

Abstract
Aim
This paper is a secondary data analysis to investigate relationships among caregiver stress appraisal, self‐rated health and health‐related Internet use.
Design
Cross‐sectional correlation design.
Methods
National Alliance for Caregiving telephone survey conducted in the USA was a primary data source collected in 2009 from 258 caregivers of persons with dementia, who used the Internet to perform care‐giving tasks. Based on Pearlin's Stress Process Model, structural equation modelling was conducted.
Results
Caregivers with poor health reported higher levels of caregiver stress appraised, which was associated with more Internet use for health‐related purposes. It is required to develop effective Internet‐based resources to meet the needs of highly stressed caregivers of persons with dementia. However, there was no relationship between self‐rated health and health‐related Internet use in dementia caregiver.
Keywords: Caregivers, dementia, internet, resources, stress
Introduction
The rapid growth of the Internet and other technology in recent years has significantly increased the distribution of health information and resources to a much wider healthcare consumer than was previously possible. Almost 80% of Internet users and 59% of US adults are seeking health/medical information on the Internet (Fox 2012). Among them, informal caregivers reported a greater use of online health information, support groups and emailing compared with non‐caregivers (Chou et al. 2011, Fox & Brenner 2012). In addition, caregivers are more likely to participate in social networks, especially when they are seeking health information, care or support (Fox & Brenner 2012). This higher rate can be explained by their intense interest in and positive perceptions of Internet‐based approaches and positive outcomes for better health and caregiving (Eysenbach 2003, Kinnane & Milne 2010, Lewis et al. 2010, Fox & Brenner 2012).
Use of Internet‐based resources for health‐related purposes (hereafter referred to as health‐related Internet use) is an important activity to informal caregivers of persons living with dementia (hereafter referred to as dementia caregivers) while performing care‐giving tasks. Dementia caregivers are known as one of the most vulnerable caregiver populations. They are experiencing higher levels of stress, care‐giving intensity and diverse health problems covering a range of physical, psychological, social and spiritual aspects (Zarit 2006, Schulz & Sherwood 2008, Family Caregiver Alliance 2009). Previous intervention studies based on an Internet‐based care modality reported positive outcomes including better health status (Marziali & Garcia 2011) and increasing levels of confidence in decision‐making, positive caregiver gain, self‐efficacy and intention to seek help, as well as a more positive attitude towards caregiving (Beauchamp et al. 2005, Powell et al. 2008, Lewis et al. 2010).
Background
Dementia caregivers have reported several important benefits of the Internet‐based modality of care, which they found to be convenient and useful because of its high accessibility regardless of time and place (Beauchamp et al. 2005). Using traditional formal services and resources in the community is difficult for them because of time‐constrained situations due to constant care, requiring another caregiver while they are absent, or due to financial burdens (Toseland et al. 1999, Beeber et al. 2008, Powell et al. 2011). Thus, they reported benefits while using Internet‐based information and support resources (Lewis et al. 2010).
Health‐related Internet use in these dyads dealing with dementia leans towards indirect use made by caregivers. Indirect internet use is defined as providing their care recipient with online information and resources when actions are requested by or on behalf of the ill care recipient, while direct use is performed for the user's own benefit (Eysenbach 2003, Kinnane & Milne 2010). Indirect use by caregivers most often occurs when their care recipients lack the necessary knowledge or skills to do so, are far less likely to be cured of their disease and may be too ill to directly use the Internet (Kinnane & Milne 2010). Cognitive impairment and functional disability (Qiu et al. 2009) inevitably hinders direct health‐related Internet use by individuals with dementia.
However, health‐related Internet use in non‐experimental settings has rarely been assessed as a resource‐use behaviour in dementia caregivers in contrast to other types of caregivers, particularly those caring for family members with cancer (Eysenbach 2003, Kinnane & Milne 2010). Previous studies have used interventional study designs because they considered the Internet as an alternative modality for delivering healthcare (Beauchamp et al. 2005, Lewis et al. 2010). Most studies of resource use have focused on the efficacy of traditional formal resources such as health and human resources (Toseland et al. 1999, 2002) or community‐based services (Beeber et al. 2008) rather than web‐based resources. Thus, it is unclear how caregivers' initiatives regarding health‐related Internet use are associated with both health and caregiving in daily living. To address the gaps identified above, this study aimed to provide an in‐depth description of this topic, extending beyond mere descriptions of Internet user profiles (National Telecommunications & Information Administration 2011, Powell et al. 2011). Our research question was ‘Are there significant relationships among caregiver stress appraisal, health‐related Internet use and self‐rated health?'
This study was guided by the Stress Process model (Pearlin et al. 1990), which was specifically designed to understand dementia caregiving. This framework emphasizes the multidimensional nature of care‐giving stress consisting of five constructs: (1) care‐giving context; (2) primary stressors; (3) secondary stressors; (4) resources; and (5) outcomes. Care‐giving context includes the socio‐demographic status of the care recipients and their caregivers, as well as the care‐giving history. Stressors include symptoms or impairments of the care recipients and subjective experiences of caregivers that have a negative impact on health or well‐being of dyads of persons with dementia and their caregivers. Resources are mediators that explain how caregivers may present their burden differently even when dealing with the same stressors; caregivers will experience more stress if they perceive the demands being placed on them as being beyond their coping resources. Outcomes include physical, emotional, psychological and spiritual issues in caregivers. This study proposes that health‐related Internet use was a behaviour to use care‐giving resources based on the Stress Process Model (Pearlin et al. 1990).
The Study
Design
This is a cross‐sectional and correlational study using a secondary data analysis. In this study, the Stress Process Model (Pearlin et al. 1990) directed the design of the hypothesized model, guided variable selection of caregiver stress in measured data and assisted data interpretation in the final model.
Method
Description of primary data source
The primary data provided by the National Alliance for Caregiving and the American Association of Retired Persons (NAC/AARP) database were collected from March–June in 2009 using a standardized computerized‐telephone interviewing system. Interviews were conducted with 6806 adults living in the states of California, Delaware, Illinois, Kansas, Ohio, Virginia and the state of Washington. Random sampling was conducted in general, but African American, Asian and Hispanic groups, as well as older adults (age 50 years or older) were oversampled. The survey collected demographic, health‐related and care‐giving information about both the caregivers and their care recipients. The NAC/AARP database was selected for the study because: (1) it provides up‐to‐date information on Internet use by dementia caregivers; (2) it has used methodologically verified sampling and data collection since 1997 (NAC/AARP 2009a,b).
Sample
A total of 258 dementia caregivers who used the Internet during caregiving were selected. Dementia caregivers were defined as persons ‘providing unpaid care or assistance to a family member, relative, friend, or anyone who had Alzheimer's dementia, other types of dementia, or dementia‐related conditions.’ Unpaid care was defined as ‘helping with personal needs or household chores without any financial compensation (NAC/AARP 2009b, p. 3).’ Exclusion criteria were: (1) the care recipients reported as being younger than 18 years of age as dementia is a rare disease in children (Qiu et al. 2009); (2) caregivers who did not report any information about the dementia condition of the care recipient; and (3) caregivers who never used the Internet seeking health and care‐giving resources.
Measures
Caregiver stress was measured based on subjective appraisal regarding physical strain, emotional stress and financial hardship. They were measured based on a 5‐point Likert scale. Higher scores indicated worse physical strain, emotional stress and financial hardship for caregivers. Across the three items, moderate correlations were observed ranging from 0·42–0·53 (Table 1) with acceptable reliability (Cronbach's α = 0·70).
Table 1.
Correlation coefficients for the measured variables.
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Physical strain | 1·00 | |||||
| 2. Emotional stress | 0·52** | 1·00 | ||||
| 3. Financial hardship | 0·53** | 0·42** | 1·00 | |||
| 4. Self‐rated health | −0·29** | −0·27** | −0·29** | 1·00 | ||
| 5. Diverse types of Internet use | 0·18** | 0·24** | 0·30** | −0·09 | 1·00 | |
| 6. Frequency of Internet use | 0·19** | 0·24** | 0·28** | −0·13* | 0·55** | 1·00 |
*P < 0·05. **P < 0·01.
Self‐rated health is an indicator used to assess the health status of caregivers. Respondents answered a single question, ‘In general, would you say your health is: 1 = poor; 2 = fair; 3 = good; 4 = very good; and 5 = excellent’ extracted from the Medical Outcomes Study 36‐Item Short‐Form General Health Survey (Ware & Sherbourne 1992). This simple measure has been found to be a valid and reliable measure and is commonly used as an index of health and well‐being for dementia caregivers in both interventional design (Mittelman et al. 2007, Elliott et al. 2010) and health and human service‐use studies (Toseland et al. 1999, 2002).
Health‐related Internet use can be defined as using the Internet with the purpose of improving health, well‐being and caregiving (Eysenbach 2003, Kinnane & Milne 2010). Both frequency and diverse types of Internet use were used to construct health‐related Internet use. Frequency was scored on a 4‐point Likert scale based on a single question: ‘How often, if at all, have you gone to Internet websites in the past year to find information in any way related to being a caregiver for your care recipient? Often, sometimes, rarely, or never? (NAC/AARP 2009b, p. 18).’ Higher scores indicated more frequent Internet use as reported by caregivers. Diversity of use was a summed score of six items related to the care recipient's condition, services, support group, a specific task, healthcare providers and care facilities (range: 0–6). Higher scores indicated more diverse use of health‐related Internet information during caregiving (Pearson r = 0·55, P < 0·01, Cronbach's α = 0·82).
Statistical analysis
A structural equation modelling (sem) tested the hypothesized relationships among: a latent variable of caregiver stress appraisal, a latent variable of health‐related Internet use and a measured variable of self‐rated health (Figure 1). This sem analytical technique not only allows simultaneous testing of multiple hypotheses representing complex relationships between latent variables but also accommodates multiple indicators with measurement errors (Loehlin 2004). The analysis was initiated using two separate confirmatory factor analyses (CFAs) for assessing measurement models of both latent variables of caregiver stress appraisal and health‐related Internet use. sems compared eight completing models using Mplus version 7. Model fit between hypothesized models and the measured data was examined based on chi‐square statistics, comparative fit Index (CFI), Tucker‐Lewis index (TLI), root mean square error of approximation, (RMSEA) and its associated 90% confidence interval (90% CI), Akaike information criterion (AIC) and Bayesian information criterion (BIC) (Hu & Bentler 1999, Schermelleh‐Engel et al. 2003). The significance‐level criterion for all statistical tests was set at α = 0·05, two‐tailed. The testing hypotheses were the following:
Figure 1.
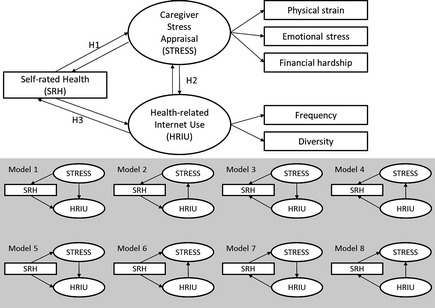
Hypothesized models and eight competing models.
H1: There is a significant relationship between caregiver stress appraisal and self‐rated health.
H2: There is a significant relationship between caregiver stress appraisal and health‐related Internet use.
H3: There is a significant relationship between self‐rated health and health‐related Internet use.
Two cases were dropped from the sem based on list‐wise deletion across all measured variables. This represented only 0·8% of the sample, thus no data imputation was conducted (Meyers et al. 2006). All statistical assumptions were checked including univariate/multivariate normality and linearity. No transformation was required to collect univariate normality, no outliers were found concerning multivariate normality and linearity. The final sample size in sem (N = 256) was deemed sufficient to conduct both CFAs and sems because there were 18 free parameters estimated in the sem and minimum required sample size was 200 (Loehlin 2004).
Ethical considerations
This study was a secondary analysis using de‐identified data without Health Insurance Portability and Accountability Act (HIPAA) identifiers. Exempt approval from the Institutional Review Board was obtained from the investigators' university and data use was approved by NAC/AARP.
Results
Sample characteristics in caregivers and their care recipients with dementia
Socio‐demographic and caregiving‐related information for the 258 caregivers and their care recipients is shown in Table 2. Persons with dementia were older adults (mean = 80·14, sd 13·20). The majority were women (68·6%) and living in home settings (52·7%). Approximately one‐fifth had Alzheimer's disease and lived with their caregivers. Dementia caregivers in our study were middle‐aged (mean = 51·95, sd 12·48), spent 28·51 hours per week on care‐giving tasks (sd 47·26) and had performed their care‐giving role for 4·89 years (sd 7·15) on average. The majority were female (64·0%), at least college‐level educated (60·5%) and not the primary caregiver (55%). Three quarters had household incomes greater than $30,000 yearly. Compared with other demographics (Toseland et al. 2002, National Family Caregivers Association & Family Caregiver Alliance 2006), our participants were more likely to be the dementia patients’ children (75·9%) rather than their spouses (3·9%); the sample in Toseland et al. (2002) consisted of 49·3% offspring and 37·0% spouses.
Table 2.
Socio‐demographic characteristics of caregivers and their care recipients with dementia (N = 258).
| Description of persons with dementia | |
| Age, Mean (SD) | 80·14 (13·20) year |
| Gender, N (%) | |
| Female | 177 (68·6%) |
| Types of dementia | |
| Alzheimer's disease | 40 (15·5%) |
| Non‐Alzheimer's disease | 218 (84·5%) |
| Resident status, N (%) | |
| Home setting | 136 (52·7%) |
| Living with the caregiver | 56 (21·7%) |
| Description of their caregivers | |
| Age (year), Mean (SD) | 51·95 (12·48) year |
| Time spent for caregiving per week, Mean (SD) | 28·51 (47·26) hours |
| Duration of caregiving, Mean (SD) | 4·89 (7·15) years |
| Gender, N (%) | |
| Female | 165 (64%) |
| Primary caregiver, N (%) | |
| Yes | 116 (45%) |
| Relationship with persons with dementia as, N (%) | |
| Spouse | 10 (3·9%) |
| Parent | 8 (3·1%) |
| Child or grandchild | 196 (75·9%) |
| Relative | 24 (9·3%) |
| Friend/ non‐relative/ neighbour | 19 (7·4%) |
| Missing | 1 (0·4%) |
| Education, N (%) | |
| High school or less | 102 (39·5%) |
| Some college or higher | 156 (60·5%) |
| Household income, N (%) | |
| Less than $30,000/year | 38 (14·7%) |
| $30,000/year or more | 193 (74·8%) |
| Missing data | 27 (10·5%) |
| Subjective responses of care‐giving stress, Mean (SD) | |
| Physical strain | 2·41 (1·27) |
| Emotional stress | 3·20 (1·21) |
| Financial hardship | 2·96 (0·76) |
| Health status, Mean (SD) | 3·62 (1·05) |
| Diverse types of Internet use, Mean (SD) | 2·73 (1·61) |
| Frequency of Internet use, N (%) | |
| Often | 70 (27·1%) |
| Sometimes | 108 (41·9%) |
| Rarely | 80 (31·0%) |
Measurement model testing
All correlation coefficients of measured variables were summarized in Table 1. The CFA provided a good fit to the observed data for the latent constructs of caregiver stress appraisal and health‐related Internet use (Loehlin 2004). For model specification, regression weights were constrained with 1 on two paths: (1) from caregiver stress appraisal to physical strain; and (2) from health‐related Internet use to frequency of use. Measurement model analyses showed that caregiver stress appraisal and health‐related Internet use had one dimension with the following fit indices. Model fit indices of the confirmatory factor analysis of caregiver stress appraisal included: χ2 (3, N = 256) = 107·46, P < 0·01; CFI = 1·00; TLI = 1·00; RMSEA < 0·01. All factor loadings of the observed variables were significant (P < 0·001), suggesting that the latent variables were well represented by their respective observed indicators. In addition, model fit indices of the confirmatory factor analysis of health‐related Internet use included: χ2 (1, N = 256) = 21·53, P < 0·01; CFI = 0·95; TLI = 1·05; RMSEA < 0·01. Two factor loadings of the observed variables were significant, suggesting that the latent variables were well represented by their respective observed indicators.
Structural model testing
sems were tested to compare 8 different models due to three possible bi‐directional relationships among caregiver stress appraisal, self‐rated health and health‐related Internet use (Figure 1). To select the best fit model, all model indices were compared and summarized in Table 3. Chi‐square statistics and most of model fit indices were identical among 8 models. However, Model 5 was chosen as the final models based on AIC and BIC results. Model 5's lowest AIC and BIC indices meant superior model fit compared with those of Models 1‐4 (Hu & Bentler 1999, Schermelleh‐Engel et al. 2003).
Table 3.
Summary of model fit indices.
| χ2(7, N = 256), P | CFI | TLI | RMSEA | 90% CI for RMSEA | AIC | BIC | |
|---|---|---|---|---|---|---|---|
| Good model fit is determined if the fit indices are: | Not significant | ≥0·95 | ≥0·95 | ≤0·06 | Smaller compared with others | Smaller compared with others | |
| Models 1–4 and 6–8 | 10·46 (d.f. = 7), 0·16 | 0·989 | 0·977 | 0·044 | 0·000, 0·095 | 4550·30 | 4621·20 |
| Model 5 (Final model) | 10·46 (d.f. = 7), 0·16 | 0·989 | 0·977 | 0·044 | 0·000, 0·095 | 3800·318 | 3864·13 |
CFI, comparative fit Index; TLI, Tucker‐Lewis index; RMSEA, root mean square error of approximation; CI, Confidence interval; AIC, Akaike information criterion; BIC, Bayesian information criterion.
The final model (model 5 in Figure 1) results indicated excellent model fit between hypothesized model and tested data, χ2 (7, N = 256) = 10·46, P = 0·16, CFI = 0·989, TLI = 0·989, RMSEA = 0·044 and 90% confidence interval around RMSEA < 0·001, 0·095 (Table 3). All conclusions were drawn from this model. Figure 2 displays interrelationships among caregiver stress appraisal, self‐rated health and health‐related Internet use. Higher caregiver stress appraisal was associated with poor self‐rated health (β = −0·36, P < 0·001) and more use of Internet for health and care‐giving purposes (β = 0·27, P < 0·001). However, there was no significant relationship between self‐rated health and health‐related Internet use (P = 0·70).
Figure 2.
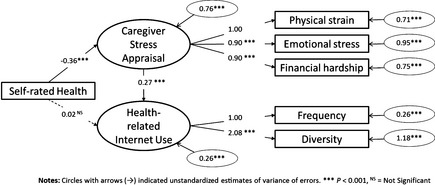
Final full structural equation model (sem). Circles with arrows (→) indicate unstandardized estimates of variance of errors. ***P < 0·001; NS, not significant.
Discussion
This study identified the relationships among caregiver stress appraisal, self‐rated health and health‐related Internet use based on the Stress Process Model (Pearlin et al. 1990). Higher levels of caregiver stress appraised were directly associated with a poor rating of health status, which is consistent with previous findings from dementia caregiver research (Pearlin et al. 1990, Elliott et al. 2010). Although dementia caregivers with higher levels of stress were more likely to engage in health‐related Internet use, this behaviour had no apparent relationship with their health status.
Stressed caregivers’ strong health‐related Internet use can be understood in terms of resource use as a coping strategy. Caregiver stressors are facilitators to use resource use as coping strategies. Dementia caregivers with higher levels of stress are more likely to use health and human services (Toseland et al. 2002), which facilitate their coping mechanisms in response to stressful situations during caregiving (Eysenbach 2003, Kinnane & Milne 2010). Stress occurs when there is an imbalance where the demands of individuals or the family exceed the existing capacity to cope (Lazarus & Folkman 1984). To resolve the recognized level of stress, individuals actively seek additional coping strategies to help them resolve the mismatch between demand and capability. Thus, the increased use of the Internet for health‐related purposes in stressed caregivers reflects their strong motivation to explore all possible coping strategies.
However, our study showed an insignificant relationship between health‐related Internet use on self‐rated health. First, dementia caregivers may consider health‐related Internet use as a new care‐giving task (Kinnane & Milne 2010) rather than a health promotion behaviour that supports their own health and well‐being. Second, self‐rated health may not be sufficiently sensitive to reflect the specific demands of caregivers related to Internet use. Thus, more diverse indicators in terms of health, well‐being and caregiving should be examined to understand the comprehensive effects of health‐related Internet use, such as improved self‐efficacy, confidence as a caregiver, or empowerment (Eysenbach 2003, Beauchamp et al. 2005). Third, Internet‐based strategies for caregivers may not always meet their needs, which vary considerably and change according to caring responsibilities over time (Kinnane & Milne 2010).
There are several clinical implications. First, healthcare providers should consider how best to integrate Internet‐based resources into their current practice (Eysenbach 2003, Powell et al. 2011). Previous researchers have suggested that health‐related Internet use should be seen as a supplement to existing health service provision rather than as a total replacement for it (Powell et al. 2011). Caregivers still preferred healthcare providers as their primary source of care and information and considered Internet‐based information and resources as secondary or adjunct sources (Eysenbach 2003, Kinnane & Milne 2010, Powell et al. 2011, Fox & Brenner 2012). Practitioners should therefore look for ways to maximize the benefits of Internet‐based resources in families dealing with dementia beyond simply listing useful Internet‐based resources. Assessing psychological stress should precede the design of tailored interventions across the disease and care‐giving trajectory.
Second, nurses should be aware of the unavoidable disadvantages and challenges inherent in many Internet‐based resources and strategies. Despite the advantages and benefits the Internet offers, its users often suffer from technical difficulties, inaccurate or low‐quality information, possible misuse or confusion and the overwhelming volume of information available (Eysenbach 2003, Lewis et al. 2010, Powell et al. 2011). Nurses are often responsible for guiding dementia caregivers to qualified resources, educating them in how to use them effectively and regularly monitoring how Internet‐based strategies are impacting their care‐giving trajectory (Kinnane & Milne 2010). Quality assurance is also important to ensure consumer satisfaction and positive outcomes and thus encourage greater use of online resources (Toseland et al. 2002).
Study Limitations and Future Directions
As our findings are based on self‐reported, cross‐sectional survey data with convenience sampling, this study inevitably suffers from limited inference of causality and generalizability as well as possible responder bias. Thus, future studies are highly recommended to adopt a longitudinal design using more comprehensive measurements of caregiver stress and Internet use. More detailed information of Internet use and health indicators will provide a better in‐depth understanding of how each type of Internet use influences specific outcomes in caregivers.
Conclusion
This study provides a better understanding of health‐related Internet use in dementia caregivers in the United States. Our findings will contribute to efforts to develop more effective Internet‐based interventions and outcome measures.
Our results highlight that the higher the levels of self‐appraised caregiver stress facilitate greater health‐related Internet use. However, greater Internet use does not appear to be related to dementia caregiver's health status.
Internet‐based resources could be a secondary adjunct to be used alongside conventional healthcare services in current practice regarding both actual and virtual healthcare use.
Health care providers, including nurses specifically, are responsible for providing guidance or recommendations for specific, high‐quality, Internet‐based resources that meet caregivers’ health and psychological needs.
Conflict of interest
No conflict of interest has been declared by the authors.
Author contributions
All authors have agreed on the final version and meet at least one of the following criteria [recommended by the ICMJE (http://www.icmje.org/ethical_1author.html)]:
substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data;
drafting the article or revising it critically for important intellectual content.
Acknowledgements
The authors appreciate the generosity of the NAC/AARP in allowing use of their data published in 2010. The data (electronic) from the NAC/AARP's National Caregiver survey are available to non‐profit research organizations and individuals and de‐identifiable for public use at no charge.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
References
- Beauchamp N., Irvine A.B., Seeley J. & Johnson B. (2005) Worksite‐based Internet multimedia program for family caregivers of persons with dementia. Gerontologist 45(6), 793–801. [DOI] [PubMed] [Google Scholar]
- Beeber A.S., Thorpe J.M. & Clipp E.C. (2008) Community‐based service use by elders with dementia and their caregivers. Nursing Research 57(5), 312–321. [DOI] [PubMed] [Google Scholar]
- Chou W.Y., Liu B., Post S. & Hesse B. (2011) Health‐related Internet use among cancer survivors: data from the Health Information National Trends Survey, 2003‐2008. Journal of Cancer Survivorship 5(3), 263–270. [DOI] [PubMed] [Google Scholar]
- Elliott A.F., Burgio L.D. & Decoster J.J. (2010) Enhancing caregiver health: findings from the resources for enhancing Alzheimer's caregiver health II intervention. Journal of the American Geriatrics Society 58(1), 30–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eysenbach G. (2003) The impact of the Internet on cancer outcomes. CA: A Cancer Journal for Clinicians 53(6), 356–371. [DOI] [PubMed] [Google Scholar]
- Family Caregiver Alliance (2009) Caregiving issues and strategies: Caregiving in the U.S. Retrieved from http://www.caregiver.org/caregiver/jsp/content_node.jsp?nodeid=2313 on 30 November 2013. [Google Scholar]
- Fox S. (2012) Pew Internet: Health. Retrieved from http://pewinternet.org/Commentary/2011/November/Pew-Internet-Health.aspx on 1 December 2013. [Google Scholar]
- Fox S. & Brenner J. (2012) Family caregivers online. Retrieved from http://pewinternet.org/Reports/2012/Caregivers-online.aspx on 1 December 2013. [Google Scholar]
- Hu L.T. & Bentler P.M. (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling 6(1), 1–55. [Google Scholar]
- Kinnane N.A. & Milne D.J. (2010) The role of the Internet in supporting and informing carers of people with cancer: a literature review. Supportive Care in Cancer 18(9), 1123–1136. [DOI] [PubMed] [Google Scholar]
- Lazarus R.S. & Folkman S. (1984) Stress, Appraisal and Coping. Springer, New York. [Google Scholar]
- Lewis M.L., Hobday J.V. & Hepburn K.W. (2010) Internet‐based program for dementia caregivers. American Journal of Alzheimer's Disease & Other Dementias 25(8), 674–679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loehlin J.C. (2004) Latent Variable Models: An Introduction to Factor, Path and Structural Equation Analysis, 4th edn Lawrence Erlbaum Associates, Mahwah, NJ. [Google Scholar]
- Marziali E. & Garcia L.J. (2011) Dementia caregivers’ responses to 2 Internet‐based intervention programs. American Journal of Alzheimer's Disease & Other Dementias 26(1), 36–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyers L.S., Gamst G. & Guarino A.J. (2006) Applied Multivariate Research: Design and Interpretation, 1st edn Sage Publications Inc, Thousand Oaks, CA. [Google Scholar]
- Mittelman M.S., Roth D.L., Clay O.J. & Haley W.E. (2007) Preserving health of Alzheimer caregivers: impact of a spouse caregiver intervention. American Journal of Geriatric Psychiatry 15(9), 780–789. [DOI] [PubMed] [Google Scholar]
- National Alliance for Caregiving, American Association of Retired Persons (NAC/AARP) (2009a) Caregiving in the U.S: Executive summary. Retrieved from http://www.caregiving.org/data/2009Caregiving_Appendix_B_Detailed_Methodology.pdf on 15 May 2013.
- National Alliance for Caregiving, American Association of Retired Persons (NAC/AARP) (2009b) Caregiving in the U.S. 2009 – Appendix A: Full questionnaire. Retrieved from http://www.caregiving.org/pdf/research/2009Caregiving_Appendix_A_Full_Questionnaire.pdf on 15 May 2013.
- National Family Caregivers Association & Family Caregiver Alliance (2006) Prevalence, Hours and Economic Value of Family Caregiving, Updated State‐by‐state Analysis of 2004 National Estimates (by Peter S. Arno, PhD). NFCA/FCA, Kensington, MD/San Francisco, CA. [Google Scholar]
- National Telecommunications and Information Administration (2011) Exploring the Digital Nation‐computer and Internet Use at Home. Retrieved from http://www.ntia.doc.gov/files/ntia/publications/exploring_the_digital_nation_computer_and_internet_use_at_home_11092011.pdf on 15 October 2013.
- Pearlin L.I., Mullan J.T., Semple S.J. & Skaff M.M. (1990) Caregiving and the stress process: an overview of concepts and their measures. Gerontologist 30(5), 583–594. [DOI] [PubMed] [Google Scholar]
- Powell J., Chiu T. & Eysenbach G. (2008) A systematic review of networked technologies supporting carers of people with dementia. Journal of Telemedicine and Telecare 14(3), 154–156. [DOI] [PubMed] [Google Scholar]
- Powell J., Inglis N., Ronnie J. & Large S. (2011) The characteristics and motivations of online health information seekers: cross‐sectional survey and qualitative interview study. Journal of Medical Internet Research 13(1), e20. doi:10.2196/jmir.1600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qiu C., Kivipelto M. & von Strauss E. (2009) Epidemiology of Alzheimer's disease: occurrence, determinants and strategies toward intervention. Dialogues in Clinical Neuroscience 11(2), 111–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schermelleh‐Engel K., Moosbrugger H. & Muller H. (2003) Evaluating the fit of structural equation models: tests of significance and descriptive goodness‐of‐fit measures. Methods of Psychological Research 8, 23–74. [Google Scholar]
- Schulz R. & Sherwood R.R. (2008) Physical and mental health effects of family caregiving. American Journal of Nursing 108(Suppl. 9), 23–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toseland R.W., McCallion P., Gerber T., Dawson C., Gieryic S. & Guilamo‐Ramos V. (1999) Use of health and human services by community‐residing people with dementia. Social Work 44(6), 535–548. [DOI] [PubMed] [Google Scholar]
- Toseland R.W., McCallion P., Gerber T. & Banks S. (2002) Predictors of health and human services use by persons with dementia and their family caregivers. Social Science & Medicine 55(7), 1255–1266. [DOI] [PubMed] [Google Scholar]
- Ware J.E. & Sherbourne C.D. (1992) The MOS 36‐item short‐form health survey (SF‐36). I. Conceptual framework and item selection. Medical Care 30(6), 473–483. [PubMed] [Google Scholar]
- Zarit S.H. (2006) Assessment of family caregivers: A research perspective. Caregiver assessment: Voices and views from the field. Report from a national consensus development conference (Vol.II). Family caregiver alliance, San Francisco, CA. [Google Scholar]