

Abstract
Objectives
To compare patient-reported outcomes (PROs) in methotrexate (MTX)-naive patients (defined as no prior treatment or ≤3 doses) receiving tofacitinib versus MTX.
Methods
In the 24-month, phase III, randomised, controlled, ORAL Start trial (NCT01039688), patients were randomised 2:2:1 to receive tofacitinib 5 mg two times per day (n=373), tofacitinib 10 mg two times per day (n=397) or MTX (n=186). PROs assessed included Patient Global Assessment of disease (PtGA), pain, Health Assessment Questionnaire-Disability Index (HAQ-DI), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) and health-related quality of life (Short Form-36 [SF-36]).
Results
PROs improved following tofacitinib and MTX treatment: benefits were sustained over 24 months. Patients receiving tofacitinib reported earlier responses which were significantly different between each tofacitinib dose and MTX at month 3 through month 24. At month 6 (primary end point), significant improvements versus MTX were observed in PtGA, pain, HAQ-DI, SF-36 Physical Component Summary (PCS), 5/8 domain scores and FACIT-F with tofacitinib 5 mg two times per day; all PROs, except SF-36 Mental Component Summary Score and Medical Outcomes Survey-Sleep, with tofacitinib 10 mg two times per day. At month 6, the proportion of patients reporting improvements ≥minimum clinically important difference were significant versus MTX with tofacitinib 5 mg two times per day in PtGA and 3/8 SF-36 domains; and with tofacitinib 10 mg two times per day in PtGA, pain, HAQ-DI, SF-36 PCS, 4/8 domains and FACIT-F.
Conclusions
Patients with rheumatoid arthritis receiving tofacitinib 5 and 10 mg two times per day monotherapy versus MTX reported statistically significant and clinically meaningful improvements in multiple PROs over 24 months; onset of benefit with tofacitinib treatment occurred earlier.
Trial registration number
Keywords: Methotrexate, Rheumatoid Arthritis, Patient perspective
Key messages.
Both tofacitinib monotherapy doses and MTX improved PROs; however, patients treated with tofacitinib reported earlier responses.
Significant differences in improvement between tofacitinib and MTX were evident by month 3 and persisted.
Improvements ≥MCID at month 6 were significant with tofacitinib versus MTX for multiple PROs.
Introduction
Rheumatoid arthritis (RA) is a chronic and debilitating autoimmune disease characterised by systemic inflammation, persistent synovitis and joint destruction. RA affects all aspects of health-related quality of life (HRQoL).1 2
Patients and physicians rate RA disease differently—while physicians focus on RA-specific clinical and radiographic outcomes, patients focus on how their General Health (GH) is affected by RA, which may lead to discordance.3–6 Patient-reported outcomes (PROs) reflect how patients with RA feel and function;7 8 therefore, an effective treatment for RA should offer benefits in terms of Physical Functioning (PF), Emotional Functioning and Social Functioning (SF), as well as clinical and radiographic end points.9–11 Furthermore, the importance of incorporating PROs into the design of randomised controlled trials (RCTs) has been emphasised by Outcome Measures in Rheumatology (OMERACT) international consensus effort, American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR).7 12–15
Tofacitinib is an oral Janus kinase (JAK) inhibitor for treatment of RA. Tofacitinib preferentially inhibits signalling by heterodimeric receptors associated with JAK3 and JAK1, with functional selectivity over receptors that signal via pairs of JAK2.16 17 Tofacitinib 5 and 10 mg two times per day have been investigated in six phase III RCTs as monotherapy or in combination with conventional disease-modifying antirheumatic drugs (DMARDs), predominantly methotrexate (MTX), in patients with RA.18–23
This RCT, ORAL Start, was designed to investigate the effects of tofacitinib monotherapy versus MTX in patients who were MTX-naive (defined as no prior treatment or ≤3 doses) over 24 months. This phase III RCT (ClinicalTrials.gov ID NCT01039688; Pfizer protocol A3921069) demonstrated that tofacitinib monotherapy resulted in clinically and statistically significant reductions in signs and symptoms of RA, improvements in PF and statistically significant inhibition of progression of structural damage compared with MTX, reported previously.21 The safety profile was similar to that previously reported in tofacitinib trials. Here we report the PRO data from this RCT.
Methods
Trial design and patients
This RCT was conducted across 151 centres worldwide; full details have been reported previously.21 Patients were ≥18 years of age with a diagnosis of RA according to the ACR 1987 Revised Criteria24 and active disease, defined as ≥6 tender and swollen joints (of 68/66 joints examined), with either erythrocyte sedimentation rate >28 mm/hour (Westergren method) or C reactive protein >7 mg/L. Patients were randomised (2:2:1) to receive tofacitinib 5 mg two times per day or tofacitinib 10 mg two times per day monotherapy (hereafter referred to as tofacitinib 5 mg and tofacitinib 10 mg), or MTX starting at 10 mg/week, increasing in increments of 5 mg/week every month to 20 mg/week by week 8.
The trial was designed to detect differences between MTX and tofacitinib 5 or 10 mg in two primary efficacy end points at month 6: ACR70 response rates (at least 90% power) and inhibition of structural damage, measured by change from baseline in modified total Sharp score. All other (efficacy) assessments were predefined as secondary end points. After the publication of the results, one of its study sites (eight patients randomised) was found non-compliant to study procedures and those patients have been removed from the PRO analyses presented here.
The trial was approved by Institutional Review Boards (IRBs) and/or Independent Ethics Committees at each investigational centre or a central IRB, and conducted in accordance with the Declaration of Helsinki and International Conference on Harmonisation Good Clinical Practice Guidelines. All patients provided written informed consent.
Assessment of PROs
The following PROs (components of the ACR response criteria) were included as predefined end points: Patient Global Assessment of disease (PtGA), pain (assessed by 100 mm visual analogue scales (VAS)) and physical function by Health Assessment Questionnaire-Disability Index (HAQ-DI). Other predefined secondary end points included HRQoL using Medical Outcomes Survey (MOS) Short Form-36 (SF-36; V.2, acute) questionnaire, fatigue by Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale and quality of sleep using MOS-Sleep scale.25 26
Minimum clinically important differences (MCIDs) were defined as: ≥10 mm decreases from baseline in PtGA and pain VAS scores;27 ≥0.22 point decrease from baseline in HAQ-DI;15 25 ≥2.5 point increases from baseline in SF-36 Physical Component Summary (PCS) and MCS scores; ≥5 point increases from baseline in SF-36 domain scores;15 25 and a 4-point increase from baseline in FACIT-F.25 MCID is not available for MOS-Sleep.28
PtGA, pain, HAQ-DI and SF-36 scores were measured at all time points (baseline, months 1, 2, 3, 6, 9, 12, 15, 18, 21 and 24); FACIT-F and MOS-Sleep at baseline, months 1, 2, 3, 6, 12, 18 and 24. The proportion of patients reporting improvements ≥MCID were compared between tofacitinib and MTX treatment groups at months 3, 6, 12 and 24.
Statistical analyses
End points were expressed as mean changes from baseline and analysed using a linear mixed-effects repeated-measures model. This model was based on the full analysis set (FAS; all patients who received ≥1 dose of study drug and with ≥1 postbaseline assessment). Treatment, visit, treatment-by-visit interaction and baseline were included as fixed effects, as well as disease duration at baseline and region of investigative site; patients were included as random effects, employing the method of maximum likelihood using least squares (LS) estimates for parameters such as mean changes from baseline (for each treatment) as well as mean differences (each tofacitinib treatment vs MTX), hereafter LS mean (LSM). Corresponding SEs for these estimates were also derived.
The percentage of patients reporting improvements ≥MCID and scores meeting or exceeding normative values were compared between tofacitinib and MTX treatment groups using the normal approximation to the binomial (FAS, no imputation). All end points presented were prespecified, except for percentages of patients reporting improvements ≥MCID for FACIT-F and percentages of patients whose scores met or exceeded normative values.
Statistical significance was declared at p<0.05, with no correction for multiple comparisons.
Number needed to treat (NNT; the number of patients who need to be treated for one patient to achieve an improvement in outcome) was calculated as 1/(proportion of patients in the tofacitinib group reporting improvements ≥MCID minus the proportion of patients in the MTX group reporting improvements ≥MCID).29
Results
Patients
Of 958 patients randomised, 373 received tofacitinib 5 mg, 397 tofacitinib 10 mg and 186 MTX (total=956). Two hundred and ninety-eight patients discontinued treatment: 80 (43.0%) with MTX compared with 107 (28.7%) and 111 (28.0%) for tofacitinib 5 and 10 mg, respectively. Most common reasons for discontinuation were adverse events with tofacitinib 5 mg (n=38) and tofacitinib 10 mg (n=39), and lack of efficacy with MTX (n=26).
Baseline values
Prior treatments, patient demographics and baseline disease characteristics were similar across treatment groups.21 Mean disease duration was 2.7–3.4 years; 65.5% and 53.9% of patients had disease duration <2 years and <1 year, respectively. Baseline mean PtGA, pain and HAQ-DI scores indicated impaired physical function (table 1). Large decrements in reported HRQoL were evident by PCS scores ∼1.5–2.0 SDs below the normative score of 50, and lower domain scores compared with an age-matched and gender-matched US non-disease population (figure 1).
Table 1.
PROs at baseline and LSM changes from baseline at months 3, 6, 12 and 24
| PRO | Baseline mean (SD) |
Month 3 LSM change from baseline (SE) |
Month 6 LSM change from baseline (SE) |
Month 12 LSM change from baseline (SE) |
Month 24 LSM change from baseline (SE) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tofacitinib 5 mg two times per day N=370 |
Tofacitinib 10 mg two times per day N=393 |
MTX N=184 |
Tofacitinib 5 mg two times per day N=351 |
Tofacitinib 10 mg two times per day N=380 |
MTX N=169 |
Tofacitinib 5 mg two times per day N=337 |
Tofacitinib 10 mg two times per day N=363 |
MTX N=156 |
Tofacitinib 5 mg two times per day N=312 |
Tofacitinib 10 mg two times per day N=328 |
MTX N=133 |
Tofacitinib 5 mg two times per day N=261 |
Tofacitinib 10 mg two times per day N=278 |
MTX N=105 |
|
| Patient Global Assessment | 60.42 (24.49) | 60.88 (22.55)a | 57.91 (24.33) | –30.12 (1.19)b** | –31.79 (1.13)c*** | –22.63 (1.67) | –31.86 (1.20)d* | –35.10 (1.15)e** | –27.67 (1.71) | –32.94 (1.23)f* | –34.63 (1.19)g*** | –26.18 (1.80) | –34.41 (1.29)h* | –35.79 (1.24)i* | –28.95 (1.94) |
| Pain | 59.23 (23.86) | 61.38 (23.06)a | 59.00 (23.61) | –30.04 (1.19)b** | –33.01 (1.13)c*** | –22.77 (1.67)j | –32.11 (1.20)k | –35.35 (1.15)e** | –28.34 (1.71) | –32.46 (1.23)l* | –35.85 (1.19)m** | –27.98 (1.80) | –34.79 (1.29)* | –37.62 (1.25)i** | –29.67 (1.94) |
| HAQ-DI | 1.54 (0.64) | 1.50 (0.67) | 1.53 (0.65) | –0.76 (0.03)*** | –0.86 (0.03)c*** | –0.48 (0.04) | –0.84 (0.03)*** | –0.94 (0.03)e*** | –0.59 (0.04) | –0.88 (0.03)** | –0.98 (0.03)m*** | –0.69 (0.04) | –0.91 (0.03)** | –1.02 (0.03)*** | –0.71 (0.05) |
| SF-36 | |||||||||||||||
| PCS | 32.82 (7.25) | 33.19 (7.33)n | 33.51 (7.83)o | 9.26 (0.43)*** | 10.34 (0.42)p*** | 5.06 (0.61) | 9.74 (0.44)*** | 11.26 (0.42)e*** | 6.66 (0.62)q | 10.34 (0.45)** | 12.37 (0.43)m*** | 7.55 (0.65)r | 11.14 (0.46)*** | 12.49 (0.45)*** | 7.72 (0.69) |
| MCS | 40.47 (12.05) | 40.69 (11.76)n | 40.86 (11.30)o | 6.19 (0.51)* | 5.85 (0.49)p | 4.33 (0.72) | 6.43 (0.52) | 6.49 (0.50)e | 4.92 (0.74)q | 6.27 (0.53) | 6.60 (0.51)m* | 4.69 (0.77)r | 6.20 (0.55) | 7.44 (0.53) | 5.59 (0.83) |
| SF-36 domain | |||||||||||||||
| PF | 30.13 (9.44) | 31.58 (9.88) | 32.04 (9.59) | 9.17 (0.52)*** | 10.16 (0.50)c*** | 4.33 (0.73)j | 9.73 (0.53)*** | 11.37 (0.51)*** | 5.75 (0.75) | 10.68 (0.54)** | 12.71 (0.52)m*** | 7.37 (0.78) | 11.74 (0.56)** | 13.04 (0.54)*** | 7.92 (0.83) |
| RP | 33.43 (9.58) | 34.10 (9.37) | 33.88 (9.39) | 8.86 (0.49)*** | 9.81 (0.46)c*** | 5.27 (0.68)j | 9.70 (0.49)** | 10.64 (0.47)*** | 6.68 (0.69) | 9.86 (0.50)* | 11.74 (0.48)*** | 7.10 (0.72) | 10.41 (0.52)* | 12.26 (0.50)*** | 7.84 (0.77) |
| BP | 33.19 (8.04) | 33.23 (7.22) | 33.77 (7.57)o | 10.72 (0.48)*** | 11.50 (0.46)c*** | 6.89 (0.68) | 11.00 (0.49)* | 12.59 (0.47)*** | 8.46 (0.70)q | 11.70 (0.50)** | 13.35 (0.48)*** | 8.54 (0.73)r | 12.18 (0.53)* | 13.80 (0.51)*** | 9.19 (0.79) |
| GH | 37.96 (9.01) | 37.20 (8.56) | 37.51 (8.56) | 6.08 (0.41)* | 6.45 (0.40)c** | 3.95 (0.58)j | 6.19 (0.42) | 6.81 (0.40)* | 4.99 (0.59) | 6.12 (0.43) | 7.21 (0.41)* | 5.36 (0.62) | 6.49 (0.44)* | 7.41 (0.43)** | 4.88 (0.66) |
| VT | 41.79 (9.89) | 41.55 (9.96)n | 41.62 (9.49) | 8.20 (0.50)** | 8.84 (0.48)p*** | 5.06 (0.70)j | 8.41 (0.50)* | 8.64 (0.48)e* | 6.01 (0.71) | 8.40 (0.51)* | 9.37 (0.50)* | 6.50 (0.75) | 8.23 (0.54) | 9.33 (0.52)* | 6.62 (0.79) |
| SF | 36.38 (11.35) | 36.67 (11.10) | 37.52 (11.33) | 8.14 (0.51)** | 7.86 (0.48)c* | 5.22 (0.71)j | 8.50 (0.51) | 9.20 (0.49)* | 6.99 (0.73) | 8.54 (0.52)* | 9.59 (0.50)*** | 5.87 (0.76) | 9.09 (0.55)* | 10.40 (0.53)** | 6.94 (0.82) |
| RE | 33.98 (13.36) | 34.73 (13.09) | 34.67 (12.61) | 7.26 (0.57)* | 7.64 (0.54)c** | 4.35 (0.80)j | 7.60 (0.57) | 9.09 (0.55) ** | 5.70 (0.82) | 7.65 (0.58) | 9.30 (0.56)** | 5.93 (0.85) | 8.64 (0.61) | 10.41 (0.59)** | 6.62 (0.92) |
| MH | 38.85 (11.92) | 39.42 (11.77)n | 39.72 (11.35) | 6.64 (0.53)* | 6.35 (0.50)p | 4.66 (0.74)j | 7.08 (0.53)* | 6.79 (0.51)e* | 4.63 (0.76) | 7.31 (0.54)* | 7.33 (0.52)* | 5.28 (0.79) | 6.81 (0.57) | 8.02 (0.55) | 6.38 (0.85) |
| FACIT-F | 28.43 (10.94) | 29.01 (10.73) | 28.49 (10.57)o | 8.19 (0.48)s** | 8.72 (0.46)c*** | 5.33 (0.67)t | 8.83 (0.48)* | 9.13 (0.46)e** | 6.45 (0.69) | 8.85 (0.49)* | 9.17 (0.48)g* | 6.91 (0.71) | 8.94 (0.51)* | 9.56 (0.49)i** | 6.32 (0.76) |
| MOS-Sleep | 42.68 (19.55)u | 42.86 (20.56)a | 42.99 (18.09) | –12.60 (0.88)s* | –11.12 (0.83)c | –9.11 (1.22)j | –11.76 (0.88)k | –12.28 (0.84) | –9.83 (1.25) | –12.34 (0.90)l* | –11.94 (0.87)m | –9.20 (1.31) | –11.57 (0.94) | –11.80 (0.91)v | –10.84 (1.40) |
Baseline data and LSM change from baseline data at months 6, 12 and 24 for HAQ-DI, and significance versus MTX, were reported previously21 and are presented here for comparison. Baseline values are descriptive; LSM change from baseline data are FAS, longitudinal model.
*p<0.05; **p<0.001; ***p<0.0001 vs MTX.
aN=394; bN=348; cN=379; dN=335; eN=362; fN=310; gN=326; hN=260; iN=277; jN=170; kN=336; lN=311; mN=327; nN=392; oN=183; pN=378; qN=155; rN=132; sN=349; tN=168; uN=369; vN=276.
BP, Bodily Pain; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; FAS, full analysis set; GH, General Health; HAQ-DI, Health Assessment Questionnaire-Disability Index; LSM, least squares mean; MCS, Mental Component Score; MH, Mental Health; MOS, Medical Outcomes Study; MTX, methotrexate; Pain, Patient Assessment of Arthritis Pain; PCS, Physical Component Score; PF, Physical Functioning; PROs, patient-reported outcomes; RE, Role Emotional; RP, Role Physical; SF, Social Functioning; SF-36, Short Form-36; VT, Vitality.
Figure 1.

Spydergrams displaying SF-36 domains at months 3, 6, 12 and 24. Study values were normed using population mean and SDs.51 52 BID, two times per day; BP, Bodily Pain; GH, General Health; MH, Mental Health; PF, Physical Functioning; RE, Role Emotional; RP, Role Physical; SF, Social Functioning; SF-36, Short Form-36; VT, Vitality.
Patient-reported outcomes
Patient Global Assessment of Disease activity
Patients who received tofacitinib 5 or 10 mg reported improvements from baseline in PtGA that were significant (p<0.05) versus MTX at all time points from month 1 to month 24 (table 1 and figure 2A); maximal effects were observed by month 6. Compared with MTX, significantly more (p<0.05) patients who received tofacitinib reported improvements ≥MCID at months 3, 6, 12 and 24 (figure 3A). NNTs ranged from 7.2 to 10.4 with tofacitinib 5 mg and from 5.9 to 9.7 with tofacitinib 10 mg (figure 3).
Figure 2.

LSM change (SE) from baseline in (A) PtGA, (B) pain, (C) HAQ-DI and (D) FACIT-F. *p<0.05; **p<0.001; ***p<0.0001 vs MTX. FAS, longitudinal model. BID, two times a day; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; FAS, full analysis set; HAQ-DI, Health Assessment Questionnaire-Disability Index; LSM, least squares mean; PtGA, Patient Global Assessment of Disease.
Figure 3.
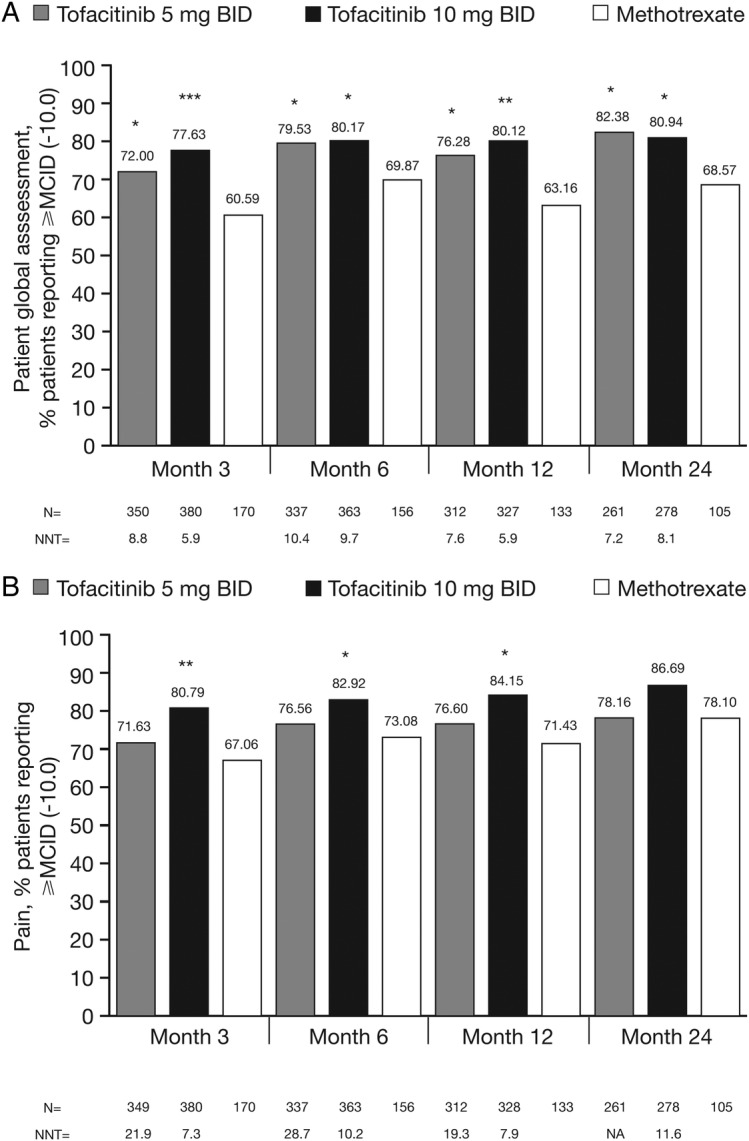
Percentage of patients reporting improvements ≥MCID and NNTs to achieve an MCID in (A) PtGA, (B) pain, (C) HAQ-DI, (D) FACIT-F and (E) SF-36 domains and summary scores. In (E) (SF-36), each bar is divided by colour (white, black or grey) to represent the treatment groups. The number displayed within each treatment group is the percentage of patients reporting improvements ≥MCID (number of patients achieving MCID divided by the total number of patients in that treatment group). The number displayed in parentheses is the NNT of that treatment compared with MTX. *p<0.05; **p<0.001; ***p<0.0001 vs MTX. All data are FAS, no imputation. BID, two times a day; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; FAS, full analysis set; HAQ-DI, Health Assessment Questionnaire-Disability Index; HRQoL, health-related quality of life; MCID, minimum clinically important difference; MTX, methotrexate; NA, not applicable (ie, NNT is negative); NNT, numbers needed to treat; Pain, Patient Assessment of Arthritis Pain; SF-36, Short Form-36.
Figure 2.

Continued
Figure 3.

Continued
Pain
Significant improvements from baseline in pain (p<0.05) versus MTX were seen at all time points from month 1 for patients who received tofacitinib 10 mg and at all time points with the exception of month 6 for those receiving tofacitinib 5 mg (table 1 and figure 2B). At months 3, 6 and 12, more patients (p<0.05) receiving tofacitinib 10 mg reported improvements ≥MCID versus MTX. NNTs were lower with tofacitinib 10 mg compared with tofacitinib 5 mg, ranging from 7.3 to 10.2 (figure 3B).
Health Assessment Questionnaire-Disability Index
Patients receiving tofacitinib reported improvements from baseline in HAQ-DI that were significant (p<0.05) versus MTX at all time points from month 1 to month 24 (table 1 and figure 3C). Significantly (p<0.05) more patients reported improvements ≥MCID in HAQ-DI with tofacitinib 10 mg versus MTX at months 3 and 6, with NNTs of 8.7 and 11.6, respectively (figure 3C). The proportions of patients who reported HAQ-DI values meeting or exceeding normative values were significantly greater with tofacitinib versus MTX at month 6 (p<0.001; table 2), month 12 and month 24 (p<0.05; data not shown).
Table 2.
Percentage of patients reporting scores ≥normative values for PROs at month 6
| Tofacitinib 5 mg two times per day N=337 |
Tofacitinib 10 mg two times per day N=363 |
MTX N=156 |
|
|---|---|---|---|
| HAQ-DI, n (%) | 149 (44.21)** | 195 (53.72)*** | 42 (26.92) |
| SF-36 domain, n (%) | |||
| PF | 99 (29.38)*** | 133 (36.64)*** | 22 (14.10) |
| RP | 104 (30.86)* | 133 (36.64)** | 33 (22.15) |
| BP | 122 (36.20)* | 153 (42.15)*** | 35 (22.44) |
| GH | 109 (32.34) | 111 (30.58) | 38 (24.36) |
| VT | 192 (56.97)* | 209 (57.58)* | 68 (43.59) |
| SF | 144 (42.73) | 166 (45.73) | 65 (41.67) |
| RE | 113 (33.53) | 138 (38.02) | 46 (29.49) |
| MH | 142 (42.14)* | 157 (43.25)* | 45 (28.85) |
| FACIT-F, n (%) | 147 (43.62) | 183 (50.41)* | 55 (35.26) |
*p<0.05; **p<0.001; ***p<0.0001 vs MTX.
BP, Bodily Pain; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; GH, General Health; HAQ-DI, Health Assessment Questionnaire-Disability Index; MH, Mental Health; MTX, methotrexate; PF, Physical Functioning; PROs, patient-reported outcomes; RE, Role Emotional; RP, Role Physical; SF, Social Functioning; SF-36, Short Form-36; VT, Vitality.
Functional Assessment of Chronic Illness Therapy-Fatigue
Patients who received tofacitinib reported significant (p<0.05) improvements from baseline in FACIT-F versus MTX at all time points from month 1 (table 1 and figure 2). At month 3, significantly more patients in both tofacitinib groups reported improvements ≥MCID in FACIT-F versus MTX (p<0.05); at month 6, significant improvements were evident with tofacitinib 10 mg but not with tofacitinib 5 mg (figure 3D). NNTs at all time points were lower with tofacitinib 10 mg than with tofacitinib 5 mg (figure 3D). At months 6, 12 and 24, significantly (p<0.05) more patients receiving tofacitinib 10 mg two times per day versus MTX reported scores ≥normative values for FACIT-F (table 2); significant improvement was evident with tofacitinib 5 mg two times per day at month 12.
HRQoL by SF-36
Patients in both tofacitinib treatment arms reported LSM changes from baseline in PCS scores that were significant (p<0.001) versus MTX at months 3, 6, 12 and 24. The proportion of patients reporting improvements ≥MCID in PCS scores was significant (p<0.05) versus MTX at month 3 for both tofacitinib doses and months 6, 12 and 24 for tofacitinib 10 mg (table 1). LSM changes from baseline in MCS scores with tofacitinib exceeded MTX at months 3, 6, 12 and 24, but were significant (p<0.05) versus MTX at month 3 for tofacitinib 5 mg and month 12 for tofacitinib 10 mg (table 1). The proportion of patients receiving tofacitinib 10 mg who reported improvements ≥MCID in MCS scores was significant (p<0.05) versus MTX at months 12 and 24 (figure 3E). NNTs were therefore lower with tofacitinib 10 mg versus tofacitinib 5 mg for PCS and MCS scores.
Significant (p<0.05) improvements versus MTX were reported with tofacitinib 5 mg in PF, Role Physical (RP) and Bodily Pain (BP; months 3, 6, 12 and 24), GH (months 3 and 24), Vitality (VT) and Mental Health (MH) (months 3, 6 and 12), SF (months 3, 12 and 24) and Role Emotional (RE; month 3) domains (table 1). Patients who received tofacitinib 10 mg reported significant improvements versus MTX in PF, RP, BP, GH, VT, SF and RE (months 3, 6, 12 and 24), and MH (months 6 and 12) domains (table 1). Significantly more (p<0.05) patients who received tofacitinib 5 or 10 mg (vs MTX) reported improvements ≥MCID in all SF-36 domains at month 3. Additionally, significantly more patients reported improvements ≥MCID with tofacitinib 5 mg in PF, BP and MH domains at month 6, PF, BP and SF domains at month 12 and PF domain at month 24; and with tofacitinib 10 mg in PF, RP, BP and RE domains at month 6, PF, BP, SF, RE and MH domains at month 12 and PF, BP, VT, SF and MH at month 24 (figure 3E). Across SF-36 domains, NNTs were generally lower with tofacitinib 10 mg than with tofacitinib 5 mg (figure 3E). Significantly more (p<0.05) patients reported scores ≥normative values with tofacitinib 5 and 10 mg two times per day in PF, RP, BP, VT and MH domains at month 6 (table 2), PF, RP, SF and BP domains at month 12, and PF and BP domains at month 24 compared with MTX.
Medical Outcomes Survey-Sleep
In general, compared with MTX, patients in both tofacitinib treatment arms reported numerically greater improvements from baseline in MOS-Sleep scores at all time points. These changes were statistically significant versus MTX with tofacitinib 5 mg at months 3 and 12, but were not statistically significant versus MTX with tofacitinib 10 mg (table 1).
Discussion
In this paper, we report PROs from the phase III ORAL Start trial, which investigated the effects of tofacitinib monotherapy at two doses versus MTX in patients with active RA. This is the first investigation of tofacitinib monotherapy versus MTX in patients who were predominantly MTX-naive. Improvements in PROs in this ORAL Start trial were consistent with those reported in other tofacitinib phase III RCTs in DMARD and tumour necrosis factor inhibitor-inadequate responder populations.30–35
Patients in all active treatment groups reported improvements across multiple PROs. However, onset of treatment effect occurred earlier with tofacitinib than with MTX. Statistically significant differences between both tofacitinib doses and MTX were first evident as early as month 1 in the case of PtGA, pain, HAQ-DI and FACITF and months 3 and 6 in other outcomes. The benefits persisted over the length of the trial. In general across the PROs, the responses with tofacitinib 10 mg dose were numerically higher than those observed with tofacitinib 5 mg.
From the patient perspective, PF, pain, HRQoL and fatigue have been shown to be important outcomes in trials of active RA. In this RCT, treatment with tofacitinib 5 and 10 mg resulted in statistically significant LSM changes from baseline (p<0.005 vs MTX) in PtGA, pain, HAQ-DI, SF-36 PCS and FACIT-F scores from month 3. With only one exception (pain at month 6 in patients receiving tofacitinib 5 mg), these changes remained significant through month 24. In addition, clinically meaningful improvements over time were reported across all of these end points, most notably PtGA, although differences between treatment groups in the proportion reporting improvements ≥MCID were not consistently statistically significant. Together, improvements in PROs were consistent with ACR responses previously reported with tofacitinib versus MTX in this RCT.21
In comparison with an age-matched and gender-matched normative population, patients enrolled in ORAL Start reported markedly diminished HRQoL at baseline, based on SF-36 domain scores, indicating a substantial burden of disease. LSM changes from baseline and improvements ≥MCID in PCS and all SF-36 domains were statistically significant in tofacitinib-treated patients at month 3, except the MH domain with tofacitinib 10 mg. LSM changes from baseline reported by tofacitinib-treated patients at subsequent time points were sustained through month 24, although not necessarily statistically significant versus MTX at later time points, when additional later improvements with MTX were evident—consistent with the known time course of benefit of MTX.
In general, NNT values over time were numerically lower with tofacitinib 10 mg compared with tofacitinib 5 mg. It must be noted that although it is usual for NNTs to be calculated against a placebo control, in this analysis, NNT values were calculated in relation to the active control MTX. For most PRO measures, NNT values increased over time, which may be a reflection of the improvement in PRO outcomes with MTX generally occurring later than with tofacitinib.
Data from RCTs have demonstrated that the onset of benefit with MTX treatment is most evident 6 months after treatment initiation, with maximal benefit observed at 9–12 months;36–39 patients with earlier disease treated aggressively are more likely to respond. As this trial population included a majority of patients with disease of <1 year duration, and those randomised to MTX received aggressive treatment (10 mg/week titrated to 20 mg/week by month 2), clinically meaningful responses would be expected with MTX. Onset of benefit with tofacitinib treatment was more rapid than with MTX, reflected by statistically significant LSM changes from baseline ≥MCID for both tofacitinib doses versus MTX in all PROs at month 3, except pain, HAQ-DI and SF-36 MCS scores with tofacitinib 5 mg and SF-36 MCS score with tofacitinib 10 mg. Across all PROs, maximal benefit was achieved by month 6 in both tofacitinib treatment arms compared with 9–12 months with MTX.
Improvements in HRQoL observed in this trial were of similar magnitude and tempo of onset as observed with biological agents plus MTX compared with MTX monotherapy in MTX-naive patients, as reported with adalimumab, etanercept, golimumab and infliximab.38 40–46 In a phase III clinical trial of adalimumab, PROs including HAQ-DI, SF-36 PCS and FACIT-F scores were significantly improved with adalimumab 40 mg every other week plus MTX versus MTX monotherapy.46 A higher percentage of patients reported improvements in HAQ-DI ≥MCID with rituximab plus MTX (30%) compared with placebo plus MTX (15%) at year 2.47 Similarly, treatment with abatacept 10 mg/kg plus MTX resulted in greater improvements in SF-36 PCS and MCS, SF-36 domain scores and FACIT-F than placebo plus MTX.48 49 Patients enrolled in the GO-BEFORE RCT reported similar improvements in HAQ-DI and SF-36 PCS regardless of whether they received golimumab 50 mg plus MTX or MTX monotherapy.50 The limitations of this study have been reported previously.21
In summary, in the ORAL Start phase III RCT, patients with moderately to severely active RA who were MTX-naive reported improvements in PROs with tofacitinib 5 and 10 mg monotherapy that were statistically superior to MTX at month 3, occurred earlier and persisted through 24 months' treatment. These results provide further evidence that tofacitinib monotherapy not only improves signs and symptoms and inhibits progression of structural damage in RA but also improves pain, physical function, HRQoL and fatigue in a range of patient populations, and with more rapid onset of these benefits than MTX.
Acknowledgments
Anne Marie Reid, PhD, of Complete Medical Communications provided editorial support under the direction of authors, funded by Pfizer. Andrew Anisfeld, Elaine Hoffman, Ryan DeMasi and Lisy Wang, all employees of Pfizer, provided intellectual input during the manuscript development.
Footnotes
Funding: This work was supported by Pfizer.
Competing interests: VS and EBL are consultants for Pfizer. REA and RF have received research grants and are consultants for Pfizer. TK, SHZ, DG, BW, SK and GW are shareholders and employees of Pfizer.
Ethics approval: The trial was approved by Institutional Review Boards (IRBs) and/or Independent Ethics Committees at each investigational centre or a central IRB.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1.Kosinski M, Kujawski SC, Martin R et al. Health-related quality of life in early rheumatoid arthritis: impact of disease and treatment response. Am J Manag Care 2002;8:231–40. [PubMed] [Google Scholar]
- 2.Strand V, Singh JA. Newer biological agents in rheumatoid arthritis: impact on health-related quality of life and productivity. Drugs 2010;70:121–45. 10.2165/11531980-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 3.Khan NA, Spencer HJ, Abda E et al. Determinants of discordance in patients’ and physicians’ rating of rheumatoid arthritis disease activity. Arthritis Care Res (Hoboken) 2012;64:206–14. 10.1002/acr.20685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bartlett SJ, Hewlett S, Bingham CO III et al. Identifying core domains to assess flare in rheumatoid arthritis: an OMERACT international patient and provider combined Delphi consensus. Ann Rheum Dis 2012;71:1855–60. 10.1136/annrheumdis-2011-201201 [DOI] [PubMed] [Google Scholar]
- 5.Desthieux C, Hermet A, Granger B et al. Patient-physician discordance in global assessment in rheumatoid arthritis: a systematic literature review with metaanalysis. Arthritis Care Res (Hoboken) 2016; doi: 10.1002/acr.22902. [Epub ahead of print 5 Apr 2016] 10.1002/acr.22902 [DOI] [PubMed] [Google Scholar]
- 6.van Tuyl LH, Hewlett S, Sadlonova M et al. The patient perspective on remission in rheumatoid arthritis: ‘You've got limits, but you're back to being you again’. Ann Rheum Dis 2015;74:1004–10. 10.1136/annrheumdis-2013-204798 [DOI] [PubMed] [Google Scholar]
- 7.Kirwan JR, Hewlett SE, Heiberg T et al. Incorporating the patient perspective into outcome assessment in rheumatoid arthritis—progress at OMERACT 7. J Rheumatol 2005;32:2250–6. [PubMed] [Google Scholar]
- 8.van Tuyl LH, Sadlonova M, Davis B et al. Remission in rheumatoid arthritis: working toward incorporation of the patient perspective at OMERACT 12. J Rheumatol 2016;43:203–7. 10.3899/jrheum.141113 [DOI] [PubMed] [Google Scholar]
- 9.Fleischmann R, Strand V, Wilkinson B et al. Relationship between clinical and patient-reported outcomes in a phase 3 trial of tofacitinib or MTX in MTX-naïve patients with rheumatoid arthritis. RMD Open 2016;2:e000232 10.1136/rmdopen-2015-000232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Strand V, Kavanaugh A, Kivitz A et al. Long-term radiographic and patient-reported outcomes based on clinical disease activity index responses with tofacitinib at 6 months. Ann Rheum Dis 2016; 75(Supp 2):243. [Google Scholar]
- 11.Strand V, Kavanaugh A, Kivitz A et al. Long-term radiographic and patient-reported outcomes based on Clinical Disease Activity Index responses with tofacitinib at 6 months. Arthritis Rheumatol 2015;67(S10):Abstr 1633. [Google Scholar]
- 12.Felson DT, Anderson JJ, Boers M et al. The American College of Rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. The Committee on Outcome Measures in Rheumatoid Arthritis Clinical Trials. Arthritis Rheum 1993;36:729–40. [DOI] [PubMed] [Google Scholar]
- 13.Gossec L, Dougados M, Rincheval N et al. Elaboration of the preliminary Rheumatoid Arthritis Impact of Disease (RAID) score: a EULAR initiative. Ann Rheum Dis 2009;68:1680–5. 10.1136/ard.2008.100271 [DOI] [PubMed] [Google Scholar]
- 14.Kirwan JR, Tugwell PS. Overview of the patient perspective at OMERACT 10—conceptualizing methods for developing patient-reported outcomes. J Rheumatol 2011;38:1699–701. 10.3899/jrheum.110388 [DOI] [PubMed] [Google Scholar]
- 15.Strand V, Boers M, Idzerda L et al. It's good to feel better but it's better to feel good and even better to feel good as soon as possible for as long as possible. Response criteria and the importance of change at OMERACT 10. J Rheumatol 2011;38:1720–7. [DOI] [PubMed] [Google Scholar]
- 16.Ghoreschi K, Jesson MI, Li X et al. Modulation of innate and adaptive immune responses by tofacitinib (CP-690,550). J Immunol 2011;186:4234–43. 10.4049/jimmunol.1003668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Meyer DM, Jesson MI, Li X et al. Anti-inflammatory activity and neutrophil reductions mediated by the JAK1/JAK3 inhibitor, CP-690,550, in rat adjuvant-induced arthritis. J Inflamm (Lond) 2010;7:41 10.1186/1476-9255-7-41 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Burmester GR, Blanco R, Charles-Schoeman C et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: a randomised phase 3 trial. Lancet 2013;381:451–60. 10.1016/S0140-6736(12)61424-X [DOI] [PubMed] [Google Scholar]
- 19.Fleischmann R, Kremer J, Cush J et al. Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N Engl J Med 2012;367:495–507. 10.1056/NEJMoa1109071 [DOI] [PubMed] [Google Scholar]
- 20.Kremer J, Li ZG, Hall S et al. Tofacitinib in combination with nonbiologic disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis: a randomized trial. Ann Intern Med 2013;159:253–61. 10.7326/0003-4819-159-4-201308200-00006 [DOI] [PubMed] [Google Scholar]
- 21.Lee EB, Fleischmann R, Hall S et al. Tofacitinib versus methotrexate in rheumatoid arthritis. N Engl J Med 2014;370:2377–86. 10.1056/NEJMoa1310476 [DOI] [PubMed] [Google Scholar]
- 22.van der Heijde D, Tanaka Y, Fleischmann R et al. Tofacitinib (CP-690,550) in patients with rheumatoid arthritis receiving methotrexate: twelve-month data from a twenty-four-month phase III randomized radiographic study. Arthritis Rheum 2013;65:559–70. 10.1002/art.37816 [DOI] [PubMed] [Google Scholar]
- 23.van Vollenhoven RF, Fleischmann R, Cohen S et al. Tofacitinib or adalimumab versus placebo in rheumatoid arthritis. N Engl J Med 2012;367:508–19. 10.1056/NEJMoa1112072 [DOI] [PubMed] [Google Scholar]
- 24.Arnett FC, Edworthy SM, Bloch DA et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988;31:315–24. 10.1002/art.1780310302 [DOI] [PubMed] [Google Scholar]
- 25.Wells G, Li T, Maxwell L et al. Responsiveness of patient reported outcomes including fatigue, sleep quality, activity limitation, and quality of life following treatment with abatacept for rheumatoid arthritis. Ann Rheum Dis 2008;67:260–5. 10.1136/ard.2007.069690 [DOI] [PubMed] [Google Scholar]
- 26.Wells GA, Li T, Kirwan JR et al. Assessing quality of sleep in patients with rheumatoid arthritis. J Rheumatol 2009;36: 2077–86. 10.3899/jrheum.090362 [DOI] [PubMed] [Google Scholar]
- 27.Strand V, Scott DL, Emery P et al. Physical function and health related quality of life: analysis of 2-year data from randomized, controlled studies of leflunomide, sulfasalazine, or methotrexate in patients with active rheumatoid arthritis. J Rheumatol 2005;32:590–601. [PubMed] [Google Scholar]
- 28.Hays RD, Stewart AL. Sleep measures. In: Stewart AL, Ware JE Jr, eds Measuring functioning and well being. Durham: (NC: ): Duke University Press, 1992:235–9. [Google Scholar]
- 29.Christensen PM, Kristiansen IS. Number-needed-to-treat (NNT)—needs treatment with care. Basic Clin Pharmacol Toxicol 2006;99:12–6. 10.1111/j.1742-7843.2006.pto_412.x [DOI] [PubMed] [Google Scholar]
- 30.Burmester G, van der Heijde D, Strand V et al. Effects of tofacitinib on patient-reported outcomes in patients with active rheumatoid arthritis receiving stable dose methotrexate: results of two Phase 3 studies. Arthritis Rheum 2012;64(Suppl 10):549.21953306 [Google Scholar]
- 31.Strand V, van der Heijde D, Zerbini CAF et al. Oral Scan effects of the oral JAK inhibitor tofacitinib in combination with methotrexate on patient reported outcomes in a 24-month phase 3 trial of active rheumatoid arthritis. Arthritis Rheum 2013;65:S996, Abstract No. 2334 (abstract). [Google Scholar]
- 32.Strand V, Kanik K, Connell CA et al. The effects of the oral JAK inhibitor CP-690,550 on patient reported outcomes in a phase 3 study of active rheumatoid arthritis. Ann Rheum Dis 2011;70:88. [Google Scholar]
- 33.Strand V, Kremer J, Li ZG et al. Tofacitinib (CP-690,550) in combination with traditional disease-modifying anti-rheumatic drugs: patient-reported outcomes from a Phase 3 study in patients with active rheumatoid arthritis and an inadequate response to disease-modifying anti-rheumatic drugs. Arthritis Rheum 2011;63:S1032–3. [Google Scholar]
- 34.van Vollenhoven RF, Wallenstein G, Lee EB et al. Effects of tofacitinib (CP-690,550), an oral Janus kinase inhibitor, or adalimumab on patient reported outcomes in a phase 3 study of active rheumatoid arthritis. Ann Rheum Dis 2012;71:206 10.1136/annrheumdis-2012-eular.211621998118 [DOI] [Google Scholar]
- 35.Genovese MC, Han C, Keystone EC et al. Effect of golimumab on patient-reported outcomes in rheumatoid arthritis: results from the GO-FORWARD study. J Rheumatol 2012;39:1185–91. 10.3899/jrheum.111195 [DOI] [PubMed] [Google Scholar]
- 36.Bathon JM, Martin RW, Fleischmann RM et al. A comparison of etanercept and methotrexate in patients with early rheumatoid arthritis. N Engl J Med 2000;343:1586–93. 10.1056/NEJM200011303432201 [DOI] [PubMed] [Google Scholar]
- 37.Breedveld FC, Weisman MH, Kavanaugh AF et al. The PREMIER study: a multicenter, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum 2006;54:26–37. 10.1002/art.21519 [DOI] [PubMed] [Google Scholar]
- 38.Emery P, Breedveld FC, Lemmel EM et al. A comparison of the efficacy and safety of leflunomide and methotrexate for the treatment of rheumatoid arthritis. Rheumatology (Oxford) 2000;39:655–65. 10.1093/rheumatology/39.6.655 [DOI] [PubMed] [Google Scholar]
- 39.Jones G, Sebba A, Gu J et al. Comparison of tocilizumab monotherapy versus methotrexate monotherapy in patients with moderate to severe rheumatoid arthritis: the AMBITION study. Ann Rheum Dis 2010;69:88–96. 10.1136/ard.2008.105197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Strand V, Cohen S, Schiff M et al. Treatment of active rheumatoid arthritis with leflunomide compared with placebo and methotrexate. Leflunomide Rheumatoid Arthritis Investigators Group. Arch Intern Med 1999;159:2542–50. [DOI] [PubMed] [Google Scholar]
- 41.Strand V, Tugwell P, Bombardier C et al. Function and health-related quality of life: results from a randomized controlled trial of leflunomide versus methotrexate or placebo in patients with active rheumatoid arthritis. Leflunomide Rheumatoid Arthritis Investigators Group. Arthritis Rheum 1999;42:1870–8. [DOI] [PubMed] [Google Scholar]
- 42.St Clair EW, van der Heijde DM, Smolen JS et al. Combination of infliximab and methotrexate therapy for early rheumatoid arthritis: a randomized, controlled trial. Arthritis Rheum 2004;50:3432–43. 10.1002/art.20568 [DOI] [PubMed] [Google Scholar]
- 43.van der Heijde D, Klareskog L, Singh A et al. Patient reported outcomes in a trial of combination therapy with etanercept and methotrexate for rheumatoid arthritis: the TEMPO trial. Ann Rheum Dis 2006;65:328–34. 10.1136/ard.2005.035709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kekow J, Moots RJ, Emery P et al. Patient-reported outcomes improve with etanercept plus methotrexate in active early rheumatoid arthritis and the improvement is strongly associated with remission: the COMET trial. Ann Rheum Dis 2010;69:222–5. 10.1136/ard.2008.102509 [DOI] [PubMed] [Google Scholar]
- 45.Emery P, Fleischmann R, van der Heijde D et al. The effects of golimumab on radiographic progression in rheumatoid arthritis: results of randomized controlled studies of golimumab before methotrexate therapy and golimumab after methotrexate therapy. Arthritis Rheum 2011;63:1200–10. 10.1002/art.30263 [DOI] [PubMed] [Google Scholar]
- 46.Strand V, Rentz AM, Cifaldi MA et al. Health-related quality of life outcomes of adalimumab for patients with early rheumatoid arthritis: results from a randomized multicenter study. J Rheumatol 2012;39:63–72. 10.3899/jrheum.101161 [DOI] [PubMed] [Google Scholar]
- 47.Strand V, Balbir-Gurman A, Pavelka K et al. Sustained benefit in rheumatoid arthritis following one course of rituximab: improvements in physical function over 2 years. Rheumatology (Oxford) 2006;45:1505–13. 10.1093/rheumatology/kel358 [DOI] [PubMed] [Google Scholar]
- 48.Emery P, Kosinski M, Li T et al. Treatment of rheumatoid arthritis patients with abatacept and methotrexate significantly improved health-related quality of life. J Rheumatol 2006;33:681–9. [PubMed] [Google Scholar]
- 49.Russell AS, Wallenstein GV, Li T et al. Abatacept improves both the physical and mental health of patients with rheumatoid arthritis who have inadequate response to methotrexate treatment. Ann Rheum Dis 2007;66:189–94. 10.1136/ard.2006.057018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Emery P, Fleischmann RM, Strusberg I et al. Efficacy and safety of subcutaneous golimumab in methotrexate-naive patients with rheumatoid arthritis: five-year results of a randomized clinical trial. Arthritis Care Res (Hoboken) 2016;68:744–52. 10.1002/acr.22759 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ware JE, Kosinski M, Dewey JE. How to score version two of the SF-36 health survey. Lincoln: (RI: ): QualityMetric, Incorporated, 2000. [Google Scholar]
- 52.Strand V, Crawford B, Singh J et al. Use of “spydergrams” to present and interpret SF-36 health-related quality of life data across rheumatic diseases. Ann Rheum Dis 2009;68:1800–4. 10.1136/ard.2009.115550 [DOI] [PMC free article] [PubMed] [Google Scholar]