

Abstract
The introduction and the extended clinical use of nilotinib in the first-line treatment of chronic myeloid leukemia have been based on company-sponsored trials. Independent confirmations are extremely important. We report an investigator-sponsored study of nilotinib 300 mg twice daily in 130 chronic myeloid leukemia patients in early chronic phase. A deep molecular response was achieved in 46% (MR4.0) and 17% (MR4.5) of patients at 2 years; 58% of the enrolled patients achieved a MR4.0 at least once, with a sustained MR4.0 in 52% of them. With a median observation of 29 months (range 24–37 months), 77% of patients were still on treatment with nilotinib. The reasons for permanent discontinuation were: 3% progression, 5% failure or suboptimal response, 8% adverse events, 1% treatment-free remission, and 5% other reasons. Thirteen thrombotic arterial events were reported in 12 patients. A prospective evaluation of metabolic effects showed an increase of fasting glucose without significant variations of glycated hemoglobin, an increase of total cholesterol (both low density lipoprotein and high density lipoprotein fractions) and a decrease of triglycerides. This study confirms a high and rapid efficacy of nilotinib 300 mg twice daily and provides detailed information on the type and incidence of non-hematologic and metabolic adverse events (clinicaltrials.gov identifier: 01535391).
Introduction
Nilotinib is a second generation BCR-ABL1 tyrosine kinase inhibitor (TKI).1 It has been approved for the first-line treatment of newly diagnosed, chronic phase (CP) Philadelphia chromosome-positive (Ph+), BCR-ABL1-positive (BCR-ABL1+) chronic myeloid leukemia (CML), following the report of a company-sponsored phase 3 prospective randomized trial (ENESTnd) comparing nilotinib to imatinib 400 mg once daily (OD).2 Several updates of the study, over 6 years, have confirmed the initial findings that nilotinib was superior to imatinib for any degree of molecular response, and for the rapidity of the response.3,4 The progression-free survival (PFS) was reported to be marginally improved and no difference in overall survival (OS) was detectable.3,4 In the ENESTnd trial, two different nilotinib doses were tested, namely 300 mg twice daily (TD) and 400 mg TD.2–4 The 300 mg TD dose was selected for approval because it was reported to be as effective as, but less toxic than, the 400 mg TD dose. A relevant issue was the cardiovascular toxicity, with focus on arterial occlusive events (ischemic heart disease (IHD), peripheral arterial occlusive disease (PAOD) and ischemic cerebrovascular events, ICVEs), that at 5 years were reported in 2.1% of patients in the imatinib arm, in 6.8% of patients in the nilotinib 300 mg TD arm, and in 12.6% of patients in the nilotinib 400 mg TD arm.3
This concern was raised and reinforced by other independent studies, for the most part retrospective and mainly in second-line treatment, reporting a significant incidence of cardiovascular adverse events (CVAEs) during nilotinib treatment.5–9 With a minimum observation of 24 months, the molecular response rates in a second single-arm company-sponsored study of nilotinib 300 mg TD, the ENEST1st trial, were even higher compared to the ENESTnd results, with consistent safety data.10 There are no independent, investigator-sponsored studies of the drug in first-line treatment, with the exception of the two small pilot studies that were performed prior to the approval of nilotinib in first-line treatment, at the dose registered for second-line treatment (400 mg TD).11–14 When the 300 mg TD dose became the standard in first-line therapy, the GIMEMA CML Working Party designed a prospective phase 3b single-arm trial of nilotinib 300 mg TD, to independently assess the efficacy and safety. Since all patients have now been followed for a minimum of two years, we herein report the results of the main analysis of response and adverse events (AEs).
Methods
A phase 3b single-arm study of nilotinib, 300 mg TD was conducted in adult patients with newly diagnosed CP BCR-ABL1+ CML (clinicaltrials.gov identifier:01535391). A dose increase to 400 mg TD was scheduled for suboptimal response or failure (2009 European LeukemiaNet, ELN, criteria),15 excluding disease progression, in the absence of toxicity or relevant BCR-ABL1 mutations. Pre-treatment with imatinib for up to 30 days was permitted. The primary endpoint was the rate of MR4.0 at 24 months. The secondary endpoints are detailed in the Online Supplementary Table S1. The study was reviewed and approved by the Internal Review Board of all the participating institutions. The cut-off date for this analysis was June 30, 2015.
The detection of a Ph chromosome and/or a BCR-ABL1 fusion gene associated with consistent morphologic features were required to confirm the CML diagnosis and the chronic (CP), accelerated (AP) or blast disease phase (BP) were defined according to current ELN criteria.16 Risk scores were calculated according to Sokal,17 Euro,18 and EUTOS19 formulations. The molecular response (MR) was assessed by peripheral blood RT-PCR, according to the International Scale (IS).20 Definitions: early molecular response (EMR), BCR-ABL1 transcript ≤ 10% at 3 months; major molecular response (MMR or MR3.0), BCR-ABL1 transcript ≤ 0.1%; MR4.0 and MR4.5, BCR-ABL1 transcript ≤ 0.01%, and ≤ 0.0032%, respectively, in samples with > 10,000, and > 32,000 ABL1 copies, respectively;21,22 sustained MR4.0 or MR4.5, stable response for > 1 year with > 3 evaluable tests. Molecular tests were performed every 3 months. The cytogenetic response was assessed by chromosome banding analysis at 3, 6 and 12 months; if there were < 20 available metaphases, a fluorescence in situ hybridization (FISH) analysis on peripheral blood cells was accepted (complete cytogenetic response, CCyR, ≤1% of BCR-ABL1 positive nuclei, > 200 nuclei analyzed).16 Mutational analysis of BCR-ABL1 kinase domain point mutations (Sanger Sequencing) was performed in case of progression, failure or suboptimal response.15,23 OS, PFS, and event-free survival (EFS, or survival without treatment discontinuation) were calculated from treatment start until death (OS), until death or progression to AP or BP (PFS), or until death, progression to AP or BP, failure on nilotinib or nilotinib treatment discontinuation for any cause, except treatment-free remission (EFS), respectively. Probabilities of OS, PFS and EFS were calculated using the Kaplan-Meier method.24 Patients who discontinued nilotinib and patients who underwent allogeneic stem cell transplantation were not censored for OS and PFS.
The rates of molecular and cytogenetic response “at” milestones were calculated by dividing the number of responders at that time-point by the number of all enrolled patients. The time to response was calculated from treatment start until the first achievement of the response. The cumulative probability of response was calculated taking into consideration the presence of competing risks (failure, progression or death).25,26
The AEs were graded according to the NCI Common Terminology Criteria for Adverse Events version 4.0 (CTCAE v4.0). Lipid modifications were graded according to adapted American Association of Clinical Endocrinologists (AACE) criteria,27 and glucose abnormalities according to adapted American Diabetes Association (ADA) criteria.28
Results
Baseline characteristics
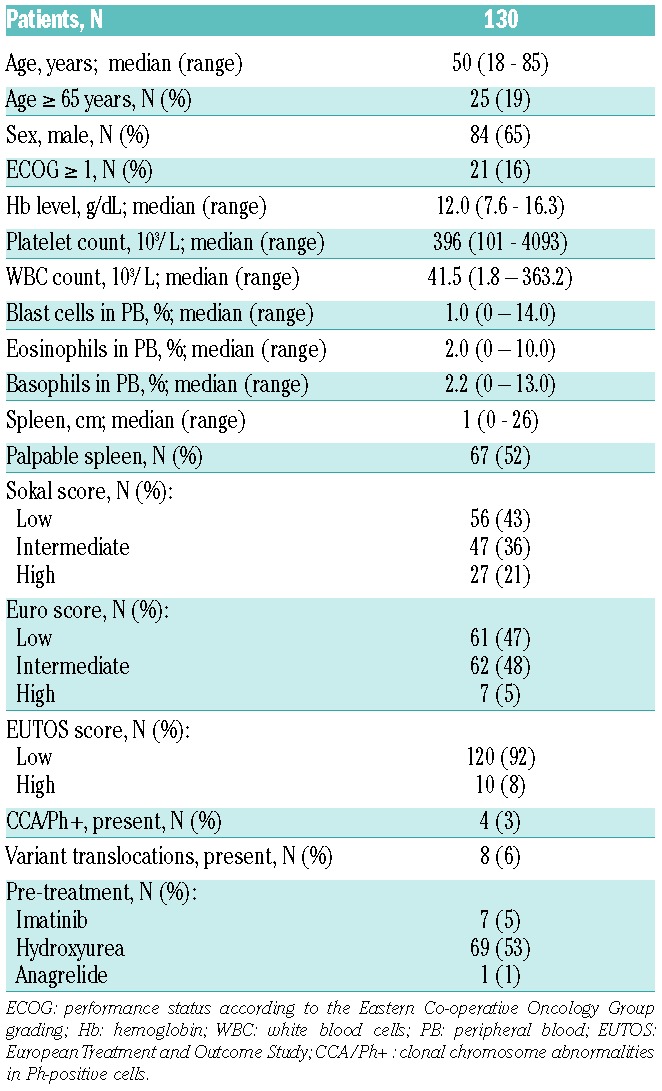
One hundred and thirty patients were enrolled between December 2011 and November 2012 at 32 GIMEMA Clinical Centers. The baseline characteristics of the patients are shown in Table 1. The median age was 50 years. Sixty-five percent were males. High-risk patients were 21% by Sokal, 5% by EURO, and 8% by EUTOS scores. Clonal chromosome abnormalities in Ph+ cells were reported in 3% of patients.
Table 1.
Patient characteristics at diagnosis.
Patient disposition
The median follow-up was 29 months (range 24–37 months). The patient disposition at the last contact is shown in Table 2. Overall, 77% of patients were still on nilotinib (80% at 2 years), mainly at the initial 300 mg TD dose. In 6 patients the nilotinib dose was escalated to 400 mg TD due to the absence of an optimal response: 4 patients are still on treatment, 2 of them with an optimal response and 2 without significant improvements, while 2 patients definitively discontinued nilotinib as a result of treatment failure. Twenty-eight patients permanently discontinued nilotinib, of whom 11 (8%) were due to failure. Four of these patients progressed to AP or BP after 1, 4, 6, and 19 months, respectively; all these patients were alive at last contact. One of these patients, a 41 year old with an patients underwent alloSCT, 2 after transformation to AP (previously described) and 1 after resistance to all TKIs, including ponatinib, without progression and without detectable BCR-ABL1 mutations.
Table 2.
Patient disposition at last contact.

Responses and outcome
According to the intention-to-treat (ITT) principle, 70% of patients were in CCyR at 6 months, and 77% at 12 months. The 3-month EMR was achieved in 80% of patients (ITT). The rates of MMR, MR4.0, and MR4.5 at 3, 6, 12, 18, and 24 months are shown in Table 3. At 24 months, according to the ITT principle, 65% of patients were in MMR, 46% were in MR4.0, and 17% were in MR4.5. Overall, 75/130 patients (58%) achieved a MR4.0 at least once and 39/75 (52%) achieved a sustained MR4.0; 40/130 patients achieved a MR4.5 and 11/40 (28%) a sustained MR4.5. The cumulative probability of achieving MR4.0 and MR4.5 is shown in Figure 1; after two years of treatment the probabilities were 51% (95% CI, 42–60%) and 24% (95% CI, 16–31%), respectively. The duration of observation is still too short for a detailed analysis of the stability of deep molecular response.
Table 3.
Molecular response at milestones.
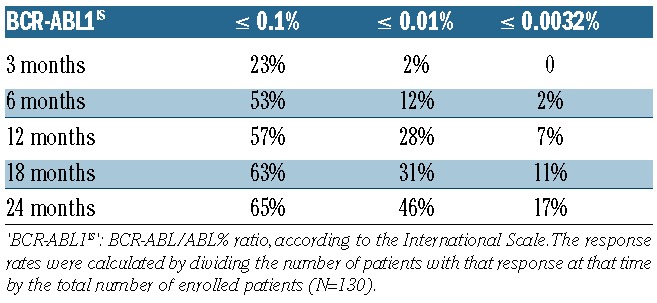
Figure 1.
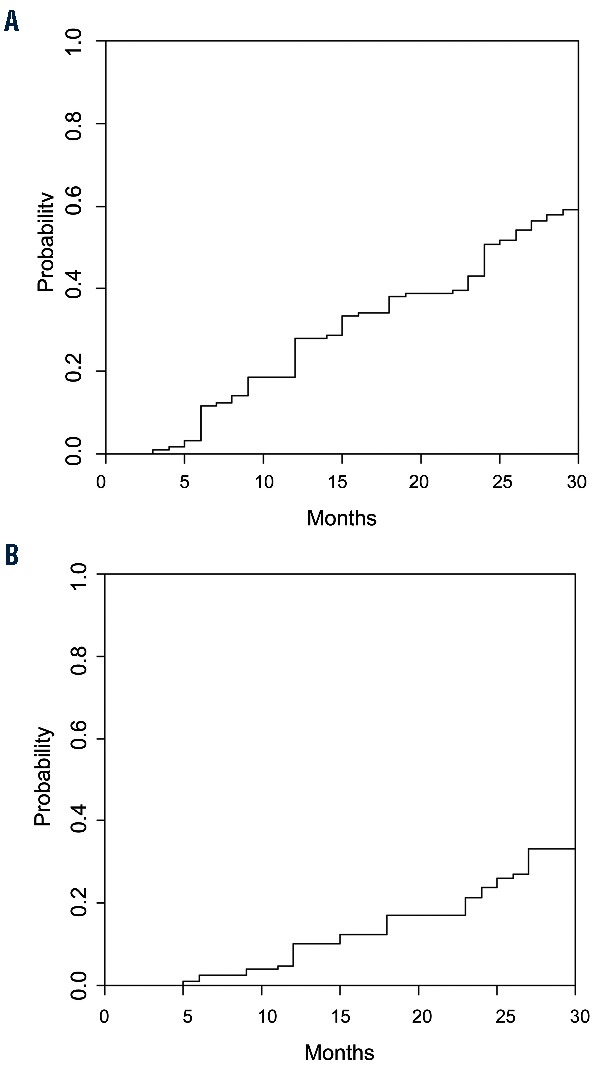
Cumulative incidence of deep molecular response. (A) MR4.0: the 2-year estimated cumulative incidence of MR4.0 was 51% (95% CI, 42–60%), B) MR4.5: the 2-year estimated cumulative incidence of MR4.5 was 24% (95% CI, 16–31%). The cumulative probability of achieving a response was calculated under consideration of competing risks, defined as failure followed by treatment change, progression or death.
Only 1 patient died, due to the worsening of a pre-existing comorbidity (chronic obstructive pulmonary disease: a worsening of general clinical conditions, followed by a switch to imatinib with a stable response, was observed). As shown in Figure 2, the 30-month OS was 99% (95% CI 91–100%), the 30-month PFS was 96% (95% CI 89–98%) and the 30-month EFS (survival without treatment discontinuation, except for treatment-free remission) was 76% (95% CI 67–83%).
Figure 2.
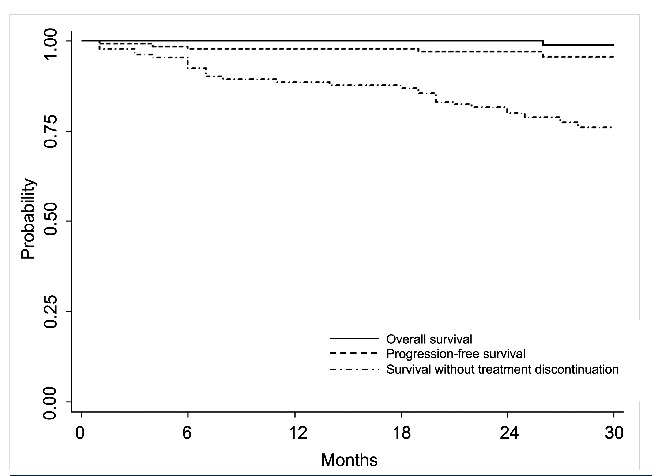
Outcome of all the 130 enrolled patients. The estimated 30-month overall survival was 99% (95% CI, 91–100%), the 30-month estimated progression-free survival was 96% (95% CI, 89–98%), the estimated 30-month survival without treatment discontinuation was 76% (95% CI, 67–83%).
Safety
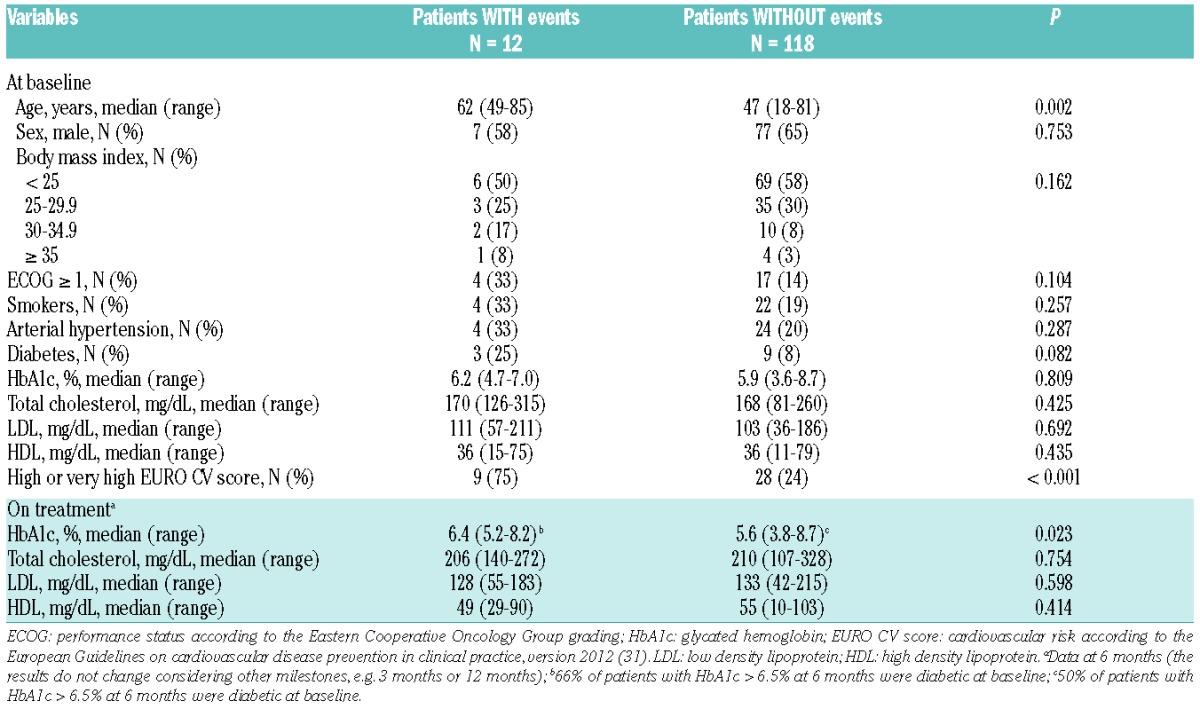
A grade 3–4 thrombocytopenia and neutropenia were recorded in 8% and 9% of patients. Hematologic AEs caused early permanent treatment discontinuation in 2 patients. Twenty-five AEs listed under a comprehensive definition of cardiovascular AEs (CVAEs) were reported in 21 patients (16%): arterial thrombosis, 13 events (Table 4); venous thrombosis, 4 events (1 deep venous thrombosis, 3 superficial thrombophlebitis); QTc prolongation, 3 events (only 1 case > 500 msec); arrhythmias, 3 events (2 atrial fibrillations, 1 atrial-ventricular blockade); congestive heart failure, 1 event; acute pericarditis, 1 event. They were reported as a grade 3 event in nine cases, and as a grade 4 event in one case. The treatment was temporarily discontinued for 9 events in 8 patients (36% of CVAEs, 6% of all patients), and it was permanently discontinued for 8 events (32% of CVAEs, 6% of all patients). A medical treatment without hospitalization was administered for 13 events; hospitalization was required for 8 events. Major surgery was performed in 2 patients: substitution of the femoral head and amputation of the right lower limb, respectively. One case of myocardial infarction was treated with coronary stents. No patient died of toxicity. The characteristics of patients with (N = 12) or without (N = 118) arterial thrombotic events are shown in Table 5. The patients with high or very high cardiovascular risk according to the European Guidelines on cardiovascular disease prevention in clinical practice,29 retrospectively assessed, had a significantly higher probability of arterial thrombotic events (Online Supplementary Figure S1). Among the other non-hematologic and non-cardiovascular AEs, only fatigue (17% grade 1–2 and 1% grade 3), bone and muscle and joint pain (22% grade 1–2 and 1% grade 3), and skin rash (29% grade 1–2 and 1% grade 3) were reported in more than 10% of patients. Grade 3–4 laboratory abnormalities were as follows: grade 3 transaminase increase 2% (permanent treatment discontinuation, 1 case), grade 3 bilirubin increase 5%, grade 3 and grade 4 lipase increase 12% and 2%, respectively, and grade 3 amylase increase 1% (no pancreatitis).
Table 4.
List of arterial thrombotic adverse events by year, all grades, irrespective of causality.
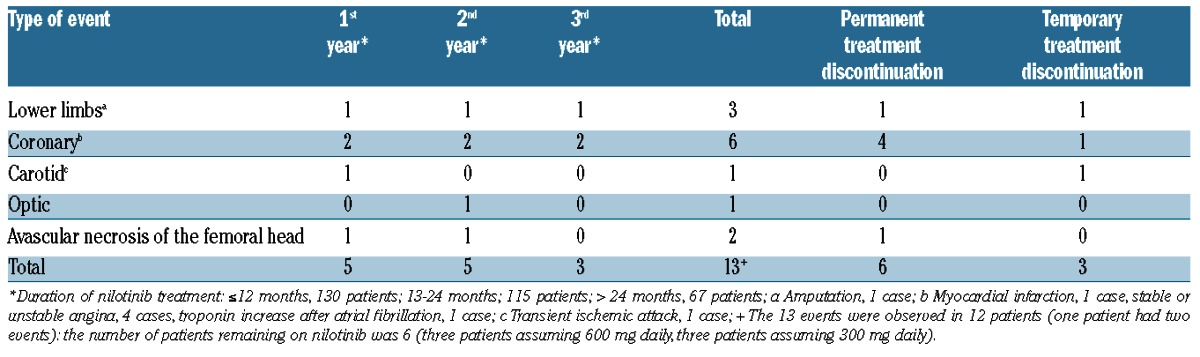
Table 5.
Characteristics of patients with and without arterial thrombotic adverse events.
According to adapted ADA criteria, and considering the maximum grade reached by each patient while on study, 47%, 11%, 5% and 6% of patients experienced a grade 1 (101–125 mg/dl), grade 2 (126–150 mg/dl), grade 3 (151–200 mg/dl) and grade 4 (>200 mg/dl) hyperglycemia, respectively; 29% of patients had an increase of fasting glucose at 1 year, compared to baseline levels (P<0.001). According to adapted ADA criteria, 47% of patients had a grade 1 (5.7–6.4%), 10% a grade 2 (6.5–6.9%), 3% a grade 3 (7–7.9%) and 5% a grade 4 (≥8%) glycated hemoglobin (HbA1c), respectively, (maximum grade reached on our study); no significant increase of glycated hemoglobin has been observed from baseline. According to the AACE criteria, 40 patients (31%) experienced a borderline (200–239 mg/dL) and 54 (42%) a high-risk (≥240 mg/dL) hypercholesterolemia (maximum grade reached on our study). A significant increase of cholesterol, both in LDL and HDL fractions (P<0.001), and a significant reduction of triglycerides (P<0.001) were detected at 1 year from baseline. The serum glucose, HbA1c and lipid concentrations at each milestone are shown in Figure 3 and Online Supplementary Table S3.
Figure 3.
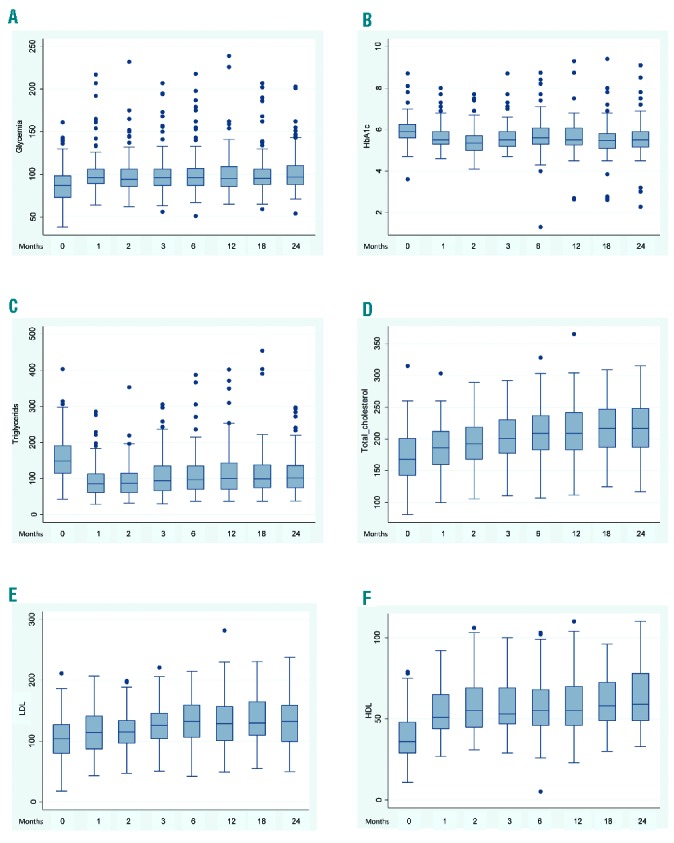
Metabolic effects of nilotinib by time. (A) Distribution of fasting glucose at milestones; (B) Distribution of glycated hemoglobin at milestones; (C) Distribution of triglycerides at milestones; (D) Distribution of total cholesterol at milestones; (E) Distribution of low density lipoprotein at milestones; (F) Distribution of high density lipoprotein at milestones.
Discussion
The introduction and the extended clinical use of second generation TKIs is becoming a very important issue in first-line therapy for CML.2–4,10,30–38 They offer a treatment choice that must be weighed for short- and long-term efficacy and toxicity, and for cost-efficacy.16,39,40 The information on nilotinib is limited to data coming from two company-sponsored studies, of which one was designed to compare nilotinib and imatinib, and the other to confirm the rate of deep molecular response on nilotinib.2–4,10 There are no data from independent, investigator-sponsored, studies. This GIMEMA trial was made possible thanks to the support of Novartis Oncology Italy, who provided the drug free of charge and a small unrestricted support. The study was designed, conducted and analyzed by GIMEMA, so that this is the first study providing company-independent data on the treatment of newly diagnosed CP CML patients with nilotinib 300 mg TD. The study has some strengths and some limitations. The strengths are the independence and the involvement of several clinical centers all over Italy. The major limitation is the short time of observation, with a minimum of 2 years, a median of 2.5 years, and a maximum of 3 years. The ENESTnd and the ENEST1st trials were reported with a minimum observation period of 6 and 2 years, respectively.4,10
Two major issues are important in the treatment of CML. One issue is the rapidity31,41–44 and the depth45 of the molecular response. We found that EMR was achieved less frequently than in both ENEST trials, but that MMR (MR3.0), MR4.0 and MR4.5 rates were in the same range of ENEST1st, and even higher than in ENESTnd (Online Supplementary Table S4).2–4,10 The significance of these differences cannot be assessed because the three studies are different, with different age distribution and proportion of high-risk (Sokal) patients (28% in ENESTnd, 18% in ENEST1st, 21% in this study), with different enrolment criteria and different guidelines for dose reduction or treatment discontinuation.
It should be noted that the molecular response rates have been calculated in two ways and reported as response rates “at” and “by” different time points, where the rate “at” the time point gives the actual proportion of patients who are in that response at the given time point, and the rate “by” the same time point gives the cumulative proportion of patients achieving the response at least once before the given time point. The estimated cumulative incidence of response (response “by”) helps to make a comparison between two treatments, as in the ENESTnd study,2–4 but overestimates the actual proportion (response “at”) of the patients who are in that response at that time, which is important for clinical decisions. The response rates “at” each time point are frequently lower than the values “by” the same time points.
The second major issue is the so-called cardiovascular toxicity, that includes different events, with different physiopathologic mechanisms and different clinical relevance: myocardial infarction, atrial fibrillation, superficial thrombophlebitis, arterial thrombosis, congestive heart failure, stroke, and many others. The incidence, the severity and the consequences of these complications are difficult to assess and to compare, because they may depend on different variables, including not only the patients characteristics, the baseline cardiovascular risk, the prior treatments and the drug dose,46–48 but also the definition of the events, and, importantly, the accuracy of the event reports, that depends on the retrospective or prospective nature of the data collection. When the GIMEMA study was designed, the cardiovascular toxicity was not yet pointed out, apart from QTc prolongation, and the cardiovascular risk at baseline was not routinely assessed. However, the cardiovascular toxicity was revealed as soon as patient enrolment began, so that the identification and the reporting of CVAEs, in facts, became prospective. However, monitoring, prophylaxis, and the treatment of CVAEs were left to local investigators, because it was not possible to provide guidelines. Several reports indicated a possible metabolic non-target effect of nilotinib, potentially related to CVAEs; importantly, in our study, fasting glucose, glycated hemoglobin and serum lipids were prospectively assessed. Moreover, to evaluate the clinical impact of metabolic effects, we decided to classify the abnormalities according to specific criteria, as recommended by ADA and AACE guidelines.27,28
With these caveats, it is possible to describe, but not to compare, the 2-year incidence of major CVAEs in the present trial and in the ENEST1st one:10 ischemic heart events were 4.6% and 3.4% respectively; arterial thrombotic events were 4.6% (including one case of retinal artery occlusion and two cases of avascular necrosis of the femoral head) and 1.9%, respectively; arrhythmias were 2.3% and 0.7%, respectively; congestive heart failure was reported in 0.8% and 0.3%, respectively. The incidence of QTc prolongation (2.3% in the GIMEMA study) and of venous thrombosis (3.1%) was not reported in the ENEST1st study. With a median follow-up of 29 months, the number of reported arterial thrombotic events was higher during the first and the second year, if compared to the third year of treatment, but considering the number of patients on nilotinib treatment, the yearly incidence was comparable (Table 4). A linear increase of the cumulative incidence of CVAEs over time was also described in the 5-year update of the ENESTnd trial; the yearly incidence of CVAE continues unabated after 5 years and may even increase.3 In our study the cumulative probability of developing a CVAE was 7 % (95% CI, 4–13%) at 1 year and 13 % (95% CI, 8–20%) at 2 years (data not shown). We confirmed a significant increase of fasting glucose level during nilotinib treatment, but we were not able to demonstrate any significant increase of glycated hemoglobin. Similar results were reported in the ENESTnd trial, in a sub-analysis including only patients with normal glycemic status at baseline:49 the majority of patients with hyperglycemia did not meet the glycated hemoglobin criteria for diabetes. The patients with arterial thrombotic events had a higher incidence of cardiovascular risk factors at baseline (in particular, a higher incidence of diabetes was observed), and were elderly (Table 5, Online Supplementary Figure S1). The exact pathogenesis of fasting glucose alterations during nilotinib is still controversial and probably related to insulin resistance: both in the ENESTnd study49 and in the ENIGMA 2 study50 an increase in insulin production and a decrease of fasting C-peptide were observed, with increased levels of HOMA-IR and HOMA-β values.
In conclusion, this independent study highlights the therapeutic efficacy of nilotinib, confirming the rates, the velocity, and the depth of molecular response; moreover, it confirms that the risk of cardiovascular toxicity, including several different events, is higher in patients with high cardiovascular risk, requiring specific measures of prophylaxis and monitoring.
Acknowledgments
The authors would like to thank the valuable assistance of Miriam Fogli and Michela Apolinari. The following members of the ‘GIMEMA Working Party on CML’ actively participated in this study, enrolling patients and collecting clinical data: Rupoli S, Scortechini AR (Hematology Department, University of Ancona, Azienda Ospedaliero Universitaria Ospedali Riuniti di Ancona, Ancona); Cantore N, Palmieri F (Hematology Division, Ospedale Civile ‘San Giuseppe Moscati’, Avellino); Luatti S, Testoni N (Institute of Hematology ‘Seràgnoli’, Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, Bologna); Rossi G, Giuliani G (Hematology Unit, Azienda Ospedaliera ‘Spedali Civili’, Brescia); Di Raimondo F, Vigneri P (Hematology Unit, ‘Ferrarotto’ Hospital, Catania); Molica S, Lentini M (Hematology Unit, ‘Pugliese’ Hospital, Catanzaro); Cuneo A, Cavazzini F (Chair of Hematology, Dipartimento di Scienze Mediche, ‘Arcispedale S Anna’ University Hospital, Ferrara); Spinosa G, Palumbo G (Hematology Unit, Azienda Ospedaliero-Universitaria Ospedali Riuniti, Foggia); Ibatici A, Beltrami G (Hematology I Unit, IRCCS AOU San Martino-IST, Genova); Pierri I, Bergamaschi M (Clinical Hematology Unit, IRCCS AOU San Martino-IST, Genova); Ciceri F, Lunghi F (Hematology Unit, “San Raffaele” University Hospital, Milano); Bassan R, Maino E (Hematology Unit, Ospedale dell’Angelo, Mestre, VE); Luppi M, Marasca R (Chair of Hematology, University of Modena and Reggio Emilia, Modena); Semenzato G, Cason G (Department of Internal Medicine, University of Padova, Padova); Fabbiano F, Turri D (Hematology Unit, ‘V Cervello’ Hospital, Palermo); Isidori A, Barulli S (Hematology Unit, ‘San Salvatore’ Hospital, Pesaro); Vallisa D, Arcari A (Hematology Division, ‘Guglielmo da Saliceto’ Hospital, Piacenza); Zaccaria A, Zuffa E (Hematology Unit, ‘Santa Maria delle Croci’ Hospital, Ravenna); Ronco F, Ielo D (Hematology Unit, Ospedali Riuniti, Reggio Calabria); Merli F, Capodanno I (Hematology Unit, Arcispedale Santa Maria Nuova, Reggio Emilia); Tosi P, Merli A (Hematology Unit, Ospedale Infermi Azienda Unità Sanitaria, Rimini); Musto P, Pietrantuono G (Hematology Unit, IRCCS Centro di Riferimento Oncologico della Basilicata, Rionero in Vulture, PZ); Latagliata R (Chair of Hematology, ‘La Sapienza’ University, Roma); De Fabritiis P, Trawiska M (Hematology Unit, ‘S. Eugenio’ Hospital, Roma); Amadori S, Cantonetti M (Department of Hematology, ‘Tor Vergata’ University, Roma); Ronci B, Cedrone M (Hematology Unit, Ente Ospedaliero San Giovanni Addolorata, Roma); Falcone AP, Sgherza N (Hematology Unit, Casa Sollievo della Sofferenza, San Giovanni Rotondo, FG); Bocchia M, Defina M (Chair of Hematology, University of Siena, Siena); Vitolo U, Pregno P (Hematology Unit, Azienda Ospedaliero Universitaria Città della Salute e della Scienza, University of Torino, Torino); Gherlinzoni F, Calistri E (Hematology Unit, ‘Ca’ Foncello’ Hospital, Treviso); Fanin R, Medeot M (Chair of Hematology, University of Udine, Udine); Pizzolo G, Bonifacio M (Chair of Hematology, University of Verona, Verona, Italy).
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/101/10/1200
References
- 1.Weisberg E, Manley PW, Breitenstein W, et al. Characterization of AMN107, a selective inhibitor of native and mutant Bcr-Abl. Cancer Cell. 2005;7(2):129–141. [DOI] [PubMed] [Google Scholar]
- 2.Saglio G, Kim DW, Issaragrisil S, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362(24):2251–2259. [DOI] [PubMed] [Google Scholar]
- 3.Hochhaus A, Saglio G, Hughes TP, et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia. 2016;30(5):1044–1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Larson R, Kim D, Issaragrisil S, et al. Efficacy and Safety of Nilotinib (NIL) vs Imatinib (IM) in Patients (pts) With Newly Diagnosed Chronic Myeloid Leukemia in Chronic Phase (CML-CP): Long-Term Follow-Up of ENESTnd [abstract]. Blood. 2014;124(21). Abstract 4541. [Google Scholar]
- 5.Aichberger KJ1, Herndlhofer S, Schernthaner GH, et al. Progressive peripheral arterial occlusive disease and other vascular events during nilotinib therapy in CML. Am J Hematol. 2011;86(7):533–539. [DOI] [PubMed] [Google Scholar]
- 6.Le Coutre P, Rea D, Abruzzese E, et al. Severe peripheral arterial disease during nilotinib therapy. J Natl Cancer Inst. 2011;103(17):1347–1348. [DOI] [PubMed] [Google Scholar]
- 7.Giles FJ, Mauro MJ, Hong F, et al. Rates of peripheral arterial occlusive disease in patients with chronic myeloid leukemia in the chronic phase treated with imatinib, nilotinib, or non-tyrosine kinase therapy: a retrospective cohort analysis. Leukemia. 2013;27(6):1310–1315. [DOI] [PubMed] [Google Scholar]
- 8.Kim TD, Rea D, Schwarz M, et al. Peripheral artery occlusive disease in chronic phase chronic myeloid leukemia patients treated with nilotinib or imatinib. Leukemia. 2013;27(6):1316–1321. [DOI] [PubMed] [Google Scholar]
- 9.Valent P, Hadzijusufovic E, Schernthaner GH, Wolf D, Rea D, le Coutre P. Vascular safety issues in CML patients treated with BCR/ABL1 kinase inhibitors. Blood. 2015;125(6):901–906. [DOI] [PubMed] [Google Scholar]
- 10.Hochhaus A, Rosti G, Cross NC, et al. Frontline nilotinib in patients with chronic myeloid leukemia in chronic phase: results from the European ENEST1st study. Leukemia. 2016;30(1):57–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kantarjian HM, Giles F, Gattermann N, et al. Nilotinib (formerly AMN107), a highly selective BCR-ABL tyrosine kinase inhibitor, is effective in patients with Philadelphia chromosome-positive chronic myelogenous leukemia in chronic phase following imatinib resistance and intolerance. Blood. 2007;110(10):3540–3546. [DOI] [PubMed] [Google Scholar]
- 12.Rosti G, Palandri F, Castagnetti F, et al. Nilotinib for the frontline treatment of Ph(+) chronic myeloid leukemia. Blood. 2009;114(24):4933–4938. [DOI] [PubMed] [Google Scholar]
- 13.Gugliotta G, Castagnetti F, Breccia M, et al. Long-term outcome of a phase 2 trial with nilotinib 400 mg twice daily in first-line treatment of chronic myeloid leukemia. Haematologica. 2015;100(9):1146–1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cortes JE, Jones D, O’Brien S, et al. Nilotinib as front-line treatment for patients with chronic myeloid leukemia in early chronic phase. J Clin Oncol. 2010;28(3):392–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Baccarani M, Cortes J, Pane F, et al. Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol. 2009;27(35):6041–6051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Baccarani M, Deininger MW, Rosti G, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood. 2013;122(6):872–884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sokal JE, Cox EB, Baccarani M, et al. Prognostic discrimination in ‘good-risk’ chronic granulocytic leukemia. Blood. 1984;63(4):789–799. [PubMed] [Google Scholar]
- 18.Hasford J, Pfirrmann M, Hehlmann R, et al. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. J Natl Cancer Inst. 1998;90(11):850–858. [DOI] [PubMed] [Google Scholar]
- 19.Hasford J, Baccarani M, Hoffmann V, et al. Predicting complete cytogenetic response and subsequent progression-free survival in 2060 patients with CML on imatinib treatment: the EUTOS score. Blood. 2011;118(3):686–692. [DOI] [PubMed] [Google Scholar]
- 20.Hughes T, Deininger M, Hochhaus A, et al. Monitoring CML patients responding to treatment with tyrosine kinase inhibitors: review and recommendations for harmonizing current methodology for detecting BCR-ABL transcripts and kinase domain mutations and for expressing results. Blood. 2006;108(1):28–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cross NC, White HE, Muller MC, Saglio G, Hochhaus A. Standardized definitions of molecular response in chronic myeloid leukemia. Leukemia. 2012;26(10):2172–2175. [DOI] [PubMed] [Google Scholar]
- 22.Cross NC, White HE, Colomer D, et al. Laboratory recommendations for scoring deep molecular responses following treatment for chronic myeloid leukemia. Leukemia. 2015;29(5):999–1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Soverini S, Hochhaus A, Nicolini FE, et al. BCR-ABL kinase domain mutation analysis in chronic myeloid leukemia patients treated with tyrosine kinase inhibitors: recommendations from an expert panel on behalf of European LeukemiaNet. Blood. 2011;118(5): 1208–1215. [DOI] [PubMed] [Google Scholar]
- 24.Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–481. [Google Scholar]
- 25.Pfirrmann M, Hochhaus A, Lauseker M, Saussele S, Hehlmann R, Hasford J. Recommendations to meet statistical challenges arising from endpoints beyond overall survival in clinical trials on chronic myeloid leukemia. Leukemia. 2011;25(9):1433–1438. [DOI] [PubMed] [Google Scholar]
- 26.Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competiting risks: new representations of old estimators. Stat Med. 1999;18(6):695–706. [DOI] [PubMed] [Google Scholar]
- 27.Mechanick JI, Camacho PM, Garber AJ, et al. American association of clinical endocrinologists and american college of endocrinology protocol for standardized production of clinical practice guidelines, algorithms and checklists-2014 update and the AACE G4G program. Endocrine Practice. 2014;20(7):692–702. [DOI] [PubMed] [Google Scholar]
- 28.American Diabetes Association. Classification and diagnosis of diabetes. Diabetes Care. 2015;38 Suppl:S8–S16. [DOI] [PubMed] [Google Scholar]
- 29.Perk J, De Backer G, Gohlke H, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J. 2012;33(13):1635–1701. [DOI] [PubMed] [Google Scholar]
- 30.Kantarjian H, Shah NP, Hochhaus A, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362(24):2260–2270. [DOI] [PubMed] [Google Scholar]
- 31.Jabbour E, Kantarjian HM, Saglio G, et al. Early response with dasatinib or imatinib in chronic myeloid leukemia: 3-year follow-up from a randomized phase 3 trial (DASISION). Blood. 2014;123(4):494–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cortes J, Saglio G, Kantarjian HM, et al. Final 5-Year Study Results of DASISION: The Dasatinib Versus Imatinib Study in Treatment-Naïve Chronic Myeloid Leukemia Patients Trial. J Clin Oncol. 2016. May 23, DOI 10.1200/JCO.2015.64.8899 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cortes JE, Kim DW, Kantarjian HM, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: results from the BELA trial. J Clin Oncol. 2012;30(28):3486–3492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Brümmendorf TH, Cortes JE, de Souza CA, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukaemia: results from the 24-month follow-up of the BELA trial. Br J Haematol. 2015;168(1):69–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lipton JH, Chuah C, Guerci-Bresler A, et al. Ponatinib versus imatinib for newly diagnosed chronic myeloid leukaemia: an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2016. April 12, DOI 10.1016/S1470-2045(16)00080-2 [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 36.Jain P, Kantarjian H, Jabbour E, et al. Ponatinib as first-line treatment for patients with chronic myeloid leukaemia in chronic phase: a phase 2 study. Lancet Haematol. 2015;2(9):e376–e383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hoffmann VS, Baccarani M, Hasford J, et al. The EUTOS population-based registry: incidence and clinical characteristics of 2904 CML patients in 20 European Countries. Leukemia. 2015;29(6):1336–1343. [DOI] [PubMed] [Google Scholar]
- 38.Castagnetti F, Gugliotta G, Breccia M, et al. Long-term outcome of chronic myeloid leukemia patients treated frontline with imatinib. Leukemia. 2015;29(9):1823–1831. [DOI] [PubMed] [Google Scholar]
- 39.Experts in Chronic Myeloid Leukemia. The price of drugs for chronic myeloid leukemia (CML) is a reflection of the unsustainable prices of cancer drugs: from the perspective of a large group of CML experts. Blood. 2013;121(22):4439–4442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.O’Brien S, Radich JP, Abboud CN, et al. Chronic myelogenous leukemia, version 1.2015. J Natl Compr Canc Netw. 2014;12(11):1590–1610. [DOI] [PubMed] [Google Scholar]
- 41.Marin D, Ibrahim AR, Lucas C, et al. Assessment of BCR-ABL1 Transcript Levels at 3 Months Is the Only Requirement for Predicting Outcome for Patients With Chronic Myeloid Leukemia Treated With Tyrosine Kinase Inhibitors. J Clin Oncol. 2012;30(3):232–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hanfstein B, Muller MC, Hehlmann R, et al. Early molecular and cytogenetic response is predictive for long-term progression-free and overall survival in chronic myeloid leukemia (CML). Leukemia. 2012;26(9): 2096–2102. [DOI] [PubMed] [Google Scholar]
- 43.Jain P, Kantarjian H, Nazha A, et al. Early responses predict better outcomes in patients with newly diagnosed chronic myeloid leukemia: results with four tyrosine kinase inhibitor modalities. Blood. 2013;121(24):4867–4874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hughes TP, Saglio G, Kantarjian HM, et al. Early molecular response predicts outcomes in patients with chronic myeloid leukemia in chronic phase treated with frontline nilotinib or imatinib. Blood. 2014;123(9):1353–1360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Hehlmann R, Muller MC, Lauseker M, et al. Deep molecular response is reached by the majority of patients treated with imatinib, predicts survival, and is achieved more quickly by optimized high-dose imatinib: results from the randomized CML-study IV. J Clin Oncol. 2014;32(5):415–423. [DOI] [PubMed] [Google Scholar]
- 46.Moslehi JJ, Deininger M. Tyrosine Kinase Inhibitor-Associated Cardiovascular Toxicity in Chronic Myeloid Leukemia. J Clin Oncol. 2015;33(35):4210–4218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Valent P, Hadzijusufovic E, Schernthaner GH, Wolf D, Rea D, le Coutre P. Vascular safety issues in CML patients treated with BCR/ABL1 kinase inhibitors. Blood. 2015;125(6):901–906. [DOI] [PubMed] [Google Scholar]
- 48.Rea D, Mirault T, Cluzeau T, et al. Early onset hypercholesterolemia induced by the 2nd-generation tyrosine kinase inhibitor nilotinib in patients with chronic phase-chronic myeloid leukemia. Haematologica 2014;99(7):1197–1203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Rea D, Gautier JF, Breccia M, et al. Incidence of hyperglycemia by 3 years in patients with newly diagnosed chronic myeloid leukemia in chronic phase treated with nilotinib or imatinib in ENESTnd. Blood. 2012;120(21). Abstract 1686. [Google Scholar]
- 50.Zdenek R, Belohlavkova P, Cetkovsky P, et al. Comparison of Glucose and Lipid Metabolism Abnormality during Nilotinib, Imatinib and Dasatinib Therapy - Results of Enigma 2 Study. Blood. 2014;124(21). Abstract 1813. [Google Scholar]