

High quality integrated post-cardiac arrest care can significantly influence the outcome of patients with cardiac arrest, especially neurological recovery, and numerous studies have been conducted on this topic. In the 2015 Korean cardiopulmonary resuscitation (CPR) guidelines, post-cardiac arrest care was emphasized with effective advanced life support as one of the essential chains for survival. Based on an in-depth scientific evidence review using a standardized methodological approach proposed by the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) working group, the guidelines either partially updated the recommendations or added new recommendations for each specific topic.
POST-CARDIAC ARREST CARE STRATEGIES (Fig. 1 and Table 1)
Fig. 1.
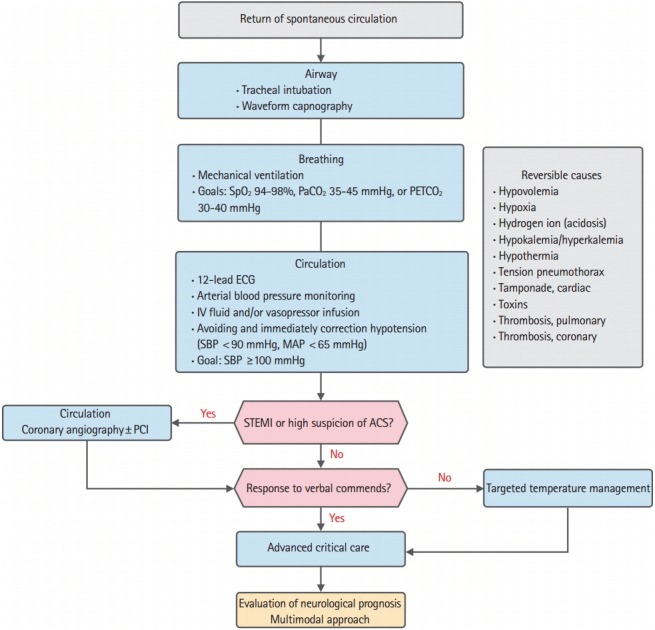
Post-cardiac arrest care algorithm. SpO2, oxygen saturation; PaCO2, arterial oxygen tension; PETCO2, partial pressure of end-tidal carbon dioxide; ECG, electrocardiography; IV, intravenous; SBP, systolic blood pressure; MAP, mean arterial pressure; PCI, percutaneous coronary intervention; STEMI, STelevation myocardial infarction; ACS, acute coronary syndrome.
Table 1.
The strategies in adult immediate post-cardiac arrest care
| Strategy | Doses/details |
|---|---|
| Airway | Consider tracheal intubation and waveform capnography |
| Breathing-oxygenation | Avoid hypoxemia |
| Goal: titrate FiO2 to achieve SpO2 94% to 98% | |
| Breathing-ventilation | Avoid excessive ventilation |
| Goal: titrate to target PaCO2 35 to 45 mmHg or PETCO2 30 to 40 mmHg | |
| Circulation-hemodynamics | Avoiding and immediately correcting hypotension (systolic blood pressure <90 mmHg, mean arterial pressure <65 mmHg) |
| Goal: systolic blood pressure ≥100 mmHg | |
| Circulation-vasoactive drugs | Norepinephrine: 0.1 to 0.5 mcg/kg/min |
| Dopamine: 5 to 10 mcg/kg/min | |
| Epinephrine: 0.1 to 0.5 mcg/kg/min | |
| Correct the reversible causes | Hypovolemia, hypoxia, hydrogen ion (acidosis), hypokalemia/hyperkalemia, hypothermia, tension pneumothorax, cardiac tamponade, toxins, pulmonary thrombosis, coronary thrombosis |
FiO2, fraction of inspired oxygen; SpO2, oxygen saturation; PaCO2, arterial oxygen tension; PETCO2, Partial pressure of end-tidal carbon dioxide.
1. Airway and breathing
When a patient is unconscious after the return of spontaneous circulation (ROSC), the airway should be secured by tracheal intubation, and this should be confirmed by measuring the end-tidal carbon dioxide (ETCO2) and oxygen saturation (SpO2) levels using waveform capnography and pulse oximetry; additionally, mechanical ventilation should be performed while continuously monitoring the ETCO2 and SpO2. To avoid hypoxia, it is reasonable to use the highest available oxygen concentration until appropriate monitoring is available to evaluate the arterial oxygen tension (PaCO2) or arterial oxygen saturation (SaO2) levels. When resources are available to titrate the fraction of inspired oxygen (FiO2) and monitor the saturation, it is reasonable to decrease the FiO2, provided that the SaO2 level can be maintained at the target range.
A study based on a registry reported that hyperoxia within 24 hours after ROSC was associated with a poor outcome compared to hypoxemia or normoxemia within 24 hours [1]. In another study, hyperoxia was shown to have a dose-dependent relationship with poor outcomes, rather than with a certain threshold level [2]. In addition, hyperoxia was associated with poor prognosis in a study of patients with cardiac arrest who had received mild therapeutic hypothermia [3]. In contrast, a study of approximately 12,000 patients with cardiac arrest reported that there was no association between hyperoxia and mortality after the inspired oxygen level and disease severity were adjusted [4]. A meta-analysis of 14 observational studies showed significant heterogeneity across studies [5]. Therefore, it is suggested to maintain the SaO2 at a level of 94% to 98% to avoid hypoxemia and the potential risk of hyperoxia.
Hypocapnia causes cerebral vasoconstriction, and it reduces cerebral blood flow [6]. Observational studies using a registry of patients with cardiac arrest have reported an association between hypocapnia and poor neurologic outcome [7,8]. Two observational studies reported that mild hypercapnia was associated with more favorable neurologic outcomes in patients with cardiac arrest in intensive care units [7,9]. However, several other studies did not show a consistent association between hypercapnia and outcome [7-10]. Therefore, it is suggested to maintain the CO2 level within a normal physiological range (PaCO2 35 to 45 mmHg or ETCO2 30 to 40 mmHg).
2. Circulation
1) Hemodynamic stabilization
Post-cardiac arrest patients are often hemodynamically unstable due to the underlying etiology of arrest, myocardial dysfunction, and systemic ischemia/reperfusion response [11]. Therefore, immediately after ROSC, an arterial catheter should be promptly inserted, and the arterial blood pressure should be monitored continuously. If an arterial catheter cannot be inserted, the blood pressure should be frequently measured noninvasively until the patient becomes hemodynamically stable. Dobutamine can be helpful for post-cardiac arrest myocardial dysfunction [12]. In addition, vasodilation occurs due to the systemic ischemia/reperfusion response; thus, dopamine or norepinephrine may be needed, and intravenous fluids can be an effective treatment depending on the situation [11]. If hemodynamic instability persists even with the infusion of intravenous fluids or vasoactive drugs, a mechanical circulatory assistance device should be considered [13].
Although there are observational studies of patients with cardiac arrest that have investigated the relationship between blood pressure and outcome, a controlled study has not been conducted on a target goal of blood pressure. An observational study examined whether treatment with a specific hemodynamic goal (e.g., a mean arterial pressure [MAP] >65 mmHg) would improve neurologic and functional outcome compared to treatment without a specific hemodynamic goal. The study reported that the mortality rate was higher and the functional recovery was lower in the patient group whose systolic blood pressure (SBP) was <90 mmHg after CPR compared to other patient groups whose SBP was ≥90 mmHg [14]. Two retrospective studies reported that the survival rate decreased in patients who maintained an SBP <90 mmHg and <100 mmHg [15,16]. As several before-and-after studies have implemented a bundle of care, which included a blood pressure goal, the effect of blood pressure cannot be evaluated alone. Moreover, different studies have shown different results regarding a specific level of blood pressure, and the level of evidence from existing studies is insufficient to determine a target blood pressure goal.
Seven studies have investigated the effect of a bundle of care on neurologic outcome, and they reported different results. Some studies have found no association between a specific target blood pressure and neurologic outcome. In one of the studies, a MAP >80 mmHg was a goal, and in another study, an intervention was performed when a goal of MAP was below 75 mmHg, and both of which reported that using a bundle of care, including a hemodynamic goal, was not associated with the neurologic outcome [17,18]. In contrast, other studies have found that a bundle of care that included a blood pressure goal improved the neurologic outcome. Two prospective observational studies have reported that maintaining a MAP >65 mmHg improved the neurologic outcome, and an additional study demonstrated that the neurologic outcome was better in the patient group who maintained a MAP >100 mmHg at 2 hours after ROSC, suggesting an association between MAP and the neurological outcome [19-21]. Yet, another study reported that in patients with a good neurologic outcome, maintaining the time-weighted MAP over 70 mmHg was associated with the neurologic outcome [22]. Two before-and-after observational studies have investigated the effect of using a bundle of care on the survival rate. Both of these studies used a bundle with a MAP >80 mmHg and >65 mmHg as a goal, but there was no significant difference in the survival rate [17,20].
Thus, the evidence is insufficient to determine a specific hemodynamic goal for post-cardiac arrest care. It is suggested that hypotension (SBP <90 mmHg or MAP <65 mmHg) should be immediately corrected, and a hemodynamic goal should be determined for individual patients, while maintaining an SBP >100 mmHg.
2) Evaluation and treatment of reversible causes
After ROSC and during CPR, the resuscitation team should make efforts to evaluate the reversible causes of cardiac arrest (i.e., the five H’s and five T’s: hypovolemia, hypoxia, hydrogen ions [acidosis], hyper/hypokalemia, hypothermia, thromboembolism, thrombosis, tension pneumothorax, cardiac tamponade, and tablets) and then treat the patient.
(1) Intervention of acute coronary syndromes
Acute coronary syndromes are a common cause of adult out-of-hospital cardiac arrest (OHCA) with no obvious extracardiac cause of arrest [23,24]. Thus, a 12-lead electrocardiography (ECG) and a cardiac marker test should be obtained as soon as possible after ROSC to confirm the presence or absence of acute coronary syndromes [25,26]. Coronary angiography should be performed emergently for patients with OHCA with suspected cardiac etiology and ST elevation on ECG, regardless of whether the patient is conscious [27-29]. If acute coronary syndromes are highly suspected in patients with OHCA with suspected cardiac etiology but their ECG does not show ST elevation after ROSC, early coronary angiography should be considered, regardless of the consciousness status [30,31].
(2) Treatment of pulmonary embolism
When cardiac arrest due to pulmonary embolism is strongly suspected, chest computed tomography (CT) should be performed, if possible. If cardiac arrest due to pulmonary embolism is confirmed, thrombolytics can be administered, or surgical or percutaneous embolectomy can be performed [32-34].
TREATMENTS FOR OPTIMIZING NEUROLOGICAL RECOVERY
1. Temperature control
1) Prevention and treatment of hyperpyrexia
Observational studies have reported an association between poor outcome and fever after ROSC in patients without targeted temperature management (TTM) [35,36]. Hyperpyrexia occurs in many patients after TTM. However, the optimal approach to subsequent TTM remains unknown. Several studies have reported conflicting conclusions regarding the association with outcome [36-38]. Although the effect of hyperpyrexia on the outcome of post-cardiac arrest patients is not proven, a poor outcome was associated with hyperpyrexia in comatose patients in whom cerebral damage was due to other causes such as cerebral hemorrhage or infarct, and it is relatively easy to treat or prevent hyperthermia [39,40]. Therefore, it is suggested to continuously prevent or treat fever in adult comatose patients after ROSC from cardiac arrest, regardless of whether the patient received TTM.
2) TTM
(1) Indications and target temperature
One randomized controlled trial (RCT) and a pseudo-randomized trial demonstrated that TTM of 32°C to 34°C improved the neurological outcome at hospital discharge and at 6 months in adult patients with OHCA with a shockable cardiac rhythm [41,42]. Therefore, OHCA with a shockable rhythm is a main indication for TTM. Regarding patients with OHCA with a non-shockable rhythm, no RCT was available. In a cohort study with a very low level of evidence, there was an association between mild induced hypothermia and 6-month survival in patients with OHCA with a nonshockable rhythm. However, a meta-analysis of two other cohort studies did not determine an association between mild induced hypothermia (32°C to 34°C) and an improvement in neurological results [43-46]. For patients with in-hospital cardiac arrest, no RCT has been published. A retrospective cohort study of 1,836 patients found no association between mild induced hypothermia and survival or a functionally favorable status at hospital discharge [47]. However, in this study, the implementation rate of TTM was very low, and the overall outcome of patients treated without TTM was poor; therefore, the aggressive implementation of TTM became necessary. Additionally, ultra-mild hypothermia (36°C) has been suggested as another target temperature since a large, well-conducted RCT compared the target temperature levels of 33°C and 36°C, as it found that the neurological outcome and survival at 6 months after ROSC were not improved when the temperature was controlled at 36°C versus 33°C [48].
Based on the scientific evidence, regardless of the initial rhythm for TTM, it is recommended to select and maintain a constant temperature between 32°C and 36°C in adult patients with cardiac arrest who do not show a meaningful response to verbal commands after ROSC. When making this recommendation, the writing group considered the characteristics of the cardiac arrest population in Korea and that pulseless electrical activity or asystole (i.e., a non-shockable cardiac rhythm) is relatively more frequently observed as the initial arrest rhythm. However, it is unknown whether TTM with mild induced hypothermia (32°C to 34°C) or ultra-mild hypothermia (36°C) is helpful to specific subgroups with cardiac arrest, thus additional studies are needed to shed light on this issue.
(2) Initiation and duration of TTM
Neuronal injury following transient global brain ischemia/reperfusion progresses for several days in a complex biochemical cascade. Mild induced hypothermia influences various stages during the process [49,50]. In particular, oxidative stress, increased excitatory amino acids, and energy depletion occur immediately after ROSC and during cardiac arrest. Theoretically, it would be helpful if mild hypothermia is induced in patients with cardiac arrest as quickly as possible [51,52]. For this reason, several studies have compared the prehospital induction of hypothermia and hospital induction of hypothermia. In all seven RCTs with a medium level of evidence, there was no significant difference between the groups in terms of a poor neurologic outcome or mortality [53-59]. A meta-analysis of seven studies also did not show differences in the mortality rate or poor neurologic outcome between the groups at hospital discharge [46]. Accordingly, based on current scientific evidence, it cannot be concluded that the prehospital induction of TTM is better than induction at the hospital; hence, more conclusive follow-up studies are needed.
A high quality interventional study is not yet available with which to determine an optimal duration of TTM after cardiac arrest. Therefore, based on the duration used in two of the largest aforementioned RCTs, it is reasonable to maintain TTM for at least 24 hours after achieving the target temperature [41,48].
(3) Methods of inducing and/or maintaining TTM
Diverse cooling methods are used to induce and maintain a target temperature, but there is no one best method. External surface cooling methods used widely in the past (e.g., a cooling blanket, ice packs, and a wet towel) are easy and convenient to use. However, they take longer to lower the patient’s core temperature, and they are difficult to maintain at a constant level, which adds to the medical staff’s high workload. Recently, body temperature control has become easier, as cooling equipment that use endovascular catheters and external cooling equipment that regulates temperature with an auto-feedback system have become available, but they are expensive. Hence, medical staff that plan to perform TTM should consider a variety of factors (e.g., the place to initiate the treatment, staff’s ability and experience, speed in induction, stability during maintenance and rewarming, mobility of the equipment, adverse events associated with specific equipment or techniques, convenience of using the equipment, cost, etc.), and the most optimal cooling technique should be chosen for individual patients [60].
Cold crystalloid intravenous fluid infusion is relatively easy to induce hypothermia, and it has been widely used in prehospital settings or during resuscitation for convenience. However, according to a meta-analysis of four RCTs, when TTM was initiated in the prehospital setting using cold crystalloid intravenous fluid infusion, the risk for re-arrest increased [46]. In addition, pulmonary edema was increased according to one large-scale RCT [58]. Therefore, it is not recommended to perform routine prehospital cooling of a patient after ROSC with the rapid infusion of cold intravenous fluid.
When TTM is performed, the patient’s core temperature should be continuously monitored in the esophagus, bladder, or pulmonary artery. The pulmonary artery is the most accurate, but it has a limitation because it requires an invasive procedure. The axillary temperature or oral temperature is not appropriate for measuring changes in the core temperature, and tympanic temperature sensors are difficult to use for a long time and they are often inaccurate. The rectal temperature is commonly used, but there can be temperature gaps when hypothermia is induced rapidly; thus, careful monitoring is needed [61].
Moreover, there is not enough evidence for an optimal speed of rewarming. Accordingly, it is suggested to rewarm at a speed of 0.25°C to 0.5°C per hour, which has been used often in previous studies [41,42,48], and maintain normothermia (36.5°C to 37.5°C) up to 72 hours after ROSC in comatose patients even after normothermia is achieved.
2. Glucose control
Hyperglycemia is associated with mortality and a poor neurologic outcome in patients who have been resuscitated from cardiac arrest, and it should be appropriately controlled. There is little evidence about a target blood glucose level to improve the outcome of patients with cardiac arrest. An RCT found no difference in the 30-day mortality rate between the groups with a target blood glucose level of 72 to 108 mg/dL and 108 to 144 mg/dL [62]. In a before-and-after study that used a bundle of care with a target blood glucose level of 90 to 144 mg/dL, the neurological outcome improved after implementing the bundle, but the effect could not be attributed only to the controlled blood glucose level [18]. Applying the findings of these studies to cardiac arrest patients may not be appropriate, because they examined the effect of controlling blood glucose level in critically ill patients [63,64]. Although is still controversy on how to control the blood glucose level in critically ill patients, the strict control of blood glucose was associated with an increased occurrence of hypoglycemia [62]. Therefore, the target range of 144 to 180 mmHg is suggested to prevent hypoglycemia, although evidence so far is insufficient. Hyperglycemia >180 mmHg should be treated with an insulin infusion per the hospital’s protocol, and care should be taken to prevent hypoglycemia (<80 mg/dL). If hypoglycemia occurs, it should be immediately corrected by administering a glucose solution. The blood glucose level, especially, fluctuates during the induction or rewarming period; therefore, it is desirable to frequently test the patient’s blood glucose level.
3. Control of seizures
No study has directly compared patients treated for seizure with those not treated for seizure. Furthermore, there is no evidence thus far that a specific anticonvulsant or combination therapy with anticonvulsant drugs is helpful in comatose patients after cardiac arrest. Therefore, if seizure occurs or is suspected, an electroencephalogram (EEG) needs to be performed immediately to determine the presence of epileptiform activity. Non-convulsive seizures can occur while TTM is performed with a neuromuscular blocking drug; thus, if possible, an EEG should be continuously monitored, and the arterial blood gas level or change in vital signs (e.g., unexplained tachycardia) should be carefully observed [65]. To control seizures, any commonly used anticonvulsant needs to be promptly injected. In a case of generalized seizure, benzodiazepine, phenytoin, sodium valproate, propofol, levetiracetam, phenobarbital, and similar drugs can be used alone or in combination with each other. In cases of myoclonus, clonazepam, sodium valproate, levetiracetam, propofol, etc. can be used alone or in combination with each other [66]. Post-anoxic myoclonic status epilepticus may not respond well to anticonvulsants [67,68]. Available evidence does not support the prophylactic administration of anticonvulsants. Therefore, the routine use of prophylactic anticonvulsants in post-cardiac arrest patients is not recommended.
4. Sedation
In most post-cardiac arrest patients, mechanical ventilation should be maintained during post-cardiac arrest care, and sedatives or analgesics may have to be intermittently or continuously administered. If a patient is sedated while TTM is performed, the time required to reach to the target temperature can be reduced because shivering is prevented or reduced. Using a sedation protocol can be helpful in these cases.
Sedation after ROSC is a commonly used treatment method, but the level of evidence is not sufficient to make a recommendation about the duration to administer a sedative or neuromuscular blocker in post-cardiac arrest patients. A meta-analysis of 44 studies reported on sedative drugs that were used while TTM was performed among 68 intensive care units in various countries found that a large variety of drugs were being used [69]. From the analysis, it is impossible to know which drugs may be associated with outcome, but mainly the combination therapy of an opioid and sedative was used. It is recommended to maintain a sedative over a short duration of action as much as possible, but no study has analyzed the effect of using sedatives in patients after cardiac arrest or has suggested treatment strategies. One study has suggested that the continuous administration of neuromuscular blockers may be associated with a low mortality rate [70]. However, neuromuscular blockers interfere with clinical examinations, and they obscure the occurrence of seizure. Therefore, if a neuromuscular blocker is continuously administered, the EEG should be continuously monitored.
EVALUATION OF NEUROLOGICAL PROGNOSTICATION
In the 2015 guidelines, studies of patients who had and had not received TTM were evaluated. These studies evaluated the diagnostic accuracy of clinical examination, electrophysiological studies, biomarkers, and imaging tests for predicting poor neurological outcome, and they recommended diagnostic tests with a false positive rate (FPR) close to 0% and a narrow 95% confidence interval (0% to 10%) as predictors.
It is recommended to predict the neurologic outcome at least 72 hours after ROSC, particularly because in most cases, a sedative and a neuromuscular blocker are administered to comatose patients after cardiac arrest while TTM is performed. An additional recommendation is to use a multimodal approach rather than relying on a single test or finding.
1. Clinical examination
For a clinical examination to predict a poor neurologic outcome within 72 hours after ROSC in comatose patients after cardiac arrest, the bilateral absence of pupillary light reflex, or the combination of the absence of pupillary light reflex and absence of corneal reflex is required in both patients with TTM (FPR 0 [0% to 3%]) and without TTM (FPR 0 [0% to 8%]) [71-79].
The lack of motor movement (M1) or extensor posturing (M2) to pain has a high FPR level (27% [12% to 48%]) for predicting a poor neurologic outcome in comatose patients who did not receive TTM after cardiac arrest, and a similar finding was observed in patients who received TTM [71,73-82]. Therefore, it is suggested to not use motor movement to pain alone to predict poor neurologic outcomes. Although they have a high sensitivity level (74% [68% to 79%]), they can be used to confirm a patient’s poor neurologic outcome or predict a poor neurologic outcome in combination with other predictors.
Myoclonus in comatose patients within 72 hours after cardiac arrest is associated with a high FPR (10% to 15%) for predicting poor neurologic outcomes; thus, it is suggested to not use it alone. In contrast, status myoclonus, which occurs within 72 hours after cardiac arrest, predicts poor neurologic outcome with a high accuracy in cases with TTM (FPR 0% [0% to 4%]) and without TTM (FPR 0% [0% to 5%]) [65,67,71,72,83,84]. Therefore, it is useful when used in combination with other predictors. If there is residual sedation and paralysis still remains, the clinical examination can be delayed to minimize the possibility of false positives. Seventy-two hours after ROSC is suggested as the earliest time to predict a poor neurologic outcome.
2. Electrophysiological studies
To predict poor neurologic outcome in comatose patients after cardiac arrest, regardless of using TTM, the use of the bilateral absence of N20 waveform recorded from somatosensory evoked potentials (SSEPs) (FPR 1% [0% to 3%]) is recommended 24 to 72 hours after cardiac arrest or after rewarming [72-75,80-82,85-89]. An SSEP recording requires appropriate skills and experience, and efforts should be considered to avoid muscle artifacts or electrical interference from the environment of the emergency room or intensive care unit.
A lack of EEG background reactivity can accurately predict poor neurologic outcome in comatose patients after cardiac arrest during TTM (FPR 2% [1% to 7%]) and within 72 hours after ROSC (FPR 0% [0% to 3%]) [80,82,90,91]. However, using the pattern of background reactivity on EEG has limitations, because they are operator dependent, unquantifiable, and lack standardization. Status epilepticus (i.e., a persistent seizure over 72 hours) is commonly associated with a poor neurologic outcome (FPR 0% to 6%), if it occurs during hypothermia or rewarming in patients who received TTM [65,92]. EEG burst-suppression can show a recovery of consciousness, if it occurs for 24 to 48 hours after ROSC in patients who did not receive TTM, or during hypothermia in patients who received TTM [82,93], but persistent burst-suppression that occurs 72 hours after ROSC is always associated with a poor neurologic outcome [72,94]. Therefore, it is suggested to use EEG predictors (e.g., the lack of EEG response to external stimulation, EEG burst-suppression after rewarming, and status epilepticus) after 72 hours after ROSC in combination with other predictors to predict a poor neurologic outcome in comatose patients after cardiac arrest, regardless of using TTM.
To predict poor neurologic outcomes of patients who received TTM, burst-suppression observed in the continuous amplitude-integrated EEG recordings, status epilepticus, and lack of normal trace over 36 hours can be used in combination with other predictors [95].
3. Biomarkers
A high level or increasing levels of neuron-specific enolase (NSE) measured at 48-72 hours after ROSC can be used in combination with other predictors to predict poor neurologic outcomes of comatose patients who received TTM after cardiac arrest [96-98]. A careful approach is necessary when testing NSE to avoid a false positive result that can occur due to hemolysis, and it is recommended to sample various points in time as much as possible. Since different studies have reported different NSE thresholds to predict a poor neurologic outcome with 0% FPR, it is recommended to not use the serum levels of NSE and S100B alone.
4. Imaging tests
Global cerebral edema and the marked reduction of the gray matter/white matter ratio (GWR) on CT obtained within 2 hours after ROSC can predict poor neurologic outcomes with 0% FPR in comatose patients who received TTM after cardiac arrest. However, different studies have reported different GWR thresholds with 0% FPR, depending on the measurement technique and the studied brain area [77,98,99]. An extensive restriction of diffusion detected on brain magnetic resonance imaging (MRI) obtained 2 to 6 days after ROSC and quantitatively measured with an apparent diffusion coefficient can predict poor neurologic outcomes with 0% FPR in comatose patients who received TTM after cardiac arrest [100,101]. However, the apparent diffusion coefficient threshold value with 0% FPR is different among studies, depending on the studied brain area and the measurement technique.
Therefore, it is recommended to use the marked reduction of the GWR on CT obtained within 2 hours after ROSC or the extensive restriction of diffusion on MRI obtained 2 to 6 days after ROSC in combination with other predictors to predict poor neurologic outcomes of comatose patients who received TTM after cardiac arrest.
5. Neurological prognostication algorithm (Fig. 2)
Fig. 2.

Neurological prognostication algorithm. N/Ex, neurological examination; CT, computed tomography; NSE, neuron specific enolase; SSEP, somatosensory evoked potential; DW-MRI, diffusion-weighted magnetic resonance imaging; EEG, electroencephalography; ROSC, return of spontaneous circulation; GWR, gray matter/white matter ratio; CT, computed tomography; aEEG, amplitude-integrated electroencephalography
In most post-cardiac arrest comatose patients, cerebral function recovery occurs within 72 hours after ROSC [84,102]. However, there is a possibility of decreased accuracy of clinical examination due to the influence of sedatives and neuromuscular blockers administered during the application of TTM.
First, it is important to exclude confounders (e.g., residual sedation and paralysis) that can impact clinical examination after 72 hours after ROSC and the completion of TTM. Second, 72 hours after ROSC, use the flowchart to differentiate comatose patients who show the absence of motor movement or extensor posturing to pain. Third, confirm the bilateral absence of pupillary light reflex and bilateral absence of N20 waveform in SSEPs, which have a low FPR and high accuracy. If all three aforementioned conditions are met, a poor neurological outcome can be predicted with accuracy (FPR <5%, narrow 95% confidence interval).
Otherwise, observe patients for at least 24 hours and assess the following predictors of poor outcome. 1) A marked reduction of the GWR on brain CT obtained within 2 hours after ROSC; 2) the lack of normal trace in the amplitude-integrated EEG recording observed for >36 hours; 3) status myoclonus occurring within 72 hours after ROSC; 4) a high serum level of NSE measured 48 to 72 hours after the ROSC; 5) unreactive burst-suppression or status epilepticus on EEG 72 hours after ROSC; and 6) extensive restriction of diffusion on MRI obtained 2 to 6 days after ROSC. A poor neurologic outcome can be predicted if two of six factors are observed. Otherwise, the outcome can be determined based on various findings in combination or after additional observation.
Acknowledgments
We appreciate to the following evidence reviewers who contribute to develop the 2015 Korean Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations for the population, intervention, comparator, and outcome questions in post-cardiac arrest care. The collaborators’ are as follows: Kyung Su Kim, Seoul National University Hospital, Seoul, Korea; Won Young Kim, Ulsan University Asan Medical Center, Seoul, Korea; Jin Joo Kim, Gachon University Gil Medical Center, Incheon, Korea; Min Seob Sim, Sungkyunkwan University Samsung Medical Center, Seoul, Korea; Yeon Ho You, Chungnam National University Hospital, Kwangju, Korea; Seung Joon Lee, Myongji Hospital, Seoul, Korea; Young Hwan Lee, Hallym University Sacred Heart Hospital, Seoul, Korea; Joo Young Lee, The Catholic University of Korea Seoul St. Mary’s Hospital, Seoul, Korea; Kyung Woon Jeung, Chonnam National University Hospital, Kwangju, Korea; Moon Gu Han, Seoul National University Bundang Hospital, Seongnam, Korea; Chul Han, Ewha University Hospital, Seoul, Korea.
REFERENCES
- 1.Kilgannon JH, Jones AE, Shapiro NI, et al. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA. 2010;303:2165–71. doi: 10.1001/jama.2010.707. [DOI] [PubMed] [Google Scholar]
- 2.Kilgannon JH, Jones AE, Parrillo JE, et al. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation. 2011;123:2717–22. doi: 10.1161/CIRCULATIONAHA.110.001016. [DOI] [PubMed] [Google Scholar]
- 3.Janz DR, Hollenbeck RD, Pollock JS, McPherson JA, Rice TW. Hyperoxia is associated with increased mortality in patients treated with mild therapeutic hypothermia after sudden cardiac arrest. Crit Care Med. 2012;40:3135–9. doi: 10.1097/CCM.0b013e3182656976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bellomo R, Bailey M, Eastwood GM, et al. Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest. Crit Care. 2011;15:R90. doi: 10.1186/cc10090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wang CH, Chang WT, Huang CH, et al. The effect of hyperoxia on survival following adult cardiac arrest: a systematic review and meta-analysis of observational studies. Resuscitation. 2014;85:1142–8. doi: 10.1016/j.resuscitation.2014.05.021. [DOI] [PubMed] [Google Scholar]
- 6.Menon DK, Coles JP, Gupta AK, et al. Diffusion limited oxygen delivery following head injury. Crit Care Med. 2004;32:1384–90. doi: 10.1097/01.ccm.0000127777.16609.08. [DOI] [PubMed] [Google Scholar]
- 7.Schneider AG, Eastwood GM, Bellomo R, et al. Arterial carbon dioxide tension and outcome in patients admitted to the intensive care unit after cardiac arrest. Resuscitation. 2013;84:927–34. doi: 10.1016/j.resuscitation.2013.02.014. [DOI] [PubMed] [Google Scholar]
- 8.Roberts BW, Kilgannon JH, Chansky ME, Mittal N, Wooden J, Trzeciak S. Association between postresuscitation partial pressure of arterial carbon dioxide and neurological outcome in patients with post-cardiac arrest syndrome. Circulation. 2013;127:2107–13. doi: 10.1161/CIRCULATIONAHA.112.000168. [DOI] [PubMed] [Google Scholar]
- 9.Vaahersalo J, Bendel S, Reinikainen M, et al. Arterial blood gas tensions after resuscitation from out-of-hospital cardiac arrest: associations with long-term neurologic outcome. Crit Care Med. 2014;42:1463–70. doi: 10.1097/CCM.0000000000000228. [DOI] [PubMed] [Google Scholar]
- 10.Lee BK, Jeung KW, Lee HY, et al. Association between mean arterial blood gas tension and outcome in cardiac arrest patients treated with therapeutic hypothermia. Am J Emerg Med. 2014;32:55–60. doi: 10.1016/j.ajem.2013.09.044. [DOI] [PubMed] [Google Scholar]
- 11.Laurent I, Monchi M, Chiche JD, et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002;40:2110–6. doi: 10.1016/s0735-1097(02)02594-9. [DOI] [PubMed] [Google Scholar]
- 12.Kern KB, Hilwig RW, Berg RA, et al. Postresuscitation left ventricular systolic and diastolic dysfunction. Treatment with dobutamine. Circulation. 1997;95:2610–3. doi: 10.1161/01.cir.95.12.2610. [DOI] [PubMed] [Google Scholar]
- 13.Manzo-Silberman S, Fichet J, Mathonnet A, et al. Percutaneous left ventricular assistance in post cardiac arrest shock: comparison of intra aortic blood pump and IMPELLA Recover LP2.5. Resuscitation. 2013;84:609–15. doi: 10.1016/j.resuscitation.2012.10.001. [DOI] [PubMed] [Google Scholar]
- 14.Trzeciak S, Jones AE, Kilgannon JH, et al. Significance of arterial hypotension after resuscitation from cardiac arrest. Crit Care Med. 2009;37:2895–903. doi: 10.1097/ccm.0b013e3181b01d8c. [DOI] [PubMed] [Google Scholar]
- 15.Bray JE, Bernard S, Cantwell K, Stephenson M, Smith K; VACAR Steering Committee. The association between systolic blood pressure on arrival at hospital and outcome in adults surviving from out-of-hospital cardiac arrests of presumed cardiac aetiology. Resuscitation. 2014;85:509–15. doi: 10.1016/j.resuscitation.2013.12.005. [DOI] [PubMed] [Google Scholar]
- 16.Kilgannon JH, Roberts BW, Reihl LR, et al. Early arterial hypotension is common in the post-cardiac arrest syndrome and associated with increased in-hospital mortality. Resuscitation. 2008;79:410–6. doi: 10.1016/j.resuscitation.2008.07.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gaieski DF, Band RA, Abella BS, et al. Early goal-directed hemodynamic optimization combined with therapeutic hypothermia in comatose survivors of out-of-hospital cardiac arrest. Resuscitation. 2009;80:418–24. doi: 10.1016/j.resuscitation.2008.12.015. [DOI] [PubMed] [Google Scholar]
- 18.Sunde K, Pytte M, Jacobsen D, et al. Implementation of a standardised treatment protocol for post resuscitation care after out-of-hospital cardiac arrest. Resuscitation. 2007;73:29–39. doi: 10.1016/j.resuscitation.2006.08.016. [DOI] [PubMed] [Google Scholar]
- 19.Orioles A, Morrison WE, Rossano JW, et al. An under-recognized benefit of cardiopulmonary resuscitation: organ transplantation. Crit Care Med. 2013;41:2794–9. doi: 10.1097/CCM.0b013e31829a7202. [DOI] [PubMed] [Google Scholar]
- 20.Walters EL, Morawski K, Dorotta I, et al. Implementation of a post-cardiac arrest care bundle including therapeutic hypothermia and hemodynamic optimization in comatose patients with return of spontaneous circulation after out-ofhospital cardiac arrest: a feasibility study. Shock. 2011;35:360–6. doi: 10.1097/SHK.0b013e318204c106. [DOI] [PubMed] [Google Scholar]
- 21.Mullner M, Sterz F, Binder M, et al. Arterial blood pressure after human cardiac arrest and neurological recovery. Stroke. 1996;27:59–62. doi: 10.1161/01.str.27.1.59. [DOI] [PubMed] [Google Scholar]
- 22.Kilgannon JH, Roberts BW, Jones AE, et al. Arterial blood pressure and neurologic outcome after resuscitation from cardiac arrest. Crit Care Med. 2014;42:2083–91. doi: 10.1097/CCM.0000000000000406. [DOI] [PubMed] [Google Scholar]
- 23.Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death: epidemiology, transient risk, and intervention assessment. Ann Intern Med. 1993;119:1187–97. doi: 10.7326/0003-4819-119-12-199312150-00006. [DOI] [PubMed] [Google Scholar]
- 24.Adabag AS, Therneau TM, Gersh BJ, Weston SA, Roger VL. Sudden death after myocardial infarction. JAMA. 2008;300:2022–9. doi: 10.1001/jama.2008.553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Authors/Task Force Members. Priori SG, Blomstrom-Lundqvist C, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC) Europace. 2015;17:1601. doi: 10.1093/europace/euv319. - 87. [DOI] [PubMed] [Google Scholar]
- 26.Jacobs AK. Regional systems of care for patients with ST-elevation myocardial infarction: being at the right place at the right time. Circulation. 2007;116:689–92. doi: 10.1161/CIRCULATIONAHA.107.720946. [DOI] [PubMed] [Google Scholar]
- 27.Strote JA, Maynard C, Olsufka M, et al. Comparison of role of early (less than six hours) to later (more than six hours) or no cardiac catheterization after resuscitation from outof-hospital cardiac arrest. Am J Cardiol. 2012;109:451–4. doi: 10.1016/j.amjcard.2011.09.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nanjayya VB, Nayyar V. Immediate coronary angiogram in comatose survivors of out-of-hospital cardiac arrest: an Australian study. Resuscitation. 2012;83:699–704. doi: 10.1016/j.resuscitation.2011.12.004. [DOI] [PubMed] [Google Scholar]
- 29.Zanuttini D, Armellini I, Nucifora G, et al. Impact of emergency coronary angiography on in-hospital outcome of unconscious survivors after out-of-hospital cardiac arrest. Am J Cardiol. 2012;110:1723–8. doi: 10.1016/j.amjcard.2012.08.006. [DOI] [PubMed] [Google Scholar]
- 30.Hollenbeck RD, McPherson JA, Mooney MR, et al. Early cardiac catheterization is associated with improved survival in comatose survivors of cardiac arrest without STEMI. Resuscitation. 2014;85:88–95. doi: 10.1016/j.resuscitation.2013.07.027. [DOI] [PubMed] [Google Scholar]
- 31.Bro-Jeppesen J, Kjaergaard J, Wanscher M, et al. Emergency coronary angiography in comatose cardiac arrest patients: do real-life experiences support the guidelines? Eur Heart J Acute Cardiovasc Care. 2012;1:291–301. doi: 10.1177/2048872612465588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Scholz KH, Hilmer T, Schuster S, Wojcik J, Kreuzer H, Tebbe U. Thrombolysis in resuscitated patients with pulmonary embolism. Dtsch Med Wochenschr. 1990;115:930–5. doi: 10.1055/s-2008-1065101. [DOI] [PubMed] [Google Scholar]
- 33.Ullmann M, Hemmer W, Hannekum A. The urgent pulmonary embolectomy: mechanical resuscitation in the operating theatre determines the outcome. Thorac Cardiovasc Surg. 1999;47:5–8. doi: 10.1055/s-2007-1013099. [DOI] [PubMed] [Google Scholar]
- 34.Konstantinov IE, Saxena P, Koniuszko MD, Alvarez J, Newman MA. Acute massive pulmonary embolism with cardiopulmonary resuscitation: management and results. Tex Heart Inst J. 2007;34:41–5. [PMC free article] [PubMed] [Google Scholar]
- 35.Zeiner A, Holzer M, Sterz F, et al. Hyperthermia after cardiac arrest is associated with an unfavorable neurologic outcome. Arch Intern Med. 2001;161:2007–12. doi: 10.1001/archinte.161.16.2007. [DOI] [PubMed] [Google Scholar]
- 36.Gebhardt K, Guyette FX, Doshi AA, Callaway CW, Rittenberger JC; Post Cardiac Arrest Service. Prevalence and effect of fever on outcome following resuscitation from cardiac arrest. Resuscitation. 2013;84:1062–7. doi: 10.1016/j.resuscitation.2013.03.038. [DOI] [PubMed] [Google Scholar]
- 37.Leary M, Grossestreuer AV, Iannacone S, et al. Pyrexia and neurologic outcomes after therapeutic hypothermia for cardiac arrest. Resuscitation. 2013;84:1056–61. doi: 10.1016/j.resuscitation.2012.11.003. [DOI] [PubMed] [Google Scholar]
- 38.Bro-Jeppesen J, Hassager C, Wanscher M, et al. Post-hypothermia fever is associated with increased mortality after out-of-hospital cardiac arrest. Resuscitation. 2013;84:1734–40. doi: 10.1016/j.resuscitation.2013.07.023. [DOI] [PubMed] [Google Scholar]
- 39.Badjatia N. Hyperthermia and fever control in brain injury. Crit Care Med. 2009;37(7 Suppl):S250–7. doi: 10.1097/CCM.0b013e3181aa5e8d. [DOI] [PubMed] [Google Scholar]
- 40.Bohman LE, Levine JM. Fever and therapeutic normothermia in severe brain injury: an update. Curr Opin Crit Care. 2014;20:182–8. doi: 10.1097/MCC.0000000000000070. [DOI] [PubMed] [Google Scholar]
- 41.Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–56. doi: 10.1056/NEJMoa012689. [DOI] [PubMed] [Google Scholar]
- 42.Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–63. doi: 10.1056/NEJMoa003289. [DOI] [PubMed] [Google Scholar]
- 43.Testori C, Sterz F, Behringer W, et al. Mild therapeutic hypothermia is associated with favourable outcome in patients after cardiac arrest with non-shockable rhythms. Resuscitation. 2011;82:1162–7. doi: 10.1016/j.resuscitation.2011.05.022. [DOI] [PubMed] [Google Scholar]
- 44.Dumas F, Grimaldi D, Zuber B, et al. Is hypothermia after cardiac arrest effective in both shockable and nonshockable patients?: insights from a large registry. Circulation. 2011;123:877–86. doi: 10.1161/CIRCULATIONAHA.110.987347. [DOI] [PubMed] [Google Scholar]
- 45.Vaahersalo J, Hiltunen P, Tiainen M, et al. Therapeutic hypothermia after out-of-hospital cardiac arrest in Finnish intensive care units: the FINNRESUSCI study. Intensive Care Med. 2013;39:826–37. doi: 10.1007/s00134-013-2868-1. [DOI] [PubMed] [Google Scholar]
- 46.Donnino MW, Andersen LW, Berg KM, et al. Temperature Management After Cardiac Arrest: An Advisory Statement by the Advanced Life Support Task Force of the International Liaison Committee on Resuscitation and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Circulation. 2015;132:2448–56. doi: 10.1161/CIR.0000000000000313. [DOI] [PubMed] [Google Scholar]
- 47.Nichol G, Huszti E, Kim F, et al. Does induction of hypothermia improve outcomes after in-hospital cardiac arrest? Resuscitation. 2013;84:620–5. doi: 10.1016/j.resuscitation.2012.12.009. [DOI] [PubMed] [Google Scholar]
- 48.Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369:2197–206. doi: 10.1056/NEJMoa1310519. [DOI] [PubMed] [Google Scholar]
- 49.Ginsberg MD, Belayev L. Biological and molecular mechanisms of hypothermic neuroprotection. In: Mayer SA, Sessler DI, editors. Therapeutic hypothermia. New York, NY: Marcel Dekker; 2005. pp. 85–140. [Google Scholar]
- 50.Liu L, Yenari MA. Therapeutic hypothermia: neuroprotective mechanisms. Front Biosci. 2007;12:816–25. doi: 10.2741/2104. [DOI] [PubMed] [Google Scholar]
- 51.Angelos MG, Menegazzi JJ, Callaway CW. Bench to bedside: resuscitation from prolonged ventricular fibrillation. Acad Emerg Med. 2001;8:909–24. doi: 10.1111/j.1553-2712.2001.tb01155.x. [DOI] [PubMed] [Google Scholar]
- 52.van Zanten AR, Polderman KH. Early induction of hypothermia: will sooner be better? Crit Care Med. 2005;33:1449–52. doi: 10.1097/01.ccm.0000166710.64724.34. [DOI] [PubMed] [Google Scholar]
- 53.Kim F, Olsufka M, Longstreth WT, Jr, et al. Pilot randomized clinical trial of prehospital induction of mild hypothermia in out-of-hospital cardiac arrest patients with a rapid infusion of 4 degrees C normal saline. Circulation. 2007;115:3064–70. doi: 10.1161/CIRCULATIONAHA.106.655480. [DOI] [PubMed] [Google Scholar]
- 54.Kamarainen A, Virkkunen I, Tenhunen J, Yli-Hankala A, Silfvast T. Prehospital therapeutic hypothermia for comatose survivors of cardiac arrest: a randomized controlled trial. Acta Anaesthesiol Scand. 2009;53:900–7. doi: 10.1111/j.1399-6576.2009.02015.x. [DOI] [PubMed] [Google Scholar]
- 55.Bernard SA, Smith K, Cameron P, et al. Induction of therapeutic hypothermia by paramedics after resuscitation from out-of-hospital ventricular fibrillation cardiac arrest: a randomized controlled trial. Circulation. 2010;122:737–42. doi: 10.1161/CIRCULATIONAHA.109.906859. [DOI] [PubMed] [Google Scholar]
- 56.Castren M, Nordberg P, Svensson L, et al. Intra-arrest transnasal evaporative cooling: a randomized, prehospital, multi-center study (PRINCE: Pre-ROSC IntraNasal Cooling Effectiveness) Circulation. 2010;122:729–36. doi: 10.1161/CIRCULATIONAHA.109.931691. [DOI] [PubMed] [Google Scholar]
- 57.Bernard SA, Smith K, Cameron P, et al. Induction of prehospital therapeutic hypothermia after resuscitation from nonventricular fibrillation cardiac arrest. Crit Care Med. 2012;40:747–53. doi: 10.1097/CCM.0b013e3182377038. [DOI] [PubMed] [Google Scholar]
- 58.Kim F, Nichol G, Maynard C, et al. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. JAMA. 2014;311:45–52. doi: 10.1001/jama.2013.282173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Debaty G, Maignan M, Savary D, et al. Impact of intra-arrest therapeutic hypothermia in outcomes of prehospital cardiac arrest: a randomized controlled trial. Intensive Care Med. 2014;40:1832–42. doi: 10.1007/s00134-014-3519-x. [DOI] [PubMed] [Google Scholar]
- 60.Geocadin RG, Koenig MA, Jia X, Stevens RD, Peberdy MA. Management of brain injury after resuscitation from cardiac arrest. Neurol Clin. 2008;26:487–506. doi: 10.1016/j.ncl.2008.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Shin J, Kim J, Song K, Kwak Y. Core temperature measurement in therapeutic hypothermia according to different phases: comparison of bladder, rectal, and tympanic versus pulmonary artery methods. Resuscitation. 2013;84:810–7. doi: 10.1016/j.resuscitation.2012.12.023. [DOI] [PubMed] [Google Scholar]
- 62.Oksanen T, Skrifvars MB, Varpula T, et al. Strict versus moderate glucose control after resuscitation from ventricular fibrillation. Intensive Care Med. 2007;33:2093–100. doi: 10.1007/s00134-007-0876-8. [DOI] [PubMed] [Google Scholar]
- 63.Marik PE, Preiser JC. Toward understanding tight glycemic control in the ICU: a systematic review and metaanalysis. Chest. 2010;137:544–51. doi: 10.1378/chest.09-1737. [DOI] [PubMed] [Google Scholar]
- 64.Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: a meta-analysis. JAMA. 2008;300:933–44. doi: 10.1001/jama.300.8.933. [DOI] [PubMed] [Google Scholar]
- 65.Rittenberger JC, Popescu A, Brenner RP, Guyette FX, Callaway CW. Frequency and timing of nonconvulsive status epilepticus in comatose post-cardiac arrest subjects treated with hypothermia. Neurocrit Care. 2012;16:114–22. doi: 10.1007/s12028-011-9565-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Caviness JN, Brown P. Myoclonus: current concepts and recent advances. Lancet Neurol. 2004;3:598–607. doi: 10.1016/S1474-4422(04)00880-4. [DOI] [PubMed] [Google Scholar]
- 67.Krumholz A, Stern BJ, Weiss HD. Outcome from coma after cardiopulmonary resuscitation: relation to seizures and myoclonus. Neurology. 1988;38:401–5. doi: 10.1212/wnl.38.3.401. [DOI] [PubMed] [Google Scholar]
- 68.Hui AC, Cheng C, Lam A, Mok V, Joynt GM. Prognosis following Postanoxic Myoclonus Status epilepticus. Eur Neurol. 2005;54:10–3. doi: 10.1159/000086755. [DOI] [PubMed] [Google Scholar]
- 69.Chamorro C, Borrallo JM, Romera MA, Silva JA, Balandin B. Anesthesia and analgesia protocol during therapeutic hypothermia after cardiac arrest: a systematic review. Anesth Analg. 2010;110:1328–35. doi: 10.1213/ANE.0b013e3181d8cacf. [DOI] [PubMed] [Google Scholar]
- 70.Salciccioli JD, Cocchi MN, Rittenberger JC, et al. Continuous neuromuscular blockade is associated with decreased mortality in post-cardiac arrest patients. Resuscitation. 2013;84:1728–33. doi: 10.1016/j.resuscitation.2013.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Samaniego EA, Mlynash M, Caulfield AF, Eyngorn I, Wijman CA. Sedation confounds outcome prediction in cardiac arrest survivors treated with hypothermia. Neurocrit Care. 2011;15:113–9. doi: 10.1007/s12028-010-9412-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Zandbergen EG, Hijdra A, Koelman JH, et al. Prediction of poor outcome within the first 3 days of postanoxic coma. Neurology. 2006;66:62–8. doi: 10.1212/01.wnl.0000191308.22233.88. [DOI] [PubMed] [Google Scholar]
- 73.Bisschops LL, van Alfen N, Bons S, van der Hoeven JG, Hoedemaekers CW. Predictors of poor neurologic outcome in patients after cardiac arrest treated with hypothermia: a retrospective study. Resuscitation. 2011;82:696–701. doi: 10.1016/j.resuscitation.2011.02.020. [DOI] [PubMed] [Google Scholar]
- 74.Bouwes A, Binnekade JM, Zandstra DF, et al. Somatosensory evoked potentials during mild hypothermia after cardiopulmonary resuscitation. Neurology. 2009;73:1457–61. doi: 10.1212/WNL.0b013e3181bf98f4. [DOI] [PubMed] [Google Scholar]
- 75.Bouwes A, Binnekade JM, Kuiper MA, et al. Prognosis of coma after therapeutic hypothermia: a prospective cohort study. Ann Neurol. 2012;71:206–12. doi: 10.1002/ana.22632. [DOI] [PubMed] [Google Scholar]
- 76.Fugate JE, Wijdicks EF, Mandrekar J, et al. Predictors of neurologic outcome in hypothermia after cardiac arrest. Ann Neurol. 2010;68:907–14. doi: 10.1002/ana.22133. [DOI] [PubMed] [Google Scholar]
- 77.Wu O, Batista LM, Lima FO, Vangel MG, Furie KL, Greer DM. Predicting clinical outcome in comatose cardiac arrest patients using early noncontrast computed tomography. Stroke. 2011;42:985–92. doi: 10.1161/STROKEAHA.110.594879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Greer DM, Yang J, Scripko PD, et al. Clinical examination for prognostication in comatose cardiac arrest patients. Resuscitation. 2013;84:1546–51. doi: 10.1016/j.resuscitation.2013.07.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Dragancea I, Horn J, Kuiper M, et al. Neurological prognostication after cardiac arrest and targeted temperature management 33°C versus 36°C: results from a randomised controlled clinical trial. Resuscitation. 2015;93:164–70. doi: 10.1016/j.resuscitation.2015.04.013. [DOI] [PubMed] [Google Scholar]
- 80.Rossetti AO, Oddo M, Logroscino G, Kaplan PW. Prognostication after cardiac arrest and hypothermia: a prospective study. Ann Neurol. 2010;67:301–7. doi: 10.1002/ana.21984. [DOI] [PubMed] [Google Scholar]
- 81.Rossetti AO, Urbano LA, Delodder F, Kaplan PW, Oddo M. Prognostic value of continuous EEG monitoring during therapeutic hypothermia after cardiac arrest. Crit Care. 2010;14:R173. doi: 10.1186/cc9276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Rossetti AO, Carrera E, Oddo M. Early EEG correlates of neuronal injury after brain anoxia. Neurology. 2012;78:796–802. doi: 10.1212/WNL.0b013e318249f6bb. [DOI] [PubMed] [Google Scholar]
- 83.Bouwes A, van Poppelen D, Koelman JH, et al. Acute posthypoxic myoclonus after cardiopulmonary resuscitation. BMC Neurol. 2012;12:63. doi: 10.1186/1471-2377-12-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Wijdicks EF, Young GB. Myoclonus status in comatose patients after cardiac arrest. Lancet. 1994;343:1642–3. doi: 10.1016/s0140-6736(94)93100-3. [DOI] [PubMed] [Google Scholar]
- 85.Stelzl T, von Bose MJ, Hogl B, Fuchs HH, Flugel KA. A comparison of the prognostic value of neuron-specific enolase serum levels and somatosensory evoked potentials in 13 reanimated patients. Eur J Emerg Med. 1995;2:24–7. doi: 10.1097/00063110-199503000-00006. [DOI] [PubMed] [Google Scholar]
- 86.Tiainen M, Kovala TT, Takkunen OS, Roine RO. Somatosensory and brainstem auditory evoked potentials in cardiac arrest patients treated with hypothermia. Crit Care Med. 2005;33:1736–40. doi: 10.1097/01.ccm.0000171536.63641.d9. [DOI] [PubMed] [Google Scholar]
- 87.Zingler VC, Krumm B, Bertsch T, Fassbender K, PohlmannEden B. Early prediction of neurological outcome after cardiopulmonary resuscitation: a multimodal approach combining neurobiochemical and electrophysiological investigations may provide high prognostic certainty in patients after cardiac arrest. Eur Neurol. 2003;49:79–84. doi: 10.1159/000068503. [DOI] [PubMed] [Google Scholar]
- 88.Rothstein TL. The role of evoked potentials in anoxic-ischemic coma and severe brain trauma. J Clin Neurophysiol. 2000;17:486–97. doi: 10.1097/00004691-200009000-00007. [DOI] [PubMed] [Google Scholar]
- 89.Zanatta P, Messerotti Benvenuti S, Baldanzi F, Bosco E. Painrelated middle-latency somatosensory evoked potentials in the prognosis of post anoxic coma: a preliminary report. Minerva Anestesiol. 2012;78:749–56. [PubMed] [Google Scholar]
- 90.Crepeau AZ, Rabinstein AA, Fugate JE, et al. Continuous EEG in therapeutic hypothermia after cardiac arrest: prognostic and clinical value. Neurology. 2013;80:339–44. doi: 10.1212/WNL.0b013e31827f089d. [DOI] [PubMed] [Google Scholar]
- 91.Oddo M, Rossetti AO. Early multimodal outcome prediction after cardiac arrest in patients treated with hypothermia. Crit Care Med. 2014;42:1340–7. doi: 10.1097/CCM.0000000000000211. [DOI] [PubMed] [Google Scholar]
- 92.Wennervirta JE, Ermes MJ, Tiainen SM, et al. Hypothermiatreated cardiac arrest patients with good neurological outcome differ early in quantitative variables of EEG suppression and epileptiform activity. Crit Care Med. 2009;37:2427–35. doi: 10.1097/CCM.0b013e3181a0ff84. [DOI] [PubMed] [Google Scholar]
- 93.Kawai M, Thapalia U, Verma A. Outcome from therapeutic hypothermia and EEG. J Clin Neurophysiol. 2011;28:483–8. doi: 10.1097/WNP.0b013e318231bfef. [DOI] [PubMed] [Google Scholar]
- 94.Oh SH, Park KN, Kim YM, et al. The prognostic value of continuous amplitude-integrated electroencephalogram applied immediately after return of spontaneous circulation in therapeutic hypothermia-treated cardiac arrest patients. Resuscitation. 2013;84:200–5. doi: 10.1016/j.resuscitation.2012.09.031. [DOI] [PubMed] [Google Scholar]
- 95.Oh SH, Park KN, Shon YM, et al. Continuous amplitude-integrated electroencephalographic monitoring is a useful prognostic tool for hypothermia-treated cardiac arrest patients. Circulation. 2015;132:1094–103. doi: 10.1161/CIRCULATIONAHA.115.015754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Oksanen T, Tiainen M, Skrifvars MB, et al. Predictive power of serum NSE and OHCA score regarding 6-month neurologic outcome after out-of-hospital ventricular fibrillation and therapeutic hypothermia. Resuscitation. 2009;80:165–70. doi: 10.1016/j.resuscitation.2008.08.017. [DOI] [PubMed] [Google Scholar]
- 97.Rundgren M, Karlsson T, Nielsen N, Cronberg T, Johnsson P, Friberg H. Neuron specific enolase and S-100B as predictors of outcome after cardiac arrest and induced hypothermia. Resuscitation. 2009;80:784–9. doi: 10.1016/j.resuscitation.2009.03.025. [DOI] [PubMed] [Google Scholar]
- 98.Lee BK, Jeung KW, Lee HY, Jung YH, Lee DH. Combining brain computed tomography and serum neuron specific enolase improves the prognostic performance compared to either alone in comatose cardiac arrest survivors treated with therapeutic hypothermia. Resuscitation. 2013;84:1387–92. doi: 10.1016/j.resuscitation.2013.05.026. [DOI] [PubMed] [Google Scholar]
- 99.Kim SH, Choi SP, Park KN, Youn CS, Oh SH, Choi SM. Early brain computed tomography findings are associated with outcome in patients treated with therapeutic hypothermia after out-of-hospital cardiac arrest. Scand J Trauma Resusc Emerg Med. 2013;21:57. doi: 10.1186/1757-7241-21-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Els T, Kassubek J, Kubalek R, Klisch J. Diffusion-weighted MRI during early global cerebral hypoxia: a predictor for clinical outcome? Acta Neurol Scand. 2004;110:361–7. doi: 10.1111/j.1600-0404.2004.00342.x. [DOI] [PubMed] [Google Scholar]
- 101.Mlynash M, Campbell DM, Leproust EM, et al. Temporal and spatial profile of brain diffusion-weighted MRI after cardiac arrest. Stroke. 2010;41:1665–72. doi: 10.1161/STROKEAHA.110.582452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Jorgensen EO, Holm S. The natural course of neurological recovery following cardiopulmonary resuscitation. Resuscitation. 1998;36:111–22. doi: 10.1016/s0300-9572(97)00094-4. [DOI] [PubMed] [Google Scholar]