

Abstract
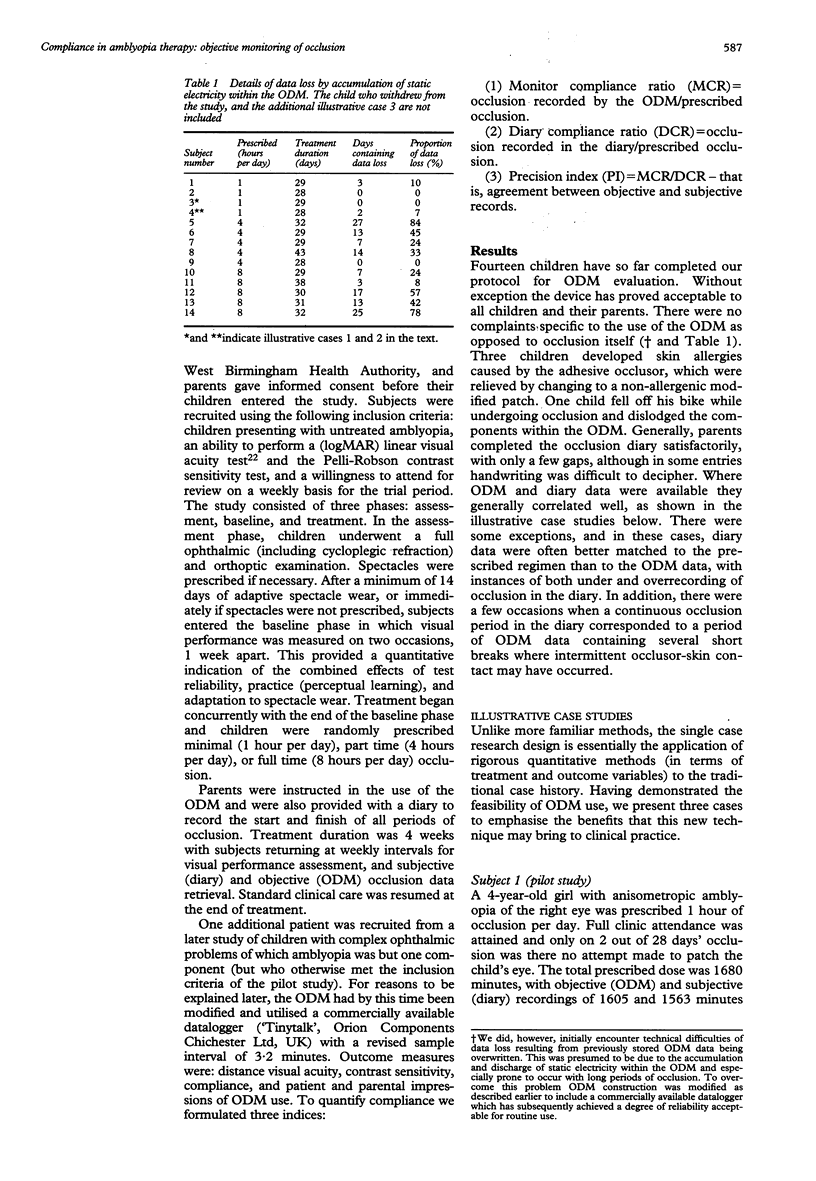
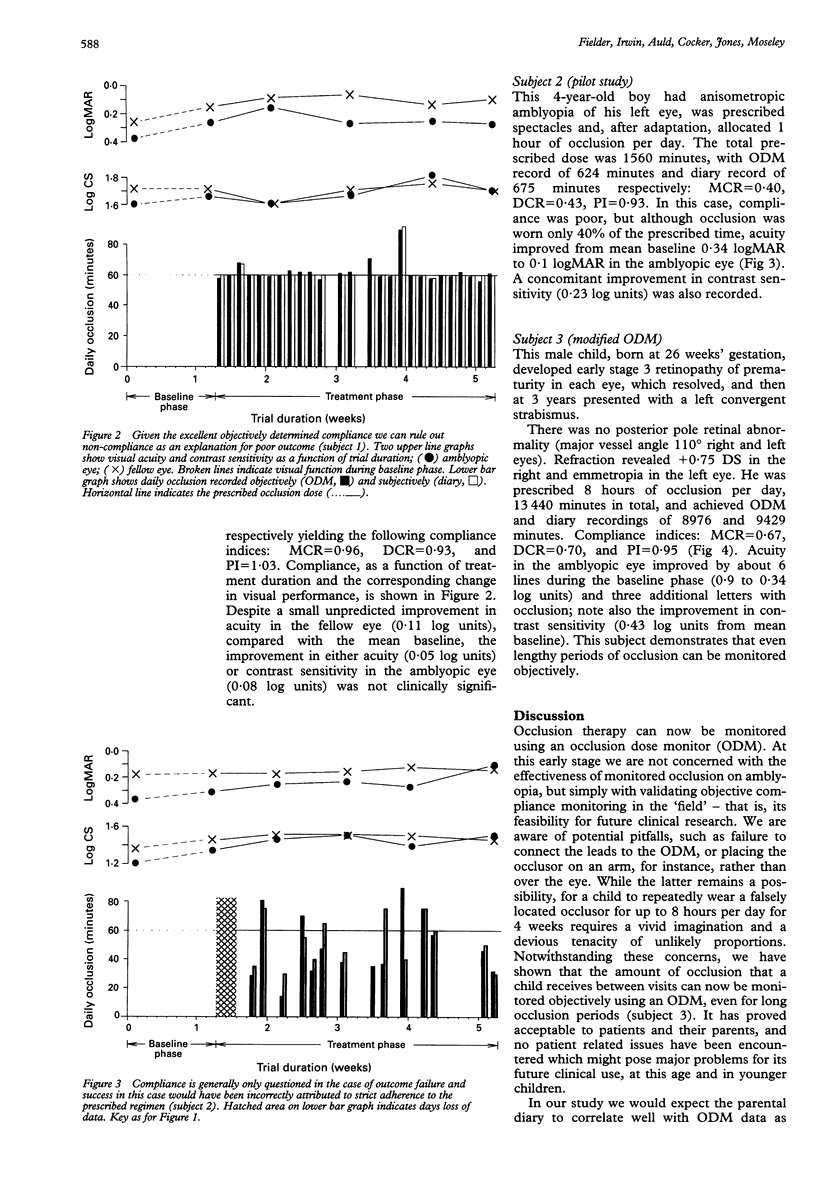
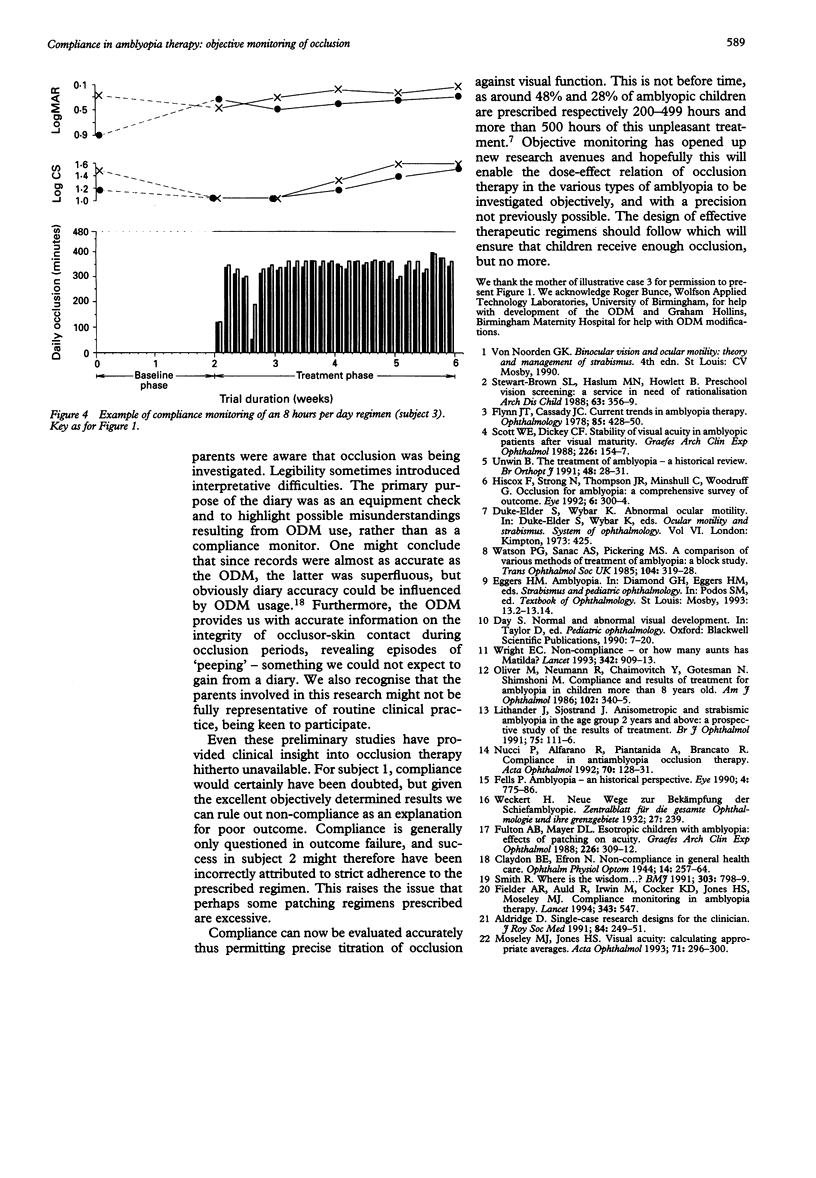
AIM/BACKGROUND--This study aimed to determine the feasibility of objective compliance monitoring of amblyopia therapy in clinical research. Occlusion has been the mainstay of amblyopia therapy for over 250 years, yet it has never been subjected to rigorous evaluation. Treatment regimens range arbitrarily from a few minutes to most of the waking hours of the day. Compliance is problematic and as, hitherto, accurate objective monitoring has been impossible it is not known how much occlusion is required to effect an improvement in vision. METHODS--An occlusion dose monitor (ODM) has been developed. The ODM consists of a modified occlusion patch and a miniature battery driven datalogger which periodically monitors patch skin contact. The patch is a standard disposable item with two miniature electrocardiogram electrodes attached to its undersurface. The datalogger comprises a high speed static RAM and a clock driven address counter. Data are retrieved using an IBM PC/AT computer. Fifteen child amblyopes were randomly allocated unilateral occlusion of 1, 4, or 8 hours per day for 4 weeks. Owing to data loss, presumed because of accumulation and discharge of static electricity, an additional child was included in the 8 hour group. Outcome measures were objective (ODM) and subjective (diary) compliance with treatment, logMAR visual acuity, and contrast sensitivity. RESULTS--Objective monitoring of occlusion is technically feasible and clinically informative. CONCLUSION--Objective monitoring of occlusion has opened up new research opportunities which, it is hoped, will enable the dose-effect relation of occlusion therapy in the various types of amblyopia to be investigated objectively, and facilitate the design of effective therapeutic regimens.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aldridge D. Single-case research designs for the clinician. J R Soc Med. 1991 May;84(5):249–252. doi: 10.1177/014107689108400502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Claydon B. E., Efron N. Non-compliance in general health care. Ophthalmic Physiol Opt. 1994 Jul;14(3):257–264. doi: 10.1111/j.1475-1313.1994.tb00006.x. [DOI] [PubMed] [Google Scholar]
- Fells P. Richardson Cross lecture 1989 amblyopia--an historical perspective. Eye (Lond) 1990;4(Pt 6):775–786. doi: 10.1038/eye.1990.122. [DOI] [PubMed] [Google Scholar]
- Fielder A. R., Auld R., Irwin M., Cocker K. D., Jones H. S., Moseley M. J. Compliance monitoring in amblyopia therapy. Lancet. 1994 Feb 26;343(8896):547–547. doi: 10.1016/s0140-6736(94)91502-4. [DOI] [PubMed] [Google Scholar]
- Flynn J. T., Cassady J. C. Current trends in amblyopia therapy. Ophthalmology. 1978 May;85(5):428–450. doi: 10.1016/s0161-6420(78)35651-7. [DOI] [PubMed] [Google Scholar]
- Fulton A. B., Mayer D. L. Esotropic children with amblyopia: effects of patching on acuity. Graefes Arch Clin Exp Ophthalmol. 1988;226(4):309–312. doi: 10.1007/BF02172956. [DOI] [PubMed] [Google Scholar]
- Hiscox F., Strong N., Thompson J. R., Minshull C., Woodruff G. Occlusion for amblyopia: a comprehensive survey of outcome. Eye (Lond) 1992;6(Pt 3):300–304. doi: 10.1038/eye.1992.59. [DOI] [PubMed] [Google Scholar]
- Lithander J., Sjöstrand J. Anisometropic and strabismic amblyopia in the age group 2 years and above: a prospective study of the results of treatment. Br J Ophthalmol. 1991 Feb;75(2):111–116. doi: 10.1136/bjo.75.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moseley M. J., Jones H. S. Visual acuity: calculating appropriate averages. Acta Ophthalmol (Copenh) 1993 Jun;71(3):296–300. doi: 10.1111/j.1755-3768.1993.tb07138.x. [DOI] [PubMed] [Google Scholar]
- Nucci P., Alfarano R., Piantanida A., Brancato R. Compliance in antiamblyopia occlusion therapy. Acta Ophthalmol (Copenh) 1992 Feb;70(1):128–131. doi: 10.1111/j.1755-3768.1992.tb02104.x. [DOI] [PubMed] [Google Scholar]
- Oliver M., Neumann R., Chaimovitch Y., Gotesman N., Shimshoni M. Compliance and results of treatment for amblyopia in children more than 8 years old. Am J Ophthalmol. 1986 Sep 15;102(3):340–345. doi: 10.1016/0002-9394(86)90008-5. [DOI] [PubMed] [Google Scholar]
- Scott W. E., Dickey C. F. Stability of visual acuity in amblyopic patients after visual maturity. Graefes Arch Clin Exp Ophthalmol. 1988;226(2):154–157. doi: 10.1007/BF02173306. [DOI] [PubMed] [Google Scholar]
- Smith R. Where is the wisdom...? BMJ. 1991 Oct 5;303(6806):798–799. doi: 10.1136/bmj.303.6806.798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart-Brown S. L., Haslum M. N., Howlett B. Preschool vision screening: a service in need of rationalisation. Arch Dis Child. 1988 Apr;63(4):356–359. doi: 10.1136/adc.63.4.356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson P. G., Sanac A. S., Pickering M. S. A comparison of various methods of treatment of amblyopia. A block study. Trans Ophthalmol Soc U K. 1985;104(Pt 3):319–328. [PubMed] [Google Scholar]
- Wright E. C. Non-compliance--or how many aunts has Matilda? Lancet. 1993 Oct 9;342(8876):909–913. doi: 10.1016/0140-6736(93)91951-h. [DOI] [PubMed] [Google Scholar]