

Abstract
Based on the demographic changes and the rapid increase of older population in Europe, major challenges are expected to rise, both in the economy as well as the society, whether the dominant care model for supporting elderly in living independently at home continues to rely on informal and formal caregivers’ assistance. To respond to the above challenges, assistive technologies are called to develop Information and Communication Technology (ICT) services for supporting seniors to remain active and independent, for as long as possible, in their chosen home environment. The work described in this Letter is based on the Miraculous-Life project and it emphasises the identification and assessment of a set of services that an ICT system for Ageing Well should support, in an actual end-users setting. The outcome of this work may inform fellow researchers and other projects in the area of Ageing Well in: (i) understanding which ICT services can be the most valuable for end-users’ Quality of Life, (ii) prioritising the development of related ICT services and (iii) facilitating better recourse allocation in order to reduce any risks associated to implementation failures of these services within their respective projects. A final trial phase is planned, aiming to validate the Miraculous Life prototype longitudinally in a naturalistic environment with a larger sample size. During this trial, it will be investigated if perceived usefulness, satisfaction and motivation could be predicted by sociodemographic variables and personality.
Keywords: geriatrics, telemedicine, patient care
Keywords: ICT services, Information and Communication Technology, active ageing, independent living, older population, Europe, elderly people, Miraculous-Life project, quality of life, recourse allocation, sociodemographic variables, personality
1. Introduction
The demographic changes of older population in Europe (aged 65 and above) anticipate the life span to increase considerably by 2050 [1]. Although this is a positive statistic, it does not necessarily means that increasing the length of living will imply a healthier, more active and independent life [2]. Currently, informal (i.e. relatives, friends etc.) and formal (care professionals) caregivers are the major components of the care model that provides assistance and support to the elderly community in European countries. This model is expected to pose major problems both in the economy as well as the society. Thus, further research is needed on building solutions for meeting the higher demand for health care, by adjusting European health systems to what can be considered as essential for the ageing population.
Along this endeavour, there is growing attention from public and private organisations for assistive technological solutions to support older adults live independently and actively, at home. Information and Communication Technology (ICT) for Ageing Well are aiming to promote ‘Positive Ageing’, by monitoring and maintaining safety and enhancement of health and psychological well-being of elders. Positive Ageing aims to develop and take a well-adjusted approach for addressing the opportunities and challenges of an ageing society rather than perceiving the increase in longevity as a burden and a threat.
This Letter is driven by the work done in Miraculous-Life (ML) [ML for Elderly Independent Living at http://www.miraculous-life.eu/] project and specifically on the identification and evaluation of a set of ICT services that a system promoting ‘Positive Ageing’ should support (Section 4). Furthermore, this is an extension of our previous work [3] which evaluated a set of services in terms of usefulness and technical feasibility alone (Sections 5.1 and 5.2). Here, a prototypical system of ML has been evaluated for Perceived Usefulness, User Satisfaction and Motivation of use (Section 5.3), with real end users from two organisations: MRPS in Geneva (Switzerland) and ZUYDELAND in Sittard (The Netherlands); where elderly live and manage their everyday activities with the most possible independence.
Section 2 provides an overview of what are considered as important areas of focus when designing support for improving elderly QoL followed by Section 3 that focuses on ICT for aging well. Section 4 will introduce a list of ICT services considered as important and Section 5 will provide a multi-level evaluation of those services. Section 6 concludes this Letter.
2. Elderly well-being
Several studies have been performed over the years on identifying what is important for elderly well-being. A recent review [4] shows that health behaviour, psychology and physiology, as well as other risks appear in the life of elderly.
Social isolation affects their quality of life (QoL) and increases their dependability on formal or informal caregivers. Health behaviour is affected mainly due to the influence that the social network of an elderly has on his/her everyday health decisions, e.g. medicine intake (reminders), adherence to medical treatment and so on. Malnutrition is a health alarming factor for elderly. Either due to mobility problems, or forgetfulness, or sometimes depression, aged people tend to skip important meals or eat unhealthy during the day. In addition, the physiology of the person deteriorates, due to lack of social interaction. Elderly stop being active and refrain from activities that they previously used to enjoy. This results in deterioration of mobility and creates a sense of low self-esteem that drives a person to further isolation that can be grown into depression [5]. Helping elderly to remain active might only requires educating them accordingly on the negative effects that refraining from activity and movement can have to their health.
On the other hand, social participation proved to affect positively their well-being and QoL, but is significantly reduced as people age [6]. Since, active aging occurs through relationships with others, e.g. friends and relatives who provide constant aid and support [7], social participation is an important aspect in this context.
3. ICT technologies and ageing
ICTs are being taken up by the health and social care markets as profitable solutions in terms of provision and efficiency [8]. There are several application contexts that have already been explored on supporting elderly, e.g.: (i) at the work context [9], by motivating them to stay productive for longer and experience better quality of work and social life balance, (ii) in the community, creating and maintaining their social contacts thus, overcoming isolation and loneliness, (iii) accessing public and private services and (iv) at home [10] by providing needed support for specific everyday tasks and activities for stimulating their independence, autonomy and dignity.
When it comes to the design and development of ICT services for active and autonomous living [11] the specific needs and requirements of the elderly users have to be prioritised in order to make sure that accessibility and usability are considered (e.g. due to their limited ability to hear, see or to control ICT devices). Similarly, the demographic differences and prospects of the elderly have to be taken into account. Experts in the field have developed several intervention mechanisms to support psychological well-being that proved to help elderly stay socially involved, increase their social circle and socialise with like-minded people. In addition, referring older adults to social activities can help avoid social isolation and will also keep the mental and physiological state of a person at a better state. These interventions can either be generated by caregivers manually or through technological support.
Several studies have also shown that the perception of social support can benefit health beyond actual received support. In this line, Ring et al. [12] show that proactive support has more positive effects on loneliness and depression scores of elderly, than passive support may have.
The above-mentioned establishes the drive for the study presented in this Letter, which aims to identify and evaluate a specific set of ICT services (social, daily activities to leisure, education, guidance, physical exercise, medication and safety). Sections 4 and 5 present the results of this study, stressing the importance and effect of the proposed ICT services in the QoL of the elderly, but also their caregivers.
4. Identification of a set of ICT services for ageing well
This study included the identification and understanding of the specific problems, needs and demands of elderly people regarding active and independent living. A requirements extraction and analysis methodology was performed in two levels: (i) literature study (e.g. Section 2); and (ii) quantitative and qualitative approaches involving real end users [3] (e.g. Sections 5.1 and 5.2).
Especially important was the qualitative data collection methods used. Structured interviews and focus groups, with the elderly and the formal and informal caregivers, have been employed, for refining or defining any new requirements that were unintentionally neglected. The overall collection of requirements was interpreted into a set of 20 ICT services (Table 1).
Table 1.
High valued ICT services for Ageing Well. Table is adapted from [3]
| Service | Description |
|---|---|
| S01. Contact Assistance | Assists the elderly to create and maintain a contact list, view their contact details and means to communicate. |
| S02. Messaging | Enables the management, organisation and communication of messages between the users. It facilitates communication, between the elderly, his/her contacts, and other users of the system. |
| S03. Shopping Assistance | Assists the elderly to create (by adding or removing items) a suitable shopping list and send the list to the (informal) caregiver to buy the missing items. |
| S04. Medication Service & Reminders | Provides medical information related to medicine associated with an elderly such as name, description, dose, frequency that a medication should be taken and route of medicine. Based on this information the system reminds, at a set times, the elderly to take his/her medication. |
| S05. Wake-up Calls | Assists the elderly to set the wake up alarms at a specific time they want to wake up (can be set for a day, weekends, weekdays etc.) and trigger the alarm clock at the specified times. |
| S06. Periodic Advice | Provides periodic advices, written by caregivers, or animators, that are periodically provided to the elderly by the system to improve the health of the elderly. |
| S07. Fall Detection & Alerting | Detects a fall event of the elderly and alert the appropriate persons (emergency contacts) in case of need. |
| S08. Dangerous Objects Adviser | Detects dangerous objects, e.g. on the floor that could potentially cause injury. Warns the elderly for obstacles, reducing the risk of fall. |
| S09. Dangerous Situations Adviser | Reminds and warns the elderly of dangerous or highly risk activities/situations that can result an injury. For example, if the system detects that the elderly is preparing a meal, after cooking it reminds him/her to switch off the stove/oven. |
| S10. Call for Help & Alerting | After a ‘Call for Help’ voice command from the elderly, the system alerts the appropriate persons (emergency contacts) in case of need. |
| S11. Windows Monitoring | Monitors the windows and reminds the elderly, after they wake up in the morning to open the windows for having fresh air, and close the windows before they go to bed, if the elderly forgets it. |
| S12. Go to bed reminder | Detects if the elderly is not in the bed during the night. If the user is not detected in the bed, the system suggests him/her to go to sleep (at a set time based on his daily pattern). |
| S13. Agenda Service | Keeps track of certain activities related to an elder. In particular, it provides details regarding agenda items that an elder should consider and/or attend. Also, the elderly can create social activities and invite friend or relatives to join activities. |
| S14. Event/Group activities | Provides information about events or group leisure activities organized by the institution or in the city, which the elderly can consult and subscribe to participate. It also allows the elderly to invite other members to participate. |
| S15. Appointment reminder | Reminds the elderly of his/her and pre-scheduled activities before the events begins. |
| S16. Object Location Assistance & Reminder | Assists the elderly on locating ‘forgotten’ objects at home, with the help of sensors, and help them retrieve them. If the system fails in locating the object lost, it will provide reminders to the elderly where they normally put their personal items so that they can find them easier. |
| S17. Notifications | A general group of messages written by caregivers, animators etc. and sent to the elderly by the system. |
| S18. Meal preparation Assistance | Provides information regarding meals, their recipe, the ingredients, and assist/teach the elderly to prepare the meal, by providing oral guidance. Also the recipes provided to the elderly by this service consider the dietary requirements and allergies of the elderly (e.g. allergies). |
| S19. Motivation for Physical Activity | Detects if the elderly is not performing sufficient physical activity, and motivates him/her, based on his profile (e.g. physical activity preferences, health status, disabilities etc.) in performing physical activities/exercises. |
| S20. Physical Activity Service | Guides the elderly during undergoing their physical exercises. E.g. the elderly can watch short video clips demonstrating physical exercises suggested by a physiotherapist that he/she can perform at home based on his/her profile (e.g. preferences, health status, disabilities etc.). |
Prior to the implementation of these services, usefulness and technical evaluations were performed in order to identify which of these services are important for the end-users and also what are the involved technical risks in the implementation of those services. The outcome of this initial evaluation resulted in a sub-set of the selected services to be implemented and tested through a prototype system with real end-users (Section 5.3).
5. Assessment of selected ICT services
The evaluation of the proposed services (Table 1) consists of three stages, each with a different purpose, but with the goal to identify which services would be more useful and suitable to be developed in an ICT system for elderly support. (i) First, we performed an analysis of the relevance that these services have to the QoL of end users (Section 5.1). (ii) Second, the technical feasibility, technical constraints and the risks (and thus the ‘cost’) associated to the development of the services was assessed (Section 5.2). (iii) Finally, selected services were built in a prototype system and evaluated with real end users (Section 5.3).
For the first two stages, questionnaires were administrated to caregivers/professionals and elderly of both MRPS and ZUYDERLAND. Participants were asked to rate each service by using a 10-point Likert scale (not useful – essential). The MRPS and ZUYDERLAND participated in this analysis, with seven (7) elderly people each and nine (9) and fourteen (14) caregivers, respectively.
5.1. Usefulness and impact assessment
The ranking and the impact analysis of the ICT services according to the participated caregivers and elderly population is presented in [3]. Consistently with related work presented in Sections 2 and 3, the outcomes illustrate that both end-users appreciate services that improves safety and quality in elderly care and stimulate socialisation and communication (ranked as essential or very useful). This was anticipated since these services provide the elderly with assurance of being attended, protected, cared-for and also increase their social interaction. Therefore, they become motivated to continue their active and autonomous life at home. As a consequence, care-stress is reduced for the formal and informal caregivers.
We were further interested in exploring any cultural differences that might occur between the two organisations MRPS and Zuyderland since they operate in two different European countries, Switzerland and Netherlands, respectively. Thus, we grouped the data collected from elderly and caregivers at MRPS and Zuyderland to form two datasets, one for each organisation. An independent sample t-test analysis was applied to the data. The results (Table 2) show strong significance (p < 0.05, in bold) in some cases and marginal significance in others, with MRPS elderly and caregivers assessing significantly higher half of the suggested ICT Services.
Table 2.
Independent sample t-test analysis between the two organisations involved
| Service | N Zuyderland | N MRPS | Mean Zuyderland | Mean MRPS | SD Zuyderland | SD MRPS | t-value | df | p |
|---|---|---|---|---|---|---|---|---|---|
| S04 | 21 | 18 | 7.28 | 8.64 | 2.66 | 1.89 | −1.80 | 37 | 0.08 |
| S05 | 21 | 18 | 6.80 | 8.13 | 1.69 | 1.95 | −2.27 | 37 | 0.02 |
| S06 | 21 | 18 | 6.52 | 8.02 | 1.80 | 2.515 | −2.16 | 37 | 0.03 |
| S07 | 21 | 18 | 8.23 | 9.55 | 1.89 | 1.25 | −2.51 | 37 | 0.01 |
| S11 | 21 | 18 | 5.42 | 7.63 | 2.13 | 1.92 | −3.37 | 37 | 0.00 |
| S13 | 21 | 18 | 6.76 | 8.30 | 2.23 | 1.72 | −2.38 | 37 | 0.02 |
| S14 | 21 | 18 | 7.04 | 8.41 | 2.22 | 1.47 | −2.22 | 37 | 0.03 |
| S15 | 21 | 18 | 7.04 | 9.08 | 2.20 | 0.80 | −3.70 | 37 | 0.00 |
| S17 | 21 | 18 | 6.66 | 7.91 | 2.43 | 1.96 | −1.74 | 37 | 0.08 |
| S18 | 21 | 18 | 4.90 | 6.36 | 2.73 | 2.28 | −1.78 | 37 | 0.08 |
In an attempt to give context to these results, we employed the Hofstede Centre model [13] that proposes six dimensions of cultural values: power distance index, individualism versus collectivism, masculinity versus femininity, uncertainty avoidance index, pragmatic versus normative, and indulgence versus restraint.
Netherland and Switzerland, where the two organisations involved in this study are based, demonstrate similarities in all cultural values, except from masculinity/femininity scale. Switzerland appears as a masculine society (i.e. characterised by competition, achievement and success), and the Netherlands appears as a feminine society (i.e. characterised by caring for others and QoL). The caring value of Dutch might show that Dutch elderly are possibly expecting from family and friends to cover their needs in a caring society, whether Swiss elderly are more independent and find the services provided more useful for keeping their independence. The results of this cultural analysis show evidences that potentially explain how Swiss and Dutch end-users assessed the ML system services in the dimensions of usefulness and impact.
5.2. Technical assessment
To evaluate the technical perspective (e.g. to identify any technical constrains and risks that might appear during development) and understand the technical ‘cost’ of each service, the technical partners involved in the development have been called to analyse the services and assess, their technical feasibility. The summary of the technical perspective analysis is presented in Table 3 and in [3].
Table 3.
Summary of technical perspective analysis of identified ICT services. Adapted from [3]
| Services | Technical feasibility |
|---|---|
| S02, S04, S05, S06, S09, S12, S13, S14, S15, S17, S18 | Feasible with not any shortcomings. |
| S01, S03, S10, S11, S20 | Feasible, but a small number of shortcomings are present. |
| S07, S08, S16, S19 | Feasible, but a number of shortcomings are present. |
5.3. End-user prototype evaluation
Three testing phases were performed on months 8, 16 and 24 of the ML project in a controlled environment; aiming to validate the selected services, evaluate the robustness of the system and assess the end-users’ acceptance in terms of perceived usefulness, satisfaction and motivation of use. Different services were tested on the three different trials (see Table 4).
Table 4.
Services evaluated at different trials
| Trial | Services evaluated |
|---|---|
| first trial | Agenda Service (S13), Appointment Reminder (S15), and Object Location Assistance & Reminder (S16) |
| second trial | Medication Service & Reminders (S04), Wake-up Calls (S05), Periodic Advice (S06), Fall Detection & Alerting (S07), Call for Help & Alerting (S10), Agenda Service (S13), Event/Group activities (S14), Appointment Reminder (S15), Object Location Assistance & Reminder (S16), Notifications (S17) |
| third trial | Contact Assistance (S01), Messaging (S02), Fall Detection & Alerting (S07), Dangerous Objects Adviser (S08), Dangerous Situations Adviser (S09), Call for Help & Alerting (S10), Physical Activity Service (S20) |
5.3.1. Methods
End-users – including both seniors and caregivers – were asked to perform specified tasks with the ML prototypes and express their thoughts, observations, feelings; aiming to capture the cognitive processes of the users based on the Think Aloud Protocol approach [14]. The data collected at this point allowed for usability problems to be identified. Scenarios were presented to the participants in a printed format – e.g. ‘you are suffering from a strong headache. Use the service ‘emergency’ in order to ask help from caregivers’, ‘use the message system service in order to (i) check some of the messages you received, (ii) write a new message to one of your friends’. A coding scheme was also developed in order to note the verbal and non-verbal behaviour of the user during the testing phase. When needed, investigators also provided assistance to the users.
At the end of the user testing phase, the participants were asked to fill in questionnaires for measuring in a Likert scale (from −3 to 3) the perceived usefulness, satisfaction, and the motivation in using the ML solution. The usefulness and the satisfaction questionnaire were administered in all three testing phases, while the motivation questionnaire was administered in the second and third testing phases. The list of questions can be found in Table 5. The averages were calculated for each participant and for each questionnaire, allowing thus to compute general means for the two groups. Finally, we estimated the portion of participants (i) who perceived the system as useful, (iii) satisfied by the system and (iii) motivated in using the system by calculating the proportion of participants who obtained a mean higher than 0 in each scale.
Table 5.
Usefulness, satisfaction and motivation questionnaire administered to elderly and their caregivers
| Perceived usefulness |
| I Think that the system could: |
| A1) help me to be more effective in carrying out my daily activities. |
| A2) give me more control over the activities/tasks in my daily life. |
| A3) make me feel less stress by making use of the system for managing my daily activities/tasks. |
| A4) help me to complete my daily activities/tasks quickly. |
| A5) help me to complete my daily activities/tasks more easily. |
| A6 make me feel more motivated to carry out my daily activities/tasks. |
| A7) make me feel safer in carrying out my daily activities/tasks. |
| A8) help me be more active (i.e., participate in more activities). |
| A9) improve my ability to perform my daily activities/tasks. |
| A10) help me be more independent/autonomous. |
| A11) help to reduce my demand for care from my carers. |
| A12) save me time when I use it. |
| Motivation |
| B1) I intend to use the services provided by the system in the future. |
| B2) I predict I would use the services provided by the system in the future. |
| B3) I plan to use the services provided by the system in the future. |
| Satisfaction |
| C1) I am satisfied with how easy it is to use this system. |
| C2) The system is pleasant to use. |
| C3) The system works the way I want it to work. |
| C4) I feel comfortable using the system. |
| C5) The interface of this system is pleasant. |
| C6) I like using the interface of this system. |
| C7) I feel I can trust the system. |
| C8) Overall I am satisfied with this system. |
5.3.2. Population
The ML prototypes were tested in the two end users’ institutions: Zuyderland and MRPS. Prior to participation, all seniors signed an informed consent form. The main characteristics of the samples are described below:
First trial: seven MRPS seniors (four females, three males; age = 81.71 ± 4.79), seven Zuyderland seniors (five females, two males; age = 81.71 ± 4.79), two MRPS caregivers (two females; nurse and nursing auxiliary), and two Zuyderland caregivers (two females; occupational therapist, care coordinator).
Second trial: nine MRPS seniors (seven females, two males; age = 82.11 ± 4.26), seven Zuyderland seniors (five females, two males; age = 81.71 ± 4.79), three MRPS caregivers (two females, one male; care coordinator, nurse, and nursing auxiliary), and two Zuyderland caregivers (two females; occupational therapist, and care coordinator).
Third trial: seven MRPS seniors (five females, two males; age = 83.86 ± 3.67), eight Zuyderland seniors (six females, two males; age = 82.5 ± 5.07), two MRPS caregivers (two females; nurse, and nursing auxiliary), and two Zuyderland caregivers (two females; occupational therapist, and care coordinator).
5.3.3. Results
Table 6 summarises the results gathered on the questionnaires. The general impression of end-users related to the system is positive: the prototypes were appreciated by both groups of end-users; especially in the first and third trials. During the second trial, the prototype revealed stability problems. This may explain why in the second trial we obtained lower results than in the first and third trials – see also Fig. 1.
Table 6.
Summary of results gathered from the questionnaires
| Indicator, group | First trial | Second trial | Third trial |
|---|---|---|---|
| usefulness, seniors | mean = 1.21 ± 0.85 | mean = −0.44 ± 1.59 | mean = 0.28 ± 1.84 |
| useful = 86% | useful = 53% | useful = 57% | |
| usefulness, caregivers | mean = 1.92 ± 0.14 | mean = 1.10 ± 1.20 | mean = 1.50 ± 1.13 |
| useful = 100% | useful = 80% | useful = 75% | |
| satisfaction, seniors | mean = 1.50 ± 0.99 | mean = 0.55 ± 1.45 | mean = 1.05 ± 1.20 |
| satisfied = 86% | satisfied = 73% | satisfied = 79% | |
| satisfaction, caregivers | mean = 1.88 ± 0.76 | mean = −0.44 ± 1.15 | mean = 0.78 ± 1.80 |
| satisfied = 100% | satisfied = 50% | satisfied = 75% | |
| motivation, seniors | NA | mean = 0.53 ± 2.36 | mean = 1.18 ± 1.51 |
| motivated = 73% | motivated = 79% | ||
| motivation, caregivers | NA | mean = 1.00 ± 0.67 | mean = 2.78 ± 0.38 |
| motivated = 100% | motivated = 100% |
Fig. 1.
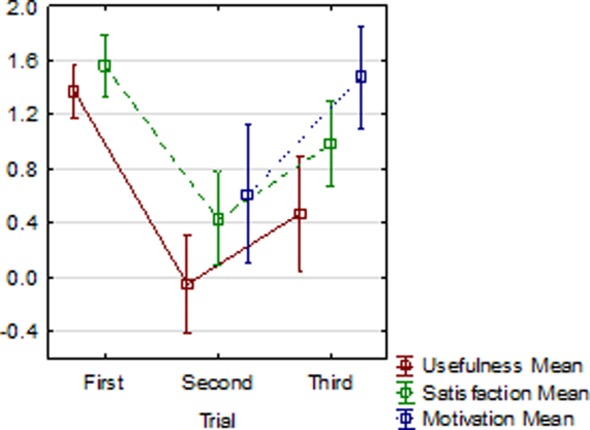
General averages of usefulness, satisfaction and motivation scales: seniors and caregivers combined. Vertical bars represent the standard error of the means. Scale range = [−3; 3]
Interestingly, seniors perceived the ML solution as being less useful than caregivers (p = 0.03), verifying also the results gathered in the costs–benefits analysis (see Section 5.2). The scores on the satisfaction and motivation scales should be considered as satisfactory at this stage of the project. These results are not different from what is continuously reported in the literature relating to the reluctance of elderly to deal with new technologies. In this study, the prototype system was also experiencing some stability and usability problems that might have affected the experience of the elderly. As a result, they would not be able to appreciate the benefits of the system in the same way as caregivers did. It is interesting to observe though, that the mean of satisfaction, usefulness and motivation (Fig. 1) are very low in the second pre-trial, but improve in the third pre-trial. This was due to the stability problems occurred during the second pre-trial.
Further analysis was run in the data collected to explore whether there are any differences between organisations in terms of the perceived usefulness, satisfaction and motivation. In this case, the caregivers’ and elderly’ replies considered as one group of data to represent the respective organisation and an independent-samples t-test was run to determine if there were differences between them. The test was run on the results of the three pre-trials separately and on the overall scores. In the first two pre-trials there were not any differences shown by the test between the two organisations. On the last pre-trial though the motivation scale shows marginal significant differences, p = 0.065 denoting MRPS's users being less motivated to use the system than Zuyderland's users. This is reflected also in the overall t-test, where we treated the results of the three pre-trials as one dataset for each organisation, where p = 0.028. This difference in motivation was not expected, but can be attributed to a number of reasons. First, the elderly and caregivers involved from MRPS have significantly less experience with ICT systems aiming at supporting their everyday needs. Although they perceived the services offered by the system as beneficial (see Section 5.1), the fact that they have used a partly functional prototype of the system, might not convinced them about its usefulness. On the other hand, Zuyderland elderly are much more experienced with ICT projects being developed within the organisation, allowing the elderly to appreciate the benefits of providing feedback for a system under development.
An additional correlation analysis was performed to assess the relationship between usefulness, motivation and satisfaction. There was significant positive correlation between the three parameters. Usefulness correlates with satisfaction (r = 0.34, p = 0.047) and motivation (r = 0.67, p = 0.000) and satisfaction also correlates with motivation (r = 0.54, p = 0.001). These results are very interesting and encouraging since they align with the technology acceptance model [15]. The model suggests that when a new technology is introduced to end-users, a number of elements influence their decision about how and when they will use it. These elements are the perceived usefulness and ease of use that will affect the motivation (attitude toward using) of a person to use a system, towards system usage and satisfaction. According to the results we obtained the strong correlations among these elements suggest that the users are keener to accept the provided technology than otherwise.
6. Conclusion
In this study, we have followed a holistic methodology for defining and assessing a set of services selected for supporting active and healthy aging at home. A literature review enlightened us with the important socio-physical and psychological aspects that need to be facilitated through a set of ICT services. The defined services have been assessed by elderly and caregivers involved in the study to reveal the most useful services from the pre-defined set. The results showed that both the elderly and caregiver users consider services that improve safety, motivation for daily activities, socialisation and communication as essential or very useful as they provide the elderly with assurance and motivation to continue their active life at home.
A technical feasibility analysis was performed by the technical partners involved in the ML consortium and a final ranking of the services is done based on the above assessment. The end-user study evaluated the most important services through a prototype system that ended to be consisted with the ranking of the services in terms of usefulness and technical assessment.
The outcome of this work may inform fellow researchers and other projects in the area of Ageing Well in: (i) understanding which ICT services can be the most valuable for end-users’ Quality of Life, (ii) prioritising the development of related ICT services, (iii) facilitating better recourse allocation in order to reduce any risks associated to implementation failures of these services within their respective projects and (iv) taking into consideration the cultural, organisational and environmental aspects into account when designing ICT systems for supporting elderly users.
On the downside, the three pre trials involved a small number of participants, thus the results should be taken with this factor in mind and cannot be generalised at the moment. However, the participants are potentially real end-users of the final system and their opinion is much appreciated and considered.
A final trial phase is planned aiming to validate the ML prototype longitudinally in a naturalistic environment with a larger sample size. During this trial, it will be investigated if perceived usefulness, satisfaction and motivation could be predicted by sociodemographic variables and personality.
7. Funding and Declaration of Interests
This work is supported by the ML project, funded by the European Commission under the 7th Framework Programme (Grant Agreement: 611421) and the GrowMeUp project, funded by the European Commission within the Horizon 2020 research and innovation programme - Societal Challenge 1 (Grant agreement: 643647). Conflict of interests: None declared.
8 References
- 1.World Economic Forum: ‘Global Population Ageing: Peril or Promise?’, Global Agenda Council on Ageing Society, 2012. available at http://www3.weforum.org/docs/WEF_GAC_GlobalPopulation Ageing_Report_2012.pdf
- 2.The 2015 Ageing Report: Economic and budgetary projections for the 28 EU Member States (2013-2060) available at http://ec.europa.eu/economy_finance/publications/european_economy/2015/pdf/ee3_ en.pdf
- 3.Christophorou C., Georgiadis D., et al. : ‘ICT systems and services for ageing well: identification and assessment of an important set (package) of ICT services for active ageing and independent living’. XIV Mediterranean Conf. on Medical and Biological Engineering and Computing 2016, 2016, pp. 897–902, Springer International Publishing [Google Scholar]
- 4.Nicholson N.: ‘A review of social isolation: An important but under assessed condition in older adults’, J. Primary Prev., 2012, 33, (2-3), pp. 137–152 (doi: ) [DOI] [PubMed] [Google Scholar]
- 5.Cole M.G., Dendukuri N.: ‘Risk factors for depression among elderly community subjects: a systematic review and meta-analysis’, Am. J. Psychiatry, 2014 [DOI] [PubMed] [Google Scholar]
- 6.Levasseur M., Richard L., et al. : ‘Inventory and analysis of definitions of social participation found in the aging literature: proposed taxonomy of social activities’, Soc. Sci. Med., 2010, 71, (12), pp. 2141–2149 (doi: ) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee H.Y., Jang S.N., et al. : ‘The relationship between social participation and self-rated health by sex and age: a cross-sectional survey’, Int. J. Nurs. Stud., 2008, 45, (7), pp. 1042–1054 (doi: ) [DOI] [PubMed] [Google Scholar]
- 8.Broek G.V.D., Cavallo F., Wehrmann C.: ‘AALIANCE ambient assisted living roadmap’ (IOS Press., 2010), vol. 6 [Google Scholar]
- 9.Belk M., Portugal D., et al. : ‘CogniMouse: on detecting users’ task completion difficulty through computer mouse interaction’. Proc. of 33rd Annual ACM CHI Extended Abstracts, 2015, pp. 1019–1024 [Google Scholar]
- 10.Santos L., Christophorou C., et al. : ‘Development strategy of an architecture for E-health personalised service robots’, IADIS Int. J. Comput. Sci. Inf. Syst., 2014, 9, (2) [Google Scholar]
- 11.Katrin G., Michael C.: ‘ICT enabled independent living for elderly’ (Institute for innovation and Technology, Germany, 2014), ISBN 978-3-89750-160-7 [Google Scholar]
- 12.Ring L., Barry B., et al. : ‘Addressing loneliness and isolation in older adults’ (Affective Computing and Intelligent Interaction, Geneva, 2013) [Google Scholar]
- 13.Hofstede G., Hofstede G.J., Minkov M.: ‘Cultures and organizations: software of the mind. Revised and expanded’ (McGraw-Hill USA, New York, 2010, 3rd edn.) [Google Scholar]
- 14.Lewis C., Rieman J.: ‘Task-centered user interface design’, A Practical Introduction, 1993 [Google Scholar]
- 15.Davis F.D., Bagozzi R.P., Warshaw P.R.: ‘User acceptance of computer technology: a comparison of two theoretical models’, Manage. Sci., 1989, 35, pp. 982–1003 (doi: ) [Google Scholar]