

Abstract
Background
Colonoscopies performed in the afternoon (PM) have been shown to have lower adenoma detection rates (ADR) compared to those in the morning (AM). Endoscopist fatigue has been suggested as a possible reason. Colonoscopies tend to be technically more challenging in female patients. Furthermore, women have a lower incidence of adenomas then men. The impact of the timing of colonoscopy based on sex has not been studied. We hypothesized that any decrease in ADR in PM colonoscopies would be more pronounced in female patients when compared to male patients.
Methods
We retrospectively reviewed colonoscopies performed for screening or surveillance in our outpatient endoscopy center from January 2008 to December 2011. Complete colonoscopies with a documented cecal intubation were included. All patients with a history of colorectal cancer or colonic resection, inadequate bowel preparation, or incomplete data were excluded.
Results
A total of 2305 patients (1207 female) were included. Overall, ADR was significantly higher in AM than in PM procedures. Multivariate analysis demonstrated that ADR for females was lower in PM than in AM colonoscopies (odds ratio [OR] 0.63, 95% confidence interval [CI] 0.44-0.91, P=0.015). There was a non-significant trend towards a lower ADR for males in PM (OR 0.84, 95% CI 0.62-1.15, P=0.28). Females had a prolonged intubation time and a longer procedure time.
Conclusion
The difference in ADR between AM and PM procedures seems to apply mainly to female patients. No significant change in ADR was noted in male patients in the afternoon.
Keywords: Adenoma detection rate, morning colonoscopies, afternoon colonoscopies, timing of colonoscopies, female
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer mortality in the United States [1], although its incidence is declining, probably as a result of increased awareness and higher rates of screening colonoscopies. Colonoscopy is the mainstay of the diagnosis and prevention of CRC via removal of adenomatous polyps before they potentially progress and become cancerous [2]. While colonoscopy remains the gold-standard screening test, the rate of cancer prevention is far from optimal. Experienced colonoscopists in the National Polyp Study failed to identify approximately 25% of patients with incident adenomas [3].
The most important benchmark for a quality colonoscopy is the adenoma detection rate (ADR). The American Society for Gastrointestinal Endoscopy (ASGE) and the American College of Gastroenterology (ACG) guidelines recommend an average ADR of ≥25% in men and ≥15% in women for risk-screening colonoscopy [4]. There are various modifiable factors that can affect ADR and therefore the quality of colonoscopy, such as withdrawal time, quality of bowel preparations and cecal intubation rate [4].
The timing of colonoscopy has been implicated as an independent predictor of outcome. Afternoon colonoscopies (PM) have higher failure rates, lower cecal intubation rates and worse bowel preparations [5,6]. Studies have shown that in PM colonoscopies both polyp detection rate (PDR) and ADR are lower than in morning (AM) colonoscopies [7-11] It has been speculated that inadequate bowel preparation and physician fatigue as the day progresses are among the possible reasons for lower ADR and PDR in afternoon procedures.
Colonoscopies in female patients tend to be more challenging and technically more difficult than in male patients, for a variety of reasons including anatomic variations. Moreover, females have a lower incidence of polyps and adenomas than do males [12]. To our knowledge, the impact of the timing of colonoscopy (AM vs. PM) on female compared to male colonoscopies has not yet been studied. We hypothesized that any decrease in ADR in PM colonoscopies would be more pronounced in female than in male patients.
Patients and methods
We performed a retrospective chart review looking at medical records of patients who underwent colonoscopies from January 2008 to December 2011. All outpatients presenting for screening or surveillance colonoscopies in our ambulatory endoscopy center were reviewed. Patients were excluded from the study if their colonoscopies were incomplete, the cecum was not intubated, patients had a history of CRC or colonic resection, the quality of the bowel preparation was inadequate on the Aronchick scale, or if the data were incomplete. We collected baseline patient characteristics, including patient age, sex, race, body mass index, and family history. The procedure-related data collected included the endoscopist performing the procedure, starting time, cecal intubation time, withdrawal time, adequacy of bowel preparation, involvement of a fellow, colonoscopic findings and histopathology of polyps resected.
The standard bowel preparation used by our practice during that period of time was the 4-L polyethylene glycol in a split dose. Patients were instructed to finish their second dose of preparation exactly 4 h prior to their scheduled procedure time which set up the runway time within optimal limits [13,14]. All colonoscopies were performed under monitored anesthesia care with propofol sedation using Olympus 160 series colonoscopes (Olympus Medical Systems, Center Valley, PA).
Morning procedures were defined as procedures whose starting time was before 12 PM; afternoon procedures were defined as those whose starting time was at or after 12 PM. Cecal intubation was defined by visualization of the ileocecal valve and the appendiceal orifice. Cecal intubation time was defined as the time from procedure start to cecal intubation. Withdrawal time was the time taken for mucosal inspection from cecal intubation to the end of the procedure. The endoscopy nurses recorded cecal intubation time and withdrawal times using a stopwatch. Withdrawal time and total procedure time were calculated from colonoscopies in which no polyp was removed, to control for possible lengthening of withdrawal time. Experienced endoscopists were defined as those with more than 5 years of clinical experience after their fellowship training. All endoscopists performed the cases in full-day blocks. Each endoscopist performed a median of 8 (range 5-11) colonoscopies on each assigned day. The quality of the bowel preparation was graded from 1 to 5 by the endoscopists during the procedure, according to Aronchick stool-preparation scale (1 = excellent, small volume of clear fluid, >95% of surface seen; 2 = good, large volume of clear liquid <25%, >90% of surface seen; 3 = fair some semi-solid stool, >90% of surface seen; 4 = poor, some semi-solid stool, <90% of surface seen; and 5 = inadequate, repeat preparation & repeat colonoscopy needed).
The main outcome measure was ADR, defined as the percentage of colonoscopies in which at least one adenoma was detected. PDR was defined as the percentage of colonoscopies in which at least one polyp was detected.
Statistical analysis
All statistical analyses were performed using STATA version 13 (STATA, College Station, TX, USA). Categorical variables were reported as percentages. Continuous variables were reported as mean with standard deviation. Continuous variables were compared using the two-sample t-test and categorical variables were compared using Person’s chi-square test. Adenoma detection was a dichotomous outcome variable and was analyzed according to time of the day (AM vs. PM and hour of the day) using logistic regression. These analyses were also made separately for males and females. The predicted probabilities of adenoma detection were plotted against the hour of the day using logistic regression and two-way scatterplots. Multivariate analysis was also performed for ADR, using logistic regression while adjusting for possible extraneous variables. A two-sided P-value of 0.05 was used to determine statistical significance.
Results
A total of 2305 complete colonoscopies performed by 18 gastroenterologists were included in the final analysis: 1574 (68.3%) colonoscopies were performed in the morning sessions and 731 (31.7%) in the afternoon sessions. Table 1 compares the baseline data points between morning and afternoon colonoscopies. The patients’ mean age was 58.0±12.5 years and 47.6% were male. The overall PDR was 37.9% and ADR was 21.6%. PDR was significantly higher in AM (39.8%) than in PM colonoscopies (33.7%) (odds ratio [OR] 0.76, 95% confidence interval [CI] 0.64-0.92, P=0.004). Similarly, ADR was 23.1% in AM compared to 18.3% in PM colonoscopies (OR 0.75, 95% CI 0.60-0.93, P=0.009].
Table 1.
A comparison of demographics, procedural factors and findings between morning and afternoon colonoscopies
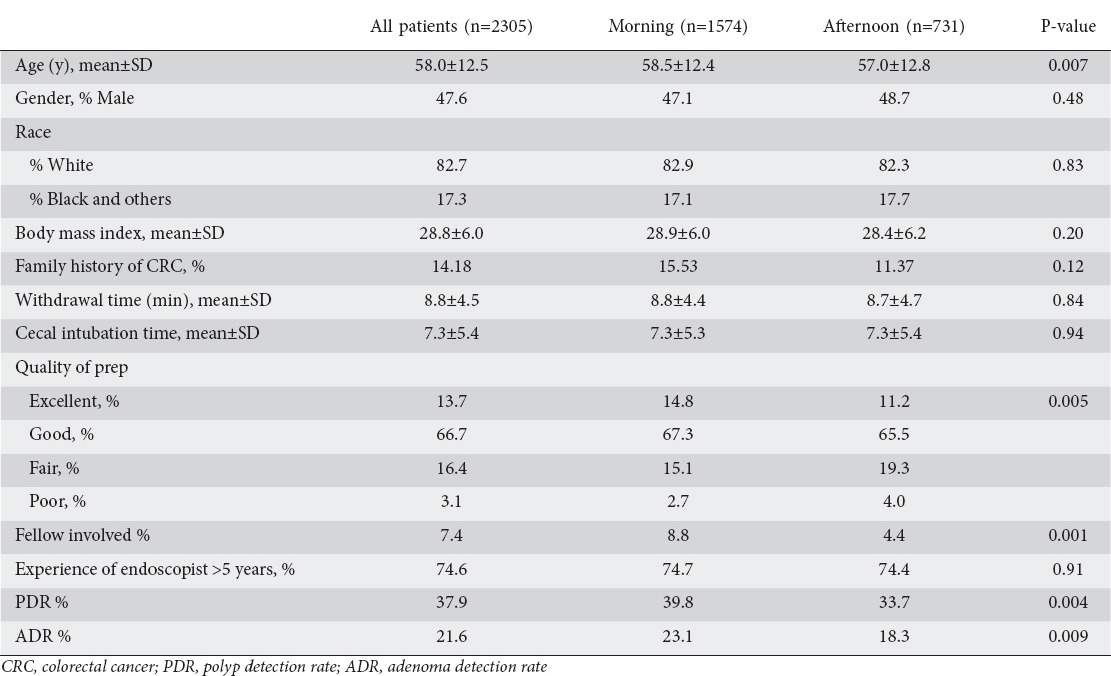
The mean age of the patients and the quality of bowel preparation were significantly different in the AM and PM groups (Table 1). In a multivariate analysis, adjusting for confounding variables including age and bowel preparation, ADR continued to be lower in afternoon colonoscopies compared to morning colonoscopies (OR 0.75, 95% CI 0.59-0.94, P=0.01). There was a trend towards a progressive decline in ADR with each subsequent hour of the day. A logistic regression analysis showed that the hour of day was an independent predictor of adenoma detection (P=0.002) (Fig. 1A). In a multivariate analysis, age (OR 1.04, 95% CI 1.03-1.5, P=0.001), female sex (OR 0.60, 95% CI 0.49-0.75, P=0.001) and longer withdrawal time (OR 1.22, 95% CI 1.12-1.32, P=0.001) were also significant determinants of ADR (Table 2).
Figure 1.
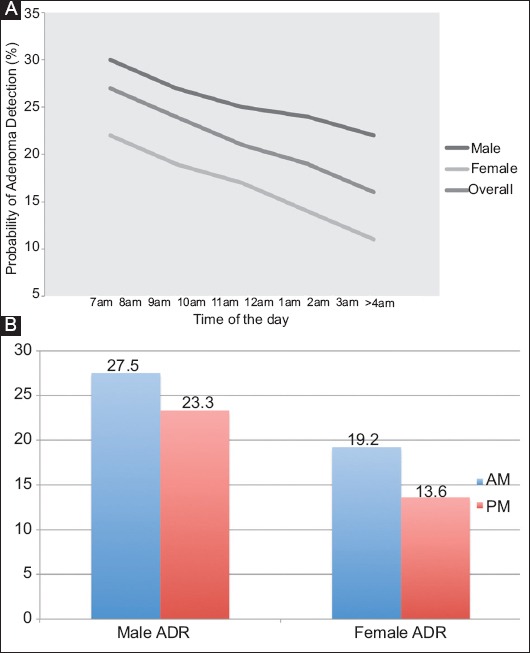
(A) Hour-by-hour analysis of overall adenoma detection along with male and female adenoma detection rates (ADR). Overall, the time of the day was an independent predictor of adenoma detection (P=0.002). (B) Male and female ADR in morning (AM) and afternoon (AM) colonoscopies. Females had a significant decrease (37%) in ADR in PM colonoscopies (OR 0.63, 95% CI 0.44-0.91, P=0.015) while the decrease in ADR for males in PM (16%) was statistically non-significant (OR 0.84, 95% CI 0.62-1.15, P=0.28).
Table 2.
Multivariate analysis of adenoma detection rate (ADR)
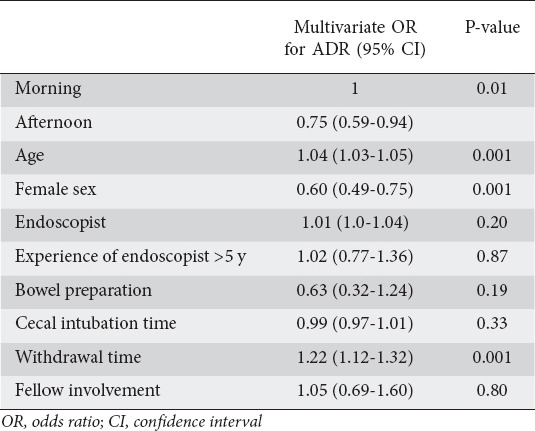
Table 3 shows a comparison between male and female colonoscopies. There was no difference in age or timing of colonoscopies between male and female patients. Women had more excellent and good bowel preparations than men. The females had a longer cecal intubation time (7.9 vs. 6.6 min, P=0.001) and total procedure time (16.7 vs. 15.5 min, P=0.002). Withdrawal time was significantly longer for males (9.1 vs. 8.5 min, P=0.028). ADR, PDR, and mean number of polyps per colonoscopy were higher for male patients.
Table 3.
Comparison of female and male colonoscopies
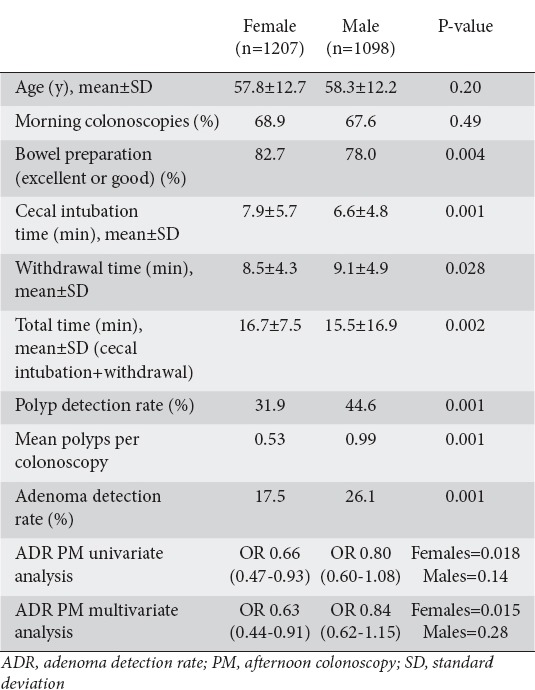
There was a significant decline in the ADR in female patients between AM and PM procedures (OR 0.66, 95% CI 0.47-0.93, P=0.017). Males also showed a trend towards a decline in ADR, but the difference was not statistically significant (OR 0.80, 95% CI 0.60-1.07, P=0.14). In a multivariate analysis, adjusting for age, race, body mass index, family history, fellow involvement, withdrawal time, cecal intubation time, endoscopist, and bowel preparations, similar findings were noted. Females had a significantly lower ADR in PM than in AM colonoscopies (OR=0.63, 95% CI 0.44-0.91, P=0.015) while the difference in ADR in PM for males remained statistically non-significant (OR 0.84, 95% CI 0.62-1.15, P=0.28) (Fig. 1B).
Discussion
Our findings show a decrease in PDR and ADR in afternoon compared to morning colonoscopies when procedures are performed in full-day blocks. These results are consistent with previous studies that compared PDRand ADR in morning and afternoon colonoscopies [7-11]. A study by Sanaka et al showed that this effect was more than just a morning versus afternoon occurrence and that there was a linear decline in ADR as the day progressed [8]. Our study also shows an hour-by-hour progressive effect on adenoma decline (Fig. 1A).
The quality of bowel preparation is critical for successful mucosal visualization and polyp detection. Better bowel preparation quality in the morning hours may have contributed to our findings, but the relationship between time of day and polyp or adenoma detection persisted even when this was adjusted for in a multivariate analysis. Our retrospective study looked at data from 2008 to 2011. While current recommendations are to document the adequacy of bowel preparation using the Boston scale [13], after all appropriate measures have been taken, including washing and suctioning to clear residual debris, the modified Aronchick scale that we used here was an acceptable measure for this time period. As far as withdrawal times are concerned, we found that they were greater than the recommended 6 min in both AM and PM colonoscopies. Moreover, there were no significant differences in either withdrawal time or cecal intubation time across the day, thus ruling this out as a possible confounding factor. In a multivariate analysis, with adjustment for multiple patient and procedure variables, there was a decline in adenoma detection in afternoon colonoscopies. ADR in afternoon colonoscopies was lower than the recommended 25% for males and 15% for females.
Endoscopist fatigue has been hypothesized as a possible explanation for the lower PDR and ADR in the afternoon when colonoscopies are performed in full-day blocks [7-9,15,16]. Polyp yield may decrease over time as a result of cognitive or perceptual errors arising from a long and repetitive activity [7]. While our study design did not allow for direct evaluation of endoscopist fatigue as the day progressed, it certainly remains a possible reasonable explanation for the decrease in polyp and adenoma yield.
Like previous studies, our study found an overall (combined male and female) decrease in polyp and adenoma yield in PM colonoscopies. However, the earlier studies did not examine the impact of timing (AM vs. PM) in male and female patients separately. We found that the time effect was different in males and females (Table 3). In a multivariate analysis, adjusting for extraneous variables, females showed a statistically significant decrease in ADR in PM colonoscopies, whereas males showed only a non-significant decrease. This represents an important sex-related difference regarding the outcomes of colonoscopies.
In our study, females had a longer cecal intubation time and total time of colonoscopy, suggesting a higher level of difficulty in female patients. Previous studies have also demonstrated that colonoscopy is technically more challenging in females than in males [17,18]. Waye and Bashkoff described cecal intubation to be more difficult in women, irrespective of the history of pelvic surgery [19]. Several anatomic variations have been implicated in this difference, including a longer colon, the dipping of the transverse into the pelvis, and the presence of more angulations and tortuosity in female colons because a longer colon is folded into a smaller abdominal cavity [17,20-22]. In addition, female patients tend to have a deeper pelvis, which creates acute angulation when the proximal sigmoid colon comes out of the pelvis over the uterus. These factors, amongst others, contribute to the higher level of difficulty of female colonoscopies. We believe that the drop in ADR may be more pronounced in women because this higher level of difficulty may enhance physician fatigue. Moreover, females have a substantially lower overall incidence of polyps and adenoma than males; this difference may contribute to the lower rate of polyp and adenoma detection in PM colonoscopies, especially when combined with endoscopist fatigue. Based on the above findings of our study, we suggest that female or difficult colonoscopies should be performed in the morning.
We acknowledge the limitations of the retrospective nature of our study, in that there is a potential for unmeasured bias. Physician fatigue was not measured, it was speculated to be the possible cause for decreased polyp detection by exclusion of other variables and no data exist to suggest a causal relationship. Similarly, we did not directly measure the difficulty level of the procedure. Female colonoscopies were considered difficult because of the longer cecal intubation time and total time of colonoscopy. We did not evaluate the impact of time of colonoscopy on either advanced adenomas or CRC. The size and site of the polyp removed are important, but they were not recorded in our study. In addition, our analysis did not include a comparison between AM versus PM colonoscopies, or female versus male patients, per endoscopist. It is also possible that these findings at an academic institution cannot be generalized to other settings, including community hospitals.
In conclusion, our study suggests that overall polyp and adenoma detection decreases as the day progresses. Both male and female patients showed a decrease in ADR in afternoon procedures but the decrease was only statistically significant in female patients. The time of colonoscopy seems to be a stronger predictor of ADR in female patients. It is possible that endoscopist fatigue is more pronounced in colonoscopies performed on female patients, since they are technically more challenging. Additional studies are needed to further assess the reasons for and implications of these findings.
Summary Box.
What is already known:
Colonoscopies performed in the afternoon tend to have lower polyp and adenoma detection rates
What the new findings are:
The lower adenoma detection rate in afternoon colonoscopies seems to apply mainly to female patients
Biography
Allegheny Health Network, Pittsburgh, PA, USA
Footnotes
Conflict of Interest: None
References
- 1.American Cancer Society. Cancer facts and figures 2014. Atlanta, GA: American Cancer Society; 2014. [Accessed 17 August 2016]. http://www.cancer.org/acs/groups/content/@research/documents/webcontent/acspc-042151.pdf . [Google Scholar]
- 2.Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981. doi: 10.1056/NEJM199312303292701. [DOI] [PubMed] [Google Scholar]
- 3.Winawer SJ, Zauber AG, O’Brien MJ, et al. Randomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. The National Polyp Study Workgroup. N Engl J Med. 1993;328:901–906. doi: 10.1056/NEJM199304013281301. [DOI] [PubMed] [Google Scholar]
- 4.Rex DK, Petrini JL, Baron TH, et al. ASGE/ACG Taskforce on Quality in Endoscopy Quality indicators for colonoscopy. Am J Gastroenterol. 2006;101:873–885. doi: 10.1111/j.1572-0241.2006.00673.x. [DOI] [PubMed] [Google Scholar]
- 5.Sanaka MR, Shah N, Mullen KD, Ferguson DR, Thomas C, McCullough AJ. Afternoon colonoscopies have higher failure rates than morning colonoscopies. Am J Gastroenterol. 2006;101:2726–2730. doi: 10.1111/j.1572-0241.2006.00887.x. [DOI] [PubMed] [Google Scholar]
- 6.Wells CD, Heigh RI, Sharma VK, et al. Comparison of morning versus afternoon cecal intubation rates. BMC Gastroenterol. 2007;7:19. doi: 10.1186/1471-230X-7-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chan MY, Cohen H, Spiegel BM. Fewer polyps detected by colonoscopy as the day progresses at a Veteran’s Administration teaching hospital. Clin Gastroenterol Hepatol. 2009;7:1217–1223. doi: 10.1016/j.cgh.2009.07.013. [DOI] [PubMed] [Google Scholar]
- 8.Sanaka MR, Deepinder F, Thota PN, Lopez R, Burke CA. Adenomas are detected more often in morning than in afternoon colonoscopy. Am J Gastroenterol. 2009;104:1659–1664. doi: 10.1038/ajg.2009.249. [DOI] [PubMed] [Google Scholar]
- 9.Long MD, Martin C, Sandler RS, Herfarth HH, Shaheen NJ, Dellon ES. Reduced polyp detection as endoscopy shift progresses: experience with screening colonoscopy at a tertiary-care hospital. J Clin Gastroenterol. 2011;45:253–258. doi: 10.1097/MCG.0b013e3181fd2998. [DOI] [PubMed] [Google Scholar]
- 10.Lee A, Iskander JM, Gupta N, et al. Queue position in the endoscopic schedule impacts effectiveness of colonoscopy. Am J Gastroenterol. 2011;106:1457–1465. doi: 10.1038/ajg.2011.87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kaneshiro M, Ho A, Chan M, Cohen H, Spiegel BM. Colonoscopy yields fewer polyps as the day progresses despite using social influence theory to reverse the trend. Gastrointest Endosc. 2010;72:1233–1240. doi: 10.1016/j.gie.2010.08.034. [DOI] [PubMed] [Google Scholar]
- 12.Regula J, Rupinski M, Kraszewska E, et al. Colonoscopy in colorectal-cancer screening for detection of advanced neoplasia. N Engl J Med. 2006;355:1863–1872. doi: 10.1056/NEJMoa054967. [DOI] [PubMed] [Google Scholar]
- 13.Johnson DA, Barkun AN, Cohen LB, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the U.S. multi-society task force on colorectal cancer. Gastrointest Endosc. 2014;80:543–562. doi: 10.1016/j.gie.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 14.Marmo R, Rotondano G, Riccio G, et al. Effective bowel cleansing before colonoscopy: a randomized study of split-dosage versus non-split dosage regimens of high-volume versus low-volume polyethylene glycol solutions. Gastrointest Endosc. 2010;72:313–320. doi: 10.1016/j.gie.2010.02.048. [DOI] [PubMed] [Google Scholar]
- 15.Gurudu SR, Ratuapli SK, Leighton JA, Heigh RI, Crowell MD. Adenoma detection rate is not influenced by the timing of colonoscopy when performed in half-day blocks. Am J Gastroenterol. 2011;106:1466–1471. [Google Scholar]
- 16.Munson GW, Harewood GC, Francis DL. Time of day variation in polyp detection rate for colonoscopies performed on a 3-hour shift schedule. Gastrointest Endosc. 2011;73:467–475. doi: 10.1016/j.gie.2010.07.025. [DOI] [PubMed] [Google Scholar]
- 17.Saunders BP, Fukumoto M, Halligan S, et al. Why is colonoscopy more difficult in women? Gastrointest Endosc. 1996;43:124–126. doi: 10.1016/s0016-5107(06)80113-6. [DOI] [PubMed] [Google Scholar]
- 18.Streett SE. Endoscopic colorectal cancer screening in women: Can we do better? Gastrointest Endosc. 2007;65:1047–1049. doi: 10.1016/j.gie.2007.02.037. [DOI] [PubMed] [Google Scholar]
- 19.Waye JD, Bashkoff E. Total colonoscopy: is it always possible? Gastrointest Endosc. 1991;37:152–154. doi: 10.1016/s0016-5107(91)70674-3. [DOI] [PubMed] [Google Scholar]
- 20.Sadahiro S, Ohmura T, Yamada Y, Saito T, Taki Y. Analysis of length and surface area of each segment of the large intestine according to age, sex and physique. Surg Radiol Anat. 1992;14:251–257. doi: 10.1007/BF01794949. [DOI] [PubMed] [Google Scholar]
- 21.Rowland RS, Bell GD, Dogramadzi S, et al. Colonoscopy aided by magnetic 3D imaging: is the technique sufficiently sensitive to detect differences between men and women? Med Biol Eng Comput. 1999;37:673–679. doi: 10.1007/BF02513366. [DOI] [PubMed] [Google Scholar]
- 22.Waye JD. Completing colonoscopy. Am J Gastroenterol. 2000;95:2681–2682. doi: 10.1111/j.1572-0241.2000.03172.x. [DOI] [PubMed] [Google Scholar]