

Abstract
Background
Children raised in institutions are at increased risk of developing internalizing and externalizing problems. However, not all children raised in institutions develop psychopathology. Deficits in error monitoring may be one risk pathway for children with a history of institutionalization given that these skills are related to both internalizing and externalizing psychiatric disorders. Error monitoring and the neural circuitry that supports it have a protracted developmental time course and are highly susceptible to the effects of adversity. As such, they may play an important moderating role between a history of institutional rearing and subsequent psychopathology.
Methods
We investigated the impact of psychosocial deprivation on behavioral and neural responses (event-related potentials: ERPs) to a Flanker task assessing error monitoring and the relations between these measures and psychopathology for 12-year-old children in the Bucharest Early Intervention Project (BEIP). The BEIP involves two groups of institutionalized children randomly assigned in infancy to receive either a foster care intervention (FCG) or care as usual (CAUG).
Results
Children who experienced institutional care, particularly those in the CAUG, showed perturbed behavioral performance and ERPs on the Flanker task. Additionally, an ERP measure of error monitoring [error-related negativity (ERN)] moderated the relations between time spent in institutions and externalizing and ADHD behaviors. When the amplitude of the ERN was smaller, time spent in institutional care was positively related to ADHD and externalizing behaviors, whereas time spent in institutions was unrelated to externalizing problems when children evidenced a larger ERN. Neural correlates of error monitoring did not moderate the relations between time spent in institutionalized care and internalizing behaviors.
Conclusions
Exposure to institutional care early in life may affect brain circuitry associated with error monitoring. Perturbations in this neural circuitry in combination with psychosocial deprivation are possibly a risk pathway associated with the development of externalizing and ADHD problems.
Keywords: institutions, externalizing disorder, internalizing disorder, cognition, event-related potentials
Introduction
Children raised in institutions experience severe psychosocial deprivation and display a myriad of negative developmental outcomes in cognition and psychopathology (C. A. Nelson, Fox, & Zeanah, 2014). Children who experience institutional care in early childhood are at increased risk of developing both internalizing and externalizing disorders later in life (Colvert et al., 2008; Humphreys et al., 2015; Tizard & Rees, 1975). Nevertheless, only some children with a history of institutional rearing subsequently develop psychopathology. Identifying factors that differentiate between those children who do and do not develop disorders are of great interest.
A good deal of evidence has linked early deprivation to deficits in executive skills throughout childhood (Colvert et al., 2008; Loman et al., 2013; Merz & McCall, 2011). One cognitive domain that is of particular interest is error monitoring because deficits have been reported among multiple samples of previously institutionalized children (Loman et al., 2013; McDermott et al., 2013). Furthermore, error monitoring has a well-defined neural correlate known as the error-related negativity (ERN; Falkenstein, Hohnsbein, Hoormann, & Blanke, 1991), which is an even-related potential (ERP) believed to be generated in the anterior cingulate cortex (Dehaene, Posner, & Tucker, 1994; Van Veen & Carter, 2002). The ERN is a negative deflection maximal at frontocentral sites and peaks within the first 100 ms following an errant response. The ERN is thought to index error and conflict detection associated with incorrect response selection (Hajcak, 2012). Data suggest that the ability to monitor errors and the ERN component emerge in childhood (Grammer, Carrasco, Gehring, & Morrison, 2014) and develop throughout adolescence, with the ERN becoming more negative and stable in late adolescence and early adulthood (Davies, Segalowitz, & Gavin, 2004).
To our knowledge, only one study from another sample (Loman et al., 2013) and two studies from the present sample (McDermott et al., 2013; McDermott, Westerlund, Zeanah, Nelson, & Fox, 2012) have examined error monitoring and the ERN in previously institutionalized children. All three studies examined the ERN in late childhood (ages 8–11) and results are inconsistent. One study showed evidence that children who experienced institutional care exhibited smaller (less negative) ERNs (McDermott et al., 2012), while the other two studies found no or mixed evidence for reduced ERN amplitudes in previously institutionalized children (Loman et al., 2013; McDermott et al., 2013). One reason for these mixed findings may be that the ERN goes through rapid changes, possibly associated with puberty, in late childhood, and adolescence (Davies et al., 2004), which results in individual variability eclipsing group differences. Another reason for inconsistent findings may be that the duration institutional care experienced by a child may influence ERN development, with longer amounts of time in institutional care associated with larger deficits in error monitoring. Indeed, other cognitive skills have been shown to be negatively impacted by prolonged exposure to institutional care (Troller-Renfree & Fox, 2016; Troller-Renfree et al., in press; Troller-Renfree, McDermott, Nelson, Zeanah, & Fox, 2015).
In addition to its association with early adversity, the ERN has been associated with both internalizing and externalizing disorders (Olvet & Hajcak, 2008). Within the internalizing domain, heightened amplitude of the ERN is associated with greater symptoms of anxiety. The ERN also has been related to externalizing behaviors, such as aggression (Dikman & Allen, 2000; L. D. Nelson, Patrick, & Bernat, 2011) and ADHD behaviors (Shiels & Hawk, 2010), especially, impulsivity (Martin & Potts, 2009; L. D. Nelson et al., 2011). Reduced amplitude of the ERN is associated with more ADHD and externalizing behaviors. To our knowledge, only one study using the present sample examined whether error monitoring moderates associations between deprived caregiving experience and the expression of socioemotional behavior problems in childhood. In this study, McDermott and colleagues (2013) demonstrated that among a subset of children – those who had been removed from institutional care and placed into foster care – a larger ERN predicted lower levels of socioemotional behavior problems. While these findings suggest that there may be a relation between the ERN, institutionalized care, and psychopathology, this link has yet to be established in a sample of previously institutionalized children who did not receive intervention. One reason for the lack of previous findings may be that the association between the ERN and psychopathology does not appear until later adolescence (Meyer, Weinberg, Klein, & Hajcak, 2012). Additionally, given that the prevalence of many internalizing and externalizing disorders increase throughout adolescence (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003; Merikangas, Nakamura, & Kessler, 2009), there may not have been enough variability in internalizing and externalizing problems to detect associations. Another reason for the heterogeneity of past findings may be that prior studies have not examined whether the duration of institutional care effects the development of the ERN and whether reduced ERN amplitudes compound with institutional care to predict the emergence of psychopathology. The identification of the ERN as a possible factor for the development of psychopathology in previously institutionalized children is thus of great interest given that it may identify one of the pathways by which psychopathology emerges as well as suggest a system to target for evidence-based interventions aimed at improving mental health.
This study examined the development of error monitoring in a sample of children who experienced early institutionalization and were enrolled in the Bucharest Early Intervention Project (BEIP) – a randomized controlled trial of foster care as an alternative to institutional care (Nelson, Fox, & Zeanah, 2014; Zeanah et al., 2003). Children in the study were randomized to one of two conditions: removed from an institution and placed into foster care (Foster Care Group; FCG) or remained in institutional care (Care as Usual Group; CAUG). Following randomization, children placed into the FCG received high quality care that was supported by project staff through age 54 months. While many FCG children remained in their assigned foster care placement, others left their foster care home for variety of reasons including reunion with their biological families. Children randomized to the CAUG received care provided by the local governmental authorities, including continued institutional care for some, but others were reunited with their biological family, placed into government-run foster care (not associated with the BEIP foster care), or adopted domestically (see Figure 1 for CONSORT diagram). In addition, a typically developing sample of children (Never Institutionalized Group; NIG) was recruited from the community. The primary reason for recruiting children from the Bucharest community was to ensure that measures collected at each age point provided normative data. Behavioral responses, reaction times, and continuous electroencephalography (EEG) were collected during a modified Flanker task when children were 12 years of age.
Figure 1.

CONSORT diagram.
Consistent with past studies examining the effect of institutionalized care on error monitoring, we predicted that previously institutionalized children would show perturbed behavioral performance and lower ERN amplitude (a neural correlate of error monitoring). Additionally, consistent with findings at 8 years of age (McDermott et al., 2013), we hypothesized that the FCG would show better performance and enhanced neural correlates related to error monitoring. Building on past findings, we also predicted that prolonged institutional care would lead to reduced ERN. Finally, given that past studies using previously institutionalized samples have suggested that neural correlates of error monitoring may moderate the relations between early adversity and externalizing behaviors, we predicted that amplitude of the ERN would moderate the relation between prolonged institutionalized care and the presentation of externalizing disorders at age 12. The specificity of this moderating effect across externalizing subscales was not hypothesized, given that no study has previously investigated this question.
Methods
Participants
The sample comprised 136 children, abandoned in infancy (M=2.57 months) and placed into institutional care in Bucharest, Romania. Hallmarks of institutional care include social deprivation (high caregiver-child ratios) and non-contingent caregiving (for more information see C. A. Nelson et al., 2014 and Zeanah et al., 2003). Following assessment, children were randomized into two groups – Care as Usual Group (CAUG) and Foster Care Group (FCG). A group of never institutionalized community children (NIG) were also assessed. At age 12, 50 CAUG (23 girls), 50 FCG (24 girls), and 48 NIG (26 girls) completed the Flanker Task and 38 CAUG, 36 FCG, and 47 NIG provided usable behavioral data. The mean age of assessment was 11.39 for CAUG, 11.92 for FCG, and 12.14 for NIG.
The University Institutional Review Boards of the principal investigators (Fox, Nelson & Zeanah) and of the University of Bucharest, Romania, approved the study protocol. The appropriate legal guardian provided consent for participation of previously and currently institutionalized children.
Flanker task
At age 12, participants completed an adapted version of the Flanker task (Eriksen & Eriksen, 1974). Stimuli were presented electronically using E-Prime 2.0 software (Psychology Software Tools, Pittsburgh, PA) and consisted of five angle brackets presented horizontally. Half of the trials were congruent with all of the arrows facing the same direction (⋘≪ or ≫⋙) and half of the trials were incongruent with the middle arrow facing the opposite direction of the four flanking arrows (<<>≪ or ≫<>>). Participants completed 20 practice trials followed by 160 test trials. Consistent with past tasks used with the present institutional sample (McDermott et al., 2013), the task dynamically adjusted the stimulus presentation time based on each participant's performance. If a participant had a cumulative accuracy greater than 60% the subsequent trial presentation time was decreased by 50ms. Conversely, if cumulative accuracy was less than 60% the subsequent trial presentation time was increased by 50ms. Presentation times were between 100 and 1450ms with a mean presentation time of 553.34ms (SD=414.46). Furthermore, to prevent against expectancy effects, stimulus presentation times were jittered by one of three values: -60ms, -10ms, +40ms. The intertrial interval was randomly assigned to be one of four durations: 773ms, 790ms, 807ms, or 824ms. Finally, to verify capacity to complete the flanker task, participants with a cumulative accuracy below 55% were excluded from all analyses (N=27).
ERP processing
Continuous EEG was recorded using a 64-channel Geodesic Sensor Net (Electrical Geodesic, Inc., Eugene, OR). Prior to data collection, electrode impedances were reduced to below 50 kΩ. Data was sampled at 250 Hz throughout collection. All electrodes were referenced online to electrode Cz and re-referenced offline to an average reference. The data were filtered using a digital band-pass FIR filter from 0.3 to 30 Hz.
Response-locked trials were segmented separately for error and correct trials. Trials began 400ms prior to response and extended to 800ms after the response (1,200ms total). Eye blinks were removed using independent component analysis (ICA) performed by the ERP PCAToolkit (Delorme & Makeig, 2004; Dien, 2010). Individual blinks were identified for each participant to create an average blink topography. The ICA components that correlated at .9 or above with the averaged blink topography and/or with the ERP PCAToolkit–supplied blink topography were removed. Next, an automated procedure was used for artifact rejection. Channels were marked bad if the fast average amplitude exceeded 130μV or if the difference between a channel and the neighboring channels was greater than 30μV for an individual segment. Channels were marked globally bad if the correlation between neighboring channels was less than .40 or if the channel was bad on greater than 20% of trials. Trials were marked bad if more than 10% of the channels were determined to be bad. Bad channels on the remaining good trials were replaced using spherical spline interpolation (Perrin, Pernier, Bertrand, & Echallier, 1989).
Correct and error trials were separately averaged for each participant and were baseline corrected to the average activity from 400ms to 200ms before the response. The ERN and CRN were evaluated as the average activity at the frontocentral electrode 4 (FCz) where the ERN was maximally negative. The ERN and CRN amplitudes were extracted as the mean activity -50–150ms. Participants were included in ERP analyses if they had at least 10 artifact-free error trials in each condition. To examine brain activity specific to errors, a difference wave was created by subtracting the brain activity on correct trials from the brain activity on error trials for the ERN (i.e., ERN – CRN; ΔERN).
Trials with reaction times faster than 200ms and slower than 1200ms were removed from the analysis. On average, less than 5% of trials were removed due to extreme reaction times (M=7.26 trials, SD=8.26). The numbers of trials excluded due to extreme reaction times were not different between groups, F(118)=.622, p=.539. Accuracy was calculated as the number of correct trials divided by the total number of trials without an extreme response. Reaction times were averaged separately for correct trials and error trials for each participant in each condition and did not include non-response trials.
MacArthur Health and Behavior Questionnaire (HBQ)
The HBQ was developed by members and affiliates of the John D. and Catherine T. MacArthur Foundation Research Network on Psychopathology and Development (for more information see: https://macarthurhbq.wordpress.com/). Although several publications have established clinically meaningful cut-points for some of the mental health scales (Lemery-Chalfant et al., 2007; Luby et al., 2002), the HBQ does not yield clinical diagnoses. Rather, the HBQ provides dimensional scales to enable researchers to assess children's mental health and well-being. The version administered to each participant's primary teacher at age 12 was comprised of 105 items. For the present paper, two composites and their subscales from the HBQ were examined: internalizing behaviors and externalizing/ADHD behaviors. The internalizing composite comprises items related to depression and overanxious behaviors. The externalizing and ADHD composite comprises measures of oppositional defiance, conduct problems, overt hostility, relational aggression, inattention, and impulsivity. The HBQ was completed by each participant's primary teacher.
Analytic plan
Behavioral differences in performance accuracy were examined using repeated measures ANOVAs using IBM SPSS, Version 22.0. Participant group (CAUG, FCG, NIG) served as a between-subjects factor and flanker trial type (congruent, incongruent) served as a within-subjects factor. Next, differences in reaction time were examined using repeated measures ANOVAs. Participant group (CAUG, FCG, NIG) served as a between-subjects factor and accuracy (correct, incorrect) served as a within-subjects factor. For analyses examining group differences in the ΔERN, a one-way ANOVA was conducted with Group (CAUG, FCG, NIG) as the between-subjects factor. Additionally, a linear regression was conducted to examine whether percentage of time spent in institutional care predicts ΔERN amplitude. Greenhouse-Geisser corrections were applied as necessary.
For analyses examining the moderating role of the ΔERN, two separate path models were conducted in M-PLUS using FIML estimation for missing data (Muthen & Muthen, 1998-2011). First, separate moderation analyses were conducted with Internalizing and Externalizing/ADHD behaviors composites as outcomes. Exploratory follow-up moderation analyses were conducted to examine the moderating role of individual subscales that compose the externalizing/ADHD composite.
Results
Behavioral analyses
Accuracy
Table 1 displays the accuracy and reaction times across group. Intent-to-treat results revealed a main effect of trial type with higher accuracy on congruent (M=79.85, SD=9.69) compared to incongruent trials (M=51.28, SD=14.36), F(1,72)=236.54, p<.001, ᶯ2=.767. The main effect of group (F(1,72)=236.54, p<.001, ᶯ2=.767) and group by trial type interaction (F(1,72)=2.776, p=.100, ᶯ2=.037) failed to reach significance. However, when compared to the community sample, an additional main effect of group emerged with the NIG (M=74.6, SD=11.32) outperforming the CAUG (M=63.8, SD=7.49) and FCG (M=67.4, SD=10.64), F(2,118)=12.658, p<.001, ᶯ2=.177.
Table 1. Reaction Time, accuracy, and demographics (standard deviations in parentheses).
| CAUG | FCG | NIG | Group Differences | |
|---|---|---|---|---|
| Subjects with behavioral data (N) | 38 | 36 | 47 | - |
| Overall Accuracy | 63.90% (7.49) | 67.37% (10.64) | 74.67% (11.32) | - |
| Congruent Accuracy | 79.34% (9.18) | 80.39% (10.30) | 87.26% (8.97) | - |
| Incongruent Accuracy | 48.34% (14.17) | 54.39% (14.08) | 61.90% (16.14) | - |
| Error Reaction Time | 458.60 (128.72) | 386.43 (78.36) | 386.75 (81.81) | - |
| Correct Reaction Time | 504.42 (102.50) | 462.98 (79.87) | 459.28 (85.20) | - |
| Age of Entry into Institution | 2.48 (3.76) | 2.52 (3.46) | - | Not Significant |
| % Time in Institution | 44.96 (27.25) | 15.76 (10.33) | - | CAUG>FCG |
| WISC IQ | 67.57 (13.20) | 78.75 (14.90) | 99.70 (13.97) | NIG>FCG>CAUG |
| Gender (% female) | 61% | 53% | 47% | Not Significant |
| Internalizing (HBQ)1 | .50 (.34) | .41 (.32) | .24 (.27) | NIG<CAUG |
| Externalizing/ADHD (HBQ)2 | .48 (.46) | .46 (.47) | .11 (.20) | NIG<CAUG & FCG |
| Oppositional Defiant (HBQ) | .70 (.57) | .65 (.65) | .15 (.27) | NIG<CAUG & FCG |
| Conduct Problems (HBQ) | .28 (.34) | .24 (.33) | .03 (.07) | NIG<CAUG & FCG |
| Overt Aggression (HBQ) | .57 (.63) | .53 (.57) | .12 (.26) | NIG<CAUG & FCG |
| Relational Aggression (HBQ) | .37 (.46) | .41 (.44) | .13 (.24) | NIG<FCG |
| Inattention (HBQ) | .90 (.57) | .77 (.65) | .25 (.34) | NIG<CAUG & FCG |
| Impulsivity (HBQ) | .72 (.58) | .67 (.60) | .28 (.29) | NIG<CAUG & FCG |
Mean of Depression and Overanxious
Mean of Oppositional Defiant, Conduct Problems, Relational Aggression, Overt Hostility, Inattention, Impulsivity
Reaction time
Intent-to-treat results revealed a main effect of trial type with quicker responses on incorrect trials (M=423.49, SD=112.52) compared to correct trials (M=484.25, SD=93.91), F(1,72)=115.45, p<.001, ᶯ2=.616 and a main effect of group with the FCG (M=424.71, SD=91.08) showing significantly faster responses than the CAUG (M=481.509, SD=91.08), F(1,72)=6.35, p=.014, ᶯ2=.081. These main effects were qualified by a group by accuracy interaction, F(1,72)=7.280, p=.009, ᶯ2=.092. Post-hoc follow-ups revealed that both groups showed faster reaction times on error trials when compared to correct trials. Furthermore, groups did not differ in reaction times on incorrect trials (CAUG: M=458.60, SD=128.72; FCG: M=368.433, SD=78.36). However, on correct trials, the CAUG was significantly slower to respond than the FCG (CAUG: M=504.42, SD=102.5; FCG: M=462.98, SD=79.87).
Follow up analyses comparing ever institutionalized children to community controls, results were almost identical with a main effect of trial type (error trials faster than correct trials; F(1,118)=239.87, p<.001, ᶯ2=.670), a main effect of group (CAUG slower than the FCG and NIG; F(2,118)=5.245, p=.007, ᶯ2=.082), and a significant group by accuracy interaction, F(2,118)=5.100, p=.008, ᶯ2=.080. Post-hoc follow-ups revealed that all groups showed faster reaction times on error trials when compared to correct trials and all three groups did not differ in reaction times on incorrect trials. However, on correct trials, the CAUG was significantly slower to respond than the FCG and NIG (CAUG: M=504.42, SD=102.5; FCG: M=462.98, SD=79.87; NIG: M=459.28, SD=85.20).
ERP analyses
Figure 2 shows the ERP waveform for each group. Intent-to-treat analyses examining differences in the ΔERN revealed a marginal main effect of Group, F(1,68)=3.57, p=.063, with the CAUG (M=-.56, SD=2.40) exhibiting a marginally smaller ΔERN than the FCG (M=-1.67, SD=2.50. Given this pattern of results, a linear regression was conducted to see if amount of time spent in institutional care predicted ΔERN amplitude. Results showed that amount of time spent in institutional care significantly predicted ΔERN amplitude, with smaller (less negative) amplitudes among children who experienced prolonged institutional care, β=.272, t(68)=2.332, p=.023.
Figure 2.
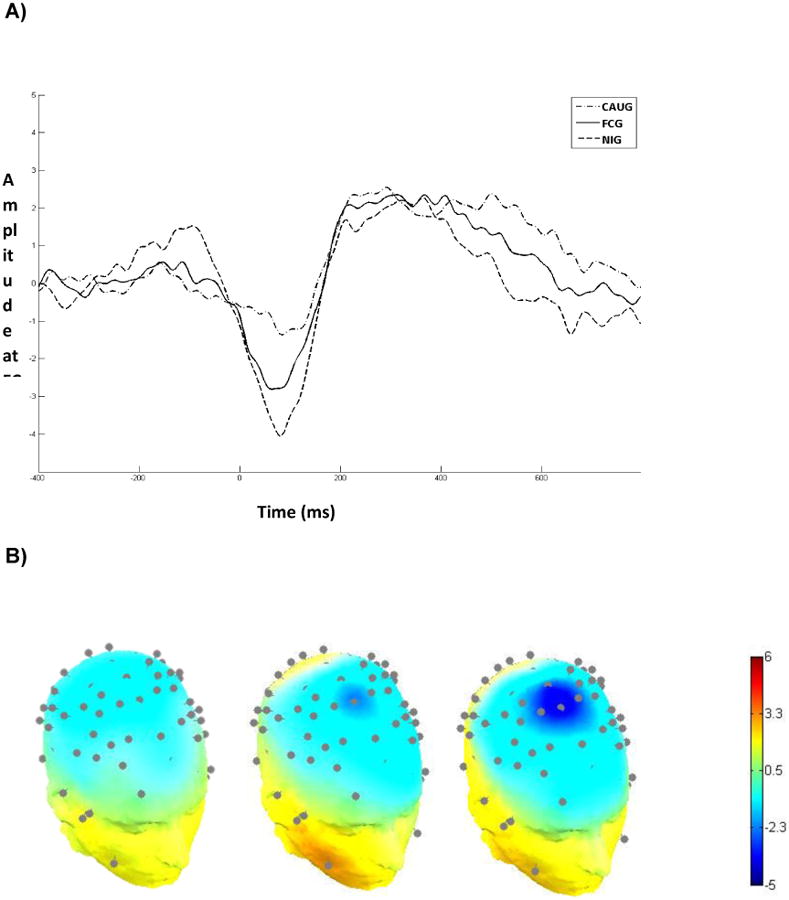
A) Response-locked event-related potential waveforms for ΔERN (ERN-CRN) at electrode FCz (where activity was maximal). B) Scalp topographies of the ΔERN for the CAUG (left), FCG (middle), and NIG (right) at 76ms after response.
Follow up analyses of ever institutionalized children and community controls examining ΔERN differences revealed a main effect of Group, F(2,111)=3.69, p=.028. Follow-up independent-samples t tests revealed that the CAUG (M=-.56, SD=2.40) showed a significantly smaller ΔERN than the NIG (M=-2.21, SD=3.167; t(79)=2.60, p=.011), but no significant difference between the FCG and NIG, t(75)=.811, p=.420.
Mental health
All moderation models are presented in Table 2. To determine whether the ΔERN exhibits moderating effects on the relations between amount of time spent in institutional care and internalizing and externalizing/ADHD symptomology, two separate moderation analyses were conducted. Results revealed that the ΔERN did not moderate the relation between percent of life spent in institutional care and internalizing behaviors (β=.002, p=.155), however the ΔERN did moderate the relationship between percent of time spent in institutional care and externalizing/ADHD behaviors (β=.003, p=.018). Follow-up analyses revealed when the ΔERN was smaller, time spent in institutional care was positively related to externalizing problems (β=.010, p=.021) whereas time spent in institutionalized care was unrelated to externalizing problems when children evidenced a larger ΔERN (β=-0.007, p=.110).
Table 2. Moderation analyses.
| B | SE B | R2 | |
|---|---|---|---|
| Internalizing1 | .162 | ||
| % Institutional Care | .002 | .002 | |
| ΔERN | -.030 | .031 | |
| % Inst*ΔERN | .002 | .001 | |
| Externalizing\ADHD2 | .349 | ||
| % Institutional Care | .001 | .002 | |
| ΔERN | -.073 | .043 | |
| % Inst*ΔERN | .003* | .001 | |
| Oppositional Defiance | .383 | ||
| % Institutional Care | .003 | .003 | |
| ΔERN | -.102 | .053 | |
| % Inst*ΔERN | .005* | .002 | |
| Conduct Problems | .386 | ||
| % Institutional Care | .000 | .002 | |
| ΔERN | -.054 | .030 | |
| % Inst*ΔERN | .003* | .001 | |
| Overt Hostility | .328 | ||
| % Institutional Care | .001 | .003 | |
| ΔERN | -.106 | .055 | |
| % Inst*ΔERN | .004* | .002 | |
| Relational Aggression | .566 | ||
| % Institutional Care | .000 | .002 | |
| ΔERN | -.103** | .039 | |
| % Inst*ΔERN | .001** | .002 | |
| Inattention | .037 | ||
| % Institutional Care | .002 | .003 | |
| ΔERN | -.004 | .057 | |
| % Inst*ΔERN | .001 | .002 | |
| Impulsivity | .257 | ||
| % Institutional Care | .002 | .003 | |
| ΔERN | -.068 | .052 | |
| % Inst*ΔERN | .003ˆ | .002 |
Notes.
p<.06,
p<.05,
p<.01.
Mean of Depression and Overanxious
Mean of Oppositional Defiant, Conduct Problems, Relational Aggression, Overt Hostility, Inattention, Impulsivity
To further investigate the moderating effects of the ΔERN on the relation between amount of time spent in institutional care and externalizing problems, separate moderation analyses were conducted for all subscales of the externalizing/ADHD composite. Results revealed a significant moderation effect for the oppositional defiant subscale (β=0.005, p=.012), conduct problems subscale (β=0.003, p=.010), overt hostility subscale (β=0.004, p=.038), relational aggression subscale (β=0.005, p<.001), and marginally with the impulsivity subscale (β=0.003, p=.053), however the inattention subscale (β=0.001, p=.499) did not appear to be moderated by the ΔERN. All moderation analyses showed a pattern similar to the externalizing/ADHD composite, with a positive link between time in institutional care and externalizing subscale when the ΔERN is smaller.
Discussion
We observed that 12-year-old children who had experienced institutionalized care showed decreased accuracy on a modified Flanker task when compared to their never institutionalized peers. Furthermore, only children who were randomized to remain in care as usual showed deficits in processing speed. This effect was specific to trials with correct responses and converges with recent work suggesting that early psychosocial deprivation alters white matter structure, which is thought to underlie processing speed (Hanson et al., 2013; Sheridan, Fox, Zeanah, McLaughlin, & Nelson, 2012). Additionally, we found that prolonged institutional care predicted reductions in the neural correlates associated with error monitoring. To our knowledge, this study is the first to link continued exposure to institutional care to decreases in ERN magnitude as well as identify the ERN as a moderator of the relation between amount of time spent in institutional care and the development of externalizing behaviors. Interestingly, this moderation effect appears to be driven by multiple behavior domains including oppositional and defiant behaviors, conduct problems, overt hostility, relational aggression, and impulsivity. Together, these results suggest that perturbed error monitoring may represent a risk for externalizing problems in previously institutionalized children.
The relations between the neural correlates of error monitoring and externalizing behaviors are well established. This study, like a previous one from the same sample using data when children were 8 years of age, establishes the neural correlates of error monitoring as a potential risk pathway for the development of externalizing behaviors in a previously institutionalized sample (McDermott et al., 2013). Extending previous findings, the present study shows that the moderating effect of error monitoring is present across a wide range of externalizing and ADHD behaviors, though not with inattention. This relation is most likely driven by the high intercorrelation of externalizing behaviors in this sample (rs between .5 and .8). It is of particular clinical interest given the high prevalence of ADHD and externalizing disorders in children placed into institutional care (see Humphreys, Gleason, et al., 2015 for more information on clinical diagnoses).
Consistent with previous findings from this sample, the neural correlates of error monitoring did not moderate the risk for internalizing behaviors (McDermott et al., 2013), despite a strong relation between the ERN and anxiety in never-institutionalized samples (Olvet & Hajcak, 2008). The lack of this relation may be attributable to the low incidence of clinical anxiety disorders in the present sample at 12 years of age (Humphreys et al., 2015).
There are a number of limitations associated with the present study. First, all analyses were conducted within an intent-to-treat framework regardless of each child's current placement. However, given that many of participants no longer reside in their randomized caregiving placement (see Figure 1), our findings likely underrepresent the potential benefits of early enhancement of caregiving quality on error monitoring and psychopathology. Second, a rather substantial portion of the sample could not complete the task with sufficient accuracy (n=26), leading to reduced sample sizes and power. The large number of participants excluded for poor accuracy is not unexpected given the substantial number of children who exhibited low IQs at age 12 years.
In sum, the current study provides evidence that one possible pathway to the development of externalizing and ADHD behaviors in children who have experienced institutionalized care is through deficits in error monitoring.
Key points.
Institutional care is associated with increased psychopathology in adolescence, however the risk factors associated with the emergence of these disorders in this sample are unknown.
Error monitoring has been implicated in the development of both internalizing and externalizing disorders.
Children randomized to continued institutional care show perturbed behavioral performance and altered neural markers of error monitoring.
Neural markers of error monitoring moderated the relationship between amount of time spent in institutional care and externalizing and ADHD behaviors, with children with reduced error monitoring exhibiting increase externalizing behaviors when compared to children with better error monitoring.
Future work should aim to investigate whether interventions targeting error monitoring may protect against the development of externalizing disorders in previously institutionalized populations.
Acknowledgments
Research reported in this publication was supported by the Binder Family, the National Institute of Mental Health of the National Institutes of Health under Award Number R01MH091363 (to C.A.N.) and by a National Science Foundation Graduate Research Fellowship (DGE1322106) to S.T.R. The content is the responsibility of the authors and does not necessarily represent the views of the funding agencies. The authors would like to thank Nichole Ruszkay, Alana Ebert-Zavos, and Jill DeJames for their help. The authors have declared that they have no competing or potential conflicts of interest in relation to this article.
Footnotes
Conflict of Interest Statement: No conflicts declared.
References
- Colvert E, Rutter ME, Beckett C, Castle J, Groothues C, Hawkins A, et al. Sonuga-Barke EJS. Emotional difficulties in early adolescence following severe early deprivation: Findings from the English and Romanian adoptees study. Development and Psychopathology. 2008;20(2):547–67. doi: 10.1017/S0954579408000278. [DOI] [PubMed] [Google Scholar]
- Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and Development of Psychiatric Disorders in Childhood and Adolescence. Archives of General Psychiatry. 2003;60(8):837. doi: 10.1001/archpsyc.60.8.837. [DOI] [PubMed] [Google Scholar]
- Davies PL, Segalowitz SJ, Gavin WJ. Development of response-monitoring ERPs in 7- to 25-year-olds. Developmental Neuropsychology. 2004;25(3):355–76. doi: 10.1207/s15326942dn2503_6. [DOI] [PubMed] [Google Scholar]
- Dehaene S, Posner MI, Tucker DM. Localization of a Neural System for Error Detection and Compensation. Psychological Science. 1994;5(5):303–305. doi: 10.1111/j.1467-9280.1994.tb00630.x. [DOI] [Google Scholar]
- Delorme A, Makeig S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. Journal of Neuroscience Methods. 2004;134(1):9–21. doi: 10.1016/j.jneumeth.2003.10.009. [DOI] [PubMed] [Google Scholar]
- Dien J. The ERP PCA Toolkit: an open source program for advanced statistical analysis of event-related potential data. Journal of Neuroscience Methods. 2010;187(1):138–45. doi: 10.1016/j.jneumeth.2009.12.009. [DOI] [PubMed] [Google Scholar]
- Dikman ZV, Allen JJB. Error monitoring during reward and avoidance learning in high- and low-socialized individuals. Psychophysiology. 2000;37(1):43–54. doi: 10.1111/1469-8986.3710043. [DOI] [PubMed] [Google Scholar]
- Eriksen BA, Eriksen CW. Effects of noise letters upon the identification of a target letter in a nonsearch task. Perception & Psychophysics. 1974;16(1):143–149. doi: 10.3758/BF03203267. [DOI] [Google Scholar]
- Falkenstein M, Hohnsbein J, Hoormann J, Blanke L. Effects of crossmodal divided attention on late ERP components. II. Error processing in choice reaction tasks. Electroencephalography and Clinical Neurophysiology. 1991;78(6):447–455. doi: 10.1016/0013-4694(91)90062-9. [DOI] [PubMed] [Google Scholar]
- Grammer JK, Carrasco M, Gehring WJ, Morrison FJ. Age-related changes in error processing in young children: a school-based investigation. Developmental Cognitive Neuroscience. 2014;9:93–105. doi: 10.1016/j.dcn.2014.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hajcak G. What We've Learned From Mistakes: Insights From Error-Related Brain Activity. Current Directions in Psychological Science. 2012;21(2):101–106. doi: 10.1177/0963721412436809. [DOI] [Google Scholar]
- Hanson JL, Adluru N, Chung MK, Alexander AL, Davidson RJ, Pollak SD. Early neglect is associated with alterations in white matter integrity and cognitive functioning. Child Development. 2013;84(5):1566–78. doi: 10.1111/cdev.12069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humphreys KL, Gleason MM, Drury SS, Miron DM, Nelson CA, Fox NA, Zeanah CH. Effects of institutional rearing and foster care on psychopathology at age 12 years in Romania: Follow-up of an open, randomized, controlled trial. The Lancet Psychiatry. 2015;2(7):625–634. doi: 10.1016/S2215-0366(15)00095-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lemery-Chalfant K, Schreiber JE, Schmidt NL, Van Hulle CA, Essex MJ, Goldsmith HH. Assessing internalizing, externalizing, and attention problems in young children: validation of the MacArthur HBQ. Journal of the American Academy of Child and Adolescent Psychiatry. 2007;46(10):1315–23. doi: 10.1097/chi.0b013e3180f616c6. [DOI] [PubMed] [Google Scholar]
- Loman MM, Johnson AE, Westerlund AJ, Pollak SD, Nelson CA, Gunnar MR. The effect of early deprivation on executive attention in middle childhood. Journal of Child Psychology and Psychiatry. 2013;54(1):37–45. doi: 10.1111/j.1469-7610.2012.02602.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luby JL, Heffelfinger A, Measelle JR, Ablow JC, Essex MJ, Dierker L, et al. Kupfer DJ. Differential performance of the macarthur HBQ and DISC-IV in identifying DSM-IV internalizing psychopathology in young children. Journal of the American Academy of Child and Adolescent Psychiatry. 2002;41(4):458–66. doi: 10.1097/00004583-200204000-00019. [DOI] [PubMed] [Google Scholar]
- Martin LE, Potts GF. Impulsivity in Decision-Making: An Event-Related Potential Investigation. Personality and Individual Differences. 2009;46(3):303. doi: 10.1016/j.paid.2008.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDermott JM, Troller-Renfree S, Vanderwert R, Nelson CA, Zeanah CH, Fox NA. Psychosocial deprivation, executive functions, and the emergence of socio-emotional behavior problems. Frontiers in Human Neuroscience. 2013;7:167. doi: 10.3389/fnhum.2013.00167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDermott JM, Westerlund AJ, Zeanah CH, Nelson CA, Fox NA. Early adversity and neural correlates of executive function: Implications for academic adjustment. Developmental Cognitive Neuroscience. 2012;2:59–66. doi: 10.1016/j.dcn.2011.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merikangas KR, Nakamura EF, Kessler RC. Epidemiology of mental disorders in children and adolescents. Dialogues in Clinical Neuroscience. 2009;11(1):7–20. doi: 10.31887/DCNS.2009.11.1/krmerikangas. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merz EC, McCall RB. Parent ratings of executive functioning in children adopted from psychosocially depriving institutions. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 2011;52(5):537–46. doi: 10.1111/j.1469-7610.2010.02335.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer A, Weinberg A, Klein DN, Hajcak G. The development of the error-related negativity (ERN) and its relationship with anxiety: evidence from 8 to 13 year-olds. Developmental Cognitive Neuroscience. 2012;2(1):152–61. doi: 10.1016/j.dcn.2011.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. Sixth. Los Angeles, USA: Muthén & Muthén; 2010. [Google Scholar]
- Nelson CA, Fox NA, Zeanah CH. Romania's abandoned children : Deprivation, brain development, and the struggle for recovery. Cambridge, MA: Harvard University Press; 2014. [Google Scholar]
- Nelson LD, Patrick CJ, Bernat EM. Operationalizing proneness to externalizing psychopathology as a multivariate psychophysiological phenotype. Psychophysiology. 2011;48(1):64–72. doi: 10.1111/j.1469-8986.2010.01047.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olvet DM, Hajcak G. The error-related negativity (ERN) and psychopathology: toward an endophenotype. Clinical Psychology Review. 2008;28(8):1343–54. doi: 10.1016/j.cpr.2008.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perrin F, Pernier J, Bertrand O, Echallier JF. Spherical splines for scalp potential and current density mapping. Electroencephalography and Clinical Neurophysiology. 1989;72(2):184–187. doi: 10.1016/0013-4694(89)90180-6. [DOI] [PubMed] [Google Scholar]
- Sheridan MA, Fox NA, Zeanah CH, McLaughlin KA, Nelson CA. Variation in neural development as a result of exposure to institutionalization early in childhood. Proceedings of the National Academy of Sciences of the United States of America. 2012;109(32):12927–32. doi: 10.1073/pnas.1200041109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiels K, Hawk LW. Self-regulation in ADHD: the role of error processing. Clinical Psychology Review. 2010;30(8):951–61. doi: 10.1016/j.cpr.2010.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tizard B, Rees J. The effect of early institutional rearing on the behaviour problems and affectional relationships of four-year-old children. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 1975;16(1):61–73. doi: 10.1111/j.1469-7610.1975.tb01872.x. [DOI] [PubMed] [Google Scholar]
- Troller-Renfree S, Fox NA. Sensitive Periods of Development. In: Luby JL, editor. Handbook of Preschool Mental Health: Detelopment, Disorders, and Treatment. 2nd. New York, NY: Guilford Publications; 2016. [Google Scholar]
- Troller-Renfree S, McDermott JM, Nelson CA, Zeanah CH, Fox NA. The effects of early foster care intervention on attention biases in previously institutionalized children in Romania. Developmental Science. 2015;18(5):713–722. doi: 10.1111/desc.12261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troller-Renfree S, McLaughlin KA, Sheridan MA, Nelson CA, Zeanah ZH, Fox NA. The beneficial effects of a positive attention bias amongst children with a history of psychosocial deprivation. Biological Psychology. doi: 10.1016/j.biopsycho.2016.04.008. n.d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Veen V, Carter CS. The timing of action-monitoring processes in the anterior cingulate cortex. Journal of Cognitive Neuroscience. 2002;14(4):593–602. doi: 10.1162/08989290260045837. [DOI] [PubMed] [Google Scholar]
- Zeanah CH, Nelson CA, Fox NA, Smyke AT, Marshall P, Parker SW, Koga SF. Designing research to study the effects of institutionalization on brain and behavioral development: The Bucharest Early Intervention Project. Development and Psychopathology. 2003;15(4):885–907. doi: 10.1017/s0954579403000452. [DOI] [PubMed] [Google Scholar]