

Abstract
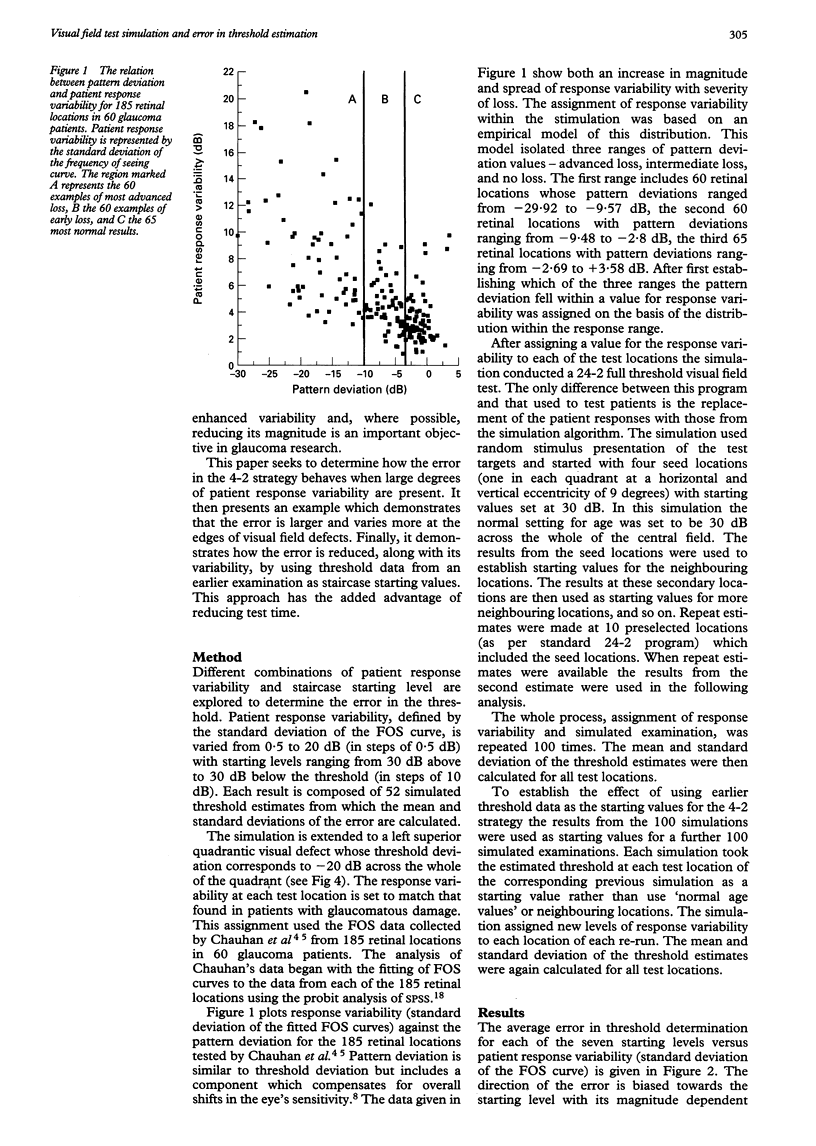
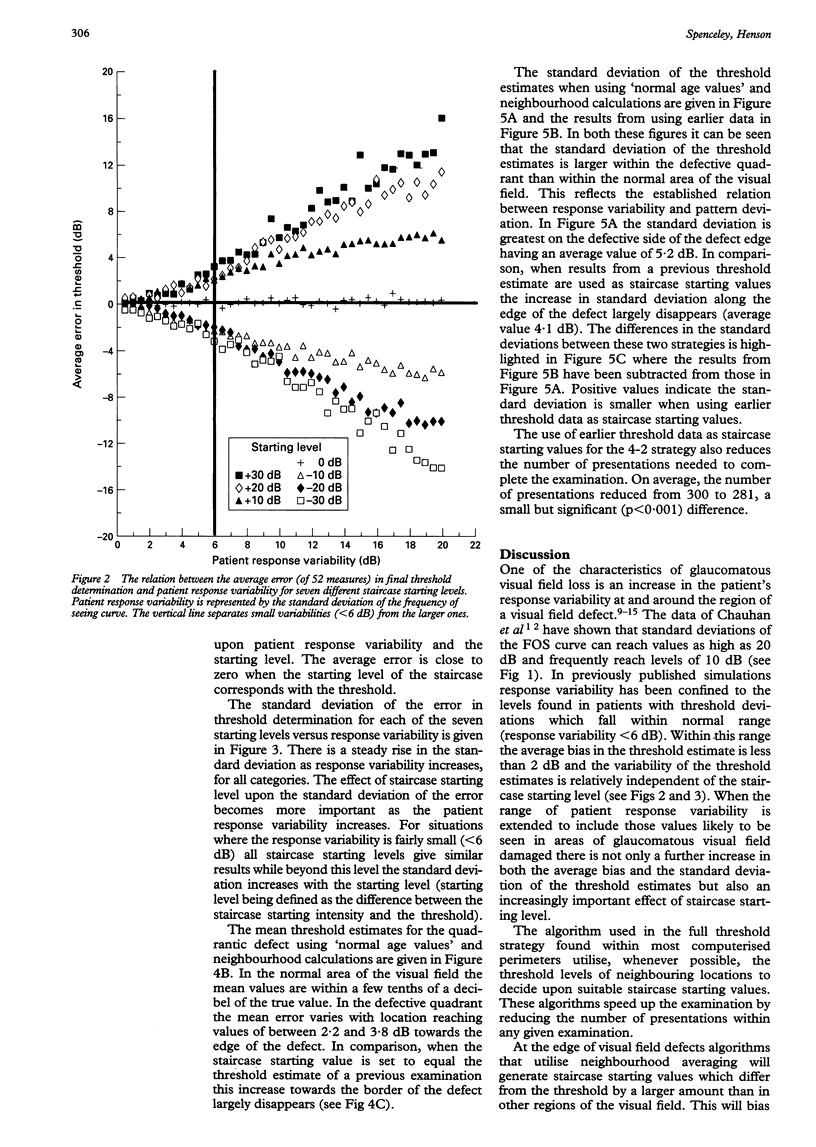
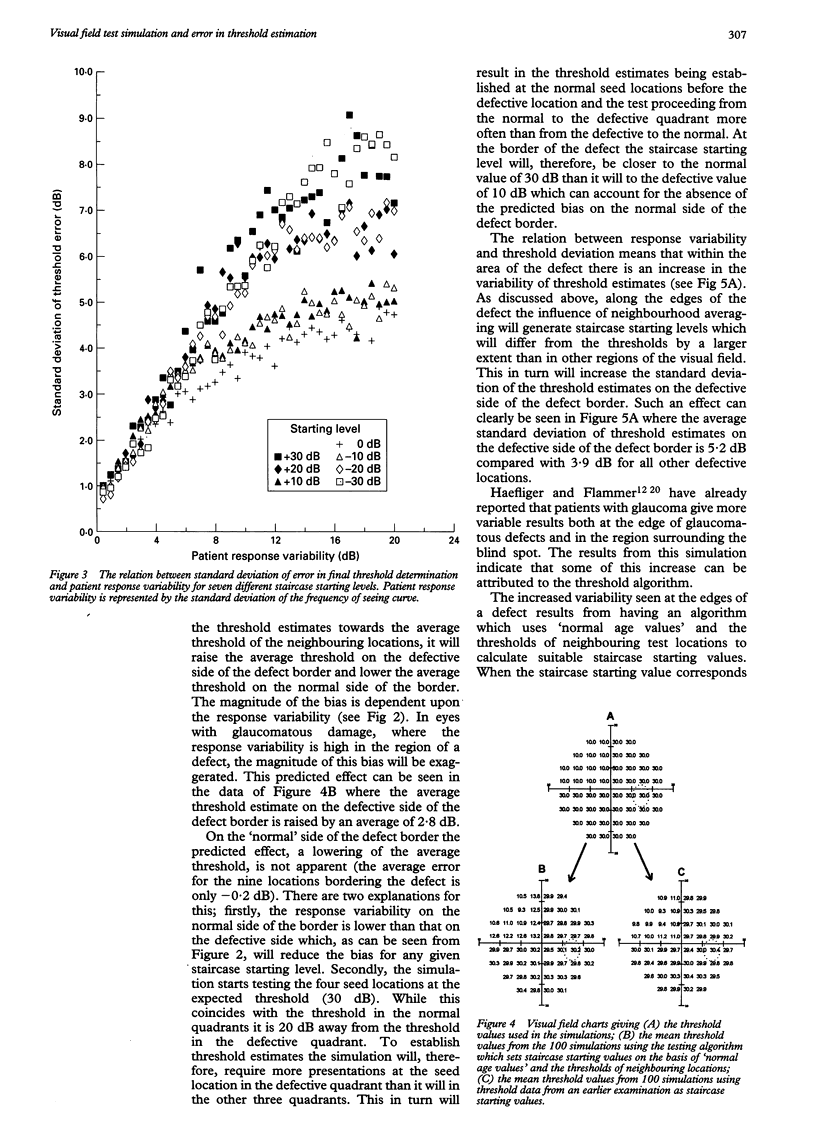
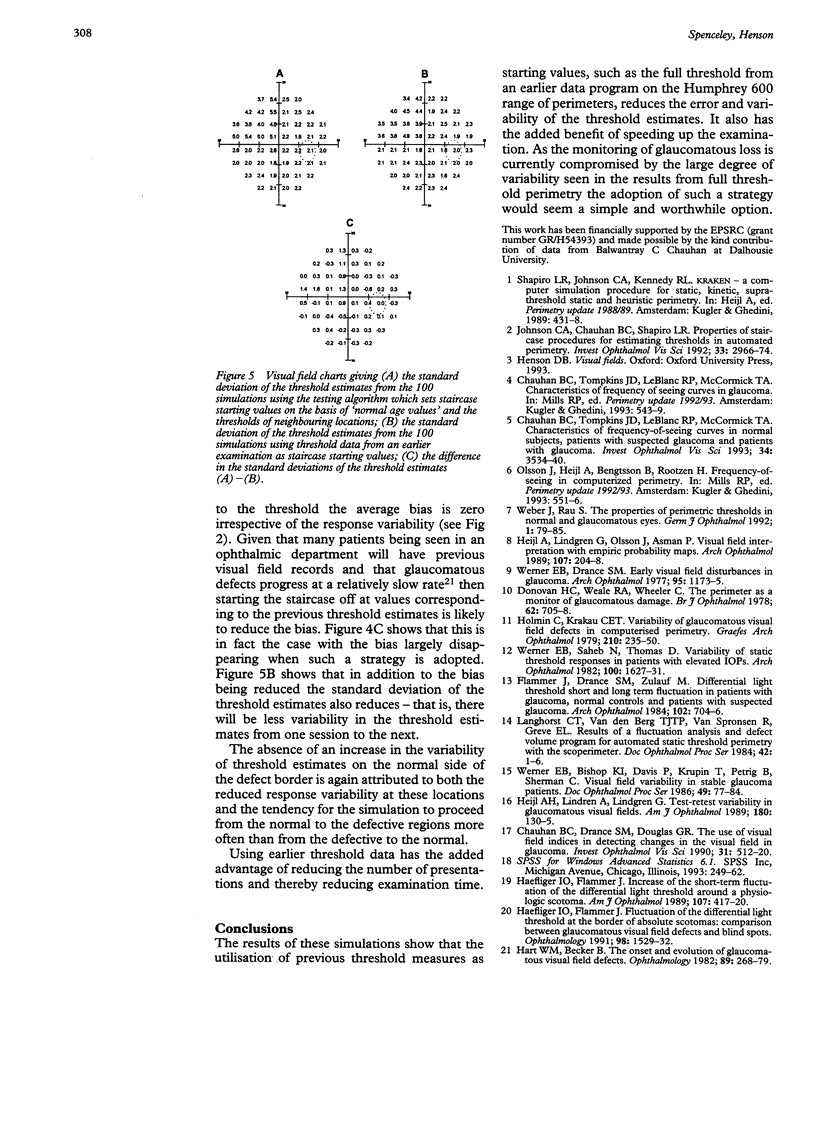
AIM: To establish, via computer simulation, the effects of patient response variability and staircase starting level upon the accuracy and repeatability of static full threshold visual field tests. METHOD: Patient response variability, defined by the standard deviation of the frequency of seeing versus stimulus intensity curve, is varied from 0.5 to 20 dB (in steps of 0.5 dB) with staircase starting levels ranging from 30 dB below to 30 dB above the patient's threshold (in steps of 10 dB). Fifty two threshold estimates are derived for each condition and the error of each estimate calculated (difference between the true threshold and the threshold estimate derived from the staircase procedure). The mean and standard deviation of the errors are then determined for each condition. The results from a simulated quadrantic defect (response variability set to typical values for a patient with glaucoma) are presented using two different algorithms. The first corresponds with that normally used when performing a full threshold examination while the second uses results from an earlier simulated full threshold examination for the staircase starting values. RESULTS: The mean error in threshold estimates was found to be biased towards the staircase starting level. The extent of the bias was dependent upon patient response variability. The standard deviation of the error increased both with response variability and staircase starting level. With the routinely used full threshold strategy the quadrantic defect was found to have a large mean error in estimated threshold values and an increase in the standard deviation of the error along the edge of the defect. When results from an earlier full threshold test are used as staircase starting values this error and increased standard deviation largely disappeared. CONCLUSION: The staircase procedure widely used in threshold perimetry increased the error and the variability of threshold estimates along the edges of defects. Using earlier data, when available, overcomes this problem and reduces examination time.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chauhan B. C., Drance S. M., Douglas G. R. The use of visual field indices in detecting changes in the visual field in glaucoma. Invest Ophthalmol Vis Sci. 1990 Mar 1;31(3):512–520. [PubMed] [Google Scholar]
- Chauhan B. C., Tompkins J. D., LeBlanc R. P., McCormick T. A. Characteristics of frequency-of-seeing curves in normal subjects, patients with suspected glaucoma, and patients with glaucoma. Invest Ophthalmol Vis Sci. 1993 Dec;34(13):3534–3540. [PubMed] [Google Scholar]
- Donovan H. C., Weale R. A., Wheeler C. The perimeter as a monitor of glaucomatous changes. Br J Ophthalmol. 1978 Oct;62(10):705–708. doi: 10.1136/bjo.62.10.705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flammer J., Drance S. M., Zulauf M. Differential light threshold. Short- and long-term fluctuation in patients with glaucoma, normal controls, and patients with suspected glaucoma. Arch Ophthalmol. 1984 May;102(5):704–706. doi: 10.1001/archopht.1984.01040030560017. [DOI] [PubMed] [Google Scholar]
- Haefliger I. O., Flammer J. Fluctuation of the differential light threshold at the border of absolute scotomas. Comparison between glaucomatous visual field defects and blind spots. Ophthalmology. 1991 Oct;98(10):1529–1532. doi: 10.1016/s0161-6420(91)32093-1. [DOI] [PubMed] [Google Scholar]
- Haefliger I. O., Flammer J. Increase of the short-term fluctuation of the differential light threshold around a physiologic scotoma. Am J Ophthalmol. 1989 Apr 15;107(4):417–420. doi: 10.1016/0002-9394(89)90667-3. [DOI] [PubMed] [Google Scholar]
- Hart W. M., Jr, Becker B. The onset and evolution of glaucomatous visual field defects. Ophthalmology. 1982 Mar;89(3):268–279. doi: 10.1016/s0161-6420(82)34798-3. [DOI] [PubMed] [Google Scholar]
- Heijl A., Lindgren A., Lindgren G. Test-retest variability in glaucomatous visual fields. Am J Ophthalmol. 1989 Aug 15;108(2):130–135. doi: 10.1016/0002-9394(89)90006-8. [DOI] [PubMed] [Google Scholar]
- Heijl A., Lindgren G., Olsson J., Asman P. Visual field interpretation with empiric probability maps. Arch Ophthalmol. 1989 Feb;107(2):204–208. doi: 10.1001/archopht.1989.01070010210024. [DOI] [PubMed] [Google Scholar]
- Holmin C., Krakau C. E. Variability of glaucomatous visual field defects in computerized perimetry. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1979 Jun 15;210(4):235–250. [PubMed] [Google Scholar]
- Johnson C. A., Chauhan B. C., Shapiro L. R. Properties of staircase procedures for estimating thresholds in automated perimetry. Invest Ophthalmol Vis Sci. 1992 Sep;33(10):2966–2974. [PubMed] [Google Scholar]
- Weber J., Rau S. The properties of perimetric thresholds in normal and glaucomatous eyes. Ger J Ophthalmol. 1992;1(2):79–85. [PubMed] [Google Scholar]
- Werner E. B., Drance S. M. Early visual field disturbances in glaucoma. Arch Ophthalmol. 1977 Jul;95(7):1173–1175. doi: 10.1001/archopht.1977.04450070071002. [DOI] [PubMed] [Google Scholar]
- Werner E. B., Saheb N., Thomas D. Variability of static visual threshold responses in patients with elevated IOPs. Arch Ophthalmol. 1982 Oct;100(10):1627–1631. doi: 10.1001/archopht.1982.01030040605010. [DOI] [PubMed] [Google Scholar]