

Abstract
Metacognitive therapy (MCT) is a recent psychological intervention for emotional disorders. Its efficacy in social anxiety disorder (SAD) is yet to be established. Aims: We examined the effectiveness of an MCT in patients with SAD. A two group case–control design with baseline, post, and 3 months follow-up was adopted. The control group received training in applied relaxation (AR). Four patients with Diagnostic and Statistical Manual-IV diagnosis of social anxiety were sequentially allotted to receive either MCT or AR. Patients were assessed on postevent processing (PEP), social anxiety, depression, and fear on negative evaluation. Clinical significance was calculated. MCT was more effective than AR in reducing social avoidance, PEP, and self-consciousness. While overall both interventions were effective in reducing social anxiety, MCT was marginally more effective. MCT may be a promising therapeutic approach in the management of SAD.
Key words: applied relaxation, metacognitive therapy, postevent processing, social anxiety
INTRODUCTION
Social anxiety disorder (SAD) is a debilitating condition[1] characterized by fear of negative evaluation (FNE), scrutiny in social and performance situations and significant avoidance of these situations.[2]
SAD affects 7-13% of individuals in Western societies across their lifetime, with a greater preponderance of males seeking treatment.[3] SAD has early onset,[4] with a mean age of onset of 10-13 years and significant co-morbidity.[5,6] Cognitive behavioral models describe four processes that maintain social anxiety. These include increased self-focused attention (SFA),[7] safety behaviors, overestimation of others' evaluation of their performance, anticipatory, and postevent processing (PEP).[8] A perceived lack of control over anxiety results in anticipation of social catastrophes, avoidance, safety behaviors, and postevent rumination.[9,10] Rumination as cognitive style,[11] has been associated with depression[12] generalized anxiety[13] and social anxiety.[10]
Despite existing evidence for the efficacy cognitive behavioral therapy (CBT) in SAD,[14,15,16,17] conventional CBT approaches in treating SAD do not focus explicitly on SFA, anticipatory and PEP.[7,18] Studies comparing CBT with applied relaxation (AR) suggest that AR is effective in reducing symptoms of anxiety.[19] There is a need to examine therapeutic interventions that focus on these factors, in addition to core symptoms of SAD.
MCT is based on the self-regulatory executive function model (S-REF).[20,21,22] According to S-REF model, people are trapped in negative emotions due to the activation of a perseverative thinking style, thought suppression, avoidance, called the cognitive-attentional syndrome. PEP, SFA, threat monitoring and thought suppression are addressed in MCT. MCT employs metacognitive techniques of external attention monitoring, banning rumination, correcting distorted self-image, and developing new strategies of processing external social environment. There is little or no verbal challenging of negative thoughts.[22] Detached mindfulness, involving the development of a reflective mode of thinking, is a key strategy in MCT to work on rumination.
Social anxiety is of significant mental health concern in India.[23] A majority of treatment seeking individuals are young adults, who experience distress and disability due to symptoms.[24] There is a need for therapeutic approaches that minimize relapse, by addressing maintaining factors in addition to core symptoms.
There is limited evidence for MCT in the treatment of SAD.[25] A few studies report the effectiveness of MCT in the treatment of generalized anxiety disorder.[26,27,28] Specific metacognitive strategies have also been included within CBT to address PEP.[29,30,31] No systematic studies have been undertaken in the Indian population, although some studies have employed mindfulness integrated CBT.[32] Research on metacognitions in social anxiety suggests a significant association with social anxiety.[33]
The present study attempted to examine the effectiveness of MCT in SAD, in reducing PEP, SFA, and social anxiety.
CASE REPORT
A case–control design with baseline, post, and follow-up assessment was adopted. Follow-up was carried out for primary outcome measures. The treatment group received MCT while the control group received AR.
Four consecutive patients, fulfilling Diagnostic and Statistical Manual-IV (DSM-IV)[1] criteria for a primary diagnosis of SAD, aged 18-45 years, stabilized on medication for 2 months were recruited from the outpatient services of the National Institute of Mental Health and Neurosciences, Bengaluru. Patients with a history of schizophrenia, psychosis, bipolar affective disorder, mental retardation, current psychoactive substance dependence (except nicotine), having undergone structured psychotherapy for SAD in the previous year were excluded.
Of the 8 patients recruited, four patients (MCT = 2; AR = 2) did not complete postassessment or attended <8 sessions. Therefore, the final sample consisted of four patients (MCT = 2; AR = 2).
Procedure
Patients were sequentially allotted to receive either MCT or AR. The study was approved by the Institute Ethics Committee, and all patients gave written informed consent. The study was registered in the clinical trials registry of the Indian Council of Medical Research (CTRI/2015/01/005394).
Diagnosis of Social Anxiety Disorder was reviewed using the MINI International Neuropsychiatric Interview 6.0.[34] The structured clinical interview for DSM-IV Axis II Personality Disorders was administered to assess for Axis II disorders.[35]
The primary outcome measure, PEP and was assessed using the PEP questionnaire PEPQ-R,[36] a nine item measure in which the individual rates anxiety following a social event, thoughts following it, attempts to reduce thinking about the event and avoidance. The scale has excellent reliabilities in clinical samples.
Severity was assessed using the clinical global impression scale-severity (CGI-S).[37] PEP-QR and CGI-S were administered by an independent rater.
The self-report version of the Liebowitz Social Anxiety Scale,[38,39] a 24 item scale was administered to assess social anxiety, fear, and avoidance. Social phobia rating scale[9] consisting of five scales for distress, avoidance, self-consciousness, frequency of safety-seeking behaviors, and negative beliefs in social situations was administered at baseline, post and follow-up. Only the self-consciousness item was selected for analysis. The brief FNE (BFNE) scale,[40] a 12-item scale was used to negative evaluation. It is a revised version of original FNE[41] with a 5-point Likert scale and correlates highly (r = 0.96) with the original FNE. The Beck's Depression Inventory-II-BDI-II;[42] a 21 item self-report measure was administered to assess the severity of depression.
Treatment program
The treatment program was based on the model described by Wells for emotional disorders. As there is no specific program for social anxiety, the transdiagnostic model was adopted.[22]
A universal case formulation approach was presented to patients receiving MCT. Treatment strategies included reducing SFA, modifying positive and negative metacognitive beliefs about SFA, situational attentional refocusing, behavioral experiments, reducing anticipatory processing, banning PEP and threat monitoring and identification of cognitive errors. Patients were trained in detached mindfulness using suppression-counter suppression strategies, and metaphors described in the manual.[22]
AR included education regarding social anxiety in, training in progressive muscle relaxation, release-only, cue-controlled, differential relaxation, and rapid relaxation.[43]
All patients received 8-10 individual sessions of 1.5 h duration. Therapy was delivered by the first author and was supervised by the second and third authors, both senior clinical psychologists. Homework was assigned and reviewed in each session. Therapist adherence to treatment was ensured by reviewing session transcripts.
Clinically significant changes (≥50%) between pre- and post-therapy and follow-up points were calculated using Blanchard and Schwarz[44] formula.

DISCUSSION
This study examined the effectiveness of MCT in patients with SAD, in reducing PEP, SFA, and social anxiety.
Sample description
All patients were male, and three out of the four were single. The mean age of the sample was 32 years (range = 26-45 years). Mean duration of illness was 4.92 years (range = 6 months 20 years) with late age at onset (mean = 28.5 years; range = 24-35 years). All patients had been stabilized on SSRIs for at least 2 months before recruitment. Both groups had one patient each with generalized social anxiety. Three patients reported moderate severity and one patient had severe social anxiety.
Postevent processing and self-focused attention
PEP-QR, patients in both groups, showed significant improvements at postintervention. Patients receiving MCT showing a greater percentage of improvement [Table 1] than those receiving AR. At 3 months follow-up, patients receiving MCT continued to improve significantly as compared to patients receiving AR [Table 1]. The magnitude of change seen on PEP for MCT was greater than AR at postintervention and follow-up points.
Table 1.
The changes in scores at baseline, post and follow-up on, postevent processing and social anxiety and self-focused attention
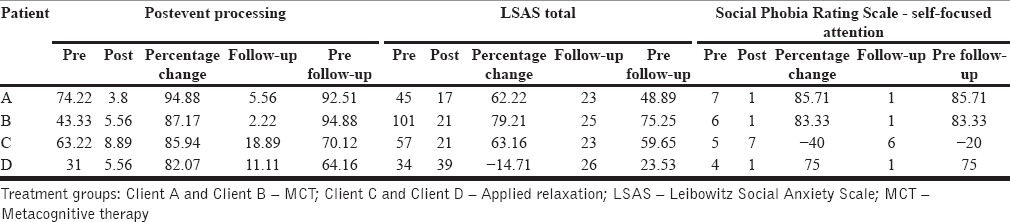
Patients receiving MCT group improved significantly on SFA (>80%) following intervention [Table 1]. One patient receiving AR showed clinically significant improvement (75%) while the other patient worsened. The magnitude change was significantly higher in patients receiving MCT. These findings indicate that MCT was effective in reducing SFA and PEP, while AR, led to limited changes. Both PEP and self-consciousness maintain social anxiety.[19] Socially anxious individuals focus excessively on detailed self-observation and monitoring[45] thereby increasing self-awareness of anxiety symptoms and enhancing arousal.[21]
Patients receiving MCT acquired skills in identifying the content of self-consciousness and were instructed to shift the focus of attention to external processing. They reported that this helped reduce anxiety. Changes in PEP were observed in the group receiving AR, but these changes were not consistently seen on SFA. The maintenance of gains at follow-up in patients receiving MCT suggests durability of gains. No significant change was seen in patients receiving AR. Thus, while patients receiving AR experienced arousal reduction, in the absence of specific strategies for SFA, there was no further impact. These findings highlight the need for specific strategies for SFA and PEP.
Social anxiety and symptom severity
Social anxiety was assessed using a self-report version of Leibowitz Social Anxiety Scale (LSAS) and the CGI-S. Patients receiving MCT showed significant improvement at posttreatment on LSAS [Table 1]. One out of two patients receiving AR showed clinically significant improvement. One patient receiving AR worsened at posttreatment. The percentage of change from baseline to follow-up indicates that two patients showed a clinically significant change (one patient each in MCT and AR group) and one other patient in the MCT group showing a trend towards clinically significant change (48.89%).
AR is a well-established program,[44] and changes in self-report of anxiety were expected. On LSAS-fear, patients receiving MCT reported clinically significant change at postintervention [Table 2], which was maintained at follow-up. The percentage of change in scores from baseline to follow-up was also clinically significant. However, in the AR group, there were no clinically significant changes on fear at both post and follow-up assessment, and one patient deteriorated at postintervention point, improving marginally at follow-up period. On the fear subscale, patients receiving MCT showing greater change at postintervention and follow-up, than patients receiving AR [Table 2].
Table 2.
The changes in scores at baseline, post and follow-up on Leibowitz Social Anxiety Scale subscales of fear and avoidance
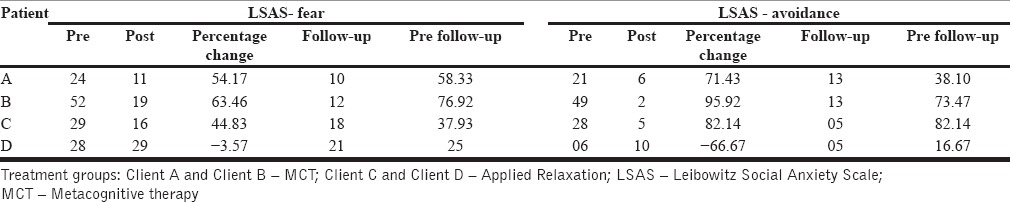
On LSAS-avoidance at postintervention, three out of the four patients reported a significant change, while one patient receiving AR worsened at postintervention on both fear and avoidance, with marginal improvement at follow-up [Table 2]. At follow-up, only two patients reported clinical significant changes. MCT resulted in greater changes in the experience of fear than avoidance at follow-up.
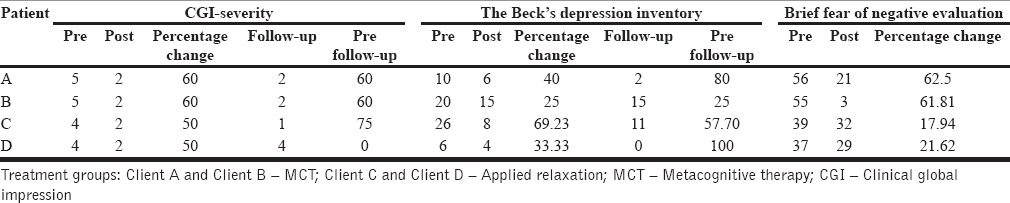
Changes on CGI-S were higher in patients receiving MCT (60%) as compared to AR (50%), further supporting the effectiveness of MCT in reducing symptom severity [Table 3].
Table 3.
The changes in scores on symptom severity, depression, and fear of negative evaluation
PEP maintains social avoidance.[19] Socially anxious individuals brood and experience distress following social events, leading to self-devaluation, anticipatory anxiety, and avoidance behaviors.[7] Identification and banning PEP is likely to have led to prevention of negative self and situational appraisal, reduced anxiety, thereby decreased social avoidance. In situation safety behaviors maintain social avoidance by preventing disconfirmation of negative beliefs.[18] Patients were instructed to drop safety behaviors during exposure, and this may have contributed to decrease in social avoidance. Studies indicate that exposure plus dropping safety behaviors reduces social anxiety and avoidance.[46]
Patients receiving MCT showed significantly greater improvement at postintervention (62.5% and 61.81%) on BFNE as compared to AR (17.94% and 21.625), indicating effectiveness of MCT in producing cognitive change [Table 3].
Patients receiving AR showed marginally greater changes than patients receiving MCT at postintervention on BDI-II. However, at 3 months follow-up, these differences were not observed [Table 3]. Thus, while anxiety reduction can impact depressive symptoms in the short period, they may not be sufficient to maintain gains, and it is important to address cognitive processes such as PEP that may increase negative affect.
MCT appears to be a promising approach to social anxiety. As this was a pilot investigation, the sample size was small and did not allow for further statistical analysis and interpretation. The strengths of the study include the use of a manualized protocol, an equal number of therapist contacts, 3 months follow-up and the inclusion of an active comparison group.
A larger sample would help in building more robust evidence for MCT in SAD. Its relative efficacy with other approaches such as exposure, CBT must be examined.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- 2.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 2000. [Google Scholar]
- 3.Furmark T. Social phobia: Overview of community surveys. Acta Psychiatr Scand. 2002;105:84–93. doi: 10.1034/j.1600-0447.2002.1r103.x. [DOI] [PubMed] [Google Scholar]
- 4.Rapee RM. Social Phobia: Diagnosis, Assessment, and Treatment. Guildford Press; 1995. Descriptive psychopathology of social phobia; pp. 41–66. [Google Scholar]
- 5.Otto MW, Pollack MH, Maki KM, Gould RA, Worthington JJ, 3rd, Smoller JW, et al. Childhood history of anxiety disorders among adults with social phobia: Rates, correlates, and comparisons with patients with panic disorder. Depress Anxiety. 2001;14:209–13. doi: 10.1002/da.1068. [DOI] [PubMed] [Google Scholar]
- 6.Schneier FR, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia. Comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282–8. doi: 10.1001/archpsyc.1992.01820040034004. [DOI] [PubMed] [Google Scholar]
- 7.Hirsch CR, Clark DM. Information-processing bias in social phobia. Clin Psychol Rev. 2004;24:799–825. doi: 10.1016/j.cpr.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 8.Rapee RM, Heimberg RG. A cognitive-behavioral model of anxiety in social phobia. Behav Res Ther. 1997;35:741–56. doi: 10.1016/s0005-7967(97)00022-3. [DOI] [PubMed] [Google Scholar]
- 9.Wells A. Cognitive Therapy of Anxiety Disorders: A Practice Manual and Conceptual Guide. Chichester, UK: Wiley; 1997. pp. 167–99. [Google Scholar]
- 10.Mellings TM, Alden LE. Cognitive processes in social anxiety: The effects of self-focus, rumination and anticipatory processing. Behav Res Ther. 2000;38:243–57. doi: 10.1016/s0005-7967(99)00040-6. [DOI] [PubMed] [Google Scholar]
- 11.Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol. 1991;100:569–82. doi: 10.1037//0021-843x.100.4.569. [DOI] [PubMed] [Google Scholar]
- 12.Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking Rumination. Perspect Psychol Sci. 2008;3:400–24. doi: 10.1111/j.1745-6924.2008.00088.x. [DOI] [PubMed] [Google Scholar]
- 13.Fresco DM, Frankel A, Mennin DS, Turk CL, Heimberg RG. Distinct and overlapping features of rumination and worry: The relationship of cognitive production to negative affective states. Cognit Ther Res. 2002;26:179–88. [Google Scholar]
- 14.Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: Current status and future directions. Biol Psychiatry. 2002;51:101–8. doi: 10.1016/s0006-3223(01)01183-0. [DOI] [PubMed] [Google Scholar]
- 15.Fedoroff IC, Taylor S. Psychological and pharmacological treatments of social phobia: A meta-analysis. J Clin Psychopharmacol. 2001;21:311–24. doi: 10.1097/00004714-200106000-00011. [DOI] [PubMed] [Google Scholar]
- 16.Gould RA, Buckminster S, Pollack MH, Otto MW, Yap L. Cognitive-behavioral and pharmacological treatment for social phobia: A meta-analysis. Clin Psychol Sci Pract. 1997;4:291–306. [Google Scholar]
- 17.Taylor S. Meta-analysis of cognitive-behavioral treatments for social phobia. J Behav Ther Exp Psychiatry. 1996;27:1–9. doi: 10.1016/0005-7916(95)00058-5. [DOI] [PubMed] [Google Scholar]
- 18.Clark DM, Ehlers A, Hackmann A, McManus F, Fennell M, Grey N, et al. Cognitive therapy versus exposure and applied relaxation in social phobia: A randomized controlled trial. J Consult Clin Psychol. 2006;74:568–78. doi: 10.1037/0022-006X.74.3.568. [DOI] [PubMed] [Google Scholar]
- 19.Clark DM, Wells A. A cognitive model of social phobia. In: Hiemberg R, Liebowitz M, Hope DA, Schneier FR, editors. Social Phobia: Diagnostic Assessment and Treatment. New York: Guildford Press; 1995. pp. 69–93. [Google Scholar]
- 20.Wells A. Cognition about cognition: Metacognitive therapy and change in generalized anxiety disorder and social phobia. Cogn Behav Pract. 2007;14:18–25. [Google Scholar]
- 21.Wells A, Matthews G. Attention and Emotion: A Clinical Perspective. Hoves (UK): Lawrence Erlbaum; 1994. [Google Scholar]
- 22.Wells A. Metacognitive Therapy for Anxiety and Depression. New York: Guilford Press; 2009. [Google Scholar]
- 23.Shah P, Kataria L. Social phobia and its impact in Indian university students. Internet J Ment Health. 2009;6:2. [Google Scholar]
- 24.Jain M, Sudhir PM. Dimensions of perfectionism and perfectionistic self-presentation in social phobia. Asian J Psychiatr. 2010;3:216–21. doi: 10.1016/j.ajp.2010.08.006. [DOI] [PubMed] [Google Scholar]
- 25.Behadouri MH, Bakhsh MJ, Kajbaf MB, Faramarzi S. The effectiveness of metacognitive therapy on meta-cognitive beliefs and cognitive trust in patients with social phobia disorder. J Clin Psychol. 2012;4:33. [Google Scholar]
- 26.Wells A, Welford M, King P, Papageorgiou C, Wisely J, Mendel E. A pilot randomized trial of metacognitive therapy vs applied relaxation in the treatment of adults with generalized anxiety disorder. Behav Res Ther. 2010;48:429–34. doi: 10.1016/j.brat.2009.11.013. [DOI] [PubMed] [Google Scholar]
- 27.Kennair LE, Nordahl HM. A randomized controlled trial comparing the effectiveness of cognitive behavior therapy with metacognitive therapy in the treatment of patients with generalized anxiety disorder. Second International Conference of Metacognitive Therapy – Programme and Abstracts. 2013 [Google Scholar]
- 28.Nordahl HM. Effectiveness of brief metacognitive therapy versus cognitive behavioral therapy in a general outpatient setting. Int J Cogn Ther. 2009;2:152–9. [Google Scholar]
- 29.McEvoy PM, Mahoney A, Perini SJ, Kingsep P. Changes in post-event processing and metacognitions during cognitive behavioral group therapy for social phobia. J Anxiety Disord. 2009;23:617–23. doi: 10.1016/j.janxdis.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 30.Price M, Anderson PL. The impact of cognitive behavioral therapy on post event processing among those with social anxiety disorder. Behav Res Ther. 2011;49:132–7. doi: 10.1016/j.brat.2010.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cassin SE, Rector NA. Mindfulness and the attenuation of post-event processing in social phobia: An experimental investigation. Cogn Behav Ther. 2011;40:267–78. doi: 10.1080/16506073.2011.614275. [DOI] [PubMed] [Google Scholar]
- 32.Salaam AK. Unpublished Doctoral Thesis Submitted to the Department of Clinical Psychology, NIMHANS (Institute of National Importance) Bengaluru. 2013. Effectiveness of Mindfulness Based Cognitive Behaviour Therapy in Social Phobia. [Google Scholar]
- 33.Shankar D. Dysfunctional cognitions and metacognitions in patients with social phobia. M.Phil Dissertation. In: Shah A, Rao K, editors. Psychological Research in Mental Health and Neurosciences, 1957-2007. Bangalore: NIMHANS (Deemed University); 2006. [Google Scholar]
- 34.Sheehan DV, Janavs J, Baker R, Harnett-Sheehan K, Knapp E, Sheehan M, et al. MINI – Mini International Neuropsychiatric Interview. English Version 5.0.0 – DSM-IV. J Clin Psychiatry. 1998;59:34–57. [PubMed] [Google Scholar]
- 35.First MB, Gibbon M, Spitzer RL, Williams JB. Structured Clinical Interview for DSM-IV Axis II Personality Disorders, (SCID-II) Washington, D.C: American Psychiatric Press, Inc\; 1997. [Google Scholar]
- 36.McEvoy PM, Kingsep P. The post-event processing questionnaire in a clinical sample with social phobia. Behav Res Ther. 2006;44:1689–97. doi: 10.1016/j.brat.2005.12.005. [DOI] [PubMed] [Google Scholar]
- 37.Guy W. US Dept Health, Education, and Welfare Publication (ADM) 76-338. Rockville, MD: National Institute of Mental Health; 1976. ECDEU Assessment Manual for Psychopharmacology; pp. 218–22. [Google Scholar]
- 38.Liebowitz MR. Social phobia. Mod Probl Pharmacopsychiatry. 1987;22:141–73. doi: 10.1159/000414022. [DOI] [PubMed] [Google Scholar]
- 39.Baker SL, Heinrichs N, Kim HJ, Hofmann SG. The liebowitz social anxiety scale as a self-report instrument: A preliminary psychometric analysis. Behav Res Ther. 2002;40:701–15. doi: 10.1016/s0005-7967(01)00060-2. [DOI] [PubMed] [Google Scholar]
- 40.Leary MR. A brief version of the fear of negative evaluation scale. Pers Soc Psychol Bull. 1983;9:371–5. [Google Scholar]
- 41.Watson D, Friend R. Measurement of social-evaluative anxiety. J Consult Clin Psychol. 1969;33:448–57. doi: 10.1037/h0027806. [DOI] [PubMed] [Google Scholar]
- 42.Beck AT, Steer R, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation; 1996. [Google Scholar]
- 43.Ost LG. Applied relaxation: Description of a coping technique and review of controlled studies. Behav Res Ther. 1987;25:397–409. doi: 10.1016/0005-7967(87)90017-9. [DOI] [PubMed] [Google Scholar]
- 44.Blanchard EB, Schwarz SP. Clinically significant changes in behavioral medicine. Behav Assess. 1988;10:171–88. [Google Scholar]
- 45.Woody SR. Effects of focus of attention on anxiety levels and social performance of individuals with social phobia. J Abnorm Psychol. 1996;105:61–9. doi: 10.1037//0021-843x.105.1.61. [DOI] [PubMed] [Google Scholar]
- 46.Garcia-Palacios A, Botella C. The effects of dropping in-situ ation safety behaviors in the treatment of social phobia. Behav Interv. 2003;18:23. [Google Scholar]