.66 | 1.37 | 1.18–1.59 | 1.26 | 1.04–1.53 | 1.26 | 1.04–1.53 |
| Childhood/adolescence | ||||||||||
| Parental SEP | ||||||||||
| Non‐manual occupation | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – |
| Manual occupation | 1.39 | 1.33–1.46 | 1.35 | 1.27–1.38 | 1.19 | 1.14–1.25 | 1.18 | 1.13–1.24 | 1.13 | 1.08–1.19 |
| No occupation | 1.54 | 1.34–1.76 | 1.44 | 1.25–1.64 | 1.26 | 1.10–1.44 | 1.24 | 1.09–1.42 | 1.20 | 1.05–1.37 |
| Divorced parents | 1.40 | 1.32–1.49 | 1.28 | 1.20–1.36 | 1.21 | 1.14–1.29 | 1.19 | 1.12–1.27 | 1.17 | 1.10–1.25 |
| Contact with police or childcare authorities | 1.48 | 1.41–1.54 | 1.37 | 1.31–1.44 | 1.26 | 1.20–1.31 | 1.19 | 1.13–1.25 | 1.16 | 1.11–1.22 |
| IQ | 1.37 | 1.34–1.39 | 1.28 | 1.25–1.31 | 1.26 | 1.23–1.29 | 1.18 | 1.15–1.21 | ||
| Social maturity | 1.26 | 1.23–1.29 | 1.11 | 1.08–1.14 | 1.11 | 1.08–1.14 | 1.09 | 1.06–1.12 | ||
| Psychiatric diagnosis | 1.38 | 1.30–1.46 | 1.01 | 0.95–1.08 | 1.00 | 0.94–1.07 | 1.01 | 0.95–1.08 | ||
| Cigarette smoking | ||||||||||
| None | 1.00 | – | 1.00 | – | 1.00 | – | ||||
| 1–10 cigarettes/day | 1.34 | 1.27–1.41 | 1.17 | 1.11–1.23 | 1.14 | 1.08–1.20 | ||||
| > 10 cigarettes/day | 1.54 | 1.46–1.62 | 1.24 | 1.17–1.31 | 1.18 | 1.12–1.25 | ||||
| Risky alcohol use | 1.48 | 1.40–1.56 | 1.06 | 0.99–1.12 | 1.04 | 0.98–1.10 | ||||
| Illicit drug use | ||||||||||
| None | 1.00 | – | 1.00 | – | 1.00 | – | ||||
| Yes | 1.29 | 1.14–1.46 | 1.02 | 0.87–1.20 | 1.03 | 0.87–1.21 | ||||
| Yes, injected | 1.75 | 1.37–2.22 | 1.05 | 0.80–1.38 | 1.01 | 0.77–1.32 | ||||
| Adulthood | ||||||||||
| Level of education | ||||||||||
| Tertiary | 1.00 | – | 1.00 | – | ||||||
| Secondary | 2.10 | 1.97–2.24 | 1.61 | 1.49–1.74 | ||||||
| Primary | 2.43 | 2.27–2.60 | 1.63 | 1.52–1.74 | ||||||
| Psychiatric disorder | 1.87 | 1.72–2.04 | 1.46 | 1.34–1.59 | ||||||
| Drug‐related disorder | 1.77 | 2.00–2.62 | 1.28 | 0.85–0.90 | ||||||
RR = relative risk; 95% CI = 95% confidence interval; SEP = socio‐economic position.
Table 3.
Relative risk of social welfare assistance as adult across levels of adolescent cannabis use (and across confounders) in a cohort of Swedish men.
| Crude model | Multivariable model | Multivariable model | Multivariable model | Multivariable model | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Adolescent cannabis use | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI |
| Never | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – |
| 1–10 times | 1.52 | 1.39–1.66 | 1.26 | 1.15–1.37 | 1.36 | 1.24–1.48 | 1.15 | 1.05–1.26 | 1.16 | 1.06–1.26 |
| 11–50 times | 2.12 | 1.84–2.44 | 1.59 | 1.39–1.83 | 1.56 | 1.35–1.79 | 1.24 | 1.06–1.46 | 1.22 | 1.04–1.42 |
| >50 times | 3.13 | 2.82–3.48 | 2.13 | 1.92–2.37 | 1.90 | 1.70–2.13 | 1.48 | 1.26–1.73 | 1.39 | 1.19–1.62 |
| Childhood/adolescence | ||||||||||
| Parental SEP | ||||||||||
| Non‐manual occupation | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – | 1.00 | – |
| Manual occupation | 1.61 | 1.52–1.70 | 1.49 | 1.41–1.57 | 1.27 | 1.20–1.34 | 1.24 | 1.17–1.31 | 1.18 | 1.12–1.25 |
| No occupation | 2.29 | 1.97–2.66 | 1.96 | 1.72–2.23 | 1.62 | 1.43–1.85 | 1.55 | 1.37–1.77 | 1.42 | 1.26–1.61 |
| Divorced parents | 1.92 | 1.80–2.03 | 1.53 | 1.44–1.63 | 1.41 | 1.32–1.50 | 1.35 | 1.27–1.44 | 1.28 | 1.20–1.36 |
| Contact with police or childcare authorities | 2.24 | 2.14–2.35 | 1.91 | 1.81–2.01 | 1.67 | 1.58–1.76 | 1.40 | 1.32–1.48 | 1.32 | 1.25–1.40 |
| IQ | 1.52 | 1.49–1.56 | 1.36 | 1.33–1.40 | 1.32 | 1.29–1.36 | 1.20 | 1.17–1.24 | ||
| Social maturity | 1.45 | 1.41–1.49 | 1.12 | 1.09–1.16 | 1.11 | 1.08–1.14 | 1.06 | 1.03–1.10 | ||
| Psychiatric diagnosis | 2.04 | 1.93–2.16 | 1.22 | 1.14–1.30 | 1.17 | 1.09–1.25 | 1.07 | 0.98–1.16 | ||
| Cigarette smoking | ||||||||||
| None | 1.00 | – | 1.00 | – | 1.00 | – | ||||
| 1–10 cigarettes/day | 1.89 | 1.77–2.02 | 1.51 | 1.40–1.62 | 1.44 | 1.35–1.54 | ||||
| > 10 cigarettes/day | 2.83 | 2.66–3.02 | 1.87 | 1.74–2.00 | 1.72 | 1.61–1.84 | ||||
| Risky alcohol use | 2.38 | 2.25–2.51 | 1.27 | 1.20–1.35 | 1.17 | 1.10–1.24 | ||||
| Illicit drug use | ||||||||||
| None | 1.00 | – | 1.00 | – | 1.00 | – | ||||
| Yes | 2.15 | 1.94–2.39 | 1.12 | 0.98–1.29 | 1.11 | 0.97–1.27 | ||||
| Yes, injected | 3.40 | 2.92–3.96 | 1.09 | 0.90–1.31 | 0.98 | 0.82–1.19 | ||||
| Adulthood | ||||||||||
| Level of education | ||||||||||
| Tertiary | 1.00 | – | 1.00 | – | ||||||
| Secondary | 3.09 | 2.83–3.37 | 1.95 | 1.76–2.15 | ||||||
| Primary | 3.84 | 3.51–4.20 | 1.99 | 1.82–2.19 | ||||||
| Psychiatric disorder | 3.97 | 3.75–4.21 | 2.52 | 2.38–2.68 | ||||||
| Drug‐related disorder | 5.67 | 5.13–6.26 | 3.00 | 2.67–3.37 | ||||||
RR = relative risk; 95% CI = 95% confidence interval; SEP = socio‐economic position.
When adjusted for confounders, the associations between cannabis use, unemployment and social welfare assistance were attenuated substantially. This was evident with every block of confounders that were included in the analysis, especially those measured in childhood and adolescence. Further, the attenuation was seen both in men with and without childhood disadvantage (parental SEP = no occupation, divorced parents, or having been in contact with police or childcare authorities), i.e. any cannabis × disadvantage interaction on unemployment and social welfare assistance was unsupported (not shown in the tables). Attained level of education and having a psychiatric and/or drug‐related diagnosis after age 20 did not affect the result to any significant extent. When all confounders where entered simultaneously, the increased RR of receiving social welfare assistance remained statistically significant in all three groups reporting cannabis use at age 18 (RR = 1.16, 1.22 and 1.39). The RR for unemployment remained significant only in the group reporting cannabis use > 50 times (RR = 1.26). It was still the case that having a psychiatric and or drug‐related disorder increased the risk of later social welfare assistance (RR = 2.52 and 3.00), as did a majority of the confounders included in the analysis with, for example, tobacco smoking of one to 10 cigarettes/day (RR= 1.44), > 10 cigarettes/day (1.72) and risky alcohol consumption (RR = 1.17).
Discussion
The results of this study suggest that high levels of cannabis use in adolescence are associated with increased risks of unemployment and receiving social welfare assistance at age 40, also after adjusting for social background, mental functions, health behaviours, educational level and psychiatric and/or drug‐related diagnoses. This is partly in line with previous studies that have reported on these associations up to age 30 6, 11. However, while prior research has found these results mainly among frequent or heavy cannabis users, we observed an increased risk of receiving social welfare assistance at all user levels in a graded manner. When adjusted for confounders, the association with later unemployment remained in the heavy‐user group only.
One possible explanation to the observed association between cannabis use and adverse life‐course outcomes is that underlying social and/or genetic factors are associated both with the risk of cannabis use and with later unemployment and social welfare assistance. A recent twin study found that environmental factors influenced both the risk of early‐onset cannabis use and early school‐leaving 22, while another stressed the importance of shared genes on the relation between drug use and subsequently resulting in a low socio‐economic position (SEP) 23. Additionally, there seems to be an association between lower childhood SEP and later cannabis use 24. In contrast, higher parental education and income has also been associated with higher rates of cannabis use in early adulthood 25, and active cannabis users have been found to have a higher educational level, on average, than the general population, while at the same time being more likely to be unemployed 26. Childhood SEP has been linked to later education level which, in turn, is linked strongly to future employment 27, thus making it difficult to disentangle the possible effects of cannabis use in this chain of associations.
As expected, our study showed that lower educational level was associated with unemployment and receiving social welfare assistance. Education, which in general is attained in young adulthood, has been described as capturing the transition from parental SEP to own adult SEP, and is also a strong determinant of later employment and social life opportunities 27. At the same time, attained educational level did not affect the association between cannabis use and social welfare assistance to any significant extent. As shown in Table 1, level of education differed surprisingly little between cannabis users and non‐users.
Recent studies have reported tobacco smoking, alcohol and cannabis use to be influenced by aggregated genetic risk factors shared between users of these substances 28, and both cannabis and tobacco use in adolescence to be associated strongly with subsequent adverse educational outcomes, with tobacco smoking consistently showing an even stronger effect than cannabis 29. In fact, cannabis use and cigarette use at age 16 have both been found to be associated, to a similar degree, with later psychotic experiences 30. In this particular study, however, almost all participants reported using cannabis with tobacco, highlighting the complexity in teasing out the effects of cannabis from tobacco 30.
We were not able to adjust for genetic factors, but we adjusted for a number of social and behavioural characteristics shown previously to be associated with cannabis use and adverse outcomes. For one thing, our results show that childhood SEP did not eliminate the observed associations between adolescent cannabis use and later social welfare assistance; nor did cognitive ability, having a psychiatric diagnosis at age 18 or other illicit drug use, even if the associations were attenuated after these adjustments. Cannabis use has been associated with psychiatric diseases 17, 18 and later drug dependence 6 that may affect future life opportunities. At the same time, several factors seem to moderate these associations, including family history, genetic factors, history of childhood abuse and the age at onset of cannabis use 31, 32. It might be pointed out that psychiatric diseases as a consequence of cannabis use, and a possible explanation of adverse outcomes, are more likely to occur later in life. However, we also examined whether having been diagnosed and hospitalized later due to psychiatric and/or drug‐related diseases would affect our results but, interestingly, this was not the case. The RRs remained largely unaffected.
Thus, we are not able to explain fully the observed associations between adolescent heavy cannabis use and later unemployment and social welfare assistance. The associations found in our study probably develop over a long period of time. The fact that almost all the relevant confounders were associated with social welfare assistance raises the question of residual confounding. It is well known that a small group engages in antisocial behaviour (e.g. drug use) during all stages of life, while for the large majority this is limited to the adolescent years 33. Another often highlighted issue is the importance of age of initiation of drug use 34. Unfortunately, we have no knowledge of initiation age or the drug history of the subjects after conscription. It is possible that continued cannabis use and/or other illicit drug use explain the increased risk of an adverse life‐course. It may also be that conduct problems in childhood precede cannabis use in our sample, and thus explains later outcomes in life. We controlled for having been in contact with the police and/or childcare authorities, which attenuated but did not eliminate the risks for later social welfare dependence. Residual confounding from, for instance, childhood problems can nevertheless not be excluded.
Our follow‐up time spans over the years 1990–95, i.e. when the participants were aged 39–46 years and at an age when they should be established on the labour market. In the 1990s there was a severe economic recession in Sweden, resulting in both increased unemployment and number of social welfare assistance recipients, which may have influenced our results. However, the situation was the same for cannabis users and non‐users, and high unemployment only increases the number of cases to study. In addition to this, high unemployment in society usually has broader effects and thus the associations found in our study may be diluted, as many non‐users also may end up unemployed. Information on unemployment during the 1980s, i.e. when unemployment rates were low in Sweden and when the cohort members were in their early 30s, is available in our data set. However, regression analyses with unemployment from 1980 to 1985 instead of unemployment from 1990 to 1995 produced very similar associations, both before and after multivariable adjustment.
In our analyses, we did not distinguish between long‐ and short‐term unemployed; it is possible that the observed associations are accounted for by one of the groups. In our study, most men had been unemployed for 6 months or longer 35. Furthermore, we had no information on the frequency of unemployment or of receiving social welfare assistance and our sample included men only, which is a limitation. However, it is a large representative sample comprising approximately 98% of the Swedish male population at that time. We have no information on the 2% (1000) of individuals who did not participate at conscription. They were exempted due to severe handicaps or congenital disorders which, if anything, may increase the risk of later social welfare assistance. Nearly 3% (1377) of individuals had died during follow‐up, and we know from previous analyses that this group reported high levels of, for example, risky alcohol consumption, smoking and conduct problems at conscription 36.
With this study, we expand previous research by examining an extensive number of possible confounders; for example, many previous studies on cannabis use and later social life outcomes have accounted only for depression and/or anxiety, and no other psychiatric and/or drug‐related diagnoses. Also, our study shows that heavy cannabis use co‐occurs with heavy cigarette smoking and risky alcohol drinking, and that all these behaviours are in fact linked to later social life outcomes.
Conclusions
This study showed that heavy cannabis use in late adolescence was associated with an increased risk of future unemployment, and that cannabis use, also at lower levels of use, was associated with receiving social welfare assistance 20 years later. These associations could be explained to some extent, but not fully, by other health‐related, social or behavioural problems.
Declaration of interests
None.
Acknowledgements
We thank Andreas Lundin for valuable help with the data linkages. This study was supported by grants provided by the Research Council for Health, Working Life and Welfare (Forte2014‐0691) and by the Stockholm County Council (ALF project 20130025).
Danielsson, A.‐K. , Falkstedt, D. , Hemmingsson, T. , Allebeck, P. , and Agardh, E. (2015) Cannabis use among Swedish men in adolescence and the risk of adverse life course outcomes: results from a 20 year‐follow‐up study. Addiction, 110: 1794–1802. doi: 10.1111/add.13042.
References
- 1. Harvey M. A., Sellman J. D., Porter R., Frampton C. M. The relationship between non‐acute use of cannabis and cognition. Drug Alcohol Rev 2007; 26: 309–19. [DOI] [PubMed] [Google Scholar]
- 2. Legleye S., Obradovic I., Janssen E., Spilka S, Le Névzet O, Beck F. Influence of cannabis use trajectories, grade repetition and family background on the school-dropout rate at the age of 17 years in France. Eur J Public Health 2010; 20: 157–63. [DOI] [PubMed] [Google Scholar]
- 3. Horwood J. L., Fergusson D. M., Hayatbakhsh M. R., Najman J. M., Coffey C. et al. Cannabis use and educational achievement: findings from three Australasian cohort studies. Drug Alcohol Depend 2010; 110: 247–53. [DOI] [PubMed] [Google Scholar]
- 4. Degenhardt L., Coffey C., Carlin J. B., Swift W, Moore E, Patton G. C. Outcomes of occasional cannabis use in adolescence: 10‐year follow‐up study in Victoria, Australia. Br J Psychiatry 2010; 196: 290–5. [DOI] [PubMed] [Google Scholar]
- 5. Fergusson D. M., Horwood J. L., Beautrais A. L. Cannabis and educational achievement. Addiction 2003; 98: 1681–92. [DOI] [PubMed] [Google Scholar]
- 6. Fergusson D. M., Boden J. M. Cannabis use and later life outcomes. Addiction 2008; 103: 969–76. [DOI] [PubMed] [Google Scholar]
- 7. Hyggen C. Does smoking cannabis affect work commitment? Addiction 2012; 107: 1309–15. [DOI] [PubMed] [Google Scholar]
- 8. Davstad I., Leifman A., Allebeck P., Romelsjö A. Predictors of a favourable socio‐economic situation in middle age for Swedish conscripts with self‐reported drug use. Drug Alcohol Depend 2013; 128: 37–44. [DOI] [PubMed] [Google Scholar]
- 9. Brook J. S., Lee J. Y., Finch S. J., Koppel J., Brook D. W. Psychosocial factors related to cannabis use disorders. Subst Abuse 2011; 32: 242–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Danielsson A. K., Agardh E., Hemmingsson T., Allebeck P., Falkstedt D. Cannabis use in adolescence and risk of future disability pension: a 39‐year longitudinal cohort study. Drug Alcohol Depend 2014; 143: 239–43. [DOI] [PubMed] [Google Scholar]
- 11. Pedersen W. Cannabis and social welfare assistance: a longitudinal study. Addiction 2011; 106: 1636–43. [DOI] [PubMed] [Google Scholar]
- 12. Silins E., Horwood J. L., Patton G. C., Fergusson D. M., Olsson C. A., Hutchinson D. M. et al. Young adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychiatry 2014; 1: 286–93. [DOI] [PubMed] [Google Scholar]
- 13. Popovici I., French M. T. Cannabis use, employment, and income: fixed‐effects analysis of panel data. J Behav Health Serv Res 2014; 1: 85–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Meier M. H., Caspia A., Amblere A., Harrington H. L., Houts R., Keefed R. S. E. et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A 2012; 109: 2657–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Fergusson D. M., Woodward L. J., Ridder E. M. Conduct and attentional problems in childhood and adolescence and later substance use, abuse and dependence: results of a 25‐year longitudinal study. Drug Alcohol Depend 2007; 88: 14–26. [DOI] [PubMed] [Google Scholar]
- 16. Rogeberg O. Correlations between cannabis use and IQ change in the Dunedin cohort are consistent with confounding from socioeconomic status. Proc Natl Acad Sci U S A 2013; 110: 4251–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Andréasson S., Allebeck P., Engström A., Rydberg U. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet 1987; 2: 1483–6. [DOI] [PubMed] [Google Scholar]
- 18. Manrique‐Garcia E., Zammit S., Dalman C., Hemmingsson T., Andreasson S., Allebeck P. Cannabis, schizophrenia and other non‐affective psychoses: 35 years of follow‐up of a population‐based cohort. Psychol Med 2012; 42: 1321–8. [DOI] [PubMed] [Google Scholar]
- 19. Statistics Sweden . 2009. Longitudinell Integrationsdatabas för Sjukförsäkrings‐ och Arbetsmarknadsstudier (LISA) 1990–2007 [Longitudinal Integrated Database for Sickness Insurance and Labour Market Research 1990–2007]. 2009: 1. Available at: http://www.scb.se/Pages/PublishingCalendarViewInfo____259923.aspx?PublObjId=11454 (accesed 4 March 2015).
- 20. Sörberg A., Lundin A., Allebeck P., Melin B., Falkstedt D., Hemmingsson T. Cognitive ability in late adolescence and disability pension in middle age: follow‐up of a national cohort of Swedish males. PLoS One 2013; 8: e78268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Zou G. A modified Poisson regression approach to prospective studies with binary data. Am J Epidemiol 2004; 159: 702–6. [DOI] [PubMed] [Google Scholar]
- 22. Verweij J. H., Huizinka A. C., Agrawal A., Martin N. G., Lynskey M. T. Is the relationship between early‐onset cannabis use and educational attainment causal or due to common liability? Drug Alcohol Depend 2013; 133: 580–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Bergen S. E., Gardner C. O., Aggen S. H., Kendler K. S. Socioeconomic status and social support following illicit drug use: causal pathways or common liability? Twin Res Hum Genet 2008; 1: 266–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Daniel J. Z., Hickman M., Macleod J., Wiles N., Lingford‐Hughes A., Farell M. et al. Is socioeconomic status in early life associated with drug use? A systematic review of the evidence. Drug Alcohol Rev 2009; 28: 142–53. [DOI] [PubMed] [Google Scholar]
- 25. Humensky J. L. Are adolescents with high socioeconomic status more likely to engage in alcohol and illicit drug use in early adulthood? Subst Abuse Treat Prev Pol 2010; 5: 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. van der Pol P., Liebregts N., de Graaf R., Ten Have M, Korf D. J., van den Brink W. Mental health differences between frequent cannabis users with and without dependence and the general population. Addiction 2013; 108: 1459–69. [DOI] [PubMed] [Google Scholar]
- 27. Galobardes B., Shaw M., Lawlor D. A., Lynch J. W., Smith D. Indicators of socioeconomic position (part 1). J Epidemiol Community Health 2006; 60: 7–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Vink J. M., Hottenga J. J., de Geus E. J. C., Willemsen G., Neale M. C., Furberg H. et al. Polygenic risk scores for smoking: predictors for alcohol and cannabis use? Addiction 2014; 109: 1141–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Stiby A. I., Hickman M., Munafò M. R., Heron J., Yip V. L., Macleod J. Adolescent cannabis and tobacco use and educational outcomes at age 16: birth cohort study. Addiction in press. doi: 10.1002/add.12827. E‐pub 2015 Feb 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Gage S. H., Hickman M., Heron J., Munafò M. R., Lewis G., Macleod J. et al. Associations of cannabis and cigarette use with psychotic experiences at age 18: findings from the Avon Longitudinal Study of Parents and Children. Psychol Med 2014; 44: 3435–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Radhakrisnan R., Wilkinson S. T., D'Souza D. C. Gone to pot—a review of the association between cannabis and psychosis. Front Psychiatry 2014; 5: article 54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Greydanus D. E., Hawver E. K., Greydanus M. M., Merrick J. Marijuana: current concepts. Front Public Health 2013; 1: 1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Moffit T. Adolescent‐limited and life‐course‐persistent life course behavior: a developmental taxonomy. Psychol Rev 1993; 100: 674–701. [PubMed] [Google Scholar]
- 34. Butterworth P., Slade T., Degenhardt L. Factors associated with the timing and onset of cannabis use and cannabis use disorder: results from the 2007 Australian National Survey of Mental Health and Well‐Being. Drug Alcohol Rev 2014; 33: 555–64. [DOI] [PubMed] [Google Scholar]
- 35. Lundin A., Hemmingsson T. Adolescent predictors of unemployment and disability pension across the life course—a longitudinal study of selection in 49 321 Swedish men. Institute for Evaluation of Labour Market and Education Policy (IFAU). Working paper 2013: 25. Available at: http://www.ifau.se/Upload/pdf/se/2013/wp‐2013‐25‐Adolescent‐predictors‐of‐unemployment‐and‐disability‐pension‐across‐the‐life‐course.pdf (accessed 4 March 2015)
- 36. Lundin A., Lundberg I., Hallsten L., Ottosson J., Hemmingsson T. Unemployment and mortality—a longitudinal prospective study on selection and causation in 49321 Swedish middle‐aged men. J Epidemiol Community Health 2010; 64: 22–8. [DOI] [PubMed] [Google Scholar]