

Abstract
The distribution of non-Hodgkin lymphoma subtypes varies around the world, but a large systematic comparative study has never been done. In this study, we evaluated the clinical features and relative frequencies of non-Hodgkin lymphoma subtypes in five developing regions of the world and compared the findings to the developed world. Five expert hematopathologists classified 4848 consecutive cases of lymphoma from 26 centers in 24 countries using the World Health Organization classification, and 4539 (93.6%) were confirmed to be non-Hodgkin lymphoma, with a significantly greater number of males than females in the developing regions compared to the developed world (P<0.05). The median age at diagnosis was significantly lower for both low- and high-grade B-cell lymphoma in the developing regions. The developing regions had a significantly lower frequency of B-cell lymphoma (86.6%) and a higher frequency of T- and natural killer-cell lymphoma (13.4%) compared to the developed world (90.7% and 9.3%, respectively). Also, the developing regions had significantly more cases of high-grade B-cell lymphoma (59.6%) and fewer cases of low-grade B-cell lymphoma (22.7%) compared to the developed world (39.2% and 32.7%, respectively). Among the B-cell lymphomas, diffuse large B-cell lymphoma was the most common subtype (42.5%) in the developing regions. Burkitt lymphoma (2.2%), precursor B- and T-lymphoblastic leukemia/lymphoma (1.1% and 2.9%, respectively) and extranodal natural killer/T-cell lymphoma (2.2%) were also significantly increased in the developing regions. These findings suggest that differences in etiologic and host risk factors are likely responsible, and more detailed epidemiological studies are needed to better understand these differences.
Introduction
The relative frequencies of various subtypes of non-Hodgkin lymphoma (NHL) vary significantly in different geographic regions of the world,1–7 and environmental and lifestyle factors, as well as host genetic makeup, appear to play an important role in the development of NHL.8–10 The International NHL Classification Project was initiated in 1995 with a goal to investigate the geographic differences in NHL subtype distribution and clinical features.1,2 Between 1995 and 2012, five expert hematopathologists visited 26 sites in 24 countries on five continents (Table 1), and found significant geographic differences in the relative frequencies and clinical features of various NHL subtypes.1–7 The aim of this study was to aggregate this data by region and evaluate the relative frequencies of NHL subtypes in five developing regions of the world. Moreover, we compare the findings in the developing regions to those in the developed world which, to our knowledge, has never been done before.
Table 1.
Geographic regions and sites included in the study.

Methods
International NHL Classification Project
Twenty six institutions form 24 countries in seven regions including North America (NA), Western Europe (WEU), Southeastern Europe (SEEU), Central and South America (CSA), North Africa/the Middle East and India (NAF/ME/IN), Southern Africa (SAF), and the Far East (FE) participated in the study (Table 1). Each institution was instructed to collect 200 consecutive, newly-diagnosed and untreated cases of NHL representative of their local region or country. Leukemias were excluded from the study unless a tissue biopsy other than bone marrow was performed prior to therapy. Approval for this study was obtained from the Institutional Review Board of the University of Nebraska Medical Center and at each of the participating institutions as required by institutional policies. This study was conducted in accordance with the Declaration of Helsinki.
At each site, hematoxylin and eosin-stained slides, immunostains, pathology reports, clinical data, and the results of ancillary studies were organized for review. A panel of five expert hematopathologists (JD, KAM, HKM-H, BNN, and DDW) then reviewed all of the cases using the 2001 World Health Organization classification.3,11 A consensus diagnosis was reached when at least four of the experts agreed on a diagnosis. For cases in which a consensus diagnosis could not be reached, a specific diagnostic algorithm was developed for each case and agreed upon by the experts. Additional requested clinical data and material, either paraffin blocks or unstained slides, were then sent to one of the experts who performed additional ancillary testing (immunostains, in situ stains, molecular studies, etc.) and assigned a consensus diagnosis to each case based on the algorithm.
For this analysis, only information on age and sex is included because the clinical data collected at the various institutions was often incomplete and quite variable. Cases of composite lymphoma were classified according to the low-grade component, and mature B-cell NHL was further subdivided into low-grade (LG) and high-grade (HG) subgroups.3 Due to the small numbers, the rare T-cell subtypes were all grouped together under the category of peripheral T-cell lymphoma, other types. The data from the two developed regions (NA and WEU) were combined and compared to the data from the five developing regions, and the information from each developing region was also compared to the combined data from the other four developing regions.
Statistical analysis
Data analysis was done using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA). Comparisons of medians for continuous variables were conducted using the Wilcoxon rank sum test. Comparisons of categorical variables were done using χ2 or Fisher’s exact tests; the latter was used when the χ2 test may not have been valid due to small numbers. The P-values for pairwise comparisons were adjusted using the Hochberg step-up Bonferroni method, and adjusted P-values of less than 0.05 were considered to be statistically significant.
Results
In this study, a total of 4848 cases were collected for expert review and 4539 (93.6%) were confirmed to be NHL, whereas the other 309 (6.4%) had diagnoses other than NHL and were excluded from further analysis. Among the excluded cases, 89 were Hodgkin lymphomas, 117 had diagnoses other than lymphoma, and 105 were unclassifiable cases. The number of reclassified cases in the developing regions (7.5%) was significantly higher than in the developed world (2.2%; P<0.05).
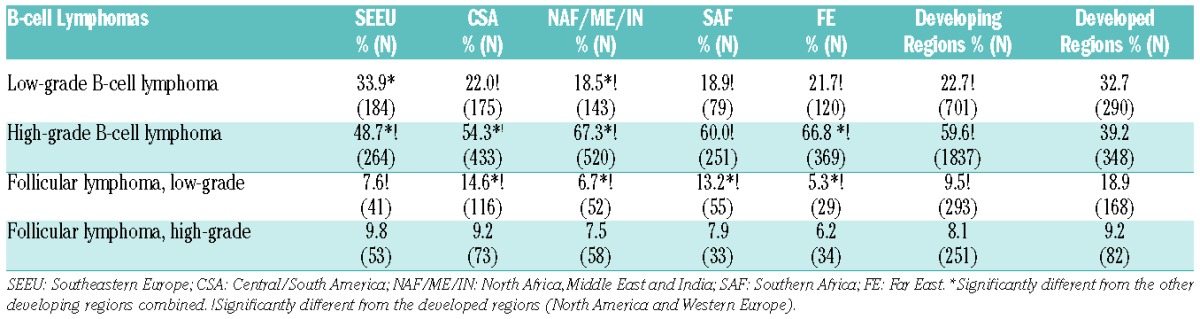
The relative distribution of NHL subtypes in the developing and developed regions are shown in Table 2. Of the 3560 cases in the developing regions, 3082 (86.6%) were B-cell lymphomas and 478 (13.4%) were T- and natural killer (NK)-cell lymphomas. The developing regions had a significantly lower relative frequency of B-NHL and a higher frequency of T- and NK-cell NHL compared to the developed world (90.7% and 9.3%, respectively). Also, the developing regions had a significantly higher relative frequency of HG B-NHL (59.6%) and a lower frequency of LG B-NHL (22.7%) compared to the developed world (39.2% and 32.7%, respectively; Table 3). Comparison of the individual developing regions with the developed world showed that all of the developing regions had higher relative frequencies of HG B-NHL. Moreover, all of the developing regions, except SEEU, had a lower frequency of LG B-NHL compared to the developed world. When compared to the rest of the developing regions, NAF/ME/IN and the FE had higher relative frequencies of HG B-NHL whereas SEEU and CSA had lower frequencies. Southeastern Europe had a significantly higher frequency of LG B-NHL whereas NAF/ME/IN had a lower frequency compared to the rest of the developing world. Cases of pediatric NHL (age <19 years) comprised only 3.3% of the study cases, too few for meaningful analysis, and these are listed in the Online Supplementary Table S1.
Table 2.
Relative frequencies of non-Hodgkin lymphoma subtypes by region.
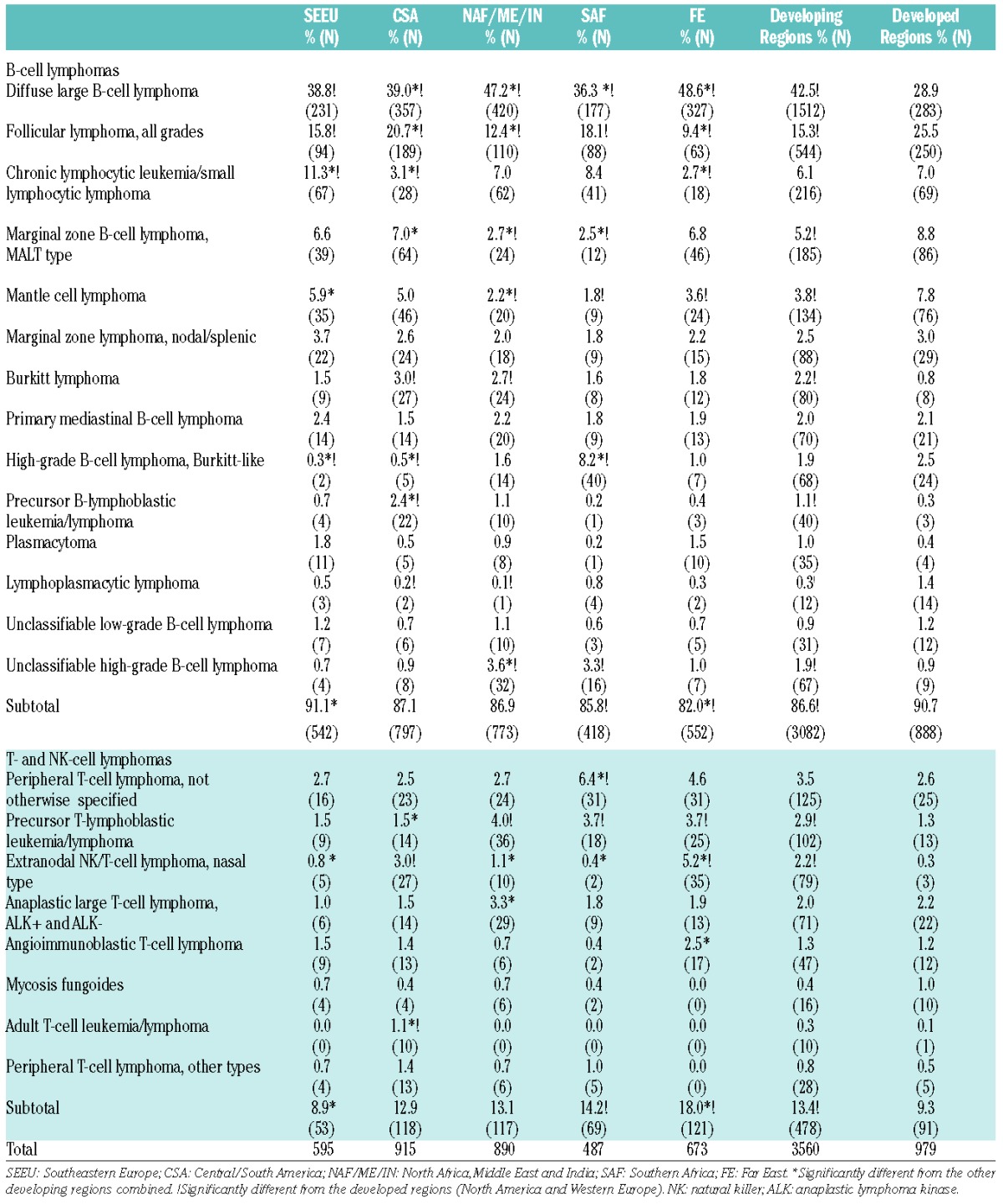
Table 3.
Relative frequencies of mature B-cell non-Hodgkin lymphomas according to grade.
Among B-cell lymphomas (Table 2), diffuse large B-cell lymphoma (DLBCL) was the most common subtype in the developing world (42.5%), as well as in each of the developing regions. Follicular lymphoma (FL) was the second most common subtype in the developing world (15.3%) and was the most common in CSA (20.7%). Among the other B-cell lymphomas, marginal zone lymphoma (MZL) of mucosa-associated lymphoid tissue (MALT) type (7%) was more common in CSA, chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL; 11.3%) and mantle cell lymphoma (MCL; 5.9%) in SEEU, precursor B-lymphoblastic leukemia/lymphoma (2.4%) in CSA, and Burkitt-like lymphoma (8.2%) in SAF.
When individual lymphoma subtypes in the developing regions were compared to the developed world (Table 2), DLBCL (42.5%) was significantly more frequent and FL (15.3%) was less frequent than in the developed world (28.9% and 25.5%, respectively). Furthermore, when FL was separated into LG and HG subtypes (Table 3), the developing regions had a significantly lower relative frequency of LG FL (9.5%) compared to the developed world (18.9%). Analysis of DLBCL and FL frequencies in the individual developing regions (Table 2) showed that all of the regions had higher relative frequencies of DLBCL and lower frequencies of FL compared to the developed world. When compared to the other developing regions, NAF/ME/IN and the FE had significantly higher relative frequencies of DLBCL and lower frequencies of FL. Burkitt lymphoma (2.2%) and precursor B-lymphoblastic leukemia/lymphoma (1.1%) were also significantly more common in the developing regions compared to the developed world (0.8% and 0.3%, respectively). Among the individual regions, CSA and NAF/ME/IN had a significantly higher frequency of Burkitt lymphoma compared to the developed world. Furthermore, CSA had a higher relative frequency of precursor B-lymphoblastic leukemia/lymphoma than the rest of the developing regions or the developed world. The developing regions had significantly lower frequencies of MZL of MALT type (5.2%) and MCL (3.8%) compared to the developed world (8.8% and 7.8%, respectively). The relative frequency of MZL of MALT type was significantly lower in the NAF/ME/IN and SAF compared to the rest of the developing regions. As for MCL, NAF/ME/IN, SAF and the FE had lower relative frequencies compared to the developed world. Southeastern Europe had a higher frequency of CLL/SLL compared to the other developing regions and the developed world. Finally, the developing regions had a higher relative frequency of unclassifiable high-grade B-cell lymphoma (1.9%) compared to the developed world (0.9%), mainly due to increases in NAF/ME/IN and SAF.
Among the T- and NK-cell lymphomas (Table 2), peripheral T-cell lymphoma (PTCL), not otherwise specified, was the most common subtype in SEEU (2.7%) and SAF (6.4%). Extranodal NK/T-cell lymphoma was the most common subtype in CSA (3%) and the FE (5.2%), whereas the most common subtype of PTCL in NAF/ME/IN was anaplastic large T-cell lymphoma. Furthermore, angioimmunoblastic T-cell lymphoma was relatively common in the FE (2.5%), and adult T-cell leukemia/lymphoma was seen only in CSA (1.1%). When compared to the developed world, the developing regions had significantly higher relative frequencies of extranodal NK/T-cell lymphoma (2.2%) and precursor T-lymphoblastic leukemia/lymphoma (2.9%). The rare subtypes and unclassifiable cases of T-cell lymphoma were too few for meaningful analysis and are listed in the Online Supplementary Table S2.
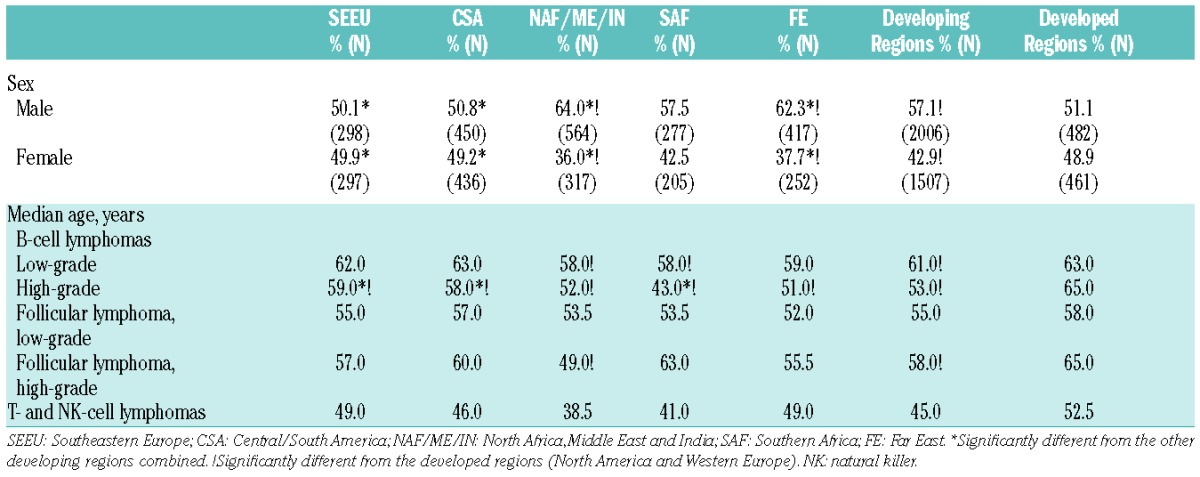
The distribution of NHL by sex and age is shown in Table 4. The ages of patients in the developing regions ranged from less than 1 to 105 years old, and 57.1% were male. In the developed world, the age range was 4 to 100 years old, and 51.1% were male. There was a significantly greater number of males in the developing regions compared to the developed world. When the individual regions were compared to the developed world, NAF/ME/IN and the FE had a significantly greater number of males. The median ages of patients with LG B-NHL (61 years) and HG B-NHL (53 years) were significantly lower in the developing regions than in the developed world (63 and 65 years, respectively). The median age of patients with HG B-NHL was also significantly lower in each of the developing regions compared to the developed world. Furthermore, in NAF/ME/IN and SAF, LG B-NHL patients also had a significantly lower median age compared to the developed world. Among the individual regions, SEEU and CSA had a significantly higher median age for HG B-NHL patients, whereas SAF had a lower median age than the other developing regions. Patients with HG FL in the developing regions also had a significantly lower median age (58 years) than those in the developed world (65 years), whereas there were no differences for LG FL. There were also no significant differences in the median ages of T- and NK-cell NHL patients between the developing and developed world.
Table 4.
Sex distribution and median ages by region for non-Hodgkin lymphoma.
Discussion
This study included 4848 cases initially diagnosed as NHL from 24 countries in the developing and developed world and, to our knowledge, represents the largest epidemiological study of this kind ever done. We found that the developing regions had a significantly higher frequency of misclassified cases (7.5%) than the developed world (2.2%).
The field of lymphoma pathology is challenging and rapidly changing.12 Lymphomas are currently classified according to the 2008 WHO Classification,13 which mandates correlation of the morphological findings with the clinical features and often requires complex ancillary studies to make a diagnosis. In resource-poor countries, pathologists often lack training and experience in hematopathology, as well as the technology to perform the necessary ancillary studies.14,15 Moreover, the developing regions had a higher number of unclassifiable cases, which mainly reflects problems associated with specimen handling and tissue processing that result in poor-quality slides.12 Our findings suggest that training in hematopathology, as well as technical improvements, are needed in the developing world to decrease the number of misdiagnosed cases.
The distribution of NHL subtypes in the five developing regions was markedly different compared to the developed world (Table 2). Overall, the developing regions had a significantly lower relative frequency of B-cell NHL and a higher frequency of T- and NK-cell NHL. Among the B-cell lymphomas, a significantly higher relative frequency of HG B-NHL and a lower frequency of LG B-NHL were observed in the developing regions compared to the developed world. The most common lymphoma in the developing regions was DLBCL, whereas the relative frequency of FL was low. Notably, a high frequency of high-grade Burkitt-like lymphoma was observed in SAF, which is likely due to the human immunodeficiency virus (HIV) epidemic occurring there.16 Other studies from developing countries have reported a similar distribution pattern of B-cell lymphoma, with a high relative frequency of DLBCL and a low frequency of FL.17–20 These differences are likely multifactorial in origin. In North America, whites have the highest incidence of FL of all races.8 Studies that have looked at the incidence of different lymphoma subtypes in foreign-born Asians and Asians born in the United States (US) have shown a higher incidence of FL in US-born Asians, supporting a role for environmental and lifestyle factors in the development of FL.21,22 Among lifestyle factors that have been studied, a high intake of red meat and saturated fat has been associated with an increased risk of FL.23–25 This could explain, at least in part, the high incidence of FL in the developed world since developing countries have lower meat consumption per capita than the developed world.26 Moreover, studies from Japan27 and Taiwan28 have reported a significant increase in the relative frequency of FL in recent times. Therefore, meat and saturated fat consumption may be surrogate markers for western lifestyle. Additional studies are needed to better understand these differences
The developing regions also had higher relative frequencies of other aggressive B-cell lymphomas including Burkitt lymphoma and unclassifiable HG B-NHL, as well as both B- and T-lymphoblastic leukemia/lymphoma. In our study, Burkitt lymphoma was more frequent in all of the developing regions compared to the developed world, but most prominently in CSA and NAF/ME/IN. Burkitt lymphoma has three clinical forms – endemic, immunodeficiency-associated and sporadic forms. Epstein-Barr virus (EBV) infection is implicated in virtually all cases of endemic Burkitt lymphoma, but is also seen in a significant proportion of the other types of Burkitt lymphoma.13 The occurrence of EBV in Burkitt lymphoma is higher in developing countries, where EBV seroconversion occurs at an early age.29 A study of US children found a significantly higher seroprevalence of EBV infection in children of lower socioeconomic status.30 Furthermore, the seroprevalence of EBV infection in Chinese children is higher compared to US children.30,31 These findings may explain, at least in part, the higher frequency of Burkitt lymphoma in the developing regions. Reasons for the higher relative frequency of B- and T-lymphoblastic leukemia/lymphoma in the developing world are unclear. Other studies from developing countries have reported similar findings,32–34 and further large epidemiological studies are needed to better understand these differences.
Our study also found a significantly higher relative frequency of T- and NK-cell lymphomas in the developing regions, with the highest frequencies observed in SAF and the FE. In western countries, T-cell lymphomas account for 5–10% of all NHL, whereas in the Asian countries, 15–20% of all NHL are classified as T- or NK-cell lymphomas.35 In the US, the incidence of PTCL increased by 280% between 1992 and 2005, and the cause for this increase is largely unknown.36 However, pathologists are diagnosing T-cell lymphomas more accurately today due to changes in lymphoma classification over the last 20 years as well as a wider availability of ancillary studies, which could be contributing to the increasing incidence of PTCL. Interestingly, in the US, the incidence of PTCL is the highest in blacks.8,36,37 which could also explain the high incidence of this lymphoma in SAF where most of the patients were black or mixed-race Africans.5 Further large epidemiological and genetic studies are needed to explain these differences.
Extranodal NK/T-cell lymphoma, nasal type, was significantly increased in CSA and the FE in our study. An increased frequency of extranodal NK/T-cell lymphoma in Asia and the native populations of CSA has been well documented.13,19,34 Extranodal NK/T-cell lymphoma has a very strong association with EBV infection and studies suggest that genetics plays a significant role in the development of this lymphoma.8 Asians who live in the US have a significantly increased incidence of this lymphoma compared to other races.8,36,37 Moreover, studies have shown a similar incidence of this lymphoma among US-born and foreign-born Asians.21,38 Our study found that extranodal NK/T-cell lymphoma was particularly increased in the native populations of Guatemala, Chile and Peru, which share a similar genetic background with Asians.3
We also observed a significant difference in the sex distribution of NHL in the developing regions, with a significantly higher number of males compared to the developed world. Even though NHL overall is more common in males,39 there are likely additional factors in the developing world that contribute to the increased number of males. Sex inequality in health care is common in some developing countries. Women may have less access to medical care or may seek medical care less frequently and, therefore, it is possible that lymphomas are underdiagnosed in females in these countries.40,41 Further study is needed to confirm and explain these findings.
The overall median age of LG and HG B-NHL patients in the developing regions was significantly lower than in the developed world. A lower median age for HG B-NHL was seen in all five of the developing regions, and NAF/ME/IN and SAF also had a significantly lower median age for LG B-NHL patients. Other studies from the developing world have also reported lower median ages in B-NHL patients.19,20,34,42 Our finding that B-NHL occurs at an earlier age seems to correlate with a lower gross domestic product in the developing world,43 and suggests that socioeconomic factors may play a role in lymphomagenesis. The much lower median age of patients with HG B-NHL observed in SAF can be attributed to HIV infection, which predominantly affects young blacks.44
In conclusion, this study is the largest systematic study of the distribution of NHL subtypes in the developing world, and the first to compare its findings to the developed world. Our data from the developed world is very similar to data recently reported from the National Cancer Database in the United States.45 We were unable to calculate the incidence rates of the different NHL subtypes in the developing regions due to the lack of centralized and comprehensive population-based cancer registries in many of the countries. However, we did find significant differences in the relative frequencies of many NHL subtypes between the developing and developed world, as well as differences in age and sex. The reasons for these differences are likely multifactorial, and large epidemiological studies are needed to confirm and better explain our findings.
Acknowledgments
We wish to thank all of the clinicians and pathologists who participated in this study (Online Supplementary Table S3).
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/101/10/1244
References
- 1.A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. The Non-Hodgkin’s Lymphoma Classification Project. Blood. 1997;89(11):3909–3918. [PubMed] [Google Scholar]
- 2.Anderson JR, Armitage JO, Weisenburger DD. Epidemiology of the non-Hodgkin’s lymphomas: distributions of the major subtypes differ by geographic locations. Non-Hodgkin’s Lymphoma Classification Project. Ann Oncol. 1998;9(7):717–720. [DOI] [PubMed] [Google Scholar]
- 3.Laurini JA, Perry AM, Boilesen E, et al. Classification of non-Hodgkin lymphoma in Central and South America: a review of 1028 cases. Blood. 2012;120(24):4795–4801. [DOI] [PubMed] [Google Scholar]
- 4.Dotlic S, Perry AM, Petrusevska G, et al. Classification of non-Hodgkin lymphoma in South-eastern Europe: review of 632 cases from the International non-Hodgkin Lymphoma Classification Project. Br J Haematol. 2015;171(3):366–372. [DOI] [PubMed] [Google Scholar]
- 5.Perry AM, Perner Y, Diebold J, et al. Non-Hodgkin lymphoma in Southern Africa: review of 487 cases from the International Non-Hodgkin Lymphoma Classification Project. Br J Haematol. 2016;172(5):716–723. [DOI] [PubMed] [Google Scholar]
- 6.Perry AM, Diebold J, Nathwani BN, et al. Relative frequency of non-Hodgkin lymphoma subtypes in selected centres in North Africa, the Middle East and India: a review of 971 cases. Br J Haematol. 2015;172(5):699–708. [DOI] [PubMed] [Google Scholar]
- 7.Perry AM, Diebold J, Nathwani BN, et al. Non-Hodgkin lymphoma in the Far East: review of 730 cases from the International non-Hodgkin Lymphoma Classification Project. Ann Hematol. 2016;95(2):245–251. [DOI] [PubMed] [Google Scholar]
- 8.Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, 1992–2001. Blood. 2006;107(1):265–276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cerhan JR, Linet MS, Maskarinec G, et al., ed. Medical history, lifestyle, family history, and occupational risk factors for non-Hodgkin lymphoma subtypes: pooled analysis from the International Lymphoma Epidemiology Consortium. J Natl Cancer Inst Monogr. 2014;(48):76–86.25174028 [Google Scholar]
- 10.Chiu BC, Hou N. Epidemiology and etiology of non-Hodgkin’s lymphoma. Cancer Treat Res. 2015;165:1–25. [DOI] [PubMed] [Google Scholar]
- 11.Jaffe ES, Harris NL, Stein H, Vardiman JW. ed. World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2001. [Google Scholar]
- 12.Wilkins BS. Pitfalls in lymphoma pathology: avoiding errors in diagnosis of lymphoid tissues. J Clin Pathol. 2011;64(6):466–476. [DOI] [PubMed] [Google Scholar]
- 13.Swerdlow SH, Campo E, Harris NL, et al., eds. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2008. [Google Scholar]
- 14.Chang C, Huang SW, Su IJ, Chang KC. Hematopathologic discrepancies between referral and review diagnoses: a gap between general pathologists and hematopathologists. Leuk Lymphoma. 2014;55(5):1023–1030. [DOI] [PubMed] [Google Scholar]
- 15.Cainelli F, Tanko MN, Vento S. The challenge of lymphomas in sub-Saharan Africa. Lancet Oncol. 2010;11(7):610–611. [DOI] [PubMed] [Google Scholar]
- 16.Wiggill TM, Mayne ES, Willem P. Challenges in lymphoma diagnosis in HIV positive patients in the South African setting. Transfus Apher Sci. 2013;49(2):157–162. [DOI] [PubMed] [Google Scholar]
- 17.World Health Organization Classification of malignant lymphomas in Japan: incidence of recently recognized entities. Lymphoma Study Group of Japanese Pathologists. Pathol Int. 2000;50(9):696–702. [DOI] [PubMed] [Google Scholar]
- 18.Abdel-Fattah MM, Yassine OG. Non-Hodgkin’s lymphomas in Alexandria, Egypt; incidence rates and trend study (1995–2004). Eur J Cancer Prev. 2007;16(5):479–485. [DOI] [PubMed] [Google Scholar]
- 19.Sun J, Yang Q, Lu Z, et al. Distribution of lymphoid neoplasms in China: analysis of 4,638 cases according to the World Health Organization classification. Am J Clin Pathol. 2012;138(3):429–434. [DOI] [PubMed] [Google Scholar]
- 20.Arora N, Manipadam MT, Nair S. Frequency and distribution of lymphoma types in a tertiary care hospital in South India: analysis of 5115 cases using the World Health Organization 2008 classification and comparison with world literature. Leuk Lymphoma. 2013;54(5):1004–1011. [DOI] [PubMed] [Google Scholar]
- 21.Herrinton LJ, Goldoft M, Schwartz SM, Weiss NS. The incidence of non-Hodgkin’s lymphoma and its histologic subtypes in Asian migrants to the United States and their descendants. Cancer Causes Control. 1996;7(2):224–230. [DOI] [PubMed] [Google Scholar]
- 22.Clarke CA, Glaser SL, Gomez SL, et al. Lymphoid malignancies in U.S. Asians: incidence rate differences by birthplace and acculturation. Cancer Epidemiol Biomarkers Prev. 2011;20(6):1064–1077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cross AJ, Ward MH, Schenk M, et al. Meat and meat-mutagen intake and risk of non-Hodgkin lymphoma: results from a NCI-SEER case-control study. Carcinogenesis. 2006;27(2):293–297. [DOI] [PubMed] [Google Scholar]
- 24.Aschebrook-Kilfoy B, Ollberding NJ, Kolar C, et al. Meat intake and risk of non-Hodgkin lymphoma. Cancer Causes Control. 2012;23(10):1681–1692. [DOI] [PubMed] [Google Scholar]
- 25.Ollberding NJ, Aschebrook-Kilfoy B, Caces DB, et al. Phytanic acid and the risk of non-Hodgkin lymphoma. Carcinogenesis. 2013; 34(1):170–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Food and Agriculture Organization of the United Nations. The State of Food and Agriculture 2009. Available from: http://www.fao.org/docrep/012/i0680e/i0680e.pdf. [Last accessed: January 10, 2016].
- 27.Miyazato H, Nakatsuka S, Miyanaga I, et al. Follicular lymphoma in Osaka, Japan: histological features and chronological change. Int J Hematol. 2002;76(4):333–337. [DOI] [PubMed] [Google Scholar]
- 28.Chuang SS. Significant increase in the relative frequency of follicular lymphoma in Taiwan in the early 21st century. J Clin Pathol. 2008;61(7):879–880. [DOI] [PubMed] [Google Scholar]
- 29.Anwar N, Kingma DW, Bloch AR, et al. The investigation of Epstein-Barr viral sequences in 41 cases of Burkitt’s lymphoma from Egypt: epidemiologic correlations. Cancer. 1995;76(7):1245–1252. [DOI] [PubMed] [Google Scholar]
- 30.Dowd JB, Palermo T, Brite J, McDade TW, Aiello A. Seroprevalence of Epstein-Barr virus infection in U.S. children ages 6–19, 2003–2010. PLoS One. 2013;8(5):e64921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Xiong G, Zhang B, Huang MY, et al. Epstein-Barr virus (EBV) infection in Chinese children: a retrospective study of age-specific prevalence. PLoS One. 2014;9(6):e99857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sukpanichnant S. Analysis of 1983 cases of malignant lymphoma in Thailand according to the World Health Organization classification. Hum Pathol. 2004;35(2):224–230. [DOI] [PubMed] [Google Scholar]
- 33.Naresh KN, Advani S, Adde M, et al. Report of an International Network of Cancer Treatment and Research workshop on non-Hodgkin’s lymphoma in developing countries. Blood Cells Mol Dis. 2004; 33(3):330–337. [DOI] [PubMed] [Google Scholar]
- 34.Yang QP, Zhang WY, Yu JB, et al. Subtype distribution of lymphomas in Southwest China: analysis of 6,382 cases using WHO classification in a single institution. Diagn Pathol. 2011;6:77–1596–6–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Vose J, Armitage J, Weisenburger D, International T-Cell Lymphoma Project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008;26(25):4124–4130. [DOI] [PubMed] [Google Scholar]
- 36.Abouyabis AN, Shenoy PJ, Lechowicz MJ, Flowers CR. Incidence and outcomes of the peripheral T-cell lymphoma subtypes in the United States. Leuk Lymphoma. 2008;49(11):2099–2107. [DOI] [PubMed] [Google Scholar]
- 37.Adams SV, Newcomb PA, Shustov AR. Racial patterns of peripheral T-cell lymphoma incidence and survival in the United States. J Clin Oncol. 2016;34(9):963–971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Pan JW, Cook LS, Schwartz SM, Weis NS. Incidence of leukemia in Asian migrants to the United States and their descendants. Cancer Causes Control. 2002;13(9):791–795. [DOI] [PubMed] [Google Scholar]
- 39.National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program. SEER Stat Fact Sheets: Non-Hodgkin Lymphoma. Available from: http://seer.cancer.gov/statfacts/html/nhl.html. [Last accessed: January 4, 2016].
- 40.Gijsbers van Wijk CM, van Vliet KP, Kolk AM. Gender perspectives and quality of care: towards appropriate and adequate health care for women. Soc Sci Med. 1996;43(5):707–720. [DOI] [PubMed] [Google Scholar]
- 41.Balarajan Y, Selvaraj S, Subramanian SV. Health care and equity in India. Lancet. 2011;377(9764):505–515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Goldman L, Ezzat S, Mokhtar N, et al. Viral and non-viral risk factors for non-Hodgkin’s lymphoma in Egypt: heterogeneity by histological and immunological subtypes. Cancer Causes Control. 2009;20(6):981–987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.The World Bank Database. GDP per capita. Available from: http://data.worldbank.org/indicator/NY.DP.PCAP.CD. [Last accessed: January 4, 2016].
- 44.UNAIDS. Countries. Available from: http://www.unaids.org/en/regionscoun-tries/countries. [Last accessed: July 10, 2015].
- 45.Al-Hamadani M, Habermann TM, Cerhan JR, Macon WR, Maurer MJ, Go RS. Non-Hodgkin lymphoma subtype distribution, geodemographic patterns, and survival in the US: A longitudinal analysis of the National Cancer Data Base from 1998 to 2011. Am J Hematol. 2015;90(9):790–795. [DOI] [PubMed] [Google Scholar]