

Abstract
Purpose
The aim of this study was to investigate whether young age at onset of breast cancer is an independent prognostic factor in patients from the Japanese Breast Cancer Registry, after adjustment of known clinicopathological prognostic factors.
Methods
Of the 53,670 patients registered between 2004 and 2006 and surveyed after a 5-year follow-up prognosis, 25,898 breast cancer patients (48.3 %), who were obtained prognostic data, were examined. Clinicopathological factors were compared between young adult (YA; <35 years), middle-aged adult (MA; 35–50 years), and older adult (OA; >50 years) patients. Five-year disease-free survival (DFS) and overall survival (OS) rates were studied.
Results
YA patients were associated with an advanced TNM stage and aggressive characteristics (e.g. human epidermal growth factor receptor 2 (HER2)-positive or oestrogen receptor (ER)-negative breast cancers) compared to MA and OA patients (P < 0.001). The 5-year DFS and OS rates were 79.4 % and 90.8, 88.5 and 95.0 %, and 87.8 % and 91.6 % for YA, MA, and OA patients, respectively. From the multivariable regression analysis, young age at onset was confirmed as an independent prognostic factor for both DFS (hazard ratio 1.73, 95 % confidence interval 1.42–2.10; P < 0.001) and OS (hazard ratio 1.58, 95 % confidence interval 1.16–2.15; P = 0.004).
Conclusions
Young age at onset is an independent negative prognostic factor in breast cancer. Further studies are required to develop new therapeutic strategies for YA breast cancer patients.
Electronic supplementary material
The online version of this article (doi:10.1007/s10549-016-3984-8) contains supplementary material, which is available to authorized users.
Keywords: Breast cancer, Young women, Surveillance data, Prognosis, Multivariable analysis
Introduction
Young adult (YA) cancers are relatively rare and represent a minority of cases. Consequently, data are lacking concerning intellectual and other psychosocial issues affecting this specific patient population [1]. YA cancer patients are significantly more likely to indicate unmet needs for supportive care services [2]. Moreover, fewer clinical trials have been conducted for YA cancers compared to other adult cancers, suggesting that there may be little evidence of high impact. Among YA cancers in women, breast cancer has the highest incidence rates (30–34 years, 13.3 per 100,000 population, and 35–39 years, 31.6 per 100,000 population [3]. However, even breast cancers account for a very small proportion (approximately 7 %) of the total number of breast cancers in these age groups [4–6].
YA breast cancer patients diagnosed in their twenties or thirties tend to have a poorer prognosis than women diagnosed in middle age (MA) [7]. Differences in survival may reflect clinical and biological variations. Indeed, YA breast cancer patients are reported to present with more aggressive biological characteristics and to behave more poorly compared to older breast cancer patients [8]. Previously, we reported the clinicopathological features of YA patients as having advanced TNM staging and human epidermal growth factor receptor 2 (HER2)-positive/oestrogen receptor (ER)-negative breast cancers compared to older patients [6]. Similarly, aggressive and unfavourable characteristics, including TNM classification, ER status, and HER2 status for YA patients with breast cancer have been reported [9–13].
However, to our knowledge, most of the data on the biological characteristics and treatment to evaluate these patients were derived from older and relatively smaller cohort studies. Moreover, whether age remains an independent predictive prognostic factor, after adjustment of breast cancer subtype (ER, PR, and HER2 status), as well as, other known prognostic factors (TNM classification, adjuvant systemic therapy, etc.) has yet to be determined, given YA patients are at risk of developing more aggressive and more advanced breast cancers.
The aim of this study was to investigate whether young age at onset of breast cancer is an independent negative prognostic factor in patients from the Japanese Breast Cancer Registry (which includes >25,000 newly treated breast cancers between 2004 and 2006).
Materials and methods
Patients
This study was conducted using the Japanese Breast Cancer Registry database, the details of which have been reported previously by Kurebayashi et al. [14]. Briefly, it is a registry managed by the Registration Committee of the Japanese Breast Cancer Society with support from the Public Health Research Foundation (Tokyo, Japan). Data on newly operated primary breast cancer patients are reported from affiliated institutes throughout Japan, which included 741 facilities in 2011, through a web-based system that collects information on >50 demographic and clinicopathological characteristics. Pathological TNM classification is registered based on the Unio Internationalis Contra Cancrum staging system (sixth edition) [15]. Histological classification is registered according to the General Rules for Clinical and Pathological Recording of Breast Cancer [16], which has been translated into the Classification of Tumours of the Breast and Female Genital Organs [17]. Age at onset was defined as the age of the beginning of treatment.
HER2 positivity was defined as immunohistochemical staining of 3+ or a positive fluorescent in situ hybridisation test according to the manufacturer’s criteria. Hormone receptor (ER/progesterone receptor [PR]) positivity was determined if ≥1 % of nuclei in the tumour stained positive for ER/PR on immunohistochemical analysis. Of the 53,670 patients registered in the Japanese Breast Cancer Registry between 2004 and 2006 and surveyed after a 5-year follow-up prognosis, 25,898 patients (48.3 %) were obtained follow-up data and used for further examinations. Cases with connective tissue properties and mixed epithelial or unclassified tumours (n = 385) were excluded, as were male cases and cases of unknown age or sex (n = 211). A patient flow chart is depicted in Fig. 1. In total, 25,302 patients were analysed in this study. YA breast cancer patients (n = 736; 2.9 %) were defined as <35 years of age, MA patients (n = 6905; 27.3 %) as between 35 and 50 years of age at onset, and OA patients (n = 17,661; 69.8 %) as >50 years of age at onset. Clinicopathological and prognostic factors were compared between the three groups. For the analysis of survival, patients who did not undergo surgery (n = 312; 1.2 %), patients who had Stage IV or an unknown disease stage (n = 987; 3.9 %), and patients with unavailable event data (n = 212; 0.8 %) were excluded.
Fig. 1.

Patient flow chart
Statistical analyses
Fisher’s exact tests were used to compare various prevalence rates among the three patient groups. Unpaired Student’s t-tests were used for inter-group comparisons of continuous variables. Survival curves were constructed using the Kaplan–Meier method with and without stratification on known prognostic factors, and were compared using a log-rank test. Multivariable analyses for disease-free survival (DFS), breast cancer-specific survival (BCSS), and overall survival (OS) were performed using a Cox proportional hazards model to estimate the hazard ratios and 95 % confidence intervals for survival. We considered the following variables as potential confounders in the Cox model; age, TNM classification, breast cancer subtype, and neo-adjuvant/adjuvant therapy. Patients with any missing or unknown data were excluded from analysis of the Cox model. DFS was defined as the time interval between the date of surgery and the point of local or distant recurrence. BCSS and OS were defined as the time intervals between the date of surgery and the date of breast cancer-related death or death from any cause. A P value of <0.05 was considered statistically significant. All statistical analyses were conducted using SAS software version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Clinicopathological characteristics
Prognostic information was available for 736 YA patients (2.9 %), 6905 MA patients (27.3 %), and 17,661 OA patients (69.8 %), indicating that the minority of all breast cancers are YA cases, as previously reported (Table 1) [4–6].
Table 1.
Patient characteristicsa
| Patients’ age at onset | |||||||
|---|---|---|---|---|---|---|---|
| <35 (n = 736) | 35–50 (n = 6905) | 50– (n = 17,661) | |||||
| N | % | N | % | N | % | P value | |
| T stage | |||||||
| Tis | 73 | 9.9 | 795 | 11.5 | 1580 | 9.0 | <.001 |
| T0 | 5 | 0.7 | 97 | 1.4 | 233 | 1.3 | |
| T1 | 229 | 31.1 | 2655 | 38.5 | 6870 | 38.9 | |
| T2 | 301 | 40.9 | 2434 | 35.3 | 6475 | 36.7 | |
| T3 | 93 | 12.6 | 579 | 8.4 | 1243 | 7.0 | |
| T4 | 26 | 3.5 | 280 | 4.1 | 1109 | 6.3 | |
| Unk | 9 | 1.2 | 65 | 0.9 | 151 | 0.9 | |
| Nodal status | |||||||
| Negative | 515 | 70.0 | 5281 | 76.5 | 13,625 | 77.2 | <.001 |
| Positive | 210 | 28.5 | 1547 | 22.4 | 3825 | 21.7 | |
| Unk | 11 | 1.5 | 77 | 1.1 | 211 | 1.2 | |
| M | |||||||
| M0 | 692 | 94.0 | 6640 | 96.2 | 16848 | 95.4 | <.001 |
| M1 | 29 | 3.9 | 128 | 1.9 | 461 | 2.6 | |
| Unknown | 15 | 2.0 | 137 | 2.0 | 352 | 2.0 | |
| Stage | |||||||
| 0 | 73 | 9.9 | 795 | 11.5 | 1576 | 8.9 | <.001 |
| 1 | 202 | 27.5 | 2468 | 35.7 | 6354 | 36.0 | |
| 2 | 338 | 45.9 | 2886 | 41.8 | 7499 | 42.5 | |
| 3 | 78 | 10.6 | 535 | 7.8 | 1511 | 8.6 | |
| 4 | 29 | 3.9 | 128 | 1.9 | 461 | 2.6 | |
| Unknown | 16 | 2.2 | 93 | 1.4 | 260 | 1.5 | |
| ER | |||||||
| Negative | 195 | 26.5 | 1307 | 18.9 | 4578 | 25.9 | <.001 |
| Positive | 517 | 70.2 | 5353 | 77.5 | 12544 | 71.0 | |
| Unknown | 24 | 3.3 | 245 | 3.6 | 539 | 3.1 | |
| PR | |||||||
| Negative | 263 | 335.7 | 1647 | 23.9 | 7594 | 43.0 | <.001 |
| Positive | 447 | 60.7 | 4997 | 72.4 | 9460 | 53.6 | |
| Unknown | 26 | 3.5 | 261 | 3.8 | 607 | 3.4 | |
| HER2 | |||||||
| Negative | 554 | 75.3 | 5231 | 75.8 | 12961 | 73.4 | <.001 |
| Positive | 101 | 13.7 | 806 | 11.7 | 2582 | 14.6 | |
| Unknown | 81 | 11.0 | 868 | 12.9 | 2118 | 12.0 | |
| Surgery | |||||||
| None | 1 | 0.1 | 4 | 0.1 | 18 | 0.1 | <.001 |
| BCT | 456 | 62.0 | 4070 | 58.9 | 9092 | 51.5 | |
| Mastectomy | 256 | 34.8 | 2671 | 38.7 | 8115 | 45.9 | |
| Others | 16 | 2.2 | 97 | 1.4 | 217 | 1.2 | |
| Unknown | 7 | 1.0 | 63 | 0.9 | 219 | 1.2 | |
| Adjuvant therapy | |||||||
| None | 126 | 17.1 | 1036 | 15.0 | 3414 | 19.3 | <.001 |
| ET | 252 | 34.2 | 2899 | 42.0 | 7725 | 43.7 | |
| ET + CT | 197 | 26.8 | 1834 | 26.6 | 3133 | 17.7 | |
| CT | 122 | 16.6 | 879 | 12.7 | 2701 | 15.3 | |
| Unknown | 39 | 5.3 | 257 | 3.7 | 688 | 3.9 | |
Bold P value <0.05
aTNM classification is shown based on the sixth edition of the Unio Internationalis Contra Cancrum staging system; ER estrogen receptor, PR progesteron receptor, HER2 human epidermal growth factorreceptor 2, BCT breast conserving therapy, ET endocrine therapy, CT Chemo therapy
YA patients were more likely to be diagnosed with a larger tumour (e.g., T3: YA patients, 12.6 %; MA patients, 8.4 %; and OA patients, 7.0 %; P < 0.001), Tis (ductal carcinoma in situ) occurred most frequently in MA patients (11.5 %) and T1 occurred more frequently in MA (38.5 %) and OA patients (38.9 %) compared to YA patients (31.1 %; P < 0.001). A greater proportion of YA patients (28.5 %) had a positive nodal status compared to MA (22.4 %) and OA patients (21.7 %; P < 0.001). Distant metastasis (M status) also occurred significantly more frequently in YA patients compared to MA and OA patients (P < 0.001). Moreover, an advanced TNM classification (Stage III/IV) occurred more frequently in YA patients (14.5 %) compared to MA (9.6 %) and OA patients (11.2 %; P < 0.001). YA patients were also associated with an aggressive breast cancer receptor status. Specifically, the proportion of ER-negative tumours was higher in YA patients compared to MA and OA patients (P < 0.001), although the difference in frequencies between YA (26.5 %) and OA patients (25.9 %) was small. A similar trend was observed in the HER2-positive group in which YA patients (13.7 %) were more frequent than MA patients (11.7 %) (P < 0.001; Table 1).
In regard to the type of surgery conducted, YA patients (62.0 %) underwent BCT more frequently compared to MA (58.9 %) and OA patients (51.5 %; P < 0.001). Adjuvant systemic therapies (endocrine therapy alone, combination chemo-endocrine therapy, chemotherapy alone, and no adjuvant therapy) were also compared. The uptake of adjuvant endocrine therapy alone was significantly lower in YA patients compared to MA and OA patients (P < 0.001). Conversely, YA patients were administered chemotherapy and combination chemo-endocrine therapy more frequently compared to MA and OA patients (P < 0.001; Table 1).
Prognosis
At 5-year follow-up, 3103 cases (12.3 %) of breast cancer recurrence, 1311 cases (5.2 %) of breast cancer-related death, and 1900 cases (7.5 %) of all-cause death were reported. The 5-year DFS rates were 79.4, 88.5, and 87.8 % for YA, MA, and OA patients, respectively. The 5-year BCSS and OS rates were 92.1 and 90.8 % for YA, 95.8 and 95.0 % for MA, and 94.6 and 91.6 % for OA patients.
YA patients were associated with a significantly poorer prognosis in relation to DFS, BCSS, and OS (P < 0.001; Fig. 2) in the univariate analysis, indicating that these results are consistent with previously reported data [9–13]. We subsequently assessed the prognostic value of young age at onset in breast cancer, stratifying on known clinicopathological prognostic factors. Stratifying on breast cancer receptor status (HER2-positive/ER-positive, HER2-positive/ER-negative, HER2-negative/ER-positive, and triple receptor negative breast cancer), YA patients were found to be significantly associated with a poorer prognosis in all breast cancer receptor subtypes (P < 0.05; Fig. 3). In ER-positive cases, there was no difference on recurrence pattern by age at onset in the early phase during this study period, and YA cases had poorer prognosis than the older cases in the late phase(Fig. 3a, b). Conversely, in ER-negative cases, the distinct pattern of the recurrence by age at onset was seen only in the early phase and no difference in the late phase(Fig. 3c, d). TNM stage, another well-known clinicopathological prognostic factor, was also stratified. YA patients were associated with a significantly poorer prognosis in the Stage I and Stage II groups (P < 0.001; Fig. S1). In the Stage 0 group, YA, MA, and OA patients with ductal carcinoma in situ were associated with similarly favourable prognoses with statistically marginal effect (P = 0.053; Fig. S1). Conversely, in the Stage III group, YA patients exhibited a trend towards a poorer prognosis. However, this was not statistically significant (P = 0.121; Fig. S1).
Fig. 2.
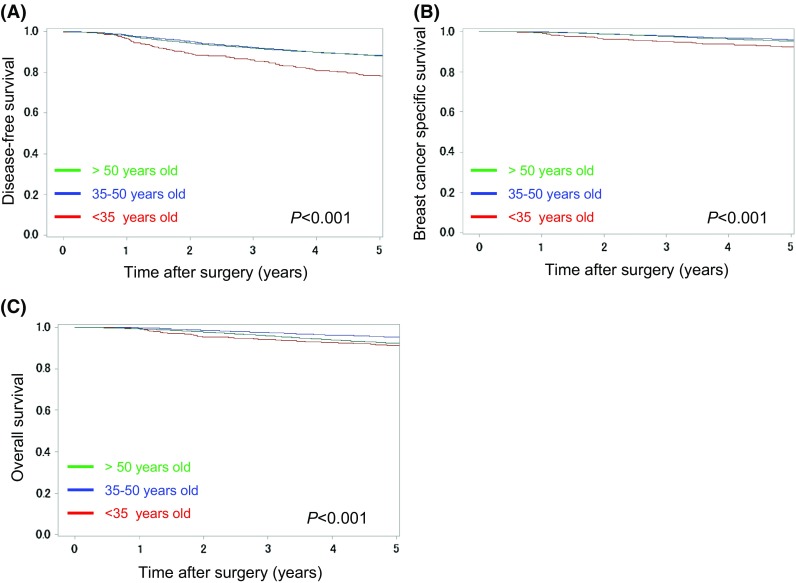
Kaplan–Meier curves for a disease-free survival, b breast cancer-specific survival, and c overall survival between young adult (<35 years; red line), middle-aged adult (35–50 years; blue line), and older adult (>50 years; green line) breast cancer patients. P-values were calculated using a log-rank test
Fig. 3.
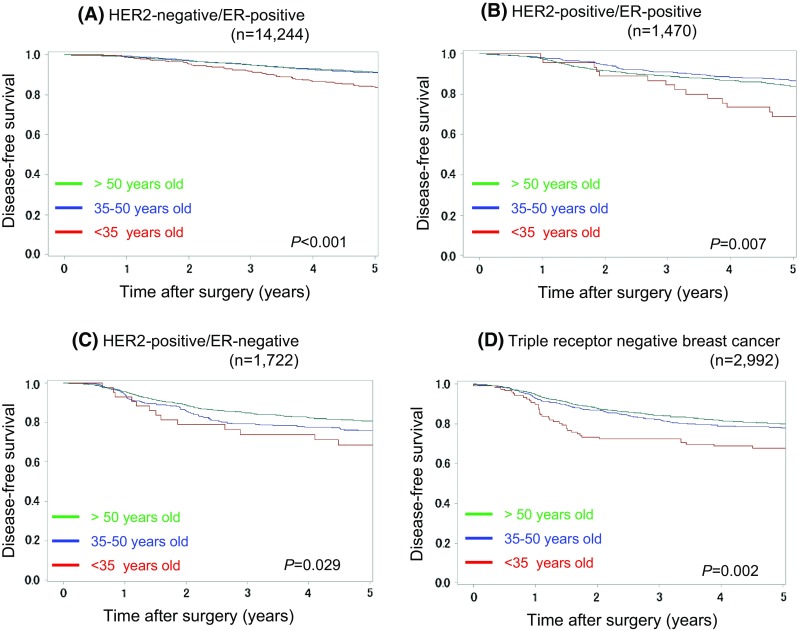
Kaplan–Meier curves for disease-free survival between young adult (<35 years; red line), middle-aged adult (35–50 years; blue line), and older adult (>50 years; green line) patients with a HER2-negative/ER-positive, b HER2-positive/ER-positive, c HER2-positive/ER-negative, and d triple receptor negative breast cancer. P-values were calculated using a log-rank test
Finally, multivariable Cox regression analysis was performed using a young age at onset adjusted by known breast cancer prognostic factors, including T/N status, breast cancer subtypes, and adjuvant therapies. YA patients were significantly associated with the poorest prognosis for all three endpoints, 5-year DFS, BCSS, and OS. Specifically, both comparisons between YA and MA patients (hazard ratio 1.58, 95 % confidence interval 1.16–2.15; P < 0.01) and between YA and OA patients (hazard ratio: 1.52, 95 % confidence interval 1.33–1.75; P < 0.001) were significant for OS (Table 2).
Table 2.
Multivariate analysis for 5 year survivala
| Hazard ratio | 95 % C.I. | P value | Hazard ratio | 95 % C.I. | P value | Hazard ratio | 95 % C.I. | P value | |
|---|---|---|---|---|---|---|---|---|---|
| Age at diagonosis | |||||||||
| <35 versus 35–50 | 1.73 | 1.42–2.10 | <.001 | 1.52 | 1.09–2.13 | 0.098 | 1.58 | 1.16–2.15 | 0.004 |
| Over 50 versus 35–50 | 0.99 | 0.821 | 1.14 | 0.98–1.34 | 0.015 | 1.52 | 1.33–1.75 | <.001 | |
| T | |||||||||
| T2–4 versus T0, 1 | 2.22 | 0.90–1.09 | <.001 | 3.04 | 2.49–3.70 | <.001 | 2.25 | 1.96–2.59 | <.001 |
| N | |||||||||
| Positive versus negative | 2.81 | 2.01–2.46 | <.001 | 4.01 | 3.46–4.64 | <.001 | 3.05 | 2.72–3.43 | <.001 |
| Breast cancer subtype | |||||||||
| ER+HER2+ versus ER+HER2− | 1.52 | 2.58–3.07 | <.001 | 1.73 | 1.35–2.23 | <.001 | 1.39 | 1.13–1.72 | 0.002 |
| ER−HER2+ versus ER+HER2− | 1.86 | 1.65–2.11 | <.001 | 2.33 | 1.89–2.88 | <.001 | 1.75 | 1.47–2.07 | <.001 |
| Triple negative versus ER + HER2− | 2.06 | 1.86–2.28 | <.001 | 4.48 | 3.84–5.23 | <.001 | 3.08 | 2.72–3.50 | <.001 |
| Adjuvant therapy | |||||||||
| Any versus none | 0.87 | 0.76–1.00 | 0.041 | 1.32 | 1.03–1.71 | 0.032 | 0.70 | 0.60–0.81 | <.001 |
Bold P value < 0.05
a DFS disease-free survival, BCSS breast cancer specific survival, OS overall survival; TNM classification is shown based on the 6th edition of the Unio Internationalis Contra Cancrum staging system; ER estrogen receptor, HER2 human epidermal growth factor receptor 2
Discussion
YA breast cancer accounts for a minority of breast cancer cases [6].
Consequently, it is unlikely that a prospective clinical trial would ever be conducted to define the optimal treatment strategy for this disease subset.
We analysed data from a large number of breast cancer patients registered by the Japanese Breast Cancer Registry database in order to characterise and advance our understanding of YA breast cancer. Using nationwide, population-based data representing approximately 70 % of all newly diagnosed breast cancer patients in Japan between 2004 and 2006, we were able to circumvent many problems associated with single institutional experiences or limited sample sizes. Our study demonstrated that a young age at onset was an independent predictive factor for poor prognosis in patients with breast cancer, after adjustment of well-known clinicopathological factors, including breast cancer receptor status, tumour size, and nodal status. Classically, it has been suggested that YA breast cancer patients are associated with a poorer prognosis because of delayed diagnosis at an advanced stage, a larger tumour size, and higher incidences of HER2-positive/ER-negative tumours [6, 9]. These reports proved consistent with our findings in the present study. Some previously published studies have already established a poorer prognosis in YA breast cancer patients as independent from other clinicopathological factors, such as tumour size, nodal status, histological grade, and hormone receptor status [8, 18, 19]. However, these reports are relatively old, have smaller sample sizes, and patients may have been treated with a classical adjuvant chemotherapy and endocrine therapy regimen. Recently, some studies using large databases have also reported similarly poor prognostic outcomes in YA breast cancer patients after stratifying on multiple prognostic factors [20–23]. Conversely, a single study has found that a young age at onset has no influence on the prognosis of individual breast cancer patients from a database of almost 3000 cases [24]. Partridge et al. [12] also reported no effect of age on breast cancer outcomes in patients with HER2-positive breast cancer from a large, randomised controlled trial. At the St Gallen International Expert Consensus meetings, a younger age at onset had been considered a high-risk factor from the 1990s to 2009. Later, a younger age at onset was no longer considered to be a poor prognostic factor and treatment strategies were recommended based on biological subtype or the concept of a ‘threshold for indication’ of each systemic treatment modality to be respected without a young age at onset [25]. Then, YA patients were treated according to various predictive factors and the subtype of the tumour, including ER, PR, and HER2 status, proliferation markers, and TNM classification and a young age itself had no impact on the treatment strategy. Based on our findings and the results of several previously published reports of large cohorts [20–23], YA breast cancer patients have a poor prognosis independent of other aggressive breast cancer features.
Another interesting finding was distinct recurrence pattern between ER-positive and -negative entities according to age at onset (Fig. 3). These differences between age at onset and ER status may lead to the distinct biological and molecular processes of age at onset by ER status. Research highlighting the genetic differences between YA and other breast cancer entities by ER status is lacking. Anders et al. [11] reported that YA breast cancer represents a unique biological entity driven by unifying a higher probability of phosphoinositide 3-kinase and Myc pathway dysregulation. Investigating how high-risk genetic mutations affect age at onset, Ford et al. [26] observed that 5.3 % of breast cancers in <40 year olds are attributable to BRCA1 mutations compared 2.2 % and 1.1 % in 40- to 49-year olds and 50- to 70-year olds, respectively. It has been established that patients with BRCA1 mutations are more likely to develop basal-like breast cancers, including the triple-negative subtype [27, 28] [29, 30]. Further research to elucidate the development of disease in this high-risk YA population and to determine the prognosis following a diagnosis of breast cancer is clearly warranted. An improved understanding of breast cancer genetics through molecular profiling may provide information that can be applied to patients with YA breast cancer.
Efficacy to adjuvant therapy in YA breast cancer patients remains controversial. Ahn et al. [10] reported that the survival differences according to age in hormone receptor-positive breast cancer patients were significant in patients who received hormone therapy as well as those who did not. This suggests YA breast cancer patients may need another strategy of treatment instead of conventional adjuvant hormone and chemo therapy. A similarly insufficient efficacy to chemotherapy has also been reported. YA breast cancer patients treated with adjuvant cyclophosphamide, methotrexate, and fluorouracil are at a higher risk of relapse and death compared to older breast cancer patients [31].
These distinct genetic patterns and clinical outcomes may lead to individual management of breast cancer patients. Previous studies reported significantly higher rates of local recurrence in YA patients who received BCT compared to OA patients who underwent a mastectomy [32, 33]. Freedoman et al. [34] reported that YA breast cancer patients were significantly more likely to have a mastectomy than BCT compared to older breast cancer patients. Efforts are required to confirm whether different types of surgery effect not only local recurrence rates but also OS rates. [35].
This study had several limitations. First, the relatively short follow-up period (median 4.5 years), which limited the power of the survival analysis. Nevertheless, prognostic analyses from this database that have previously been published were relatively consistent with the well-known consensus and clinical outcomes [36–38]. Second, during the study period, trastuzumab (which should exert a favourable effect on HER2-positive breast cancers) had not been widely prescribed as the standard agent and was only partially received. Third, we have no proliferation data, such as grade and genomic signatures. They are primarily prognostic and secondary predictive markers to chemotherapy response especially in ER-positive cases.
In conclusion, the present study confirmed that YA breast cancer patients have a poor prognosis independent of well-known clinicopathological prognostic factors. The different prognoses between YA, MA, and OA patients may require different screening algorithms, therapies, and follow-up. In order to establish an optimal strategy for YA breast cancer patients, further studies will need to be conducted.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Fig. S1: Kaplan–Meier curves for disease-free survival between young adult (<35 years; red line), middle-aged adult (35–50 years; blue line), and older adult (>50 years; green line) patients with (A) Stage 0, (B) Stage I, (C) Stage II, and (D) Stage III breast cancer. P-values were calculated using a log-rank test (PPTX 119 kb)
Acknowledgments
The authors thank the Public Health Research Foundation for their data collection and analysis. They also thank the affiliated institutes participating in the Breast Cancer Registry of the JBCS for their efforts to register patients’ data.
Funding
This work was supported by the research fund from the JBCS and JSPS KAKENHI Grant Numbers 15H04796.
Compliance with ethical standards
Conflict of Interest
AT, HK, and HM are affiliated with the Department of Healthcare Quality Assessment at the University of Tokyo, and the department is endowed by Johnson & Johnson K.K., Nipro Corporation, Teijin Pharma Ltd., Kaketsuken K.K., St. Jude Medical Japan Co., Ltd., Novartis Pharma K.K., Taiho Pharmaceutical Co., Ltd., W. L. Gore & Associates, Co., Ltd., Olympus Corporation, and Chugai Pharmaceutical Co., Ltd. The other authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or JBCS and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
The study was approved by the review boards of JBCS. The study used only unidentifiable patient information, and no informed consent was required.
Research involving human and animal rights
This article does not contain any studies with animals performed by any of the authors.
References
- 1.Soliman H, Agresta SV. Current issues in adolescent and young adult cancer survivorship. Cancer Control. 2008;15(1):55–62. doi: 10.1177/107327480801500107. [DOI] [PubMed] [Google Scholar]
- 2.Zebrack B. Information and service needs for young adult cancer patients. Support Care Cancer. 2008;16(12):1353–1360. doi: 10.1007/s00520-008-0435-z. [DOI] [PubMed] [Google Scholar]
- 3.http://seer.cancer.gov/archive/csr/1975_2011/ [Accessed 19 April 2016]
- 4.Yankaskas BC. Epidemiology of breast cancer in young women. Breast Dis. 2005;23:3–8. doi: 10.3233/BD-2006-23102. [DOI] [PubMed] [Google Scholar]
- 5.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. doi: 10.3322/caac.21166. [DOI] [PubMed] [Google Scholar]
- 6.Kataoka A, Tokunaga E, Masuda N, Shien T, Kawabata K, Miyashita M. Clinicopathological features of young patients (<35 years of age) with breast cancer in a Japanese Breast Cancer Society supported study. Breast cancer. 2014;21(6):643–650. doi: 10.1007/s12282-013-0466-2. [DOI] [PubMed] [Google Scholar]
- 7.Kroman N, Jensen MB, Wohlfahrt J, Mouridsen HT, Andersen PK, Melbye M. Factors influencing the effect of age on prognosis in breast cancer: population based study. BMJ. 2000;320(7233):474–478. doi: 10.1136/bmj.320.7233.474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nixon AJ, Neuberg D, Hayes DF, Gelman R, Connolly JL, Schnitt S, Abner A, Recht A, Vicini F, Harris JR. Relationship of patient age to pathologic features of the tumor and prognosis for patients with stage I or II breast cancer. J Clin Oncol. 1994;12(5):888–894. doi: 10.1200/JCO.1994.12.5.888. [DOI] [PubMed] [Google Scholar]
- 9.Gonzalez-Angulo AM, Broglio K, Kau SW, Eralp Y, Erlichman J, Valero V, Theriault R, Booser D, Buzdar AU, Hortobagyi GN, Arun B. Women age ≤35 years with primary breast carcinoma: disease features at presentation. Cancer. 2005;103(12):2466–2472. doi: 10.1002/cncr.21070. [DOI] [PubMed] [Google Scholar]
- 10.Ahn SH, Son BH, Kim SW, Kim SI, Jeong J, Ko SS, Han W, Korean Breast Cancer S. Poor outcome of hormone receptor-positive breast cancer at very young age is due to tamoxifen resistance: nationwide survival data in Korea–a report from the Korean Breast Cancer Society. J Clin Oncol. 2007;25(17):2360–2368. doi: 10.1200/JCO.2006.10.3754. [DOI] [PubMed] [Google Scholar]
- 11.Anders CK, Hsu DS, Broadwater G, Acharya CR, Foekens JA, Zhang Y, Wang Y, Marcom PK, Marks JR, Febbo PG, Nevins JR, Potti A, Blackwell KL. Young age at diagnosis correlates with worse prognosis and defines a subset of breast cancers with shared patterns of gene expression. J Clin Oncol. 2008;26(20):3324–3330. doi: 10.1200/JCO.2007.14.2471. [DOI] [PubMed] [Google Scholar]
- 12.Partridge AH, Gelber S, Piccart-Gebhart MJ, Focant F, Scullion M, Holmes E, Winer EP, Gelber RD. Effect of age on breast cancer outcomes in women with human epidermal growth factor receptor 2-positive breast cancer: results from a herceptin adjuvant trial. J Clin Oncol. 2013;31(21):2692–2698. doi: 10.1200/JCO.2012.44.1956. [DOI] [PubMed] [Google Scholar]
- 13.McGuire A, Brown JA, Malone C, McLaughlin R, Kerin MJ. Effects of age on the detection and management of breast cancer. Cancers. 2015;7(2):908–929. doi: 10.3390/cancers7020815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kurebayashi J, Miyoshi Y, Ishikawa T, Saji S, Sugie T, Suzuki T, Takahashi S, Nozaki M, Yamashita H, Tokuda Y, Nakamura S. Clinicopathological characteristics of breast cancer and trends in the management of breast cancer patients in Japan: based on the Breast Cancer Registry of the Japanese Breast Cancer Society between 2004 and 2011. Breast Cancer. 2015;22(3):235–244. doi: 10.1007/s12282-015-0599-6. [DOI] [PubMed] [Google Scholar]
- 15.Greene F. TNM classification of malignant tumours. 6. New York: Wiley; 2002. pp. 131–141. [Google Scholar]
- 16.The Japanese Breast Cancer Society, editor. General rules for clinical and pathological recording of breast cancer. 17. Tokyo: Kanehara Shuppan; 2012. [Google Scholar]
- 17.Lakhani S, Ellis I, Schnitt S, Tan P, van de Vijver M. WHO classification of tumours of the breast. 4. Lyon: IARC Press; 2012. [Google Scholar]
- 18.de la Rochefordiere A, Asselain B, Campana F, Scholl SM, Fenton J, Vilcoq JR, Durand JC, Pouillart P, Magdelenat H, Fourquet A. Age as prognostic factor in premenopausal breast carcinoma. Lancet. 1993;341(8852):1039–1043. doi: 10.1016/0140-6736(93)92407-K. [DOI] [PubMed] [Google Scholar]
- 19.Albain KS, Allred DC, Clark GM. Breast cancer outcome and predictors of outcome: are there age differentials? J Natl Cancer Inst Monogr. 1994;16:35–42. [PubMed] [Google Scholar]
- 20.Gnerlich JL, Deshpande AD, Jeffe DB, Sweet A, White N, Margenthaler JA. Elevated breast cancer mortality in women younger than age 40 years compared with older women is attributed to poorer survival in early-stage disease. J Am Coll Surg. 2009;208(3):341–347. doi: 10.1016/j.jamcollsurg.2008.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cancello G, Maisonneuve P, Rotmensz N, Viale G, Mastropasqua MG, Pruneri G, Veronesi P, Torrisi R, Montagna E, Luini A, Intra M, Gentilini O, Ghisini R, Goldhirsch A, Colleoni M. Prognosis and adjuvant treatment effects in selected breast cancer subtypes of very young women (<35 years) with operable breast cancer. Ann Oncol. 2010;21(10):1974–1981. doi: 10.1093/annonc/mdq072. [DOI] [PubMed] [Google Scholar]
- 22.Han W, Kang SY, Korean Breast Cancer S. Relationship between age at diagnosis and outcome of premenopausal breast cancer: age less than 35 years is a reasonable cut-off for defining young age-onset breast cancer. Breast Cancer Res Treat. 2010;119(1):193–200. doi: 10.1007/s10549-009-0388-z. [DOI] [PubMed] [Google Scholar]
- 23.Azim HA, Jr, Michiels S, Bedard PL, Singhal SK, Criscitiello C, Ignatiadis M, Haibe-Kains B, Piccart MJ, Sotiriou C, Loi S. Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin Cancer Res. 2012;18(5):1341–1351. doi: 10.1158/1078-0432.CCR-11-2599. [DOI] [PubMed] [Google Scholar]
- 24.Kollias J, Elston CW, Ellis IO, Robertson JF, Blamey RW. Early-onset breast cancer–histopathological and prognostic considerations. Br J Cancer. 1997;75(9):1318–1323. doi: 10.1038/bjc.1997.223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Goldhirsch A, Ingle JN, Gelber RD, Coates AS, Thurlimann B, Senn HJ, Panel m. Thresholds for therapies: highlights of the St Gallen International Expert Consensus on the primary therapy of early breast cancer 2009. Ann Oncol. 2009;20(8):1319–1329. doi: 10.1093/annonc/mdp322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ford D, Easton DF, Peto J. Estimates of the gene frequency of BRCA1 and its contribution to breast and ovarian cancer incidence. Am J Hum Genet. 1995;57(6):1457–1462. [PMC free article] [PubMed] [Google Scholar]
- 27.Honrado E, Benitez J, Palacios J. The molecular pathology of hereditary breast cancer: genetic testing and therapeutic implications. Mod Pathol. 2005;18(10):1305–1320. doi: 10.1038/modpathol.3800453. [DOI] [PubMed] [Google Scholar]
- 28.Cancer Genome Atlas N. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70. doi: 10.1038/nature11412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Balmana J, Domchek SM, Tutt A, Garber JE. Stumbling blocks on the path to personalized medicine in breast cancer: the case of PARP inhibitors for BRCA1/2-associated cancers. Cancer Discov. 2011;1(1):29–34. doi: 10.1158/2159-8274.CD-11-0048. [DOI] [PubMed] [Google Scholar]
- 30.Azim HA, Jr, Partridge AH. Biology of breast cancer in young women. Breast Cancer Res. 2014;16(4):427. doi: 10.1186/s13058-014-0427-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Aebi S, Gelber S, Castiglione-Gertsch M, Gelber RD, Collins J, Thurlimann B, Rudenstam CM, Lindtner J, Crivellari D, Cortes-Funes H, Simoncini E, Werner ID, Coates AS, Goldhirsch A. Is chemotherapy alone adequate for young women with oestrogen-receptor-positive breast cancer? Lancet. 2000;355(9218):1869–1874. doi: 10.1016/S0140-6736(00)02292-3. [DOI] [PubMed] [Google Scholar]
- 32.Voogd AC, Nielsen M, Peterse JL, Blichert-Toft M, Bartelink H, Overgaard M, van Tienhoven G, Andersen KW, Sylvester RJ, van Dongen JA, Danish Breast Cancer Cooperative Group. Breast Cancer Cooperative Group of the European Organization for R, Treatment of C Differences in risk factors for local and distant recurrence after breast-conserving therapy or mastectomy for stage I and II breast cancer: pooled results of two large European randomized trials. Journal of Clin Oncol. 2001;19(6):1688–1697. doi: 10.1200/JCO.2001.19.6.1688. [DOI] [PubMed] [Google Scholar]
- 33.de Bock GH, van der Hage JA, Putter H, Bonnema J, Bartelink H, van de Velde CJ. Isolated loco-regional recurrence of breast cancer is more common in young patients and following breast conserving therapy: long-term results of European Organisation for Research and Treatment of Cancer studies. Eur J Cancer. 2006;42(3):351–356. doi: 10.1016/j.ejca.2005.10.006. [DOI] [PubMed] [Google Scholar]
- 34.Freedman RA, Virgo KS, Labadie J, He Y, Partridge AH, Keating NL. Receipt of locoregional therapy among young women with breast cancer. Breast Cancer Res Treat. 2012;135(3):893–906. doi: 10.1007/s10549-012-2156-8. [DOI] [PubMed] [Google Scholar]
- 35.Ohuchi N, Suzuki A, Sobue T, Kawai M, Yamamoto S, Zheng YF, Shiono YN, Saito H, Kuriyama S, Tohno E, Endo T, Fukao A, Tsuji I, Yamaguchi T, Ohashi Y, Fukuda M, Ishida T, groups JSi Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan strategic anti-cancer randomized trial (J-START): a randomised controlled trial. Lancet. 2016;387(10016):341–348. doi: 10.1016/S0140-6736(15)00774-6. [DOI] [PubMed] [Google Scholar]
- 36.Kinoshita T, Fukui N, Anan K, Iwamoto T, Niikura N, Kawai M, Hayashi N, Tsugawa K, Aogi K, Ishida T, Masuoka H, Masuda S, Iijima K, Nakamura S, Tokuda Y. Comprehensive prognostic report of the Japanese Breast Cancer Society Registry in 2004. Breast Cancer. 2015 doi: 10.1007/s12282-015-0644-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Anan K, Fukui N, Kinoshita T, Iwamoto T, Niikura N, Kawai M, Hayashi N, Tsugawa K, Aogi K, Ishida T, Masuoka H, Masuda S, Iijima K, Nakamura S, Tokuda Y. Comprehensive prognostic report of the Japanese Breast Cancer Society Registry in 2005. Breast Cancer. 2015 doi: 10.1007/s12282-015-0645-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Iwamoto T, Fukui N, Kinoshita T, Anan K, Niikura N, Kawai M, Hayashi N, Tsugawa K, Aogi K, Ishida T, Masuoka H, Masuda S, Iijima K, Nakamura S, Tokuda Y. Comprehensive prognostic report of the Japanese Breast Cancer Society registry in 2006. Breast Cancer. 2015 doi: 10.1007/s12282-015-0646-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig. S1: Kaplan–Meier curves for disease-free survival between young adult (<35 years; red line), middle-aged adult (35–50 years; blue line), and older adult (>50 years; green line) patients with (A) Stage 0, (B) Stage I, (C) Stage II, and (D) Stage III breast cancer. P-values were calculated using a log-rank test (PPTX 119 kb)