

Short abstract
This article assesses the types of resources, ranging from face-to-face interactions with mental health professionals to texting a crisis line, that adults in California prefer to utilize for suicidal thoughts or feelings.
Abstract
This article assesses the types of resources, ranging from face-to-face interactions with mental health professionals to texting a crisis line, that adults in California prefer to utilize for suicidal thoughts or feelings.
Resources available to help people experiencing suicidal thoughts range from face-to-face interactions (e.g., counselors, clergy, family, or friends) to remote communication (e.g., crisis hotlines and web-based chat) and informational or educational materials (e.g., informational websites or books). Having such a wide variety of options allows people to seek help in the way that is most convenient and comfortable for them, but it is important in the development of resources to consider which options people prefer to utilize and why. While some literature has compared the utilization or efficacy of various help-seeking resources, very little has focused on comparing attitudes or preferences toward available options.*
As part of its evaluation of California's Statewide Prevention and Early Intervention activities funded under Proposition 63, RAND launched a statewide telephone (landline or cell phone) survey of 2,568 adults (ages 18 and older) in California. For the suicide prevention initiative, the survey was designed to estimate the proportion of Californians exposed to social media campaigns funded under Proposition 63, as well as to better understand Californians' preferences for suicide crisis services and confidence in their ability to intervene with persons at risk of suicide. We initially surveyed a random sample of 2,001 adults in the spring of 2013 and then surveyed additional African American and Asian American adults in the summer of 2013 to enhance the diversity of the sample so that racial/ethnic differences could be tested. In total, the sample included 1,014 White, 631 Latino, 401 Asian American, and 360 African American individuals, as well as 108 individuals who identified as another race or multiracial. Fifty-four respondents declined to report their race. Participants were allowed to choose the language of survey administration, including English, Spanish, Cantonese, Mandarin, Vietnamese, Hmong, and Khmer. A total of 305 Latino individuals completed the survey in Spanish; 254 Asian Americans completed it in an Asian language. We applied a weighting procedure to the data so the results of the survey approximate those of the adult population of California. However, because our additional sampling of Asian Americans emphasized Chinese and Southeast Asian subgroups, the views of Korean, Filipino, Japanese, or other Asian groups residing in California may not be fully represented.
In one question, survey respondents were asked, “If you were seeking help for suicidal thoughts and knew where to find resources to help, how likely would you be to use each of the following resources …” and were presented with a list of six options that they could rate from 1 (very likely) to 4 (very unlikely). Preference for a given resource was defined as answering “1” or “2.”
As shown in Figure 1, adult respondents expressed a preference for face-to-face resources, either from a counselor or other mental health professional or from family and friends. The next most commonly endorsed resource was visiting a website for information or calling a crisis line or hotline. Least preferred were web-based crisis chat services or texting a crisis chat line. Differences by age and gender will be the subject of a forthcoming fact sheet, though we note here that the rank order of preferences did not differ by either characteristic.
Figure 1.
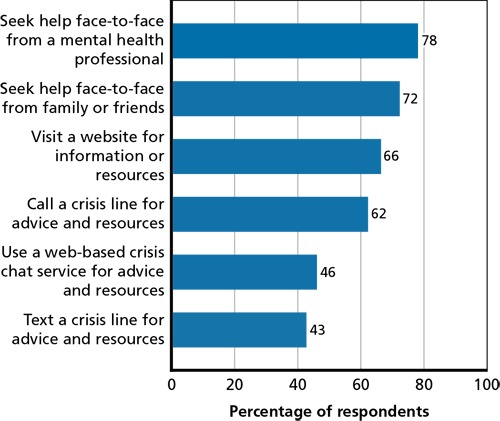
Preferences for Help for Suicidal Thoughts
These findings suggest the importance of enhancing California's face-to-face capacities to prevent suicide by ensuring that there is sufficient capacity of mental health professionals who can provide face-to-face care, and that those seeking such care can access it. These resources are also the most expensive and require the most effort to access for the individual. Therefore, coordination among resources is important. It also means that equipping family members and friends with knowledge about the warning signs for suicide and how to intervene, which are additional activities funded under Proposition 63, may be valuable. However, care must be taken when interpreting these results. Specifically, young people, who make up 5 percent of all suicides in the state, were not captured by the RAND survey, and may prefer using newer technologies like web-based chat or text services when reaching out for help.
This research was conducted in RAND Health, a division of the RAND Corporation.
Notes
One exception is a study showing that adolescents reported more use of face-to-face interactions with mental health professionals, school counselors, the Internet, clergy, and health professionals over hotlines (Gould et al., 2006); another study asked respondents what they would do first if they knew someone was suicidal and most reported “call a suicide hotline,” followed by consult a psychiatrist, talk to their family, call 911, and go to the ER (Larkin et al., 2011).
References
- Gould, M. S., Greenberg T., Munfakh J. L. H., Kleinman M., and Lubell K., “Teenagers' Attitudes About Seeking Help from Telephone Crisis Services (Hotlines),” Suicide and Life-Threatening Behavior, Vol. 36, No. 6, 2006, pp. 601–613. [DOI] [PubMed] [Google Scholar]
- Larkin, G. L., Rivera H., Xu H., Rincon E., and Beautrais A. L., “Community Responses to a Suicidal Crisis: Implications for Suicide Prevention,” Suicide and Life-Threatening Behavior, Vol. 41, No. 1, 2011, pp. 79–86. [DOI] [PubMed] [Google Scholar]