

Abstract
Hepatitis C recurrence continues to present a major challenge in liver transplantation (LT). Approximately 10% of hepatitis C virus (HCV)-positive recipients will develop fibrosing cholestatic hepatitis (FCH) after LT. FCH is clinically characterized as marked jaundice with cholestatic hepatic dysfunction and high titers of viremia. Pathologically, FCH manifests as marked hepatocyte swelling, cholestasis, periportal peritrabecular fibrosis and only mild inflammation. This progressive form usually involves acute liver failure, and rapidly results in graft loss. A real-time and precise diagnosis based on histopathological examination and viral measurement is indispensable for the adequate treatment of FCH. Typical pathological findings of FCH are shown. Currently, carefully selected combinations of direct-acting antivirals (DAAs) offer the potential for highly effective and safe regimens for hepatitis C, both in the pre- and post-transplant settings. Here, we review FCH caused by HCV in LT recipients, and current strategies for sustained virological responses after LT. Only a few cases of successfully treated FCH C after LT by DAAs have been reported. The diagnostic findings and therapeutic dilemma are discussed based on a literature review.
Keywords: Fibrosing cholestatic hepatitis, hepatitis C, liver transplantation, intractable ascites, portal hypertension
Introduction
In Japan, the United States and western Europe, chronic infection with hepatitis C virus (HCV) is the leading cause of death from liver disease and the leading indication for adult liver transplantation (LT) [1,2]. Reinfection of the allograft with HCV is inevitable in HCV-positive LT recipients [2], though this reinfection is avoidable if antiviral treatment accomplishes a sustained virological response (SVR) before LT. In a few cases, histopathological recurrence is minimal and non-progressive. However, disease course frequently evolves into cirrhosis with transplanted graft loss [2].
History of fibrosing cholestatic hepatitis (FCH)
FCH is an often fatal form of hepatitis B or C in patients receiving immunosuppressive treatment [1-3]. This condition was originally described in hepatitis B virus-infected recipients after LT [3]. The term FCH was first coined in 1991 to describe a severe and fulminant form of recurrent hepatitis B in LT recipients [4,5], although cases with similar presentations of clinical and pathological findings had been recorded earlier [6,7]. It has also been described using other names, such as “fibrosing cytolytic liver failure” [8] and “fibroviral hepatitis” [9].
FCH C after LT
Approximately 10% of HCV-positive recipients will develop FCH after LT [1,2,10,11]. FCH is clinically characterized as marked jaundice with cholestatic hepatic dysfunction and high titers of viremia [2]. Pathologically, FCH manifests as marked hepatocyte swelling, cholestasis, periportal peritrabecular fibrosis with mild inflammation [1-3]. This progressive form of disease usually involves acute liver failure, and rapidly results in graft loss after LT [1-3].
Conventional therapy with pegylated interferon (IFN) and ribavirin
A therapeutic goal of chronic HCV infection is a SVR that reflects HCV eradication [12]. Historically, treatments for recurrent hepatitis C have been limited by their low rate of success and high rate of side effects [1-3]. Until recently, the standard care for treatment of recurrent hepatitis C was combination therapy with IFN and ribavirin [1-3]. Dual therapy with these agents improved LT results [13]. However, this treatment induced a high rate of side effects, with an SVR rate of only approximately 30% [1,2]. Over the past few years, promising therapies with a high rate of SVR and lacking IFN have emerged for the treatment of hepatitis C [1,2]. Furthermore, these treatments have a lower incidence of side effects [1,2].
Advanced strategy with direct-acting antivirals (DAAs)
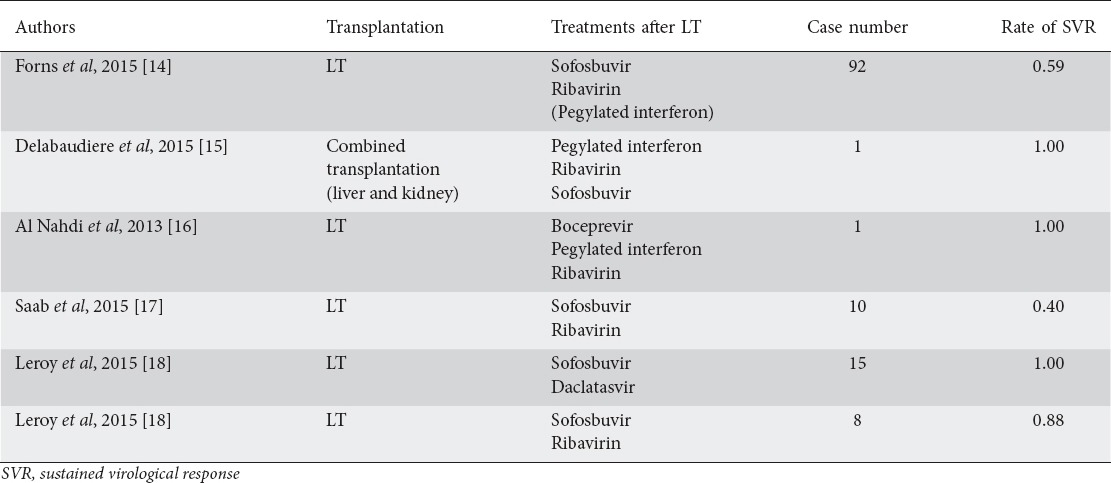
This review focuses on recent therapeutic advances and highlights areas of ongoing research. Therapeutic strategies against HCV have dramatically improved with the recent availability of DAAs including telaprevir, boceprevir, sofosbuvir, simeprevir, daclatasvir, ledipasvir, paritaprevir, ombitasvir, and dasabuvir [1,2,12]. Carefully selected combinations of these DAAs offer the potential for highly effective all-oral safe regimens even for patients with decompensated cirrhosis or LT recipients [12]. These treatments have become the standard care in the pre-transplant setting [1,2], and, moreover, have an expanding role for post-transplant patients [1,2,12]. To date, only a few cases of successfully treated FCH C after LT by DAAs have been reported [14-18] (Table 1).
Table 1.
Definitive diagnosis of fibrosing cholestatic hepatitis (FCH) C after liver transplantation (LT)
HCV viremia after LT
Allograft injuries caused by HCV viremia occur immediately after graft recirculation [19], and 95% of LT patients develop recurrent hepatitis C [2]. Acute infection with detectable HCV viremia manifests in approximately 60% of LT recipients [1,2,20]. HCV infection in LT recipients is characterized by high viral titers, characteristic histological changes, and variable transaminitis [1-3,21]. The levels of viremia are generally higher than before LT [22]. Recently, a novel non-invasive technique (hepatic elastography) was developed, which appears to correlate well with the stage of fibrosis. This technique can detect the degree of fibrosis (F≥2) from 6 months after LT, and has an excellent diagnostic capacity at 12 months after LT [23].
Definitive diagnosis of FCH C
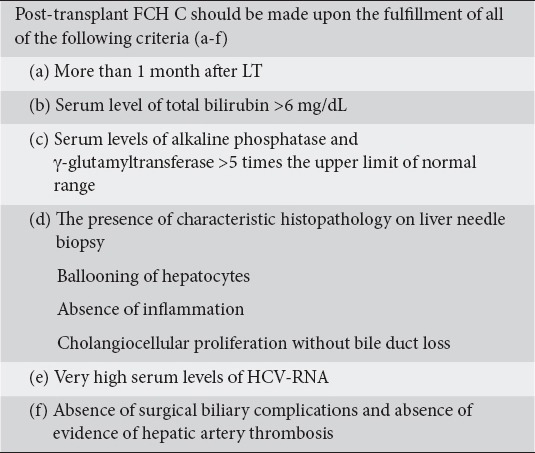
The diagnosis of FCH C is mainly made based on histopathological assessment [3,24]. Histopathological confirmation is necessary to establish a diagnosis of HCV recurrence, as well as enabling assessment of the degree of activity and a periodic follow up of disease progression [2,3]. This not only provides information about the prognosis, but also establishes the differential diagnosis with other complications, such as rejection, biliary disease or vascular obstruction [2,25,26]. The criterion of definitive diagnosis of FCH C after LT has been already established [1,27] (Table 2).
Table 2.
Successfully treated cases of fibrosing cholestatic hepatitis C after liver transplantation (LT) by direct-acting antivirals
Recurrent hepatitis C in LT recipients
The rate of fibrosis progression is not uniform, and may change over time [21]. Morbidity and mortality rates are increased in HCV-positive recipients, and both allograft and patient survivals are reduced in LT recipients with recurrent hepatitis C compared with HCV-negative recipients [1,2,21]. Severe recurrent hepatitis C can manifest in two ways: as a chronic recurrent hepatitis C or as aggressive FCH C [2,27]. From the viewpoint of a donor pool, recurrent hepatitis C puts further strain on the donor shortage [1], because HCV infection is responsible for approximately 30-40% of re-transplantations [1,2].
FCH usually does not occur until a couple of months after LT [3], although it can occur much earlier in re-transplanted recipients [6,7]. During the LT procedure, intraoperative blood loss is significant, and has a similar effect to phlebotomy on reducing HCV viremia [28]. However, it also decreases HCV antibody levels, which is not advantageous for HCV control. We have no conclusive opinion on the effect of intraoperative blood loss on the onset of recurrent hepatitis C.
Therapeutic strategies in LT recipients
Two therapeutic strategies for HCV can be adopted once the patient has received LT [1,2,29]. The aim of preemptive therapy is to eliminate HCV before the appearance of hepatic lesions [2,29]. The potential advantage of treating recipients at an early stage, usually from the first month after LT, is the absence of severe graft involvement or fibrosis [2]. However, during this stage, patients are still recovering from surgery and are receiving multiple drugs and high doses of immunosuppressants, thus they have a greater risk of rejection, so that postponing antiviral therapy is recommended [2,30,31]. Although this treatment is effective in 1-13% of cases, 35% of patients with this option require drug withdrawal because of intolerance or side effects [31]. Recipients with a history of aggressive infection or who are co-infected may be candidates for early treatment provided the presence of rejection is excluded.
However, treatment can be delayed until after recurrent hepatitis C, and this is the most widely used strategy. It involves initiating antiviral therapy once the histopathological consequences of recurrent hepatitis C have been detected by a histopathological investigation of the allograft [2,29]. In this later state, the recipient receives fewer immunosuppressants, and usually has a better clinical and analytical status, which permits antiviral treatment to be optimized and is efficient in 20-40% of cases [32-35]. Even so, approximately 30% of recipients require early withdrawal of the treatment, and approximately 70% require the dose of antivirals to be minimized [32-35]. This reduced exposure to the treatment, together with greater viral replication and unfavorable genotypes, explains the reduced treatment response compared with non-transplanted patients [36].
Thus, treatment strategies should be individualized, and should consider patient comorbidities (renal failure, hyperglycemia), graft function, history of rejection, and HCV characteristics [2,37]. As described above, therapeutic strategies after LT have changed from dual therapy with IFN and ribavirin [1-3] to DAAs without IFN [1,38].
Typical findings of FCH C in the transplanted allograft
Histopathological findings are characterized as lobular infiltrates, hepatocyte necrosis and fatty infiltration (Fig. 1). Hepatocyte ballooning and cholestasis are observed. Feathery degeneration of hepatic parenchyma caused by cholestasis is confirmed. Apoptotic hepatocytes were also observed. Increased numbers of inflammatory cells infiltrated into the periportal area, and piecemeal necrosis is observed. These damages result in the bridging fibrosis. During a recovery term from FCH C, apoptotic hepatocytes and inflammatory infiltration at the periportal area decreased, and finding of chronic hepatitis C which manifested as spotty and patchy necrosis. In this case, HCV-ribonucleic acid (HCV-RNA) level increased. Serum levels of aspartate transaminase, alanine aminotransferase, total bilirubin and γ-glutamyltransferase peaked as 157 U/L, 311 U/L, 19.2 mg/dL and 269 U/L, respectively. Direct bilirubin was dominant for jaundice.
Figure 1.
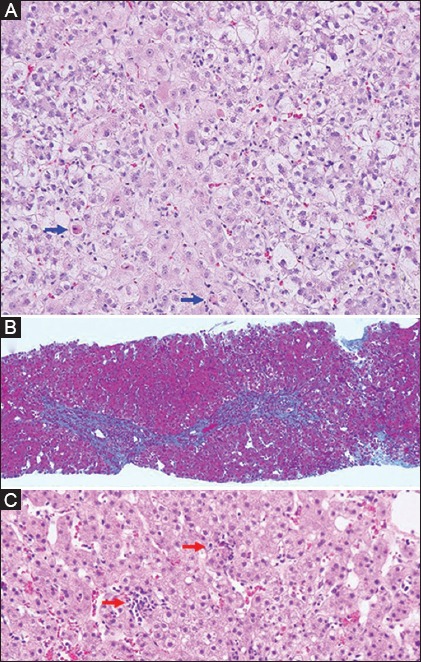
Diagnostic findings of fibrosing cholestatic hepatitis (FCH) C. (A) Findings of hematoxylin and eosin staining are shown (magnification x400). Hepatocyte ballooning and cholestasis are observed. Feathery degeneration of hepatic parenchyma caused by cholestasis is confirmed. Apoptotic hepatocytes were observed (blue arrows). Increased numbers of inflammatory cells infiltrated into the periportal area, and piecemeal necrosis is observed. There is a bridging necrosis. (B) Azan staining is shown (magnification x40). Bridging fibrosis is observed at the periportal area, and was classified as F2 on the METAVIR score. (C) Findings at a recovery term of FCH C are shown (magnification x200). Apoptotic hepatocytes and inflammatory infiltration at the periportal area is decreased. Finding of chronic hepatitis C manifested as spotty and patchy necrosis (red arrows)
Predictors of recurrent hepatitis C after LT
High viral loads in the first 3 months after LT were associated with the severity of recurrent hepatitis C [10], and the level of HCV-RNA at 2 weeks after LT is an important risk factor of FCH C after LT [10]. Previously, we routinely performed splenectomy in HCV-positive recipients, because the side effect of pancytopenia often prevented treatment with IFN after LT [29,38]. Splenectomy is not a standard practice in LT for HCV-positive patients, and splenectomy is stated as just a historic reason. The necessity of splenectomy in HCV-positive recipients will be answered by the many ongoing studies in the coming year, because treatment with DAAs does not cause pancytopenia. To overcome the inevitable insufficiency of allograft size during adult living-donor LT, we intentionally establish portal vein pressure (PVP) under 15 mmHg [39,40]. From the viewpoint of recurrent hepatitis C, hepatic venous portal pressure gradients (HVPGs) are good predictors of clinical decompensation due to recurrent hepatitis C, with only 2% of patients with a normal HVPG and 67% of patients with abnormal HVPG progressing to decompensation [41]. The PVP value during LT might have been an informative predictor, nevertheless this value is not relevant to the long term outcome. Only indirect measurements of PVP with HVPG after LT have been correlated with prognosis [42]. Currently, a liver stiffness which reflects the degree of liver fibrosis can be measured by a non-invasive, rapid, quantitative and low-cost method, and this reliable value have been correlated with HVPG [43].
From the viewpoint of hepatitis recurrence, several donor factors, especially donor graft steatosis and older donor age, are associated with an earlier and more severe recurrence of hepatitis C [2,44].
Effects of immunosuppressants on recurrent hepatitis C in LT recipients
The use of tacrolimus after LT is associated with significantly reduced rates of death, graft loss, acute rejection, and steroid-resistant rejection [45]. Immunosuppression has been associated with increased disease severity in recurrent hepatitis C cases [1-3]. The use of stronger immunosuppression was linked to worse outcomes in recurrent hepatitis C cases [46]. No correlation between the type of calcineurin inhibitors (cyclosporine and tacrolimus) and the risk of recurrent hepatitis C was reported [47]. Corticosteroid usage also has an important role in recurrent hepatitis C [48-51]. Treatment of both acute cellular rejection with multiple boluses of corticosteroids and rapid tapering of steroids have been linked to recurrent disease [50,51]. The reduced progression of recurrent hepatitis C and better patient outcomes were demonstrated following the use of slow tapering steroid regimens [48,49].
Is an assessment of Child-Pugh score for DAA induction necessary for allograft dysfunction after LT?
Child-Pugh score is used to predict the outcome of surgery in cirrhotic patients in general, and more recently, to stratify patients on the waiting list for LT [52]. Then, a simple question arises. Even if serum levels of alanine aminotransferase and the METAVIR system for histologic findings in chronic hepatitis C can be used in transplanted allografts [53,54], is an assessment of the Child-Pugh score necessary even in allograft dysfunction after LT?
Initially, cirrhosis with a Child-Pugh score of B or C contraindicates these drugs because of side effects. When there is a decision against using FCH, allograft dysfunction is severe if based on the Child-Pugh score. Even though the Child-Pugh scoring system is useful for assessing liver cirrhosis, it is not suitable for allograft dysfunction after LT. Currently, new DAAs are safe and effective with few side effects, even in a majority of Child’s B and C class, when properly selected. The issues here are the reduced efficacy in advanced cirrhosis and in severe renal impairment [12]. The DAAs should be aggressively introduced for FCH C in LT recipients, and that they might improve the clinical course of patients.
Discussion
Although FCH is a rare variant of viral hepatitis, it should be emphasized that a prompt diagnosis is important for the management of adult recipients after LT. Histopathological examination and HCV-RNA measurement should be performed in the event of unexplained laboratory findings and/or intractable ascites [1-3].
Hepatitis C recurrence continues to present a major challenge in LT [1-3]. Despite recent advances, the results in recipients with recurrent hepatitis C are not satisfactory, mainly because of a recurrence of the primary disease and a lack of availability of an efficient prophylactic therapy [1,2]. The last few years have seen the introduction of DAAs [1,2]. Carefully considered DAA induction provides hope for the development of new protocols that are safer and more effective, even in post-transplant situations.
Recent researchers documented excellent results of DAAs, especially in the treatments for patients with hepatitis C before LT. Sofosbuvir-based antiviral therapy is highly effective even in recurrent hepatitis C after LT [55,56], and the SVR rate of sofosbuvir-based therapy was reported as >90% even for hepatitis C in LT recipients [55]. In the recent data for hepatitis C patients, the SVR rates of sofosbuvir/daclatasvir [18,57] and sofosbuvir/ledipasvir [58,59] were reported as 95-100% and 90-97%, respectively. However, these SVR rates were mainly investigated in patients before LT. Moreover, these researchers focused on patients with hepatitis C, not with FCH. There are only a few reports of successful treatments with DAAs for LT recipients with FCH which had fulfilled with diagnostic criterion [14-18] (Tables 1, 2). In the era of all oral therapies with DAAs, no recipients who undergoes LT for HCV-related cirrhosis should have their graft failures because of recurrent hepatitis C [56].
We know that some DAAs should not be used in patients with Child C cirrhosis and/or severe renal impairment. However, the Child-Pugh score is not suitable for the assessment of allograft dysfunction after LT. We all respect health insurance systems around the world. However, even if the broad application of DAAs is unfortunately limited by their high costs [58,60], we suggest that DDAs should be carefully but aggressively induced for fatal FCH C even in LT recipients. We hope this review will be informative for those who care for post-transplant patients with fatal FCH C.
Acknowledgment
We are grateful to Shigeo Nakamura and Yosie Shimoyama (Department of Pathology, Nagoya University Hospital, Nagoya, Japan), for their special supports.
Biography
Nagoya University Hospital, Nagoya, Japan
Footnotes
Conflict of Interest: None
References
- 1.Mitchell O, Gurakar A. Management of hepatitis C post-liver transplantation: a comprehensive review. J Clin Transl Hepatol. 2015;3:140–148. doi: 10.14218/JCTH.2015.00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jimenez-Perez M, Gonzalez-Grande R, Rando-Munoz FJ. Management of recurrent hepatitis C virus after liver transplantation. World J Gastroenterol. 2014;20:16409–16417. doi: 10.3748/wjg.v20.i44.16409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Xiao SY, Lu L, Wang HL. Fibrosing cholestatic hepatitis: clinicopathologic spectrum, diagnosis and pathogenesis. Int J Clin Exp Pathol. 2008;1:396–402. [PMC free article] [PubMed] [Google Scholar]
- 4.Davies SE, Portmann BC, O’Grady JG, Aldis PM, Chaggar K, Alexander GJ, Williams R. Hepatic histological findings after transplantation for chronic hepatitis B virus infection, including a unique pattern of fibrosing cholestatic hepatitis. Hepatology. 1991;13:150–157. [PubMed] [Google Scholar]
- 5.O’Grady JG, Smith HM, Davies SE, et al. Hepatitis B virus reinfection after orthotopic liver transplantation. Serological and clinical implications. J Hepatol. 1992;14:104–111. doi: 10.1016/0168-8278(92)90138-f. [DOI] [PubMed] [Google Scholar]
- 6.Demetris AJ, Todo S, Van Thiel DH, et al. Evolution of hepatitis B virus liver disease after hepatic replacement. Practical and theoretical considerations. Am J Pathol. 1990;137:667–676. [PMC free article] [PubMed] [Google Scholar]
- 7.Todo S, Demetris AJ, Van Thiel D, Teperman L, Fung JJ, Starzl TE. Orthotopic liver transplantation for patients with hepatitis B virus-related liver disease. Hepatology. 1991;13:619–626. [PMC free article] [PubMed] [Google Scholar]
- 8.Benner KG, Lee RG, Keeffe EB, Lopez RR, Sasaki AW, Pinson CW. Fibrosing cytolytic liver failure secondary to recurrent hepatitis B after liver transplantation. Gastroenterology. 1992;103:1307–1312. doi: 10.1016/0016-5085(92)91521-5. [DOI] [PubMed] [Google Scholar]
- 9.Phillips MJ, Cameron R, Flowers MA, et al. Post-transplant recurrent hepatitis B viral liver disease. Viral-burden, steatoviral, and fibroviral hepatitis B. Am J Pathol. 1992;140:1295–1308. [PMC free article] [PubMed] [Google Scholar]
- 10.Graziadei IW, Zoller HM, Schloegl A, et al. Early viral load and recipient interleukin-28B rs12979860 genotype are predictors of the progression of hepatitis C after liver transplantation. Liver Transpl. 2012;18:671–679. doi: 10.1002/lt.23402. [DOI] [PubMed] [Google Scholar]
- 11.Berenguer M, Aguilera V, Prieto M, et al. Effect of calcineurin inhibitors on survival and histologic disease severity in HCV-infected liver transplant recipients. Liver Transpl. 2006;12:762–767. doi: 10.1002/lt.20655. [DOI] [PubMed] [Google Scholar]
- 12.Cholongitas E, Pipili C, Papatheodoridis G. Interferon-free regimens for the treatment of hepatitis C virus in liver transplant candidates or recipients. World J Gastroenterol. 2015;21:9526–9533. doi: 10.3748/wjg.v21.i32.9526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Veldt BJ, Poterucha JJ, Watt KD, et al. Impact of pegylated interferon and ribavirin treatment on graft survival in liver transplant patients with recurrent hepatitis C infection. Am J Transplant. 2008;8:2426–2433. doi: 10.1111/j.1600-6143.2008.02362.x. [DOI] [PubMed] [Google Scholar]
- 14.Forns X, Charlton M, Denning J, et al. Sofosbuvir compassionate use program for patients with severe recurrent hepatitis C after liver transplantation. Hepatology. 2015;61:1485–1494. doi: 10.1002/hep.27681. [DOI] [PubMed] [Google Scholar]
- 15.Delabaudiere C, Lavayssière L, Dörr G, et al. Successful treatment of fibrosing cholestatic hepatitis with pegylated interferon, ribavirin and sofosbuvir after a combined kidney-liver transplantation. Transpl Int. 2015;28:255–258. doi: 10.1111/tri.12428. [DOI] [PubMed] [Google Scholar]
- 16.Al Nahdi N, Ford JA, Greanya ED, et al. First successful treatment of post-liver transplant hepatitis C fibrosing cholestatic hepatitis with boceprevir, peginterferon and ribavirin in a pre-transplant null responder. Ann Hepatol. 2013;12:156–160. [PubMed] [Google Scholar]
- 17.Saab S, Jimenez M, Bau S, et al. Treating fibrosing cholestatic hepatitis C with sofosbuvir and ribavirin: a matched analysis. Clin Transplant. 2015;29:813–819. doi: 10.1111/ctr.12584. [DOI] [PubMed] [Google Scholar]
- 18.Leroy V, Dumortier J, Coilly A, et al. Efficacy of sofosbuvir and daclatasvir in patients with fibrosing cholestatic hepatitis C after liver transplantation. Clin Gastroenterol Hepatol. 2015;13:1993–2001. doi: 10.1016/j.cgh.2015.05.030. [DOI] [PubMed] [Google Scholar]
- 19.Pelletier SJ, Raymond DP, Crabtree TD, et al. Hepatitis C-induced hepatic allograft injury is associated with a pretransplantation elevated viral replication rate. Hepatology. 2000;32:418–426. doi: 10.1053/jhep.2000.9408. [DOI] [PubMed] [Google Scholar]
- 20.Gane EJ, Portmann BC, Naoumov NV, et al. Long-term outcome of hepatitis C infection after liver transplantation. N Engl J Med. 1996;334:815–820. doi: 10.1056/NEJM199603283341302. [DOI] [PubMed] [Google Scholar]
- 21.Gane E. The natural history and outcome of liver transplantation in hepatitis C virus-infected recipients. Liver Transpl. 2003;9:S28–S34. doi: 10.1053/jlts.2003.50248. [DOI] [PubMed] [Google Scholar]
- 22.Garcia-Retortillo M, Forns X, Feliu A, et al. Hepatitis C virus kinetics during and immediately after liver transplantation. Hepatology. 2002;35:680–687. doi: 10.1053/jhep.2002.31773. [DOI] [PubMed] [Google Scholar]
- 23.Carrion JA, Torres F, Crespo G, et al. Liver stiffness identifies two different patterns of fibrosis progression in patients with hepatitis C virus recurrence after liver transplantation. Hepatology. 2010;51:23–34. doi: 10.1002/hep.23240. [DOI] [PubMed] [Google Scholar]
- 24.Rodriguez-Luna H, Vargas HE. Management of hepatitis C virus infection in the setting of liver transplantation. Liver Transpl. 2005;11:479–489. doi: 10.1002/lt.20424. [DOI] [PubMed] [Google Scholar]
- 25.Berenguer M, Aguilera V, Prieto M, et al. Delayed onset of severe hepatitis C-related liver damage following liver transplantation: a matter of concern? Liver Transpl. 2003;9:1152–1158. doi: 10.1053/jlts.2003.50240. [DOI] [PubMed] [Google Scholar]
- 26.Berenguer M, Rayon JM, Prieto M, et al. Are posttransplantation protocol liver biopsies useful in the long term? Liver Transpl. 2001;7:790–796. doi: 10.1053/jlts.2001.23794. [DOI] [PubMed] [Google Scholar]
- 27.Wiesner RH, Sorrell M, Villamil F. Report of the first International Liver Transplantation Society expert panel consensus conference on liver transplantation and hepatitis C. Liver Transpl. 2003;9:S1–S9. doi: 10.1053/jlts.2003.50268. [DOI] [PubMed] [Google Scholar]
- 28.Sartori M, Andorno S, Rossini A, et al. A case-control histological study on the effects of phlebotomy in patients with chronic hepatitis C. Eur J Gastroenterol Hepatol. 2011;23:1178–1184. doi: 10.1097/MEG.0b013e328349923c. [DOI] [PubMed] [Google Scholar]
- 29.Marubashi S, Umeshita K, Asahara T, et al. Steroid-free living donor liver transplantation for HCV--a multicenter prospective cohort study in Japan. Clin Transplant. 2012;26:857–867. doi: 10.1111/j.1399-0012.2012.01627.x. [DOI] [PubMed] [Google Scholar]
- 30.Chalasani N, Manzarbeitia C, Ferenci P, et al. Peginterferon alfa-2a for hepatitis C after liver transplantation: two randomized, controlled trials. Hepatology. 2005;41:289–298. doi: 10.1002/hep.20560. [DOI] [PubMed] [Google Scholar]
- 31.Shergill AK, Khalili M, Straley S, et al. Applicability, tolerability and efficacy of preemptive antiviral therapy in hepatitis C-infected patients undergoing liver transplantation. Am J Transplant. 2005;5:118–124. doi: 10.1111/j.1600-6143.2004.00648.x. [DOI] [PubMed] [Google Scholar]
- 32.Berenguer M, Palau A, Aguilera V, Rayon JM, Juan FS, Prieto M. Clinical benefits of antiviral therapy in patients with recurrent hepatitis C following liver transplantation. Am J Transplant. 2008;8:679–687. doi: 10.1111/j.1600-6143.2007.02126.x. [DOI] [PubMed] [Google Scholar]
- 33.Carrion JA, Navasa M, Garcia-Retortillo M, et al. Efficacy of antiviral therapy on hepatitis C recurrence after liver transplantation: a randomized controlled study. Gastroenterology. 2007;132:1746–1756. doi: 10.1053/j.gastro.2007.03.041. [DOI] [PubMed] [Google Scholar]
- 34.Gurusamy KS, Tsochatzis E, Xirouchakis E, Burroughs AK, Davidson BR. Antiviral therapy for recurrent liver graft infection with hepatitis C virus. Cochrane Database Syst Rev. 2010;1:CD006803. doi: 10.1002/14651858.CD006803.pub3. [DOI] [PubMed] [Google Scholar]
- 35.Picciotto FP, Tritto G, Lanza AG, et al. Sustained virological response to antiviral therapy reduces mortality in HCV reinfection after liver transplantation. J Hepatol. 2007;46:459–465. doi: 10.1016/j.jhep.2006.10.017. [DOI] [PubMed] [Google Scholar]
- 36.Berenguer M. Systematic review of the treatment of established recurrent hepatitis C with pegylated interferon in combination with ribavirin. J Hepatol. 2008;49:274–287. doi: 10.1016/j.jhep.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 37.Aytaman A, Kaufman M, Terrault NA. Management of posttransplant hepatitis C infection. Curr Opin Organ Transplant. 2010;15:301–309. doi: 10.1097/MOT.0b013e3283398237. [DOI] [PubMed] [Google Scholar]
- 38.Nyalakonda H, Utay NS. A new era of therapy for hepatitis C virus infection. Curr Opin Infect Dis. 2015;28:471–478. doi: 10.1097/QCO.0000000000000190. [DOI] [PubMed] [Google Scholar]
- 39.Hori T, Ogura Y, Ogawa K, et al. How transplant surgeons can overcome the inevitable insufficiency of allograft size during adult living-donor liver transplantation: strategy for donor safety with a smaller-size graft and excellent recipient results. Clin Transplant. 2012;26:E324–E334. doi: 10.1111/j.1399-0012.2012.01664.x. [DOI] [PubMed] [Google Scholar]
- 40.Ogura Y, Hori T, El Moghazy WM, et al. Portal pressure <15 mm Hg is a key for successful adult living donor liver transplantation utilizing smaller grafts than before. Liver Transpl. 2010;16:718–728. doi: 10.1002/lt.22059. [DOI] [PubMed] [Google Scholar]
- 41.Blasco A, Forns X, Carrion JA, et al. Hepatic venous pressure gradient identifies patients at risk of severe hepatitis C recurrence after liver transplantation. Hepatology. 2006;43:492–499. doi: 10.1002/hep.21090. [DOI] [PubMed] [Google Scholar]
- 42.Sebastiani G, Alshaalan R, Wong P, et al. Prognostic value of non-invasive fibrosis and steatosis tools, hepatic venous pressure gradient (HVPG) and histology in nonalcoholic steatohepatitis. PLoS One. 2015;10:e0128774. doi: 10.1371/journal.pone.0128774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Schwabl P, Bota S, Salzl P, et al. New reliability criteria for transient elastography increase the number of accurate measurements for screening of cirrhosis and portal hypertension. Liver Int. 2015;35:381–390. doi: 10.1111/liv.12623. [DOI] [PubMed] [Google Scholar]
- 44.Subramanian V, Seetharam AB, Vachharajani N, et al. Donor graft steatosis influences immunity to hepatitis C virus and allograft outcome after liver transplantation. Transplantation. 2011;92:1259–1268. doi: 10.1097/TP.0b013e318235a1ab. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.McAlister VC, Haddad E, Renouf E, Malthaner RA, Kjaer MS, Gluud LL. Cyclosporin versus tacrolimus as primary immunosuppressant after liver transplantation: a meta-analysis. Am J Transplant. 2006;6:1578–1585. doi: 10.1111/j.1600-6143.2006.01360.x. [DOI] [PubMed] [Google Scholar]
- 46.Berenguer M, Prieto M, San Juan F, et al. Contribution of donor age to the recent decrease in patient survival among HCV-infected liver transplant recipients. Hepatology. 2002;36:202–210. doi: 10.1053/jhep.2002.33993. [DOI] [PubMed] [Google Scholar]
- 47.Liu Z, Chen Y, Tao R, Xv J, Meng J, Yong X. Tacrolimus-based versus cyclosporine-based immunosuppression in hepatitis C virus-infected patients after liver transplantation: a meta-analysis and systematic review. PLoS One. 2014;9:e107057. doi: 10.1371/journal.pone.0107057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Berenguer M, Aguilera V, Prieto M, et al. Significant improvement in the outcome of HCV-infected transplant recipients by avoiding rapid steroid tapering and potent induction immunosuppression. J Hepatol. 2006;44:717–722. doi: 10.1016/j.jhep.2006.01.005. [DOI] [PubMed] [Google Scholar]
- 49.Vivarelli M, Burra P, La Barba G, et al. Influence of steroids on HCV recurrence after liver transplantation: A prospective study. J Hepatol. 2007;47:793–798. doi: 10.1016/j.jhep.2007.07.023. [DOI] [PubMed] [Google Scholar]
- 50.Neumann UP, Berg T, Bahra M, et al. Long-term outcome of liver transplants for chronic hepatitis C: a 10-year follow-up. Transplantation. 2004;77:226–231. doi: 10.1097/01.TP.0000101738.27552.9D. [DOI] [PubMed] [Google Scholar]
- 51.Berenguer M, Ferrell L, Watson J, et al. HCV-related fibrosis progression following liver transplantation: increase in recent years. J Hepatol. 2000;32:673–684. doi: 10.1016/s0168-8278(00)80231-7. [DOI] [PubMed] [Google Scholar]
- 52.Cholongitas E, Papatheodoridis GV, Vangeli M, Terreni N, Patch D, Burroughs AK. Systematic review: The model for end-stage liver disease--should it replace Child-Pugh’s classification for assessing prognosis in cirrhosis? Aliment Pharmacol Ther. 2005;22:1079–1089. doi: 10.1111/j.1365-2036.2005.02691.x. [DOI] [PubMed] [Google Scholar]
- 53.Pradat P, Alberti A, Poynard T, et al. Predictive value of ALT levels for histologic findings in chronic hepatitis C: a European collaborative study. Hepatology. 2002;36:973–977. doi: 10.1053/jhep.2002.35530. [DOI] [PubMed] [Google Scholar]
- 54.The French METAVIR Cooperative Study Group. Intraobserver and interobserver variations in liver biopsy interpretation in patients with chronic hepatitis C. Hepatology. 1994;20:15–20. [PubMed] [Google Scholar]
- 55.Faisal N, Bilodeau M, Aljudaibi B, et al. Sofosbuvir-based antiviral therapy is highly effective in recurrent hepatitis C in liver transplant recipients: Canadian multicenter “Real-Life” experience. Transplantation. 2016;100:1059–1065. doi: 10.1097/TP.0000000000001126. [DOI] [PubMed] [Google Scholar]
- 56.Kwo PY. Direct acting antiviral therapy after liver transplantation. Curr Opin Gastroenterol. 2016;32:152–158. doi: 10.1097/MOG.0000000000000266. [DOI] [PubMed] [Google Scholar]
- 57.Poordad F, Schiff ER, Vierling JM, et al. Daclatasvir with sofosbuvir and ribavirin for hepatitis C virus infection with advanced cirrhosis or post-liver transplantation recurrence. Hepatology. 2016;63:1493–1505. doi: 10.1002/hep.28446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Do A, Mittal Y, Liapakis A, et al. Drug authorization for sofosbuvir/ledipasvir (Harvoni) for chronic HCV infection in a Real-World Cohort: A new barrier in the HCV care cascade. PLoS One. 2015;10:e0135645. doi: 10.1371/journal.pone.0135645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ciesek S, Proske V, Otto B, et al. Efficacy and safety of sofosbuvir/ledipasvir for the treatment of patients with hepatitis C virus re-infection after liver transplantation. Transpl Infect Dis 2016. 2016;18:326–332. doi: 10.1111/tid.12524. [DOI] [PubMed] [Google Scholar]
- 60.Ferenci P. Treatment of hepatitis C in difficult-to-treat patients. Nat Rev Gastroenterol Hepatol. 2015;12:284–292. doi: 10.1038/nrgastro.2015.53. [DOI] [PubMed] [Google Scholar]